ABOS Part I Orthopedic Surgery Review: Proximal Humerus, Hip Arthroplasty & Acetabular Fractures | Part 21544
Key Takeaway
This orthopedic surgery review module offers 41 advanced multiple-choice questions designed for ABOS Part I and AAOS OITE preparation. It comprehensively covers high-yield clinical topics including proximal humerus fractures, total hip arthroplasty, and complex acetabular fractures, providing detailed explanations to enhance understanding and exam readiness.
ABOS Part I Orthopedic Surgery Review: Proximal Humerus, Hip Arthroplasty & Acetabular Fractures | Part 21544
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 72-year-old female presents to the emergency department after a low-energy fall onto her outstretched arm. Radiographs reveal a displaced two-part surgical neck fracture of the proximal humerus with 1.2 cm displacement and 50 degrees of varus angulation. She has a history of well-controlled hypertension and type 2 diabetes. She lives independently, is right-hand dominant, and enjoys gardening and playing cards. On examination, she has intact neurovascular status distally. Based on the provided case information, which of the following is the MOST appropriate initial management strategy?
Explanation
Correct Answer: D
The case describes a 72-year-old female with a displaced two-part surgical neck fracture. While the fracture is displaced beyond the typical non-operative criteria (>1 cm displacement, >45 degrees angulation), the text emphasizes that non-operative management is often appropriate for 'two-part surgical neck fractures in elderly, low-demand patients with minimal displacement' and for 'elderly, low-demand, sedentary patients' even with significant comorbidities. However, the patient's activity level (gardening, playing cards) suggests she is not entirely sedentary. The PROXIMAL trial (2015) specifically found no significant difference in outcomes between locking plate fixation and non-operative treatment for displaced proximal humerus fractures in adults, particularly in an older population. This supports a more critical selection of surgical candidates and often favors non-operative management initially, especially for two-part surgical neck fractures, even if displaced, in older individuals who are not high-demand athletes. Early pendulum exercises are a cornerstone of non-operative rehabilitation to prevent stiffness.
Option A (ORIF) might be considered for younger, active patients or specific fracture patterns, but for an elderly patient with a two-part surgical neck fracture, the PROXIMAL trial suggests it may not offer superior outcomes to non-operative care, and carries surgical risks.
Options B (Hemiarthroplasty) and C (RTSA) are typically reserved for more complex fractures (e.g., comminuted three- or four-part fractures, head-splitting fractures, severe osteopenia, or compromised rotator cuff), which are not described here. A two-part surgical neck fracture does not typically warrant arthroplasty as an initial treatment.
Option E (Closed reduction and percutaneous pinning) is less common for displaced surgical neck fractures in the elderly due to concerns about pin tract infection, loss of reduction, and difficulty achieving stable fixation in osteoporotic bone compared to locking plates, and is not explicitly mentioned as a primary option for this specific scenario in the text.
Question 2
A 35-year-old male sustains a high-energy trauma resulting in a complex proximal humerus fracture. Imaging reveals displacement of the greater tuberosity, lesser tuberosity, and surgical neck fragments relative to the humeral head. The humeral head itself remains in anatomical alignment with the glenoid. According to the Neer classification system, how would this fracture be categorized?
Explanation
Correct Answer: D
The Neer classification system categorizes PHFs based on the number of displaced 'parts' (humeral head, greater tuberosity, lesser tuberosity, and surgical neck) and displacement criteria (>1 cm displacement or >45 degrees angulation). The question states 'displacement of the greater tuberosity, lesser tuberosity, and surgical neck fragments relative to the humeral head.' This means three segments (greater tuberosity, lesser tuberosity, surgical neck) are displaced relative to the humeral head, which itself is considered the fourth part. Therefore, this is a four-part fracture.
A one-part fracture is nondisplaced or minimally displaced.
A two-part fracture involves displacement of one major segment relative to the others (e.g., surgical neck, greater tuberosity).
A three-part fracture involves displacement of two segments relative to the humeral head.
A fracture-dislocation involves any of the above combined with glenohumeral dislocation, which is not described here as the humeral head remains in anatomical alignment with the glenoid.
Question 3
During open reduction and internal fixation of a displaced proximal humerus fracture via a deltopectoral approach, the surgeon is meticulously dissecting to expose the surgical neck. Which neurovascular structure is at the HIGHEST risk of iatrogenic injury in this specific region, approximately 5-7 cm distal to the acromion?
Explanation
Correct Answer: D
The text explicitly states: 'The Axillary Nerve: Most commonly injured nerve in PHFs or during surgical approaches. It wraps around the surgical neck, approximately 5-7 cm distal to the acromion, innervating the deltoid and teres minor.' This makes it the structure at highest risk during dissection around the surgical neck.
The Musculocutaneous nerve is located more medially and anteriorly, supplying the biceps and brachialis, and is generally less vulnerable during a standard deltopectoral approach to the surgical neck.
The Radial nerve is located more distally and posteriorly in the spiral groove, making it less susceptible to injury during proximal humerus plating via a deltopectoral approach.
The Axillary artery and vein are positioned medially and anteriorly, at risk during medial screw placement or extreme retraction, but the axillary nerve is more directly in the path of dissection around the surgical neck.
The Brachial plexus is vulnerable in high-energy injuries or fracture-dislocations but is generally not the most commonly injured structure during a standard deltopectoral approach for fracture fixation unless there is extreme retraction or a very proximal and medial dissection.
Question 4
A 68-year-old male undergoes open reduction and internal fixation with a locking plate for a three-part proximal humerus fracture. Postoperatively, radiographs show good reduction and hardware placement. Six months later, he presents with persistent shoulder pain, limited range of motion, and new radiographs demonstrate collapse of the humeral head into a varus deformity, with several screws having penetrated the articular surface. Which of the following factors is MOST likely to have contributed to this complication?
Explanation
Correct Answer: D
The scenario describes 'collapse of the humeral head into a varus deformity, with several screws having penetrated the articular surface.' This is a classic presentation of screw cutout and varus collapse. The text explicitly states: 'Loss of medial calcar support significantly increases the risk of screw cutout and construct failure.' It further notes that 'Calcar Screws: Crucial for medial column support. At least one, ideally two, calcar screws should be directed inferiorly and medially towards the calcar region to resist varus collapse.' Therefore, inadequate medial calcar support is the most direct cause of varus collapse and subsequent screw cutout.
Inadequate fixation of the lesser tuberosity (A) would primarily lead to internal rotation deformity or subscapularis dysfunction, not typically varus collapse and screw cutout.
Excessive external rotation during early rehabilitation (B) could stress tuberosity repairs or lead to dislocation in unstable fractures, but is not the primary mechanism for varus collapse and screw cutout.
Disruption of the posterior circumflex humeral artery (C) contributes to avascular necrosis (AVN), which is a different complication, although AVN can eventually lead to collapse. However, the immediate description of varus collapse and screw cutout points more directly to mechanical failure of fixation due to lack of support.
Premature removal of the sling at 2 weeks post-op (E) would primarily risk loss of reduction or stress on healing soft tissues, but the fundamental mechanical failure described (varus collapse, screw cutout) is more related to the initial construct stability, particularly medial support.
Question 5
A 55-year-old female sustains a displaced greater tuberosity fracture of the right shoulder after a fall. Radiographs confirm a >5 mm displacement of the greater tuberosity fragment. She is active, right-hand dominant, and has no significant comorbidities. Which of the following is the MOST compelling reason for operative intervention in this patient?
Explanation
Correct Answer: C
The text states, 'Displaced Greater Tuberosity Fractures: Displacement >5 mm, particularly in active patients, due to the high risk of impingement and rotator cuff dysfunction if left unreduced. Can lead to subacromial impingement and weakness.' This directly addresses the scenario of a displaced greater tuberosity fracture in an active patient.
High risk of avascular necrosis of the humeral head (A) is primarily associated with multi-part fractures (three- and four-part) and head-splitting fractures, not typically an isolated displaced greater tuberosity fracture.
Potential for internal rotation contracture (B) is more commonly associated with displaced lesser tuberosity fractures, which affect the subscapularis tendon.
Difficulty achieving union with non-operative management (D) is not the primary concern for displaced greater tuberosity fractures; rather, it's the functional impairment from malunion (impingement, cuff dysfunction) that drives operative indications.
Increased risk of axillary nerve injury with conservative care (E) is incorrect. Axillary nerve injury is a risk of the initial trauma or surgical intervention, not conservative management.
Question 6
A 78-year-old male with severe osteoporosis and a history of a massive, irreparable rotator cuff tear presents with a highly comminuted four-part proximal humerus fracture after a fall. He is physiologically fit for surgery and desires to regain as much function as possible. Based on the current literature and guidelines, which surgical option is MOST likely to provide predictable pain relief and functional improvement in this specific patient?
Explanation
Correct Answer: D
The patient presents with a 'highly comminuted four-part proximal humerus fracture,' 'severe osteoporosis,' and a 'massive, irreparable rotator cuff tear' in an 'elderly' patient. The text explicitly states: 'Reverse Total Shoulder Arthroplasty (RTSA) has gained significant traction, especially in elderly patients with complex PHFs, pre-existing rotator cuff dysfunction, or severe osteopenia. Multiple studies demonstrate more predictable pain relief and functional outcomes with RTSA compared to hemiarthroplasty or ORIF in this specific demographic, as it bypasses the need for tuberosity healing and relies on the deltoid for elevation.' This perfectly matches the patient's profile and desired outcome.
ORIF with a locking plate (A) would be highly challenging and likely to fail given the severe comminution, severe osteoporosis, and irreparable rotator cuff tear. The ability to achieve stable fixation and tuberosity healing would be severely compromised.
Hemiarthroplasty (B) has historically been an option for complex fractures in older patients, but the text notes 'outcomes can be variable, often limited by tuberosity healing and rotator cuff function.' Given the irreparable rotator cuff tear and severe osteoporosis, hemiarthroplasty would likely yield poor functional results.
Non-operative management (C) for a highly comminuted four-part fracture in a patient desiring function would likely result in significant pain, malunion, and very poor function.
Intramedullary nailing (E) is less common for complex PHFs and is generally not indicated for four-part fractures, especially with severe osteoporosis and rotator cuff compromise, due to difficulty controlling head rotation and potential for AVN.
Question 7
A 60-year-old patient is undergoing open reduction and internal fixation of a displaced proximal humerus fracture. The surgical team is preparing for patient positioning. The image provided shows a typical setup for shoulder surgery. Which of the following statements accurately describes a key advantage of the Beach Chair position, as depicted in the general context of shoulder surgery setups?
Explanation
Correct Answer: C
The text states, regarding the Beach Chair Position: 'Advantages: Excellent visualization for the deltopectoral approach, allows for easy assessment of shoulder range of motion during the procedure, less blood loss due to reverse Trendelenburg, and ability to assess rotator cuff integrity.' The image depicts a patient draped for shoulder surgery, consistent with either beach chair or lateral decubitus, but the question specifically asks about the advantages of the Beach Chair position.
Option A is incorrect; the text suggests lateral decubitus 'May offer improved stability for patients with certain comorbidities,' implying beach chair might be less stable in some cases.
Option B is incorrect; while arthroscopy can be done in beach chair, the text mentions lateral decubitus 'Can be preferred... if shoulder arthroscopy is concurrently planned.'
Option D is incorrect; the text explicitly lists 'Monitor blood pressure closely for potential cerebral hypoperfusion ("beach chair hypotension")' as a precaution, indicating a risk, not a minimization of risk.
Option E is incorrect; the text states beach chair provides 'Excellent visualization for the deltopectoral approach,' which is an anterior approach. Lateral decubitus 'Can be preferred for certain posterior approaches.'
Question 8
A 48-year-old male presents with a displaced two-part surgical neck fracture. He is a highly active individual and desires to return to competitive sports. During pre-operative planning, a CT scan is obtained. Which of the following pieces of information obtained from the CT scan is MOST critical for planning the surgical approach and fixation strategy?
Explanation
Correct Answer: B
The text highlights the importance of CT scans: 'Computed Tomography (CT) Scan: Indispensable for complex fractures, particularly three- and four-part fractures, fracture-dislocations, and head-splitting injuries. Provides detailed information on comminution, articular involvement, glenoid impression fractures, and precise tuberosity displacement. 3D reconstructions are invaluable for understanding fracture morphology and planning reduction maneuvers.' For a displaced two-part surgical neck fracture, understanding the extent of comminution and any subtle articular involvement (even if not a primary head-splitting fracture) is crucial for selecting the appropriate plate, screw trajectories, and reduction techniques to restore anatomy and prevent complications like screw cutout or post-traumatic arthritis.
Assessment of rotator cuff integrity (A) is more typically done with MRI, though severe tears might be suspected clinically. While important, CT's primary strength for fracture planning is bony detail.
Identification of brachial plexus pathology (C) is also better assessed with MRI or clinical neurophysiological studies, not typically the primary role of CT in acute fracture planning.
Confirmation of axillary nerve course (D) is generally understood anatomically (5-7 cm distal to acromion) and protected surgically; CT is not typically used to map nerve courses for routine PHF planning.
Evaluation of pre-existing shoulder arthritis (E) can be seen on radiographs and CT, but for an acute fracture, the primary focus of the CT is the fracture itself and its implications for fixation, rather than pre-existing arthritis unless it's a major factor influencing arthroplasty decision-making.
Question 9
A 65-year-old female undergoes ORIF with a locking plate for a three-part proximal humerus fracture. Postoperatively, she is placed in a sling. According to the rehabilitation protocol described, which of the following activities is MOST appropriate to initiate during Phase I (Immobilization and Early Passive Motion), typically within the first week, assuming fracture stability?
Explanation
Correct Answer: C
The text describes Phase I (Immobilization and Early Passive Motion) goals as 'Protect surgical repair, minimize pain and swelling, initiate early passive range of motion (PROM) to prevent stiffness, maintain distal extremity function.' Under 'Exercises,' it specifically lists 'Pendulum Exercises: Gentle, gravity-assisted swings of the arm (flexion/extension, internal/external rotation, circumduction). Initiated early, often within the first week, based on pain and fracture stability.'
Active shoulder abduction against gravity (A) is an active movement and is explicitly contraindicated in Phase I, which states 'No active shoulder movement.'
Resistive isometric external rotation (B) is a strengthening exercise, typically introduced in Phase II or III, not Phase I.
Active-assisted shoulder flexion using a pulley system (D) is an AAROM exercise, typically introduced in Phase II, not Phase I.
Weight-bearing on the affected arm (E) is a strict precaution throughout early phases and is explicitly stated as 'No weight-bearing on the affected arm' in Phase I precautions.
Question 10
A 58-year-old male undergoes ORIF of a complex proximal humerus fracture. During the deltopectoral approach, the surgeon identifies the cephalic vein. According to the described technique, what is the typical management of the cephalic vein?
Explanation
Correct Answer: C
The text states, under 'Deltopectoral Groove' dissection: 'The cephalic vein is typically retracted laterally with the deltoid, but can be ligated and divided if necessary for better exposure, particularly in revision cases or when space is limited. Care should be taken to preserve smaller venous tributaries.'
Option A is incorrect because it is not routinely ligated and divided, but rather 'if necessary.'
Option B is incorrect; it is retracted laterally with the deltoid, not medially with the pectoralis major.
Option D is incorrect; there is no mention of dissecting it free and transposing it.
Option E is incorrect; while preservation is preferred, it is often retracted, and can be ligated if necessary, so 'always preserved without retraction' is too absolute.
Question 11
A 70-year-old female with a displaced three-part proximal humerus fracture is undergoing ORIF with a locking plate. The surgeon is about to insert screws into the humeral head. Based on the biomechanical principles and surgical technique described, which type of screw is considered CRUCIAL for resisting varus collapse and providing critical support for internal fixation?
Explanation
Correct Answer: C
The text explicitly highlights the importance of the medial calcar: 'Medial Calcar: This dense trabecular bone region acts as a crucial weight-bearing structure, resisting varus collapse and providing critical support for internal fixation. Loss of medial calcar support significantly increases the risk of screw cutout and construct failure.' Furthermore, under 'Head Fixation,' it states: 'Calcar Screws: Crucial for medial column support. At least one, ideally two, calcar screws should be directed inferiorly and medially towards the calcar region to resist varus collapse.'
Cortical screws in the greater tuberosity (A) are important for tuberosity fixation and rotator cuff integrity but do not primarily resist varus collapse of the humeral head.
Lag screws across the anatomical neck (B) are not specifically mentioned as crucial for resisting varus collapse in the context of locking plate fixation for PHFs; locking screws provide angular stability.
Screws placed through the bicipital groove (D) are not a standard or recommended practice for head fixation and could damage the biceps tendon.
Screws directed superiorly into the acromion (E) would be an extra-articular fixation and is not part of standard proximal humerus plating for head fixation.
Question 12
A 68-year-old male presents with a 5-year history of progressive left hip pain, significantly limiting his ability to walk more than 100 meters and perform activities of daily living. He has undergone multiple courses of NSAIDs, physical therapy, and a single intra-articular corticosteroid injection 18 months prior, which provided only 3 months of partial relief. Radiographs confirm Kellgren-Lawrence Grade IV osteoarthritis. He is medically optimized with controlled hypertension, hyperlipidemia, and diet-controlled Type 2 Diabetes Mellitus. He is motivated for surgical intervention.
Based on this patient's presentation, what is the most compelling indication for proceeding with Total Hip Arthroplasty (THA)?

Explanation
Correct Answer: C
The most compelling indication for Total Hip Arthroplasty (THA) in this patient is the failure of comprehensive non-operative management to provide sustained symptomatic relief and functional improvement. The case explicitly states the patient had a 5-year history of debilitating pain, failed NSAIDs, physical therapy, and only transient relief from a corticosteroid injection. This, combined with severe functional limitations (walking <100m, difficulty with ADLs) and radiographic evidence of Kellgren-Lawrence Grade IV osteoarthritis, are the primary drivers for surgical intervention. While age (A), BMI (B), controlled comorbidities (D), and patient motivation (E) are all important factors in surgical decision-making, they are not the primary indications for the procedure itself. Age is a factor for implant choice and overall health, BMI is a risk factor, controlled comorbidities are necessary for medical fitness, and patient desire is crucial for compliance and realistic expectations, but none of these alone indicate the need for surgery without the underlying pathology and failure of conservative care.
Question 13
During the clinical examination, the patient's left hip demonstrated significantly restricted and painful range of motion (ROM). Key findings included flexion to 80° (normal >120°), extension to 0° (normal 15-20°) with a fixed flexion deformity of 10°, and internal rotation of 5° (normal 30-40°) with severe pain.
This specific pattern of ROM restriction, particularly the loss of internal rotation and fixed flexion deformity, is most characteristic of which of the following hip pathologies?
Explanation
Correct Answer: C
The described pattern of range of motion (ROM) restriction, particularly the significant loss of internal rotation and the presence of a fixed flexion deformity, is a classic presentation of advanced primary osteoarthritis of the hip. Osteoarthritis typically affects the anterior and superior aspects of the joint first, leading to a progressive loss of internal rotation and extension. The fixed flexion deformity is a common compensatory mechanism to reduce pain. While other conditions can cause hip pain and ROM restriction, early avascular necrosis (A) might present with pain and restricted IR but typically without the extensive fixed flexion deformity or global ROM loss seen in advanced OA. Inflammatory arthropathy (B) often presents with more symmetric polyarticular involvement and different pain characteristics (worse with rest). A labral tear (D) typically causes mechanical symptoms like clicking or catching and pain with specific movements, but not usually the global, severe ROM restriction and fixed deformity of advanced OA. Greater trochanteric bursitis (E) causes lateral hip pain and tenderness, with ROM typically preserved, especially internal rotation.
Question 14
Anteroposterior (AP) pelvis radiographs of the patient's left hip revealed severe tricompartmental joint space narrowing, subchondral sclerosis, extensive osteophyte formation along the femoral head-neck junction and acetabular rim, and subchondral cyst formation in both the femoral head and acetabulum. There was also evidence of mild acetabular retroversion indicated by a positive cross-over sign, and superolateral migration of the femoral head.
According to the Kellgren-Lawrence classification, these findings are consistent with which grade of osteoarthritis?
Explanation
Correct Answer: D
The Kellgren-Lawrence classification system is a widely used radiographic grading scale for osteoarthritis. The described findings of 'severe tricompartmental joint space narrowing, subchondral sclerosis, extensive osteophyte formation, subchondral cyst formation, and definite deformity of bone ends' are the hallmarks of Grade IV osteoarthritis. Grade I involves doubtful narrowing and possible osteophytes. Grade II shows definite osteophytes and possible narrowing. Grade III includes moderate osteophytes, definite joint space narrowing, and some sclerosis. Grade V is not a standard Kellgren-Lawrence grade; the highest is Grade IV, which represents severe disease. The case explicitly states the Kellgren-Lawrence grade for the left hip was IV, reinforcing this answer.
Question 15
Digital templating was performed using a calibrated AP pelvis radiograph. The goals for acetabular component placement included maximizing coverage (80-90%), achieving appropriate inclination (40-45°) and anteversion (15-20°). For the femoral component, templating aimed to restore femoral offset, leg length, and potential for restoration of femoral anteversion. The lesser trochanter was used as a key landmark for stem depth and leg length adjustments.
Which of the following biomechanical parameters, when optimally restored during THA, is most critical for improving abductor muscle efficiency and minimizing the risk of a post-operative Trendelenburg gait?
Explanation
Correct Answer: B
Restoration of femoral offset is most critical for optimizing abductor muscle efficiency and minimizing the risk of a post-operative Trendelenburg gait. Femoral offset refers to the horizontal distance from the center of rotation of the femoral head to the long axis of the femur. Increasing the offset lengthens the abductor lever arm, allowing the gluteus medius and minimus muscles to generate more torque with less force, thereby improving their efficiency and reducing the likelihood of abductor insufficiency (Trendelenburg gait). While acetabular inclination (A) and anteversion (C) are crucial for stability and wear, and femoral stem anteversion (E) is important for preventing impingement and dislocation, they do not directly impact the abductor lever arm as significantly as femoral offset. Femoral head diameter (D) primarily influences range of motion and jump distance for stability, but not directly abductor mechanics.
Question 16
The patient's clinical presentation included insidious onset of progressive groin and lateral thigh pain, mechanical catching, and morning stiffness lasting 45 minutes. Radiographs showed severe tricompartmental joint space narrowing, subchondral sclerosis, extensive osteophytes, and subchondral cysts. Inflammatory markers (ESR, CRP) were normal.
Considering these findings, which of the following conditions is least likely to be the primary diagnosis?
Explanation
Correct Answer: C
Rheumatoid arthritis (RA) is least likely to be the primary diagnosis. The patient's presentation with mechanical pain, morning stiffness lasting 45 minutes (typical for OA, RA is usually >1 hour), and radiographic findings of osteophytes, subchondral sclerosis, and cysts are classic for osteoarthritis. RA typically presents with inflammatory pain (worse with rest), symmetric polyarthritis, and radiographic features of concentric joint space narrowing, erosions, and juxta-articular osteopenia, with an absence of osteophytes. Furthermore, inflammatory markers (ESR, CRP) would typically be elevated in active RA, which were normal in this patient. Primary osteoarthritis (A) is the most likely diagnosis. AVN (B) can cause similar pain but has distinct radiographic features (crescent sign, patchy sclerosis/lucency) and MRI is diagnostic. Post-traumatic OA (D) and DDH leading to secondary OA (E) are forms of osteoarthritis and would present with similar clinical and radiographic features to primary OA, making them plausible differential diagnoses for the type of OA, but not fundamentally different conditions like RA.
Question 17
Pre-operative planning included assessing the femoral canal morphology. The patient's radiographs suggested a Dorr Type B femur, characterized by good metaphyseal-diaphyseal flare and adequate cortical thickness.
This specific femoral morphology (Dorr Type B) is generally considered most favorable for which type of femoral stem fixation in primary Total Hip Arthroplasty?
Explanation
Correct Answer: C
A Dorr Type B femur, characterized by good metaphyseal-diaphyseal flare and adequate cortical thickness, provides excellent bone stock for achieving primary press-fit stability. This morphology is considered ideal for a fully uncemented (cementless) femoral stem. Uncemented stems rely on this initial mechanical stability (press-fit) and subsequent biological fixation through bone ingrowth into a porous coating. Dorr Type A femurs (champagne flute, thick cortex, narrow canal) are at higher risk of fracture with uncemented stems and may sometimes benefit from cemented stems. Dorr Type C femurs (stovepipe, thin cortex, wide canal) often lack sufficient metaphyseal bone for press-fit and are typically better suited for cemented stems or specific uncemented designs that achieve diaphyseal fixation. Cemented stems (A, B) are generally preferred in osteoporotic bone or in cases where primary press-fit cannot be reliably achieved. Resurfacing arthroplasty (D) is a bone-preserving option for younger, active patients with good bone quality, but not directly related to the Dorr classification for stem fixation. Custom-made stems (E) are reserved for severe deformities or bone loss, not typically a standard Dorr Type B femur.
Question 18
The planned surgical approach for this patient's uncemented Total Hip Arthroplasty was a posterior (Kocher-Langenbeck) approach. During the procedure, the short external rotators (piriformis, gemelli, obturator internus) were identified, tenotomized close to their femoral insertion, and tagged with non-absorbable sutures. The posterior hip capsule was also incised and tagged.
At the time of closure, meticulous repair of which of the following structures is most crucial for enhancing post-operative stability and significantly reducing the risk of posterior dislocation, a known complication of this approach?
Explanation
Correct Answer: D
In a posterior approach to the hip, the short external rotators (piriformis, gemelli, obturator internus) and the posterior capsule are incised to gain access to the hip joint. Meticulous repair of these structures at the time of closure is paramount for enhancing post-operative stability and significantly reducing the risk of posterior dislocation. This repair helps to restore the natural soft tissue restraints against posterior dislocation. The gluteus medius (A) is typically split or retracted, but its primary role is abduction, and its repair is not as directly linked to posterior stability as the rotators and capsule. The iliopsoas (B) and rectus femoris (C) are anterior structures and are not typically violated in a posterior approach. The vastus lateralis fascia (E) is part of the quadriceps mechanism and not directly involved in hip joint stability in this context.
Question 19
During the femoral preparation phase of a primary THA, the surgeon is broaching the femoral canal. The patient's femur is noted to have a narrow canal with very thick cortical bone, consistent with a Dorr Type A morphology. The surgeon is attempting to achieve a stable metaphyseal press-fit for an uncemented stem.
In this scenario, which intraoperative complication is the surgeon at the highest risk for during forceful broaching and subsequent stem impaction?
Explanation
Correct Answer: C
A Dorr Type A femur, characterized by a narrow canal and very thick cortical bone (often described as a 'champagne flute' shape), is particularly susceptible to intraoperative femoral fracture during broaching or stem impaction, especially when attempting to achieve a press-fit with an uncemented stem. The rigid, thick cortex offers little elasticity, and forceful impaction can lead to a crack or fracture. Sciatic nerve injury (A) is a risk with excessive leg lengthening or aggressive posterior retraction, but not directly from broaching in a Dorr A femur. Acetabular medial wall perforation (B) and external iliac artery injury (D) are risks associated with acetabular reaming or screw placement, not femoral preparation. Excessive leg lengthening (E) is a concern during trial reduction and final component selection, not typically a direct result of broaching itself, though an undersized stem in a large canal could contribute to instability requiring lengthening.
Question 20
Following an uncemented Total Hip Arthroplasty performed via a posterior approach, the patient is initiated on a post-operative rehabilitation protocol. This protocol includes immediate weight-bearing as tolerated with an assistive device and specific hip precautions.
Which of the following activities should the patient be most strictly instructed to avoid in the immediate post-operative period to minimize the risk of dislocation?
Explanation
Correct Answer: D
For a patient who has undergone THA via a posterior approach, the combination of hip flexion beyond 90 degrees, adduction past midline, and internal rotation is the classic position that places the hip at highest risk for posterior dislocation. Therefore, patients are strictly instructed to avoid this combination of movements in the immediate post-operative period. Immediate weight-bearing as tolerated (A) is standard for uncemented components. Gentle hip abduction exercises (B) are encouraged to strengthen abductors. Sleeping on the operative side with a pillow between the legs (C) is often recommended to maintain abduction and prevent adduction. Stationary cycling (E) is a low-impact exercise that can be introduced in early rehabilitation, provided the seat height is adjusted to prevent excessive hip flexion.
Question 21
The patient's X-rays showed classic features of severe osteoarthritis, making advanced imaging unnecessary. However, the case notes that a CT scan would be indicated for complex acetabular or femoral deformity, previous trauma, significant bone loss, or for detailed surgical planning for revision arthroplasty.
If the patient's symptoms were highly suggestive of a hip pathology but initial X-rays were equivocal or normal, an MRI scan would be most indicated to rule out which of the following conditions?
Explanation
Correct Answer: C
An MRI scan is considered the diagnostic gold standard for avascular necrosis (AVN) of the femoral head, especially in early stages where X-ray findings may be equivocal or normal. MRI can detect marrow edema, serpentine low signal lines, and characteristic T1/T2 signal changes indicative of AVN before subchondral collapse or other radiographic signs become apparent. Severe acetabular retroversion (A) and significant femoral anteversion (B) are bony deformities best assessed by CT scan, which provides superior bony detail and 3D reconstruction. Extensive heterotopic ossification (D) is typically visible on X-rays, and CT can provide more detail, but MRI is not the primary modality for its diagnosis. Periprosthetic joint infection (E) is diagnosed based on clinical signs, lab markers (ESR, CRP, leukocyte count), aspiration, and sometimes nuclear imaging, with MRI having limited specific utility for PJI diagnosis due to artifact from metal implants.
Question 22
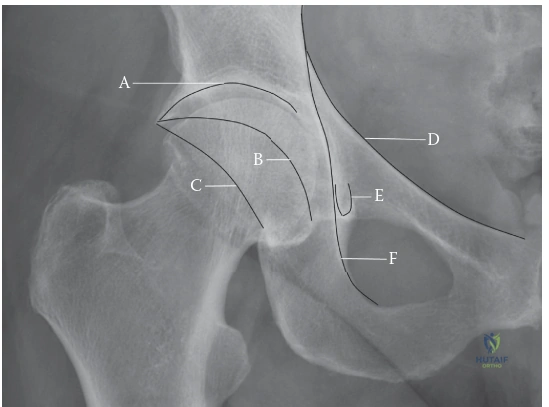
A 45-year-old male presents after a high-energy motor vehicle collision. Imaging reveals a complex acetabular fracture involving the anterior superior iliac spine (ASIS), extending through the iliopectineal line, and involving the superior pubic ramus. Based on the Judet and Letournel classification system and the provided anatomical understanding:

Explanation
Correct Answer: C
The correct answer is the Anterior column. The case explicitly states that the fracture involves the anterior superior iliac spine (ASIS), extends through the iliopectineal line, and involves the superior pubic ramus. According to the 'Surgical Anatomy & Biomechanics' section, the anterior column is defined as extending from the ASIS through the iliopectineal line, crossing the anterior acetabulum to the superior pubic ramus. It also includes the anterior half of the acetabular roof. This description perfectly matches the fracture pattern described in the vignette. The posterior column, posterior wall, transverse, and both column fractures involve different anatomical structures and fracture lines as detailed in the Judet and Letournel classification.
Question 23
A 35-year-old male sustains a displaced posterior column acetabular fracture after a fall from height. Surgical fixation is planned via a Kocher-Langenbeck approach. During the dissection, as depicted in the image, the short external rotators are identified and potentially detached. Which of the following neurovascular structures is most critically at risk and typically protected by careful medial retraction during this approach?
Explanation
Correct Answer: C
The correct answer is the Sciatic nerve. The 'Detailed Surgical Approach / Technique' section, specifically under the Kocher-Langenbeck Approach, highlights the sciatic nerve as a 'CRITICAL' structure. It states that the sciatic nerve lies deep to the piriformis and obturator internus, medial to the lesser sciatic notch, and 'It must be carefully identified, protected, and retracted (usually medially).' Traction on the limb should also be monitored to prevent iatrogenic nerve stretch. The femoral nerve and external iliac vein are anterior structures, primarily at risk during anterior approaches. The superior gluteal artery is vulnerable during extended iliofemoral and Kocher-Langenbeck approaches, particularly near the greater sciatic notch, but the sciatic nerve is the most prominent and consistently at risk nerve during posterior approaches. The obturator nerve is located more medially within the pelvis, deep to the quadrilateral plate.
Question 24
A 40-year-old female presents with a displaced anterior column acetabular fracture requiring an ilioinguinal approach. During the dissection for the medial window, as illustrated in the image, the surgeon is working between the external iliac artery/vein laterally and the rectus abdominis/pubic symphysis medially. Which anatomical variant must be carefully identified and potentially ligated to prevent significant hemorrhage in this region?

Explanation
Correct Answer: D
The correct answer is the Corona Mortis. The 'Surgical Anatomy & Biomechanics' section explicitly mentions the 'Corona Mortis (Aberrant Obturator Artery)' as an anatomical variant, a vascular connection between the obturator and external iliac/inferior epigastric arteries, often crossing the superior pubic ramus. It states that 'Laceration can lead to significant hemorrhage during Stoppa or ilioinguinal approaches.' The 'Detailed Surgical Approach / Technique' section, under the Ilioinguinal Approach, further emphasizes this, stating, 'CRITICAL: Identify and ligate the "Corona Mortis"... if present, to prevent significant hemorrhage.' While the obturator artery is involved in this anastomosis, the specific term for the variant connection at risk in this region is the Corona Mortis. The superior gluteal artery is posterior, and the femoral and inferior epigastric arteries are typically identified but the specific variant at high risk of unexpected hemorrhage in the medial window is the Corona Mortis.
Question 25
A 28-year-old male presents with an acetabular fracture after a motorcycle accident. CT scan reveals a posterior wall fracture involving 30% of the articular surface. There is a 3 mm articular step-off, and the hip joint is concentrically reduced and stable on examination. No intra-articular fragments are noted. Based on the provided case information and the teaching material, which of the following is the most appropriate management strategy?
Explanation
Correct Answer: C
The correct answer is Open reduction and internal fixation (ORIF). The 'Indications & Contraindications' section clearly states that a primary indication for operative management is 'Displacement: Intra-articular displacement of ≥ 2 mm (some argue for 1 mm in younger patients in the weight-bearing dome).' In this vignette, the patient has a 3 mm articular step-off, which exceeds the 2 mm threshold, making operative management indicated despite the hip being stable and the posterior wall involvement (30%) being below the 40-50% threshold for inherent instability. Non-operative management is reserved for displacements less than 2 mm. Urgent closed reduction and spica cast are not appropriate for a stable, displaced posterior wall fracture. Primary total hip arthroplasty is typically considered for elderly patients with osteoporotic, complex fractures or as a salvage procedure for PTOA. Delaying ORIF beyond 3 weeks is a relative contraindication due to callus formation, making reduction more challenging.
Question 26
A 55-year-old patient sustains a complex acetabular fracture after a fall from height. Initial plain radiographs (AP pelvis, iliac oblique, and obturator oblique views) are obtained, which help classify the fracture according to Judet and Letournel. However, the surgeon requires more detailed information for definitive diagnosis and meticulous surgical planning. According to the case, which imaging modality is considered essential for this purpose?
Explanation
Correct Answer: C
The correct answer is Thin-slice CT with 2D and 3D reconstructions. The 'Pre-Operative Planning & Patient Positioning' section, under 'Imaging Analysis,' explicitly states that 'Computed Tomography (CT) Scan: Essential for definitive diagnosis and surgical planning.' It further elaborates that 'Thin-slice CT with 2D and 3D Reconstructions provides detailed visualization of fracture lines, comminution, articular step-off, intra-articular fragments, quadrilateral surface involvement, and femoral head integrity. It is invaluable for understanding fracture morphology and choosing the appropriate surgical approach.' While plain radiographs are initial and help classify, they lack the detail needed for surgical planning. MRI is rarely indicated acutely unless specific soft tissue or chondral injuries are suspected. Ultrasound and bone scintigraphy have no primary role in acute acetabular fracture diagnosis and surgical planning.
Question 27
A 42-year-old male undergoes successful open reduction and internal fixation of a both column acetabular fracture via an extended iliofemoral approach. He has no history of head injury. Given the extensive nature of the surgical approach and the patient's demographics, which prophylactic measure should be initiated post-operatively to minimize the risk of a common complication associated with this type of surgery?
Explanation
Correct Answer: D
The correct answer is NSAIDs or radiation therapy. The 'Complications & Management' section lists Heterotopic Ossification (HO) as a common complication with an incidence of 10-50% (radiographically), noting it is 'More common with extended approaches, head injury, male sex, concomitant elbow injury.' The management strategy for HO prophylaxis is 'NSAIDs (e.g., Indomethacin) for 3-6 weeks post-op, or single-dose post-op radiation therapy (700-800 cGy).' Long-term oral antibiotics are not a standard prophylactic measure for HO. Early full weight-bearing is generally contraindicated in the immediate post-operative period for acetabular fractures. CPM may be used for ROM but is not specifically for HO prophylaxis. Urgent hardware removal is a treatment for hardware-related complications, not a prophylactic measure.
Question 28
A 30-year-old patient underwent open reduction and internal fixation for a transverse acetabular fracture 5 years ago. Despite initial good recovery and radiographic evidence of fracture union, he now presents with progressive hip pain, stiffness, and radiographic findings of joint space narrowing, subchondral sclerosis, and osteophytes. Based on the long-term outcomes discussed in the case, what is the most likely underlying cause of this patient's current symptoms and radiographic findings?
Explanation
Correct Answer: D
The correct answer is Post-traumatic osteoarthritis (PTOA). The 'Complications & Management' section identifies PTOA as a very common long-term complication (20-80% incidence), described as 'Progressive degeneration of the articular cartilage, leading to pain, stiffness, and functional limitation. Directly correlated with quality of reduction.' The symptoms of progressive hip pain, stiffness, and radiographic findings of joint space narrowing, subchondral sclerosis, and osteophytes are classic signs of osteoarthritis. While AVN, hardware failure, HO, and nonunion are possible complications, the clinical presentation and radiographic findings described are most consistent with PTOA, especially given the 5-year post-operative timeframe and initial fracture union.
Question 29
A 25-year-old patient underwent open reduction and internal fixation of a posterior column acetabular fracture. The surgeon emphasizes strict adherence to the post-operative protocol to protect the fixation and promote healing. In the immediate post-operative phase (weeks 0-6), which of the following weight-bearing and range of motion guidelines is generally recommended for this patient?
Explanation
Correct Answer: C
The correct answer is Non-weight bearing (NWB) on the operative extremity. The 'Post-Operative Rehabilitation Protocols' section, under 'Phase Immediate Post-Operative (Weeks 0-6),' clearly states for weight-bearing: 'Non-Weight Bearing (NWB) on the operative extremity. Ambulation with crutches or a walker. Foot-flat weight-bearing or toe-touch weight-bearing (TTWB) may be allowed by some surgeons for stability, but NWB is generally safer.' Regarding range of motion, it advises 'Active-Assisted ROM (AAROM) and Gentle Passive ROM (PROM): Within pain limits. Avoid extremes of motion, especially positions that stress the fracture fragments (e.g., deep flexion, adduction, internal rotation for posterior fractures).' Therefore, full or partial weight-bearing and unrestricted or deep hip flexion are not appropriate in this immediate phase.
Question 30
The teaching case emphasizes that the primary goal of acetabular fracture treatment is to restore the anatomical congruity of the hip joint to minimize long-term complications. According to the summary of key literature and guidelines, which factor is most strongly correlated with superior long-term functional outcomes and reduced rates of post-traumatic osteoarthritis after acetabular fracture fixation?
Explanation
Correct Answer: D
The correct answer is Anatomical reduction with <1-2 mm step-off/gap. The 'Summary of Key Literature / Guidelines' section explicitly states: 'Long-term follow-up studies consistently demonstrate a strong correlation between anatomical reduction (< 1-2 mm step-off/gap) and superior functional outcomes, reduced rates of PTOA, and less need for subsequent THA.' While other factors like DVT prophylaxis are important for preventing complications, and surgical approach is critical for achieving reduction, the quality of the articular reduction itself is the most direct and consistently cited predictor of long-term joint health and function. Early full weight-bearing is not recommended and patient age is a risk factor for certain complications, but not the primary determinant of long-term outcome quality after fixation.
Question 31
An 82-year-old female with severe osteoporosis sustains a highly comminuted both column acetabular fracture after a low-energy fall, as shown in the image. She is otherwise medically stable and ambulates independently with a cane. Considering the patient's age, bone quality, and fracture pattern, which of the following treatment strategies might be considered as a primary option, as discussed in the case, despite the general preference for open reduction and internal fixation (ORIF) in younger patients?
Explanation
Correct Answer: C
The correct answer is Primary total hip arthroplasty (THA). The 'Summary of Key Literature / Guidelines' section, under 'Management in the Elderly,' states: 'Acetabular fractures in osteoporotic elderly patients present unique challenges. While anatomical reduction and fixation are still desirable, bone quality can make fixation tenuous. Debates continue regarding the role of primary total hip arthroplasty (THA) in severely comminuted or multi-column fractures in this population, as it may offer earlier mobilization and potentially better functional outcomes in selected cases, despite being a more extensive procedure.' Given the patient's advanced age, severe osteoporosis, and a highly comminuted both column fracture, primary THA is a recognized alternative to ORIF, which might be challenging to achieve stable fixation in poor bone quality. Non-operative management with prolonged bed rest is generally associated with high morbidity in the elderly. External fixation is typically for pelvic ring injuries or temporary stabilization, not definitive acetabular fixation. Arthrodesis is rarely performed and generally offers poorer quality of life.
Question 32
A 32-year-old male presents to the emergency department after a high-speed motor vehicle collision. He sustained a dashboard injury, resulting in a posterior hip dislocation. On examination, his hip is flexed, adducted, and internally rotated. Distal pulses are intact, and he has a partial foot drop. The most critical factor influencing the long-term outcome, specifically regarding avascular necrosis (AVN) of the femoral head, is:
Explanation
Correct Answer: C
The case explicitly states, "Prolonged dislocation time directly correlates with increased rates of critical complications, particularly avascular necrosis (AVN) of the femoral head and sciatic nerve injury." It further emphasizes, "The incidence is directly proportional to the time to reduction and the energy of the injury." Numerous studies consistently demonstrate a direct inverse relationship between prompt reduction (ideally within 6 hours, optimally within 1-2 hours) and the incidence of AVN. Delays beyond 12-24 hours dramatically increase AVN rates to over 40-50%. While other factors listed can influence overall outcome, the time to reduction is the single most critical determinant for preventing AVN.
Question 33
A 48-year-old male undergoes open reduction for a complex posterior hip dislocation with an incarcerated osteochondral fragment. During the posterior approach, the surgeon is meticulously identifying and protecting structures to minimize the risk of iatrogenic injury and preserve femoral head vascularity. Which of the following arteries is considered the primary blood supply to the adult femoral head and is most vulnerable in this injury?
Explanation
Correct Answer: C
The case highlights the "Medial Circumflex Femoral Artery (MCFA): The primary blood supply to the femoral head in adults, ascending posteriorly and superiorly along the posterior aspect of the femoral neck, deep to the quadratus femoris and obturator externus. Damage to this artery, particularly its retinacular branches, is the main etiology of femoral head AVN following dislocation." The obturator artery via the ligamentum teres provides minimal blood supply in adults. The superior and inferior gluteal arteries supply the gluteal muscles and surrounding structures, while the lateral circumflex femoral artery primarily supplies the greater trochanter and vastus lateralis, not the femoral head itself.
Question 34
A 28-year-old male presents with a posterior hip dislocation after a fall from height. Initial AP and lateral radiographs confirm the dislocation. However, the lateral view also raises suspicion for an ipsilateral femoral neck fracture. Given this finding, which of the following is the most appropriate next step in management?
Explanation
Correct Answer: C
The case explicitly states, "Absolute contraindications to attempting closed reduction are rare but include: Femoral neck fracture: This is a crucial contraindication. Attempting closed reduction in the presence of an ipsilateral femoral neck fracture can convert a non-displaced fracture into a displaced one, or cause further displacement, increasing the risk of AVN or nonunion. This requires careful pre-reduction imaging." Therefore, before any reduction attempt, a CT scan is essential to definitively rule out or characterize a femoral neck fracture, which would necessitate operative management.
Question 35
Following a successful closed reduction of a posterior hip dislocation in a 40-year-old male, a palpable clunk was noted, and the hip appears stable on clinical examination. Post-reduction AP and lateral X-rays show a seemingly concentric reduction. What is the most appropriate next diagnostic step to ensure optimal long-term outcomes?
Explanation
Correct Answer: C
The case emphasizes that "A CT scan of the pelvis and hip is generally recommended after successful closed reduction to: Confirm concentric reduction. Identify incarcerated osteochondral fragments or soft tissue within the joint. Precisely characterize associated acetabular or femoral head fractures (size, displacement, articular involvement). Assess for occult femoral neck or intertrochanteric fractures missed on plain radiographs." While plain X-rays may appear concentric, a CT scan is crucial to detect subtle intra-articular fragments or occult fractures that could lead to post-traumatic arthritis or instability if not addressed. MRI is more sensitive for AVN, but AVN is a later complication, and the immediate priority after reduction is to confirm concentricity and rule out incarcerated fragments/fractures.
Question 36
A 25-year-old athlete presents with an acute posterior hip dislocation. The emergency physician is preparing for closed reduction. Which of the following principles is paramount for a safe and successful reduction, regardless of the specific maneuver chosen?
Explanation
Correct Answer: C
The case clearly outlines the key principles for emergency closed reduction: "Regardless of the specific maneuver, key principles apply: 1. Adequate Muscle Relaxation: Absolutely paramount. Without it, forceful reduction attempts can lead to iatrogenic fractures or cartilage damage. 2. Axial Traction: Apply steady, sustained axial traction in line with the femoral shaft, aiming to distract the femoral head from the acetabulum." Forceful maneuvers without adequate relaxation increase the risk of iatrogenic injury. Hip flexion (often 60-90 degrees) is typically used to relax the powerful hip flexors and iliofemoral ligament, making option E incorrect. Immediate post-reduction weight-bearing is not recommended, especially for complex dislocations.
Question 37
A 55-year-old male requires open reduction for an irreducible posterior hip dislocation with a large posterior acetabular wall fracture. The surgeon opts for the Kocher-Langenbeck approach. During the deep dissection, as depicted in the illustration below, which critical neurovascular structure must be carefully identified and protected, typically by retracting it medially?
Explanation
Correct Answer: C
The case describes the Kocher-Langenbeck approach and states, "The sciatic nerve lies deep to the piriformis and superficial to the quadratus femoris. It is highly vulnerable. Careful identification and protection are paramount. Identify the nerve early and retract it gently, typically medially." The illustration shows the posterior aspect of the hip, where the sciatic nerve is located. The femoral and obturator nerves are anterior/medial, and the superior gluteal nerve is more superior. While the medial circumflex femoral artery is critical for femoral head vascularity, the question specifically asks about a neurovascular structure to be identified and retracted during the deep dissection of the posterior approach, making the sciatic nerve the most prominent and vulnerable neural structure in this field.
Question 38
A 38-year-old male sustains a posterior hip dislocation. After successful closed reduction, he is noted to have a new-onset foot drop and weakness in ankle dorsiflexion and eversion. Sensation is diminished over the dorsum of the foot. This neurological deficit most likely involves which division of the sciatic nerve, and what is its typical prognosis?
Explanation
Correct Answer: C
The case states, "Sciatic Nerve Injury: The peroneal division is more commonly affected due to its relative fixation and more superficial course. Most sciatic nerve palsies following hip dislocation are neurapraxias and resolve spontaneously within 6-12 months." Foot drop, weakness in ankle dorsiflexion and eversion, and sensory loss over the dorsum of the foot are classic symptoms of common peroneal nerve injury. Most of these injuries are neurapraxias (stretch injuries) and have a good prognosis for spontaneous recovery over several months.
Question 39
A 60-year-old male with a history of traumatic brain injury (TBI) undergoes open reduction and internal fixation of a complex posterior hip dislocation with an acetabular fracture. Given his risk factors, which of the following prophylactic measures is most effective in preventing heterotopic ossification (HO)?
Explanation
Correct Answer: C
The case states, "Heterotopic Ossification (HO): ...Patients undergoing open reduction, especially those with associated head injuries, are at higher risk for HO. Prophylaxis with non-steroidal anti-inflammatory drugs (NSAIDs) such as indomethacin (e.g., 25 mg TID for 3-6 weeks) or a single dose of post-operative radiation (700-800 cGy) has been shown to be effective in preventing symptomatic HO." A history of TBI is a well-known risk factor for HO. LMWH is for DVT prophylaxis, not HO. Aggressive ROM or strict immobilization are not primary HO prophylaxis methods and can be detrimental.
Question 40
A 42-year-old male presents with a posterior hip dislocation and an associated femoral head fracture, classified as Pipkin Type II. After initial closed reduction, a post-reduction CT scan confirms the femoral head fragment is displaced and involves the weight-bearing superior aspect of the femoral head. What is the most appropriate definitive management for this injury?
Explanation
Correct Answer: D
The case outlines the management of Pipkin fractures: "Pipkin Type I (below fovea) and Type II (above fovea): Require anatomical reduction and stable internal fixation (typically headless compression screws). Excision of small, non-weight-bearing fragments may be considered." Given that the fragment is displaced and involves the weight-bearing superior aspect of the femoral head, anatomical reduction and stable internal fixation are crucial to restore articular congruity and prevent post-traumatic arthritis. Excision is typically reserved for very small, non-weight-bearing fragments. THA is generally reserved for end-stage arthritis or advanced AVN, not as an immediate treatment for an acute Pipkin Type II fracture in a 42-year-old.
Question 41
A 30-year-old male underwent open reduction and internal fixation of a posterior hip dislocation with an associated posterior acetabular wall fracture. He is now 3 days post-operative. Which of the following is the most appropriate initial weight-bearing and range of motion protocol for this patient?
Explanation
Correct Answer: C
The case details post-operative rehabilitation: "Open Reduction / Associated Fractures (e.g., posterior wall): Strict non-weight-bearing (NWB) for 6-12 weeks, depending on fracture stability, hardware, and surgeon preference. This protects the healing capsule, repaired soft tissues, and any internal fixation. Range of Motion (ROM): Gentle, pain-free ROM within protective limits. Avoid the 'dislocating position' (flexion > 90°, adduction, internal rotation)." Full or partial weight-bearing would jeopardize the healing fracture and fixation. Unrestricted ROM or full flexion/internal rotation would risk re-dislocation or damage to the repair. Therefore, strict NWB with protected ROM is the safest initial approach.
Question 42
Which artery is now recognized as providing the predominant blood supply to the humeral head, contradicting historical anatomical teaching?
Explanation
Question 43
During a direct anterior approach for a total hip arthroplasty, the surgeon dissects the superficial interval between the sartorius and the tensor fasciae latae. Which nerve is at greatest risk of iatrogenic injury during this phase of the dissection?
Explanation
Question 44
An orthopedic surgeon is performing an ilioinguinal approach for an anterior column acetabular fracture. During dissection over the superior pubic ramus, brisk arterial bleeding is encountered. This is most likely due to an anastomosis between which two vascular systems?
Explanation
Question 45
A 78-year-old female undergoes a reverse total shoulder arthroplasty for a complex 4-part proximal humerus fracture. Healing of the greater tuberosity to the proximal humerus shaft and prosthesis is most highly associated with improved outcomes in which of the following postoperative clinical parameters?
Explanation
Question 46
Radiographic evaluation of an acetabular fracture reveals disruption of the iliopectineal line, the ilioischial line, and an inferior fracture line splitting the obturator ring. However, a portion of the articular surface remains attached to the axial skeleton via an intact posterior ilium. This fracture is best classified as:
Explanation
Question 47
A 45-year-old active male underwent total hip arthroplasty with a ceramic-on-ceramic bearing surface two years ago. He presents complaining of an audible squeaking sound from his hip when walking. What component malpositioning is most commonly associated with this phenomenon?
Explanation
Question 48
During a hemiarthroplasty for a comminuted proximal humerus fracture, proper restoration of humeral head height is crucial. Placing the prosthesis too high (proud) relative to the greater tuberosity most commonly results in which of the following complications?
Explanation
Question 49
A 28-year-old male sustains an isolated posterior wall acetabular fracture after a motor vehicle collision. The hip joint is congruously reduced on static radiographs. Which of the following is the most definitive indication for open reduction and internal fixation of this fracture?
Explanation
Question 50
A 68-year-old female is evaluated for a total hip arthroplasty. Standing and sitting lateral radiographs reveal a stiff lumbar spine with less than 10 degrees of pelvic tilt change between positions. To minimize the risk of posterior dislocation during sitting, how should the acetabular component be positioned?
Explanation
Question 51
When utilizing an anterolateral deltoid-splitting approach for locked plating of a proximal humerus fracture, which anatomic structure dictates the absolute safe distal extent of the deltoid split?
Explanation
Question 52
A 42-year-old male undergoes open reduction and internal fixation of a transverse posterior wall acetabular fracture via a Kocher-Langenbeck approach. Postoperatively, he exhibits a foot drop and inability to extend his great toe. Which specific nerve division is most susceptible to this iatrogenic injury?
Explanation
Question 53
A 60-year-old male presents with a painful total hip arthroplasty 3 years post-surgery. Serum CRP is 15 mg/L and ESR is 45 mm/hr. Hip aspiration yields a synovial WBC count of 2,500 cells/uL with 75% neutrophils. Which of the following synovial fluid biomarkers provides the highest specificity for confirming a periprosthetic joint infection (PJI)?
Explanation
Question 54
A 55-year-old male sustains an anterior shoulder dislocation combined with a displaced greater tuberosity fracture. Prior to reduction, he has a loss of sensation over the lateral aspect of his shoulder. Injury to which of the following nerve roots primarily contributes to this specific sensory deficit?
Explanation
Question 55
During the ilioinguinal approach for an anterior column acetabular fracture, the surgeon operates through three distinct anatomical windows. Which structures define the lateral and medial borders of the middle window?
Explanation
Question 56
Which of the following represents the strongest radiographic predictor of humeral head ischemia following a displaced proximal humerus fracture, according to Hertel's criteria?
Explanation
Question 57
On an anteroposterior (AP) radiograph of the pelvis, which underlying anatomic structure is defined by the iliopectineal line?
Explanation
Question 58
During a direct anterior approach for total hip arthroplasty, the superficial inter-nervous plane is developed between muscles innervated by which two nerves?
Explanation
Question 59
A patient with an acetabular fracture has an obturator oblique radiograph demonstrating a pathognomonic "spur sign". What does this specific radiographic finding represent?
Explanation
Question 60
A 78-year-old female sustains a displaced 4-part proximal humerus fracture with significant tuberosity comminution and marked osteopenia. To maximize reliable active forward elevation, which of the following is the most appropriate surgical intervention?
Explanation
Question 61
During total hip arthroplasty, increasing the femoral component offset without altering leg length will have which of the following primary biomechanical effects?
Explanation
Question 62
When performing a Kocher-Langenbeck approach for a posterior wall acetabular fracture, maintaining the hip in which position minimizes tension on the sciatic nerve?
Explanation
Question 63
A 65-year-old male presents with groin pain 5 years after an uncomplicated metal-on-crosslinked polyethylene total hip arthroplasty. Workup reveals a sterile pseudotumor. Which design factor is most strongly associated with mechanically assisted crevice corrosion at the head-neck junction?
Explanation
Question 64
Following a proximal humerus fracture, a patient demonstrates profound weakness in shoulder abduction and decreased sensation over the lateral deltoid. Through which anatomic space does the injured nerve typically exit the axilla?
Explanation
Question 65
On the anteroposterior (AP) radiograph of the pelvis, a pure transverse fracture of the acetabulum will characteristically disrupt which of the following lines?
Explanation
Question 66
A 45-year-old male with a ceramic-on-ceramic total hip arthroplasty complains of an audible squeaking sound during hip flexion. Which of the following factors most strongly contributes to this phenomenon?
Explanation
Question 67
During open reduction and internal fixation of a proximal humerus fracture with a locked plate, which intraoperative step is most essential for preventing the most common hardware-related complication?
Explanation
Question 68
During a modified Stoppa approach for anterior column acetabular fixation, the surgeon must identify the corona mortis. At what approximate distance from the pubic symphysis is this anastomosis typically located?
Explanation
Question 69
A 70-year-old female presents with a periprosthetic femur fracture around a cemented total hip arthroplasty. Radiographs show a fracture at the stem tip, a loose femoral component, but adequate distal diaphyseal bone stock. Based on the Vancouver classification, what is the most appropriate definitive management?
Explanation
Question 70
During hemiarthroplasty for a comminuted proximal humerus fracture, restoring proper prosthesis height is critical. The superior border of the pectoralis major tendon insertion is consistently located at what distance distal to the superior aspect of the native humeral head?
Explanation
Question 71
A 32-year-old male sustains an acetabular fracture demonstrating disruption of the ilioischial line and a large posterior wall fragment, with an intact iliopectineal line. Which surgical approach provides the most optimal access for reducing and fixing this specific fracture pattern?
Explanation
Question 72
In a patient undergoing revision total hip arthroplasty for recurrent instability, a dual mobility construct is selected. Which of the following best describes its primary biomechanical advantage in preventing dislocation?
Explanation
Question 73
A 65-year-old female sustains a three-part proximal humerus fracture. The treating surgeon evaluates the radiographs to determine the risk of humeral head ischemia. According to Hertel's criteria, which of the following findings is the most reliable predictor of subsequent avascular necrosis?
Explanation
Question 74
During open reduction and internal fixation of an anterior column acetabular fracture via an ilioinguinal approach, massive hemorrhage is encountered while dissecting posterior to the superior pubic ramus. This bleeding is most likely originating from the corona mortis, an anastomosis between which two vascular structures?
Explanation
Question 75
A 55-year-old male presents with groin pain 15 years after a primary total hip arthroplasty. Radiographs demonstrate significant eccentric wear of the polyethylene liner and large osteolytic lesions around the acetabular component. Which cell type is primarily responsible for initiating the biologic cascade that leads to this osteolysis?
Explanation
Question 76
A 50-year-old male undergoes open reduction and internal fixation of a proximal humerus fracture using a proximal humeral locking plate. At his 6-month follow-up, he complains of mechanical catching and pain during shoulder abduction. Radiographs show severe joint space narrowing and glenoid erosion. What is the most common complication of this specific surgical intervention?
Explanation
Question 77
A trauma patient is undergoing radiographic evaluation for a suspected acetabular fracture. The surgeon orders standard AP pelvis and Judet views. On the iliac oblique view of the pelvis, which primary radiographic landmark is best evaluated?
Explanation
Question 78
A 78-year-old male presents after a mechanical fall with a periprosthetic femur fracture around a cemented total hip arthroplasty stem placed 10 years ago. Radiographs demonstrate a fracture at the tip of the stem. The stem is radiographically loose with subsidence, but there is adequate proximal femoral bone stock. According to the Vancouver classification, what is the most appropriate surgical management?
Explanation
Question 79
During preoperative templating for a total hip arthroplasty, the surgeon plans to use a high-offset femoral stem. Compared to a standard offset stem, what is the primary biomechanical advantage of increasing the femoral offset without changing the leg length?
Explanation
Question 80
A 45-year-old female sustains an acetabular fracture in a high-speed motor vehicle collision. An obturator oblique radiograph demonstrates the pathognomonic "spur sign." This radiographic finding is diagnostic for which type of acetabular fracture?
Explanation
Question 81
A 75-year-old female with a history of severe osteoporosis sustains a displaced four-part proximal humerus fracture. The greater and lesser tuberosities are severely comminuted. To provide the most reliable restoration of active forward elevation, which surgical option is preferred?
Explanation
Question 82
A 30-year-old male sustains a posterior wall acetabular fracture with an associated posterior hip dislocation. On physical examination, he has a profound foot drop and inability to extend his toes. Which specific portion of the sciatic nerve is most commonly injured in this scenario, and what is its anatomic position within the greater sciatic notch?
Explanation
Question 83
A 40-year-old male who underwent a total hip arthroplasty 2 years ago reports excellent range of motion and no pain, but complains of a high-pitched, audible "squeaking" sound from his hip when bending or walking. Which bearing surface combination is most classically associated with this phenomenon?
Explanation
Question 84
A surgeon is performing an open reduction and internal fixation of a highly comminuted proximal humerus fracture with medial calcar disruption. She decides to incorporate an intramedullary fibular strut allograft into her locked plating construct. What is the primary biomechanical advantage of this addition?
Explanation
Question 85
A 65-year-old female is 5 years post-primary total hip arthroplasty using a large-diameter metal head on a titanium stem. She presents with persistent groin pain. MRI reveals a large, cystic pseudotumor. Inflammatory markers are normal and joint aspiration is negative for infection. Her presentation is most likely secondary to mechanically assisted crevice corrosion occurring at which interface?
Explanation
Question 86
During open reduction and internal fixation of a posterior wall acetabular fracture via a Kocher-Langenbeck approach, the surgeon identifies a large area of marginal impaction of the articular cartilage. What is the most appropriate management of this impacted fragment?
Explanation
Question 87
A 55-year-old female undergoes a primary total hip arthroplasty via a direct anterior approach. Postoperatively, she reports a burning numbness over the anterolateral aspect of her proximal thigh. Motor function is completely intact. Which nerve was most likely stretched or injured during the superficial surgical dissection?
Explanation
Question 88
A 45-year-old male falls onto his shoulder. Radiographs demonstrate a proximal humerus fracture with the surgical neck displaced 1.5 cm and angulated 20 degrees. The greater tuberosity is fractured but displaced only 8 mm with no angulation. According to the Neer classification, how is this fracture categorized?
Explanation
None
