ABOS Part I Comprehensive Orthopaedic Review: Knee, Hip & Femur Trauma, Acetabular Reconstruction | Part 21543

Key Takeaway
This ABOS Part I Orthopaedic Review module offers 43 advanced multiple-choice questions covering complex knee dislocations, femoral neck and subtrochanteric femur fractures, and challenging acetabular revision surgery including pelvic discontinuity. It's designed to mirror board examinations, providing high-yield clinical cases for comprehensive preparation in orthopaedic trauma and reconstruction.
ABOS Part I Comprehensive Orthopaedic Review: Knee, Hip & Femur Trauma, Acetabular Reconstruction | Part 21543
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old male presents to the emergency department after a high-energy motor vehicle accident resulting in a knee dislocation. On initial assessment, the knee is grossly deformed. After successful closed reduction, palpable dorsalis pedis and posterior tibial pulses are present, but the ankle-brachial index (ABI) is measured at 0.85 on the affected limb. The patient denies paresthesias or severe pain, and the limb appears warm with good capillary refill. Which of the following is the MOST appropriate next step in management?
Explanation
Correct Answer: C
The case states that an ABI < 0.9 in an awake patient is highly suspicious for arterial injury and warrants further investigation, typically with a CT angiogram. While the limb appears viable and pulses are palpable, an ABI of 0.85 falls below this critical threshold, indicating a high probability of popliteal artery injury (e.g., intimal tear, partial occlusion) that may not yet manifest as overt ischemia. Delaying definitive diagnosis can lead to limb loss. Therefore, an immediate CT angiogram is the most appropriate next step to precisely delineate the vascular injury.
Option A is incorrect as a knee dislocation is a severe injury with high complication rates and requires admission and comprehensive workup.
Option B is insufficient. While serial neurovascular checks are important, an abnormal ABI mandates immediate advanced imaging (CTA) to rule out or characterize arterial injury, even in the absence of 'hard signs' or overt ischemia. The case explicitly states that if the ABI is normal (>0.9) and the physical examination is completely benign, serial clinical examinations may be an alternative, but not with an ABI of 0.85.
Option D, proceeding directly to surgical exploration, is generally reserved for 'hard signs' of vascular injury (e.g., absent pulses, expanding hematoma, pulsatile bleeding, limb ischemia) where time is of the essence and imaging would cause undue delay. In this scenario, with palpable pulses and a viable limb, a CTA provides crucial information to guide the vascular surgeon and plan the repair, without significant delay.
Option E is incorrect. While an MRI is essential for assessing ligamentous injuries, vascular assessment takes absolute priority in knee dislocations due to the limb-threatening nature of popliteal artery injury. MRI should be performed after vascular integrity is confirmed or addressed.
Question 2
A 35-year-old collegiate football player sustains a knee injury during a game, characterized by a direct blow to the proximal tibia with the knee flexed, resulting in a posterior knee dislocation (Schenck KD II). After successful reduction, the knee demonstrates significant posterior sag and a positive posterior drawer test. Additionally, a varus stress test at 30 degrees of flexion reveals significant laxity, and a positive dial test at 30 and 90 degrees of flexion is noted. Based on this clinical presentation, which of the following structures is MOST likely to be involved in addition to the PCL?
Explanation
Correct Answer: D
The clinical presentation describes a posterior knee dislocation (KD II), which classically involves PCL rupture, consistent with the posterior sag and positive posterior drawer test. The additional findings of significant varus laxity at 30 degrees of flexion and a positive dial test at both 30 and 90 degrees of flexion are pathognomonic for a posterolateral corner (PLC) injury. The dial test assesses external rotation of the tibia relative to the femur, with increased external rotation at 30 degrees indicating an isolated PLC injury, and increased external rotation at both 30 and 90 degrees indicating a combined PLC and PCL injury. The case emphasizes that the PLC is a complex of structures crucial for varus and external rotation stability, and its unrecognized or inadequately treated injury is a leading cause of persistent instability.
Option A (MCL) is incorrect. MCL injury would present with valgus instability, not varus instability.
Option B (ACL) is incorrect. While ACL injury can occur with KD, the specific findings of varus laxity and a positive dial test point more directly to PLC involvement in this scenario, especially with a posterior dislocation.
Option C (PMC) is incorrect. PMC injury contributes to valgus and internal rotation stability, not varus and external rotation instability.
Option E (Quadriceps tendon) is a dynamic stabilizer and its injury would typically present as an extensor mechanism disruption, not the specific instability patterns described.
Question 3
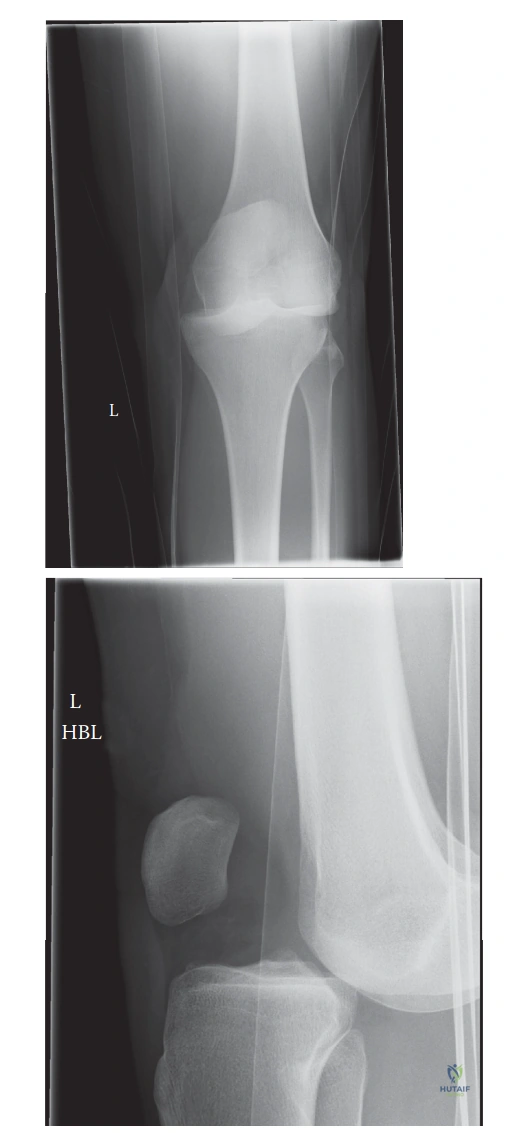
A 42-year-old obese male presents to the emergency department after a low-energy fall where his knee hyperextended. On examination, the tibia is visibly displaced anterior to the femur, and the knee is locked in extension. Distal pulses are present and strong, and neurological examination is intact. According to the Schenck classification system, what type of knee dislocation does this patient most likely have?
Explanation
Correct Answer: C
The Schenck classification system categorizes knee dislocations based on the direction of tibial displacement relative to the femur. The case explicitly states that 'KD I (Anterior): Tibia anterior to femur. Most common, often due to hyperextension.' The patient's presentation of the tibia displaced anterior to the femur following a hyperextension injury perfectly matches the description of a KD I (Anterior) dislocation.
Option A (KD II - Posterior) involves the tibia posterior to the femur, often due to a direct blow to the proximal tibia with the knee flexed.
Option B (KD III - Medial/Lateral) involves the tibia medial or lateral to the femur, resulting from varus or valgus stress.
Option D (KD IV - Rotatory) is a combination of displacements.
Option E (KD V - Irreducible) refers to a dislocation that cannot be reduced, often due to soft tissue interposition, which is not described as the primary classification type in this scenario, although it could be an associated feature if reduction fails.
Question 4
A 22-year-old male presents to the emergency department with a knee dislocation after a motorcycle accident. Initial assessment reveals a grossly deformed knee, absent dorsalis pedis and posterior tibial pulses, and a cold, pale foot. After immediate closed reduction, pulses remain absent. Which of the following is an absolute indication for immediate surgical intervention in this patient?
Explanation
Correct Answer: D
The case clearly identifies 'Vascular Compromise' as the most urgent indication for operative management. It states: 'Any signs of vascular injury (absent pulses, diminished Ankle-Brachial Index (ABI < 0.9), expanding hematoma, cold limb, pulsatile bleeding) necessitate immediate surgical exploration and repair by a vascular surgeon.' In this patient, absent pulses and a cold, pale foot indicate acute limb ischemia due to popliteal artery injury, which persists even after reduction. This is a limb-threatening emergency requiring immediate surgical exploration and repair to prevent amputation.
Option A (Gross instability after reduction) is an indication for surgical stabilization, but not necessarily immediate, limb-salvaging surgery like vascular compromise. The timing for ligamentous reconstruction can be debated (acute vs. staged).
Option B (Concomitant fibular head fracture) may require surgical fixation if it contributes to instability or joint incongruity, but it is not an immediate limb-threatening indication.
Option C (Suspected multi-ligamentous injury on MRI) is an indication for definitive surgical reconstruction, but MRI is typically performed after acute limb-threatening issues are addressed, and the timing of reconstruction can be acute or staged.
Option E (Open dislocation with minimal contamination) is an indication for immediate surgical debridement and stabilization to prevent infection, but persistent vascular compromise takes precedence as it directly threatens limb viability.
Question 5
A 30-year-old female sustains a knee dislocation during a skiing accident. She is brought to the emergency department where the knee is successfully reduced. Initial neurovascular assessment reveals palpable distal pulses and an ABI of 1.0. Neurological exam is intact. Plain radiographs confirm reduction and show no acute fractures. The patient is stable and comfortable in a splint. What is the MOST appropriate next imaging study to guide definitive surgical planning?
Explanation
Correct Answer: C
The case outlines the imaging sequence for knee dislocations. After initial reduction and confirmation of vascular integrity (normal pulses, ABI 1.0), the next critical step is to precisely delineate the extent of soft tissue injuries. The text states: 'MRI: Performed after stabilization, often within the first 7-10 days (or acutely if limb is stable and patient is going to OR for vascular repair) to precisely delineate the extent of ligamentous, meniscal, and chondral injuries. This guides definitive surgical planning.' Given the patient is stable with no vascular compromise, MRI is essential to plan the multi-ligament reconstruction.
Option A (Repeat plain radiographs) is unnecessary unless there's clinical suspicion of re-dislocation or new fracture.
Option B (Immediate CT angiogram) is not indicated here because the ABI is normal (1.0) and pulses are palpable, indicating no suspicion of arterial injury. CTA is reserved for abnormal ABI or 'hard signs' of vascular injury.
Option D (Ultrasound of the popliteal fossa) might be used to assess for hematoma or pseudoaneurysm if there was suspicion of vascular injury, but CTA is the gold standard for arterial assessment, and MRI is superior for soft tissue structures.
Option E (Bone scan) is not indicated for acute knee dislocation; it's used for conditions like stress fractures or osteomyelitis, which are not the primary concern here.
Question 6
During a multi-ligament knee reconstruction for a chronic posterior knee dislocation, the surgeon is performing a PCL reconstruction using an allograft. To ensure proper graft tensioning and prevent posterior sag, at what knee position and with what maneuver should the PCL graft be tensioned?
Explanation
Correct Answer: C
The case explicitly states the correct tensioning protocol for PCL reconstruction: 'Tensioning: Tension at 90 degrees of knee flexion with an anterior drawer applied to neutralizes the posterior sag.' This maneuver helps to restore the normal posterior stability of the knee by counteracting the tendency for posterior tibial translation, which is the primary function of the PCL.
Option A (Full extension with a valgus stress) is incorrect. This position and maneuver are not specific for PCL tensioning and would primarily stress the MCL.
Option B (30 degrees of flexion with neutral rotation) is the typical position for tensioning an ACL graft, not the PCL.
Option D (Full flexion with a posterior drawer applied) would actually increase posterior sag and potentially over-tension the graft in an incorrect position, leading to stiffness or failure.
Option E (15 degrees of flexion with a varus stress) is incorrect. This position and maneuver are not specific for PCL tensioning and would primarily stress the LCL/PLC.
Question 7
A 25-year-old male undergoes multi-ligament knee reconstruction following a high-energy knee dislocation. Post-operatively, he develops a foot drop and numbness in the first web space of his foot. Clinical examination confirms a common peroneal nerve palsy. What is the MOST appropriate initial management strategy for this complication?
Explanation
Correct Answer: B
The case describes the management of common peroneal nerve palsy: 'Management: Usually a stretch injury (neurapraxia or axonotmesis). Often managed non-operatively with observation, physical therapy, and ankle-foot orthosis (AFO) to prevent foot drop. If nerve laceration is suspected (e.g., open injury), surgical exploration and repair/grafting may be indicated.' Given that this is a post-operative complication following a closed injury (implied by reconstruction), a stretch injury is most likely. An AFO provides functional support for the foot drop, and observation allows for potential spontaneous recovery.
Option A (Immediate surgical exploration and nerve repair) is generally reserved for suspected nerve laceration (e.g., in open injuries) or if there is no recovery after several months (typically 3-6 months), not as an immediate first step for a post-operative palsy.
Option C (High-dose corticosteroid administration) is not a standard treatment for peripheral nerve palsies.
Option D (Referral for immediate NCS and EMG) is useful for confirming the extent of nerve injury and prognosis, but it is typically performed at 3-6 weeks post-injury, not immediately, as nerve degeneration needs time to occur for these studies to be diagnostic. The immediate priority is functional support and observation.
Option E (MUA) is used for arthrofibrosis/stiffness, not for nerve compression or palsy.
Question 8
A 38-year-old recreational athlete is undergoing rehabilitation after a multi-ligament knee reconstruction, including a PCL reconstruction. During the initial maximum protection phase (weeks 0-6), which of the following exercises or activities should be MOST strictly avoided to protect the PCL graft?
Explanation
Correct Answer: C
The case specifically highlights precautions for PCL reconstruction during rehabilitation: 'PCL Specific: Avoid isolated hamstring strengthening and excessive knee flexion (>90 degrees) during the initial weeks to protect the posterior graft. No active knee flexion beyond 45 degrees.' Active knee flexion, especially against resistance or beyond 45 degrees, can generate posterior shear forces on the tibia, which directly stresses the healing PCL graft and risks failure. Therefore, avoiding this is crucial.
Option A (PROM 0-90 degrees) is generally encouraged for cruciate ligaments to prevent arthrofibrosis, as long as it's controlled and within comfortable limits.
Option B (Quadriceps sets and SLR) are typically safe and encouraged early on to maintain muscle tone and prevent atrophy, as they primarily generate anterior shear forces, which are protective for the PCL.
Option D (TDWB with crutches) is a common weight-bearing progression in the initial phase, though for PLC reconstructions, NWB/TDWB may be extended. It's not the most strictly avoided activity for PCL specifically.
Option E (Cryotherapy and elevation) are standard post-operative measures to control pain and swelling and are always encouraged.
Question 9
A 29-year-old male is undergoing arthroscopic-assisted ACL reconstruction following a knee dislocation. The surgeon is preparing to pass the graft through the femoral and tibial tunnels. The image below depicts a common technique for graft fixation during this procedure. Based on the image and the case description, what is the primary purpose of the structure being fixed in the femoral tunnel?
Explanation
Correct Answer: C
The image provided shows an ACL reconstruction with a graft being fixed in the femoral tunnel, likely with an Endobutton or similar cortical suspension device. The question context specifies ACL reconstruction. The case explicitly states that the 'Anterior Cruciate Ligament (ACL): Resists anterior translation of the tibia relative to the femur and secondary valgus/varus and internal/external rotation.' Therefore, the primary purpose of the reconstructed ACL, and thus the graft being fixed, is to resist anterior translation of the tibia relative to the femur.
Option A (To provide primary resistance to posterior tibial translation) is the primary function of the PCL, not the ACL.
Option B (To reconstruct the posterolateral corner (PLC) of the knee) is incorrect. PLC reconstruction addresses varus and external rotation instability, distinct from ACL function.
Option D (To stabilize the medial collateral ligament (MCL) complex) is incorrect. The MCL is the primary restraint to valgus stress.
Option E (To repair a meniscal bucket-handle tear) is incorrect. Meniscal repair addresses meniscal pathology, not primary ligamentous stability.
Question 10
A 33-year-old active duty military personnel sustains a multi-ligamentous knee injury (ACL, PCL, and MCL tears) during a training exercise. After successful reduction and confirmation of vascular integrity, the orthopedic surgeon discusses the timing of definitive ligament reconstruction. According to current literature and guidelines, what is the most common approach regarding the timing of multi-ligament knee reconstruction?
Explanation
Correct Answer: C
The case discusses the timing of ligament reconstruction: 'Timing of Surgery: ...Acute (within 1-3 weeks): Many surgeons prefer early ligament repair/reconstruction to capitalize on tissue healing potential and facilitate rehabilitation, provided soft tissue swelling has subsided.' It further states under 'Summary of Key Literature and Guidelines': 'Current Consensus: The trend leans towards early surgical intervention for ligamentous reconstruction (within 1-3 weeks) once swelling has subsided and the knee has achieved a relatively quiescent state.'
Option A (Immediate reconstruction) is generally reserved for vascular repair, open dislocations, or irreducible dislocations. For ligamentous reconstruction, waiting for soft tissue swelling to subside (1-3 weeks) is often preferred to reduce the risk of arthrofibrosis and improve surgical conditions.
Option B (Delayed reconstruction 6-12 months) is typically too late and can lead to chronic instability, muscle atrophy, and increased difficulty in reconstruction due to scar tissue and retraction.
Option D (Non-operative management) is rarely indicated for true multi-ligament knee dislocations, as it almost universally leads to significant long-term instability and functional deficits in active individuals.
Option E (Staged reconstruction at 3-month intervals) is a possibility for very complex cases or specific patient factors, but the 'acute' (1-3 weeks) approach for all ligaments in a single setting (or closely staged) is more common once the acute inflammatory phase has passed.
Question 11
A 38-year-old male presents to the emergency department after a high-speed motor vehicle accident. He complains of severe right hip pain and is unable to bear weight. Radiographs reveal a Garden IV femoral neck fracture. The patient is otherwise hemodynamically stable after initial ATLS resuscitation. Which of the following statements regarding the management of this patient's fracture is most accurate?
Explanation
Correct Answer: C
The case emphasizes that intracapsular hip fractures in young, neurologically intact patients are high-energy injuries requiring urgent management. For a Garden IV (completely displaced) fracture in a young patient, the primary goal is native hip preservation by achieving anatomic reduction and stable fixation. The literature review highlights that 'time to surgery' is a critical factor, with intervention ideally within 6-12 hours (and certainly within 24 hours) to decompress the intracapsular hematoma and restore blood flow, thereby minimizing the risk of avascular necrosis (AVN) and nonunion. Multiple cannulated screws in an inverted triangle configuration are considered the gold standard for stable internal fixation in this population.
Option A is incorrect: Primary total hip arthroplasty is generally avoided in young patients with acute fractures unless there is severe pre-existing hip pathology or established AVN, as the goal is native hip preservation due to their expected longevity and functional demands.
Option B is incorrect: Non-operative management is not indicated for displaced (Garden III or IV) intracapsular fractures in young patients due to the extremely high risk of nonunion and AVN. Even for undisplaced Garden I/II fractures in young patients, operative fixation is generally recommended to prevent secondary displacement.
Option D is incorrect: While a DHS is effective for intertrochanteric fractures, the case states that multiple cannulated screws (typically three in an inverted triangle) are the gold standard for true intracapsular femoral neck fractures in young patients, offering superior rotational and shear stability with less bulk and less iatrogenic damage compared to a DHS.
Option E is incorrect: The case explicitly states that 'time is bone' and 'delays beyond 24 hours are associated with increased rates of AVN and nonunion.' While ATLS protocols prioritize life-threatening injuries, once the patient is stable, urgent hip surgery is paramount.
Question 12
A 28-year-old male sustains a femoral neck fracture after a fall from height. Pre-operative imaging reveals a Pauwels Type III fracture. During surgical planning, the orthopedic surgeon must consider the biomechanical implications of this fracture pattern. Which of the following statements best describes the Pauwels Type III classification and its management implications?
Explanation
Correct Answer: C
The case details the Pauwels classification, which focuses on the angle of the fracture line relative to the horizontal plane, reflecting the shear forces acting on the fracture site. Pauwels Type III fractures are defined by an angle greater than 50 degrees. This high angle indicates that the fracture is subjected to predominantly shear forces, making it highly unstable and prone to nonunion without robust fixation. The goal of surgical fixation is to counteract these shear forces.
Option A is incorrect: This describes a Pauwels Type I fracture, which has an angle less than 30 degrees and is primarily subjected to compressive forces, making it relatively stable.
Option B is incorrect: This describes a Pauwels Type II fracture, with an angle between 30 and 50 degrees, experiencing mixed compressive and shear forces and moderate instability.
Option D is incorrect: Pauwels Type III fractures are highly unstable and have a significant risk of nonunion, necessitating stable operative fixation, not non-operative management.
Option E is incorrect: The Pauwels classification specifically focuses on the fracture angle and shear forces, whereas the Garden classification describes the degree of displacement and impaction (Garden I-IV).
Question 13
A 42-year-old male presents with a displaced femoral neck fracture. During pre-operative planning, the surgeon reviews the critical blood supply to the femoral head. Which of the following arteries is considered the dominant source of blood supply to the femoral head and is most vulnerable in an intracapsular fracture?
Explanation
Correct Answer: C
The case explicitly states that the Medial Femoral Circumflex Artery (MFCA) is the dominant source of blood supply to the femoral head. It typically arises from the profunda femoris artery and gives off ascending branches that form the retinacular vessels (posterior superior, posterior inferior, anterior superior, anterior inferior) which ascend along the femoral neck within the synovium. The posterior superior retinacular vessels, derived from the MFCA, are considered the most critical, supplying the majority of the superior and posterior femoral head. An intracapsular fracture, especially with displacement, directly threatens these retinacular vessels, leading to ischemia and a high risk of avascular necrosis.
Option A is incorrect: The LFCA contributes primarily to the extracapsular arterial ring but typically has less direct supply to the femoral head itself compared to the MFCA.
Option B is incorrect: The profunda femoris artery is the origin of the MFCA, but not the direct dominant supply to the femoral head itself.
Option D is incorrect: The artery of the ligamentum teres (foveal artery), a branch of the obturator artery, supplies a small, variable portion of the inferomedial femoral head. Its contribution is generally minor in adults.
Option E is incorrect: The superior gluteal artery primarily supplies the gluteal muscles and contributes to the blood supply of the greater trochanter, but not directly to the femoral head.
Question 14
A 55-year-old active patient sustains a Garden II femoral neck fracture. After initial closed reduction attempts, fluoroscopy shows a near-anatomic reduction with less than 2mm displacement. The surgeon proceeds with internal fixation. Which of the following fixation constructs is considered the gold standard for this patient, and what is its typical configuration?
Explanation
Correct Answer: C
The case, particularly the 'Detailed Surgical Approach / Technique' and 'Summary of Key Literature / Guidelines' sections, explicitly states that 'multiple cannulated screws' are the most common and effective method for internal fixation of intracapsular hip fractures in young patients. Specifically, 'three parallel cannulated cancellous screws are used' in an 'inverted triangle configuration' to provide optimal biomechanical stability against shear and rotational forces. The screws should be placed parallel to the axis of the femoral neck and end in the subchondral bone of the femoral head, as depicted in the provided image.
Option A is incorrect: A single lag screw is insufficient for rotational stability. While a DHS (Dynamic Hip Screw) is a type of lag screw, the case states it is 'less commonly used for true intracapsular fractures in young patients due to the larger metalwork, potential for hardware prominence, and less ideal biomechanics for pure femoral neck fractures.' The image clearly shows three screws, not a single large one.
Option B is incorrect: Two screws provide less stability than three, especially against rotational forces. The inverted triangle configuration with three screws is preferred.
Option D is incorrect: Angulated blade plates were historically used but have largely been supplanted by cannulated screws due to less invasive application and similar or superior biomechanical performance.
Option E is incorrect: A dynamic condylar screw (DCS) is typically used for distal femoral fractures, not femoral neck fractures.
Question 15
A 32-year-old male undergoes internal fixation for a displaced femoral neck fracture. Post-operatively, he develops persistent hip pain, a limp, and radiographs at 8 months show no signs of healing and progressive implant failure. The femoral head appears viable. Which of the following complications is most likely, and what is the appropriate next step in management?
Explanation
Correct Answer: C
The patient's symptoms of persistent pain, limp, inability to bear weight, and radiographic evidence of progressive implant failure and lack of healing at 8 months post-op are classic signs of nonunion. The case defines nonunion as 'persistent pain, limb shortening, inability to bear weight, progressive implant failure, and lack of radiographic healing >6 months post-op.' Since the femoral head is described as viable, the management options for nonunion include 'revision internal fixation with improved fixation (e.g., more stable construct, valgus osteotomy to convert shear to compression) and bone grafting (autograft or allograft)' or, if deemed unlikely to succeed, 'Total Hip Arthroplasty (THA).'
Option A is incorrect: While AVN is a common complication, the question states the femoral head appears viable. AVN would typically show signs like sclerosis, cystic changes, or subchondral collapse. Core decompression and vascularized fibula grafting are treatments for early, pre-collapse AVN.
Option B is incorrect: Malunion implies the fracture healed in an incorrect position, leading to deformity. Here, the fracture has not healed (nonunion), and there is implant failure. A corrective osteotomy is for symptomatic malunion, not nonunion.
Option D is incorrect: While infection is a possibility, the symptoms described (persistent pain, limp, implant failure, lack of healing) are more indicative of nonunion. There are no signs of infection mentioned (fever, erythema, drainage, elevated inflammatory markers).
Option E is incorrect: Hardware prominence would typically cause localized pain over the hardware, not necessarily a limp, inability to bear weight, or progressive implant failure. Hardware removal is considered only after fracture union is complete, or if it's causing direct impingement/pain, not as a primary treatment for nonunion.
Question 16
A 48-year-old male with a displaced femoral neck fracture is brought to the operating room. The surgeon attempts closed reduction using the Leadbetter maneuver. Which of the following describes the correct sequence of the Leadbetter maneuver and its primary goal?
Explanation
Correct Answer: B
The case describes the classic Leadbetter maneuver under 'Reduction Maneuvers': 'While applying longitudinal traction, gently internally rotate the leg, abduct slightly, and then flex the hip.' The detailed surgical approach section refines this: 'gentle hip flexion to 30-45 degrees, maximal internal rotation (often to 45 degrees), and then gentle abduction. This maneuver aims to disimpact the fracture, correct external rotation, and restore the neck-shaft angle.' The primary goal is to achieve an anatomic reduction, correcting the common varus and external rotation deformities seen in displaced femoral neck fractures.
Option A is incorrect: This describes maneuvers that would likely worsen a displaced femoral neck fracture, which is typically externally rotated and in varus.
Option C is incorrect: While longitudinal traction is applied, adduction and external rotation would not typically reduce a displaced femoral neck fracture effectively.
Option D is incorrect: Hip flexion to 90 degrees is generally avoided in the early post-operative period due to stress on the fracture, and axial compression is not the primary mechanism of the Leadbetter maneuver.
Option E is incorrect: The sequence is incorrect, and the specific angles and goals are not accurately represented.
Question 17
A 35-year-old female sustains a Garden III femoral neck fracture. After several attempts at closed reduction fail to achieve an anatomic reduction (defined as >2mm displacement), the surgeon decides to proceed with open reduction. Which surgical approach is generally preferred for open reduction of femoral neck fractures in young patients, and why?
Explanation
Correct Answer: C
The case explicitly states under 'Open Reduction (if closed reduction fails)' that the 'Anterior (Smith-Petersen or Modified Watson-Jones) is the preferred approach for open reduction of femoral neck fractures.' The rationale provided is that 'It allows direct visualization of the fracture site, debridement of hematoma, and precise manipulation of fragments. It protects the posterior superior retinacular vessels, which are the primary blood supply.'
Option A is incorrect: The posterolateral approach is generally avoided for acute femoral neck fractures 'due to the risk of further damaging the posterior superior retinacular vessels and the greater muscle stripping required.'
Option B is incorrect: While the anterolateral approach can be used, the anterior approach is generally preferred for direct visualization and protection of the critical posterior blood supply.
Option D is incorrect: A direct lateral approach is not typically used for femoral neck fractures; it's more common for femoral shaft or trochanteric fractures.
Option E is incorrect: The medial approach is rarely used for adult femoral neck fractures and would not provide adequate visualization for reduction and fixation, nor is the artery of the ligamentum teres the primary blood supply in adults.
Question 18
A 22-year-old collegiate athlete undergoes internal fixation for a Garden I impacted valgus femoral neck fracture. Post-operatively, the rehabilitation protocol is initiated. Which of the following is the most appropriate initial weight-bearing instruction for this patient?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols' section clearly outlines the initial weight-bearing instructions: 'Toe-Touch Weight-Bearing (TTWB) or Partial Weight-Bearing (PWB) (10-20% body weight): This is the standard for 6-8 weeks.' The rationale is to 'provide micromotion believed to enhance osteogenesis while minimizing excessive shear or compressive forces that could displace the fracture or cause hardware failure.' Even for a stable Garden I fracture in a young, active patient, optimizing union and avoiding AVN is paramount, hence protected weight-bearing is crucial.
Option A is incorrect: Full weight-bearing immediately is generally too aggressive and carries a significant risk of fracture collapse, loss of reduction, or nonunion, even in a Garden I fracture, especially in a young patient where long-term outcomes are critical.
Option B is incorrect: Non-weight-bearing for 12 weeks is overly conservative for a Garden I fracture and would unnecessarily delay rehabilitation and increase the risk of stiffness and muscle atrophy. TTWB/PWB is preferred to allow for some loading.
Option D is incorrect: Weight-bearing as tolerated after only 2 weeks is too early for most femoral neck fractures, even Garden I, given the high risk of complications in young patients.
Option E is incorrect: While CPM can be used for some joint conditions, it's not the primary weight-bearing instruction for a femoral neck fracture, and complete non-weight-bearing for 4 weeks is not the standard initial approach for a Garden I fracture.
Question 19
A 40-year-old male with a history of a displaced femoral neck fracture treated with internal fixation 18 months ago presents with chronic, worsening hip pain. Radiographs show flattening and sclerosis of the femoral head with a subchondral crescent sign. The fracture appears united. What is the most likely complication, and what is the definitive treatment for this stage?
Explanation
Correct Answer: C
The clinical presentation of chronic, worsening hip pain 18 months post-fixation, coupled with radiographic findings of 'flattening and sclerosis of the femoral head with a subchondral crescent sign,' is highly indicative of advanced avascular necrosis (AVN) with femoral head collapse. The case describes AVN diagnosis: 'Radiographs show later stages (sclerosis, cystic changes, subchondral collapse, flattening of the femoral head).' For 'Late, Post-collapse (Ficat Stage III/IV)' AVN, the definitive treatment is 'Total Hip Arthroplasty (THA). '
Option A is incorrect: The question states the fracture appears united, ruling out nonunion. Revision internal fixation is for nonunion, not established AVN with collapse.
Option B is incorrect: Malunion would involve a healed fracture in a deformed position, leading to pain and altered biomechanics, but not typically the specific radiographic signs of AVN with collapse. A corrective osteotomy is for symptomatic malunion.
Option D is incorrect: While hardware removal is considered for symptomatic hardware after union, the described radiographic changes (flattening, sclerosis, crescent sign) point to a more severe underlying pathology (AVN) than just hardware irritation.
Option E is incorrect: There are no signs of infection (fever, erythema, drainage, elevated inflammatory markers) mentioned in the vignette.
Question 20
A 50-year-old patient presents with an intracapsular hip fracture. During pre-operative assessment, a CT scan is ordered. What is the primary utility of a CT scan in the acute setting for this type of injury, as described in the case?
Explanation
Correct Answer: C
The 'Pre-Operative Planning & Patient Positioning' section states that a 'Computed Tomography (CT) Scan is essential for detailed fracture morphology, especially for comminution, impaction patterns, and articular involvement. It aids in surgical planning for reduction maneuvers and screw placement. It can also rule out occult fractures.'
Option A is incorrect: MRI is the gold standard for early detection of AVN, not CT in the acute setting.
Option B is incorrect: MRI is valuable post-operatively for assessing occult nonunion or early chondral damage, not CT in the acute setting.
Option D is incorrect: While advanced imaging techniques can assess vascularity, a standard CT scan is not primarily used to evaluate the integrity of retinacular vessels or quantify blood flow. Angiography or MRI with contrast might provide some vascular information, but this is not the primary role of a routine pre-operative CT for fracture morphology.
Option E is incorrect: AP Pelvis and Cross-Table Lateral Hip X-rays are the standard initial imaging to confirm diagnosis and classify the fracture. CT provides more detail, but X-rays are usually sufficient for initial diagnosis.
Question 21
A 30-year-old male sustains a femoral neck fracture. The surgeon is considering the optimal placement of cannulated screws for fixation. Which of the following principles of screw placement is most crucial for maximizing stability and preventing complications?
Explanation
Correct Answer: C
The 'Fixation Technique' section, specifically under 'Cannulated Screws (CS),' details the crucial principles: 'The screws should be placed parallel to each other and parallel to the axis of the femoral neck, ending in the subchondral bone of the femoral head. This maximizes purchase and stability.' The image also visually reinforces the parallel placement and engagement with the subchondral bone.
Option A is incorrect: The case states: 'The screws should be partially threaded, allowing for interfragmentary compression, or fully threaded if no compression is desired (e.g., if there is already good impaction).' Fully threaded screws do not allow for interfragmentary compression, which is often desired. Excessive compression can also lead to collapse.
Option B is incorrect: Screws are typically placed parallel to the femoral neck axis, not perpendicular to the fracture line, to provide optimal stability and compression along the neck axis.
Option D is incorrect: While the inferior screw along the calcar is important, the inverted triangle configuration requires superior screws as well to provide rotational stability. Avoiding the superior retinacular vessels is achieved by careful surgical technique and approach (e.g., anterior open reduction), not by avoiding screw placement in the superior neck altogether.
Option E is incorrect: The case states: 'The guide wire should be centrally placed in the femoral neck on both views and approximately 5-10mm from the articular surface in the femoral head.' Placing them too close risks breaching the articular cartilage, leading to iatrogenic damage and potential early arthritis.
Question 22
A 45-year-old male with a displaced femoral neck fracture is being prepared for surgery. The surgical team is discussing the management of the joint capsule. Based on the case, what is the current understanding regarding the role of capsulotomy in preventing avascular necrosis (AVN)?
Explanation
Correct Answer: C
The 'Capsular Management' section states: 'After open reduction and fixation, the decision to close the capsule is debated... Current evidence does not definitively support one approach over the other for preventing AVN.' The 'Summary of Key Literature / Guidelines' further reinforces this: 'The practice of capsulotomy to decompress the intracapsular hematoma and potentially improve femoral head perfusion has been debated. While some studies suggest a benefit, current evidence is not conclusive that it independently reduces the rate of AVN.'
Option A is incorrect: The case explicitly states that evidence is not conclusive regarding its independent role in reducing AVN.
Option B is incorrect: Capsulotomy is often performed, especially in open reduction, and is not generally considered contraindicated. The concern is about further vascular disruption, but the anterior approach aims to protect vessels.
Option D is incorrect: While capsulotomy is essential for visualization in open reduction, the debate specifically addresses its role in decompressing the hematoma to improve vascularity, which is directly related to AVN prevention.
Option E is incorrect: While some advocate leaving the capsule open for decompression, the case clearly states that this is a debated topic and not universally recommended, as conclusive evidence is lacking.
Question 23
A 72-year-old female with a history of osteoporosis and 8 years of alendronate use presents to the emergency department after a low-energy fall. She complains of severe left thigh pain. Radiographs reveal a transverse fracture of the left subtrochanteric femur with a characteristic medial spike and minimal comminution. She reports prodromal thigh pain for the past 3 months. Which of the following classifications or associated conditions best describes this fracture?
Explanation
Correct Answer: C
The case explicitly describes Atypical Femoral Fractures (AFFs) as typically presenting as transverse or short oblique fractures with a characteristic medial spike, often preceded by prodromal thigh pain, and associated with prolonged bisphosphonate use, particularly in the elderly. The patient's history of 8 years of alendronate use, low-energy fall, prodromal thigh pain, and the radiographic description (transverse fracture with a medial spike) are all classic features of an AFF. Russell-Taylor and AO/OTA classifications describe general subtrochanteric patterns but do not specifically identify the etiology or unique features of AFFs. While AFFs are a type of subtrochanteric fracture, 'Atypical Femoral Fracture' is the most specific and accurate description given the detailed clinical vignette. It is not a high-energy trauma fracture, nor is there information to suggest a pathologic fracture from metastatic disease.
Question 24
A 35-year-old male sustains a high-energy subtrochanteric femur fracture. During surgical planning, the orthopedic surgeon anticipates significant displacement of the proximal fragment. Which combination of muscles is primarily responsible for the classic flexion, abduction, and external rotation deformity of the proximal fragment?
Explanation
Correct Answer: B
The case details the muscular attachments and deforming forces on the proximal fragment of a subtrochanteric fracture. It states: 'The iliopsoas, inserting on the lesser trochanter, causes flexion and external rotation of the proximal fragment. The gluteus medius and minimus, inserting on the greater trochanter, cause abduction. The short external rotators (piriformis, obturators, gemelli, quadratus femoris) further contribute to external rotation.' Therefore, the combination of gluteus medius, gluteus minimus, iliopsoas, and short external rotators is responsible for the classic flexion, abduction, and external rotation deformity.
Question 25
A 68-year-old female with severe osteoporosis presents with a comminuted subtrochanteric femur fracture. The surgical team is debating between intramedullary nailing (IMN) and plate fixation. Based on the biomechanical principles discussed in the case, which statement accurately describes the advantage of IMN in this scenario?
Explanation
Correct Answer: C
The case clearly differentiates between load-sharing and load-bearing devices under the 'Biomechanics' section. It states: 'Intramedullary Nails (IMN): As load-sharing devices, IMNs are placed within the medullary canal, closer to the mechanical axis of the femur. This central placement allows the bone-implant construct to share axial and bending loads, reducing stress shielding and promoting bone healing. IMNs are particularly effective in resisting bending forces, which are predominant in the subtrochanteric region. Their inherent stability against torsion, especially with two proximal and two distal locking screws, is a significant advantage.' Conversely, plates are described as load-bearing devices, 'more susceptible to fatigue failure, particularly in comminuted or osteoporotic bone.' Options A, B, D, and E contradict the information provided in the case.
Question 26
A 92-year-old male with end-stage heart failure, severe dementia, and a life expectancy estimated at less than 3 months, sustains a minimally displaced subtrochanteric femur fracture after a fall. He is bed-bound, non-ambulatory, and experiences only mild pain managed with oral analgesics. His medical team deems him unfit for anesthesia and surgery due to prohibitive risks. Based on the case, which of the following is the most appropriate management strategy?
Explanation
Correct Answer: C
The case outlines specific, highly limited circumstances for non-operative management. It states: 'Non-operative management for subtrochanteric fractures is exceedingly rare and generally reserved for specific, highly limited circumstances: Non-Ambulatory Patients with Minimal Pain: Patients who are bed-bound or severely debilitated with very limited functional demands, and who experience minimal pain from their fracture, may be considered for palliative non-operative care if surgical risks outweigh potential benefits. Extremely Poor Medical Status: Patients with severe, uncontrolled medical comorbidities where the risk of anesthesia and surgery is deemed prohibitive, and whose life expectancy is very limited, may be managed non-operatively (e.g., hospice care).' This patient's profile (92 years old, end-stage heart failure, severe dementia, bed-bound, minimal pain, prohibitive surgical risks, limited life expectancy) perfectly aligns with these non-operative indications.
Question 27
A 55-year-old male with a subtrochanteric femur fracture is undergoing pre-operative planning for intramedullary nailing. The surgeon is reviewing the radiographs, including the image below, to assess the fracture pattern, comminution, and femoral bowing.
Which of the following is a critical step during pre-operative radiographic assessment and templating, as highlighted in the case, to ensure optimal nail selection and prevent complications?
Explanation
Correct Answer: C
The 'Pre-Operative Planning' section emphasizes the importance of comprehensive radiographic assessment. It specifically states under 'Radiographic Assessment': 'Contralateral Femur: AP and lateral views of the contralateral, uninjured femur can be invaluable for templating nail length, diameter, and assessing normal femoral bow.' This step is crucial for selecting the correct implant size and curvature to match the patient's anatomy and prevent complications like iatrogenic fracture or malalignment. Options A, B, D, and E contradict the detailed planning steps outlined in the case. Standard views of the entire femur are needed, not just the hip. Intraoperative measurements are confirmatory, not primary. CT scans are useful for complex comminution. Reaming is typically 1-2mm larger than the nail, not smaller.
Question 28
During intramedullary nailing of a subtrochanteric femur fracture, the surgeon encounters difficulty reducing the classic deformity: the proximal fragment is flexed, abducted, and externally rotated, while the distal fragment is adducted and shortened. Which intraoperative maneuver or adjunct is most effective in overcoming the adduction of the distal fragment and facilitating reduction?
Explanation
Correct Answer: C
The 'Fracture Reduction' section explicitly addresses challenges in reduction and lists various aids. It states: 'Reduction Aids: Manual Manipulation: Direct pressure on the proximal or distal fragment. Percutaneous Clamps/Bone Hooks: Large pointed reduction clamps or bone hooks can be inserted percutaneously to grasp and manipulate fragments, particularly to overcome the adduction of the distal fragment or the flexion/external rotation of the proximal fragment.' While traction helps with length and some alignment, it alone may not overcome strong adduction. Manual pressure for internal rotation addresses the proximal fragment's external rotation, not the distal fragment's adduction. Decreasing reamer size is incorrect technique. Applying a plate to the medial cortex is not a primary reduction maneuver for IMN and is a different fixation strategy.
Question 29
A surgeon is preparing to insert an intramedullary nail for a subtrochanteric femur fracture. The case emphasizes the importance of selecting the correct entry point. For a subtrochanteric fracture, which entry point is often preferred for providing a more central alignment with the femoral shaft, and what is a key consideration for its placement?
Explanation
Correct Answer: B
The 'Entry Point & Guidewire Insertion' section under 'Intramedullary Nailing Antegrade Technique' discusses entry point selection. It states: 'Piriformis Fossa Entry: Often preferred for subtrochanteric fractures as it provides a more central alignment with the femoral shaft. The entry point is located slightly medial to the tip of the greater trochanter and slightly posterior.' It also emphasizes that 'Fluoroscopic Guidance: A guidewire is advanced under fluoroscopy (AP and lateral views) to confirm the optimal entry point. It should be placed centrally in both planes of the proximal femoral canal.' This aligns perfectly with option B. Other options describe incorrect or less preferred entry points for antegrade subtrochanteric nailing.
Question 30
A 58-year-old male undergoes intramedullary nailing for a comminuted subtrochanteric femur fracture. Six months post-operatively, radiographs show no signs of union, and he experiences persistent pain and inability to bear full weight. There are no signs of infection. The surgeon diagnoses an aseptic nonunion. Based on the case, what is generally considered the most common and effective salvage procedure for this complication?
Explanation
Correct Answer: C
The 'Late Postoperative' complications section, specifically under 'Nonunion/Delayed Union,' addresses the management of this issue. It states: 'Revision surgery is often required. Exchange nailing (removing the current nail and inserting a larger diameter nail) is the most common and effective salvage procedure for aseptic nonunion. This can be augmented with bone grafting (autograft or allograft), particularly if there is a significant bone defect.' Inserting a smaller diameter nail (Option A) would reduce stability. Applying a plate without removing the nail (Option B) is not the primary or most effective salvage. Prolonged non-weight-bearing (Option D) is unlikely to resolve an established nonunion. Total hip arthroplasty (Option E) is not typically indicated for subtrochanteric nonunion unless there is severe femoral head pathology, which is not described here.
Question 31
A 42-year-old active male undergoes intramedullary nailing for a stable subtrochanteric femur fracture with good bone quality and anatomical reduction. Post-operatively, the surgeon discusses the rehabilitation plan. Based on the general principles outlined in the case, what is the most likely initial weight-bearing status prescribed for this patient?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols' section, under 'General Principles,' discusses weight-bearing status. It states: 'Weight-Bearing As Tolerated (WBAT): Generally allowed for stable intramedullary nail constructs with good bone quality and adequate reduction. This allows patients to use pain as a guide and often accelerates functional recovery.' Given the patient's profile (active male, stable IMN construct, good bone quality, anatomical reduction), WBAT with an assistive device is the most appropriate initial weight-bearing status. NWB is rarely indicated, and TTWB/PWB are typically reserved for more comminuted or unstable fractures. Full weight-bearing immediately without an assistive device is too aggressive.
Question 32
A 70-year-old patient presents with a subtrochanteric femur fracture that extends into the piriformis fossa, making standard intramedullary nail insertion challenging. The surgeon is considering alternative fixation methods. Based on the 'Summary of Key Literature / Guidelines' section, which statement best reflects the current consensus regarding the primary treatment for most subtrochanteric fractures and the role of alternative fixation?
Explanation
Correct Answer: B
The 'Summary of Key Literature / Guidelines' section explicitly addresses this. Under 'Intramedullary Nailing vs Plate Fixation,' it states: 'Numerous Level I and II studies, systematic reviews, and meta-analyses consistently demonstrate the superiority of intramedullary nailing (IMN) over extramedullary plate fixation for the treatment of most subtrochanteric femoral fractures.' It then clarifies the role of plates: 'While modern locking compression plates (LCPs) offer improved angular stability, their use for primary fixation of subtrochanteric fractures remains generally limited to specific scenarios (e.g., extensive piriformis fossa comminution, specific atypical fracture patterns, or cases where IMN insertion is impossible due to existing hardware).' This directly supports option B. Options A, C, D, and E contradict the established consensus and evidence presented in the case.
Question 33
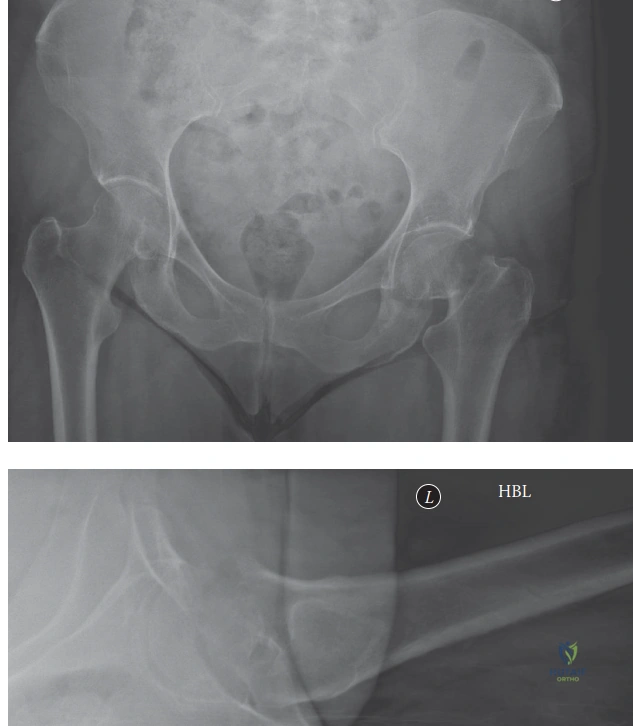
A 68-year-old male presents with a two-year history of worsening left hip pain, progressive instability, and a 3.5 cm leg length discrepancy following a revision THA 5 years prior. Clinical examination reveals a profound Trendelenburg gait, severely restricted range of motion, and an audible/palpable mechanical clunk. Preoperative radiographs, including the AP pelvis shown below, demonstrate catastrophic failure of the left acetabular construct with significant superior and medial migration, violation of Kohler's line, and extensive periacetabular osteolysis. The previously placed bulk femoral head allograft shows signs of advanced resorption and structural collapse.
Based on these findings, which of the following is the most appropriate initial classification of the acetabular defect, prior to advanced imaging?

Explanation
Correct Answer: E
The AP pelvis radiograph clearly demonstrates significant superior migration of the acetabular component exceeding 3 cm, violation of Kohler's line (indicating medial wall deficiency), and extensive periacetabular osteolysis in all three DeLee and Charnley zones. The superior dome is entirely deficient, and the previously placed bulk allograft has failed. These findings are characteristic of a Paprosky Type IIIB defect, which involves severe bone loss with a non-supportive rim and significant column compromise, specifically superior bone loss greater than 3 cm, severe destruction of the teardrop, Kohler's line, and both columns. While a pelvic discontinuity is strongly suspected clinically and radiographically (discontinuity of the ilioischial line), the Paprosky classification primarily describes bone loss morphology. The presence of a discontinuity is a distinct, often co-occurring, finding that further dictates surgical strategy but is not the primary descriptor within the Paprosky system itself for the defect morphology.
Paprosky Type I defects have minimal bone loss and an intact rim. Type IIA involves superior bone loss but intact columns. Type IIB involves superior and lateral bone loss. Type IIC involves a medial wall defect. None of these adequately describe the catastrophic bone loss and superior migration seen in the image and described in the vignette.
Question 34
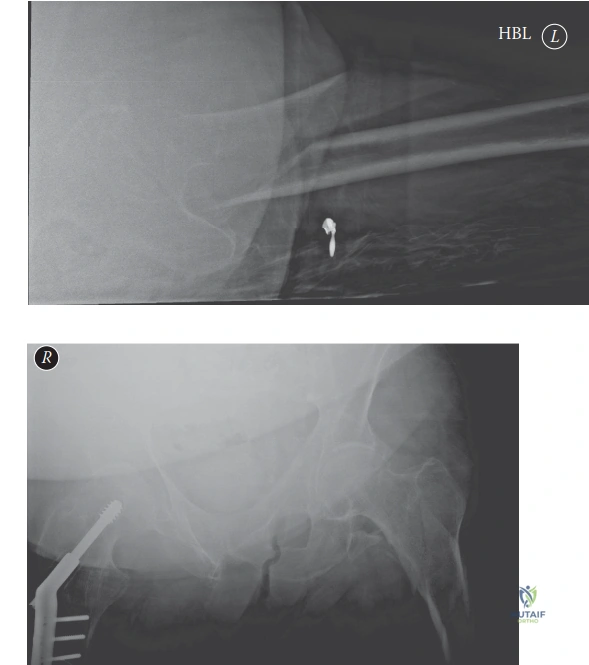
Following the initial AP pelvis radiograph, Judet oblique views were obtained. The obturator oblique view revealed near-complete destruction of the anterior column and quadrilateral plate, while the iliac oblique view demonstrated severe posterior column osteolysis extending into the ischium. These findings, combined with the AP view, raised a high suspicion for pelvic discontinuity, as shown in the image below.
Which of the following statements best describes the biomechanical significance of a complete pelvic discontinuity in the context of acetabular revision surgery?

Explanation
Correct Answer: B
A complete pelvic discontinuity is defined as a transverse fracture through the acetabulum that separates the superior hemipelvis (ilium) from the inferior hemipelvis (ischium and pubis). This mechanical uncoupling leads to gross instability of the acetabulum, where the two halves of the pelvis move independently. This instability prevents biological ingrowth into a standard cementless cup and requires a reconstructive strategy that can mechanically bridge and stabilize this fracture, such as a reconstruction cage or a custom triflange component, to allow for fracture healing and provide a stable foundation for the acetabular component.
Option A is incorrect because while superior dome deficiency often coexists, pelvic discontinuity is a distinct structural fracture, not just a bone loss pattern. A jumbo hemispherical cup alone cannot stabilize a discontinuity. Option C is incorrect; medial wall erosion is a component of severe defects, but discontinuity is a much more severe structural issue requiring robust mechanical bridging. Impaction bone grafting alone is insufficient for discontinuity. Option D is incorrect; while challenging, pelvic discontinuity is a well-recognized indication for advanced revision techniques like cup-cage constructs, not an absolute contraindication to reconstruction. Option E is incorrect; a contained cavitary defect is a Paprosky Type II defect, whereas discontinuity represents a much more severe, uncontained structural failure that cannot be managed with a standard cementless cup and screws alone.
Question 35
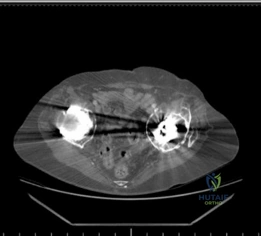
A high-resolution Computed Tomography (CT) scan of the pelvis with Metal Artifact Reduction Sequence (MARS) was obtained to precisely quantify volumetric bone loss and definitively diagnose pelvic discontinuity. The multi-planar reformatted images, as shown below, confirmed a massive Paprosky Type IIIB acetabular defect with complete absence of the superior dome, medial wall, and significant portions of both the anterior and posterior columns. Crucially, the axial and coronal cuts confirmed a frank pelvic discontinuity.
Given the confirmed Paprosky Type IIIB defect with pelvic discontinuity, which of the following reconstructive strategies is biomechanically most appropriate for this patient?

Explanation
Correct Answer: D
For a Paprosky Type IIIB defect with an associated pelvic discontinuity, the cup-cage reconstruction is a highly effective and commonly utilized strategy. The trabecular metal cup provides a porous surface for biological ingrowth into the remaining host bone (often with limited contact), while the ilioischial reconstruction ring (cage) mechanically bridges the pelvic discontinuity, providing immediate rigid stability by fixing to the intact bone of the ilium superiorly and the ischium inferiorly. This construct neutralizes shear forces across the discontinuity, allowing for fracture healing and protecting the biological ingrowth of the cup.
Option A (Impaction bone grafting with a standard cementless cup) has a high failure rate in the presence of discontinuity due to a lack of initial mechanical stability. Option B (Large diameter cementless cup with multiple screws) is insufficient to stabilize a pelvic discontinuity, as the underlying bone is uncoupled. Option C (Custom triflange acetabular component) is a viable option for this defect, offering excellent stability. However, the question asks for the most appropriate given the context, and CTACs require extensive preoperative manufacturing time, are highly expensive, and offer limited intraoperative flexibility, making the cup-cage a more readily available and flexible solution that achieves similar biomechanical goals. Option E (Girdlestone resection arthroplasty) is a salvage procedure typically reserved for intractable infection or failed reconstructions where further attempts are deemed futile, which is not the case here as a reconstructive option is being sought.
Question 36
The patient's prior revision THA 5 years ago utilized a bulk femoral head structural allograft to address a significant uncontained superior dome defect. The current failure mechanism is characterized by progressive functional decline, indicating mechanical failure secondary to particulate debris-induced osteolysis and subsequent massive periacetabular bone loss. The case specifically mentions that structural allografts carry a known risk of late failure due to incomplete creeping substitution, central necrosis, structural collapse, and loss of component support.
Which of the following cytokines is most directly implicated in the excessive osteoclastic bone resorption associated with particulate debris-induced osteolysis in total hip arthroplasty?
Explanation
Correct Answer: C
The case explicitly states that the generation of wear debris initiates a macrophage-mediated inflammatory cascade, releasing cytokines including Interleukin-1 (IL-1), Tumor Necrosis Factor-alpha (TNF-alpha), and Receptor Activator of Nuclear Factor Kappa-B Ligand (RANKL), which stimulate excessive osteoclastic bone resorption. RANKL is a critical cytokine that directly binds to its receptor, RANK, on osteoclast precursors, promoting their differentiation, activation, and survival, thereby driving bone resorption. It is a central mediator in the pathogenesis of periprosthetic osteolysis.
Options A (IL-4) and D (IL-10) are primarily anti-inflammatory cytokines. Option B (TGF-β) is involved in bone formation and remodeling, but not directly in the excessive osteoclastic resorption seen in osteolysis. Option E (PDGF) is a growth factor involved in cell proliferation and angiogenesis, not directly in osteoclast activation in this context.
Question 37
Preoperative laboratory diagnostics were obtained to definitively rule out subacute periprosthetic joint infection (PJI) prior to undertaking a massive reconstructive procedure. The Erythrocyte Sedimentation Rate (ESR) was 12 mm/hr (normal <20 mm/hr), and the C-Reactive Protein (CRP) was 0.4 mg/dL (normal <1.0 mg/dL). Given these normal inflammatory markers and the classic radiographic appearance of aseptic mechanical failure, preoperative joint aspiration was deemed unnecessary.
In a patient presenting with a painful THA, which combination of synovial fluid findings would most strongly suggest a periprosthetic joint infection (PJI) according to current diagnostic criteria?
Explanation
Correct Answer: B
According to the Musculoskeletal Infection Society (MSIS) criteria and other widely accepted guidelines, a synovial fluid white blood cell (WBC) count greater than 3,000 cells/µL and a polymorphonuclear neutrophil (PMN) percentage greater than 70% are highly suggestive of periprosthetic joint infection (PJI). The case specifically mentions these thresholds in its differential diagnosis table for PJI.
Option A represents findings typically associated with aseptic loosening. Option C has a high WBC count but a low PMN percentage, which would be atypical for PJI. Option D has a low WBC count despite a high PMN percentage, which would not meet PJI criteria. Option E represents an indeterminate zone, where further investigation (e.g., alpha-defensin, cultures) would be necessary, but it is not the most strongly suggestive combination for PJI.
Question 38
During the surgical intervention for this patient's massive Paprosky Type IIIB defect with pelvic discontinuity, an extended posterior approach was utilized. Extensive scar tissue from previous surgeries was encountered. Careful dissection was performed to identify and protect the sciatic nerve, which was found to be encased in dense fibrous tissue and tethered medially due to the superior migration of the acetabular construct. A formal sciatic nerve neurolysis was performed from the greater sciatic notch down to the proximal thigh.
The intraoperative image above shows the massive acetabular defect after explantation. What is the primary reason for the sciatic nerve being tethered medially in this specific clinical scenario?

Explanation
Correct Answer: C
The case explicitly states that the sciatic nerve was found to be encased in dense fibrous tissue and tethered medially 'due to the superior migration of the acetabular construct.' When the acetabular component migrates superiorly and medially into the true pelvis, it effectively shortens the distance between the greater sciatic notch (where the nerve exits) and the medial aspect of the pelvis, thereby pulling and tethering the sciatic nerve medially. This places the nerve at high risk of injury during subsequent revision surgery, necessitating careful neurolysis.
Option A is incorrect; the femoral stem was noted to be well-fixed and not implicated in nerve tethering. Option B is incorrect; while metallosis can cause pseudotumors and nerve compression, the case denies ALTR/metallosis as the primary issue and attributes the tethering to component migration. Option D is a contributing factor to scar tissue, but the primary mechanical cause of medial tethering is the component migration. Option E is an anatomical variation but does not explain the acquired medial tethering in the context of a failed THA.
Question 39
During the cup-cage reconstruction, a jumbo, highly porous trabecular metal multi-hole acetabular shell was selected and impacted into the prepared defect. Due to the massive bone loss, host bone contact was estimated at approximately 30-40%, primarily located superiorly against the ilium and inferiorly against the ischium. Multiple locking and non-locking screws were placed through the cup into the superior ilium and the posterior column to achieve initial press-fit stability. Despite the screws, the cup alone did not provide sufficient rigidity to neutralize the pelvic discontinuity, necessitating the cage construct.
What is the primary biomechanical role of the highly porous trabecular metal cup in this specific cup-cage construct for a Paprosky IIIB defect with pelvic discontinuity?
Explanation
Correct Answer: B
The case explicitly states that the highly porous trabecular metal cup is impacted into the remaining viable host bone, and its high coefficient of friction and osteoconductive properties promote rapid biological ingrowth, eventually providing long-term, durable fixation. This is the primary role of the porous cup: to achieve biological fixation and osseointegration with the host bone. The cage, not the cup, provides the immediate mechanical stability across the discontinuity.
Option A is incorrect; the cage provides the immediate rigid mechanical fixation across the discontinuity, protecting the cup. Option C is a secondary effect, but not its primary biomechanical role. Option D is incorrect; the polyethylene liner, cemented into the cage, provides the articulating surface, not the metal cup itself. Option E is a function of the entire construct, but the specific role of the porous cup is biological fixation.
Question 40
After the trabecular metal cup was inserted and secured, an ilioischial reconstruction cage was contoured and placed over the porous cup. The inferior flange of the cage was carefully slotted into the ischium, and the superior flange was contoured to lay flat against the lateral aspect of the ilium. Multiple cortical screws were placed through the superior flange into the dense bone of the ilium, and additional screws were placed through the central dome of the cage, passing through the multi-hole trabecular metal cup and into the host bone. A highly cross-linked polyethylene dual-mobility liner was then cemented into the cage, allowing for independent setting of version and inclination.
What is the critical biomechanical advantage of cementing the polyethylene liner into the cage, rather than using a press-fit or screw-in liner, in this cup-cage construct?
Explanation
Correct Answer: C
The case explicitly states: 'This step allows the surgeon to independently set the final version and inclination of the articular surface (targeting 15-20 degrees of anteversion and 40-45 degrees of inclination), regardless of the orientation of the underlying cage or host bone defect.' In complex revision cases with massive bone loss and pelvic discontinuity, achieving ideal anatomical orientation of the cage can be challenging. Cementing the liner allows for precise adjustment of the articular surface's orientation, which is crucial for optimizing hip stability and range of motion, independent of the cage's fixed position.
Option A is a benefit of dual-mobility liners in general, but not specific to the cementation aspect within the cage. Option B is incorrect; cementation provides mechanical fixation of the liner to the cage, not biological fixation to the host bone. Option D is incorrect; the cage still requires screws for rigid fixation to the ilium and ischium to bridge the discontinuity. Option E is partially true as it eliminates a modular junction between the liner and cage, but the primary biomechanical advantage highlighted in the case is the ability to adjust version and inclination.
Question 41
Following the curing of the cement, a trial reduction was performed using a dual-mobility femoral head on the existing well-fixed femoral stem. The hip was taken through a full range of motion, demonstrating remarkable stability with no impingement or tendency for dislocation. Leg length was assessed and found to be restored to within 5mm of the contralateral side, correcting the preoperative 3.5cm discrepancy. Intraoperative fluoroscopy was utilized to confirm the final component position.
The postoperative AP radiograph above demonstrates excellent restoration of the hip center of rotation, secure fixation of the ilioischial cage bridging the discontinuity, and appropriate seating of the cemented dual-mobility liner. Which of the following radiographic features on this image confirms the successful bridging of the pelvic discontinuity?
Explanation
Correct Answer: C
The primary purpose of the ilioischial reconstruction cage in the setting of pelvic discontinuity is to mechanically bridge the transverse fracture separating the superior and inferior hemipelves. This is achieved by securing the cage with screws into the intact bone of the ilium superiorly and the ischium inferiorly, effectively spanning and stabilizing the discontinuity. On the postoperative radiograph, the visible screws extending from the cage into both the ilium and ischium, crossing the presumed fracture line, are the direct radiographic evidence of this bridging and stabilization.
Option A (dual-mobility articulation) is a feature of the bearing surface, not the discontinuity stabilization. Option B (restoration of hip center of rotation) is a goal of the reconstruction but does not specifically confirm bridging of the discontinuity. Option D (well-fixed femoral stem) refers to the femoral side, which was not the primary focus of the acetabular reconstruction. Option E (absence of a superior dome defect) is a result of the reconstruction, but the bridging of the discontinuity is specifically confirmed by the cage's fixation to both hemipelves.
Question 42
Postoperatively, the patient was placed on a strict rehabilitation protocol. For the initial 8 weeks, the patient was restricted to Toe-Touch Weight Bearing (TTWB) or Flat-Foot Weight Bearing (FFWB) on the operative extremity. This restriction was deemed absolutely critical, despite the immediate mechanical stability provided by the cup-cage construct.
What is the primary rationale for strict weight-bearing restrictions during the early postoperative phase (Weeks 0-8) following a cup-cage reconstruction for pelvic discontinuity?
Explanation
Correct Answer: D
The case explicitly states: 'The initial stability of the construct relies on the mechanical fixation of the cage. However, long-term success requires biological bone ingrowth into the trabecular metal cup. Excessive early axial loading can cause micromotion, leading to fibrous encapsulation rather than osseointegration.' Therefore, the primary rationale for strict weight-bearing restrictions is to protect the biological fixation of the trabecular metal cup. Micromotion at the bone-implant interface inhibits osteointegration and promotes the formation of a fibrous interface, which can lead to early aseptic loosening.
Option A is less critical with a dual-mobility articulation, which significantly mitigates dislocation risk. Option B is a secondary benefit but not the primary reason for such strict weight-bearing restrictions. Option C is incorrect; the femoral stem was noted to be well-fixed preoperatively. Option E (DVT risk reduction) is addressed by pharmacological and mechanical prophylaxis, not by weight-bearing restrictions.
Question 43
The patient's past surgical history included a primary THA 15 years prior, followed by a revision THA 5 years ago due to aseptic loosening of the primary acetabular component. The prior revision involved the implantation of a larger, multi-hole cementless acetabular component supplemented with multiple trans-acetabular screws and a bulk femoral head structural allograft to address a significant uncontained superior dome defect. The current failure is attributed to the insidious mechanism of particulate debris-induced osteolysis and subsequent massive periacetabular bone loss, with the structural allograft showing signs of advanced resorption and collapse.
Considering the patient's history of a failed structural allograft, which of the following is the most significant long-term disadvantage of using bulk structural allografts in acetabular reconstruction for massive defects?
Explanation
Correct Answer: C
The case explicitly highlights the known risk of late failure with structural allografts: 'Structural allografts frequently undergo creeping substitution, which can be incomplete, leading to central necrosis, structural collapse, and subsequent loss of component support.' This inherent biological limitation, where the allograft may not fully integrate or may resorb over time, is the most significant long-term disadvantage, leading to loss of support for the acetabular component and subsequent failure.
Option A (acute PJI) is a risk with any implant, but not a specific long-term disadvantage unique to structural allografts compared to other options. Option B (difficulty in achieving initial mechanical stability) can be a challenge, but with proper fixation (e.g., reconstruction rings), initial stability can often be achieved. The long-term issue is biological. Option D (limited availability and high cost) can be practical concerns but are not biomechanical or biological disadvantages related to their long-term performance. Option E (increased risk of nerve injury) is a surgical risk associated with complex revision surgery but not a specific long-term disadvantage of the allograft material itself.
Question 44
A 45-year-old male is brought to the trauma bay after a motor vehicle collision. Radiographs and CT of the pelvis reveal a complex acetabular fracture. A 'spur sign' is identified on the obturator oblique radiograph. This radiographic finding is pathognomonic for which of the following fracture patterns?
Explanation
Question 45
A 24-year-old male sustains a high-energy Pauwels type III vertical femoral neck fracture. Which of the following fixation constructs provides the greatest biomechanical stability and lowest rate of mechanical failure for this specific fracture pattern?
Explanation
Question 46
During an ilioinguinal approach for an anterior column acetabular fracture, excessive bleeding is encountered while dissecting over the superior pubic ramus. The bleeding is most likely originating from an anastomosis between which of the following vessels?
Explanation
Question 47
A 55-year-old male sustains a subtrochanteric femur fracture. Following injury, the proximal fragment typically assumes a characteristic deformed position. Which of the following muscle combinations is primarily responsible for the flexion and abduction of the proximal segment?
Explanation
Question 48
A 25-year-old male sustains a high-energy vertical shear femoral neck fracture (Pauwels Type III) following a motor vehicle collision. Which of the following fixation constructs offers the highest biomechanical stability against shear forces for this specific fracture pattern?
Explanation
Question 49
A 35-year-old male sustains a subtrochanteric femur fracture. On the AP radiograph, the proximal fragment is visibly flexed, abducted, and externally rotated. Which of the following muscle insertions is primarily responsible for the external rotation deformity of the proximal fragment?
Explanation
Question 50
In the evaluation of a patient with a complex acetabular fracture, an obturator oblique radiograph is obtained. Which two primary structures of the acetabulum are best visualized in profile on this specific radiographic view?
Explanation
Question 51
A 45-year-old male undergoes open reduction and internal fixation of a transverse acetabular fracture via a Kocher-Langenbeck approach. Intraoperatively, what is the optimal positioning of the ipsilateral lower extremity to minimize iatrogenic tension on the sciatic nerve?
Explanation
Question 52
A 75-year-old, active, community-ambulating female presents with a displaced intracapsular femoral neck fracture. She has no significant cognitive deficits. What is the primary advantage of performing a total hip arthroplasty (THA) compared to a hemiarthroplasty in this specific patient population?
Explanation
Question 53
An 82-year-old female sustains a periprosthetic femur fracture around a cemented total hip arthroplasty following a mechanical fall. Radiographs demonstrate a fracture at the tip of the stem. The stem is clinically and radiographically loose, but there is adequate proximal bone stock. According to the Vancouver classification, what is the most appropriate surgical treatment?
Explanation
Question 54
A 30-year-old male undergoes antegrade intramedullary nailing for an isolated, high-energy femoral shaft fracture. The surgeon utilizes a piriformis fossa entry portal. Damage to which of the following structures is the most significant concern if the starting point is inadvertently placed too anteriorly and medially?
Explanation
Question 55
During an ilioinguinal approach for an anterior column acetabular fracture, surgical dissection proceeds through the middle window. Which of the following structures defines the lateral border of this middle window?
Explanation
Question 56
A 50-year-old male sustains a posterior hip dislocation with an associated femoral head fracture. CT imaging reveals a fracture fragment that involves the weight-bearing surface of the femoral head, extending superior to the fovea capitis. According to the Pipkin classification, what type of fracture is this?
Explanation
Question 57
A 45-year-old male presents after a motor vehicle collision with an acetabular fracture. Radiographs and CT demonstrate a fracture line separating the anterior half of the ilium and the anterior wall from the intact posterior ilium, exiting through the obturator ring, combined with a transverse fracture through the posterior column. A portion of the posterior articular surface remains attached to the intact axial skeleton. What is the Letournel classification of this fracture pattern?
Explanation
Question 58
A 25-year-old male sustains a vertically oriented (Pauwels type III) femoral neck fracture. To maximize biomechanical stability and reduce the risk of varus collapse and nonunion, which of the following fixation constructs is most appropriate?
Explanation
Question 59
A 32-year-old female presents with a distal femur fracture following a high-energy trauma. CT imaging reveals a coronal plane fracture of the lateral femoral condyle. Which of the following is the most appropriate biomechanical fixation technique for this specific fracture fragment?
Explanation
Question 60
A 40-year-old male sustains a posterior hip dislocation with an associated femoral head fracture. CT scan confirms the femoral head fracture involves the fovea capitis and extends superiorly to the weight-bearing zone, with an associated posterior wall acetabular fracture. Based on the Pipkin classification, what type of fracture is this?
Explanation
Question 61
In a subtrochanteric femur fracture, the proximal fragment typically assumes a characteristic position due to unopposed muscle forces. Which combination of muscles is primarily responsible for the flexion, abduction, and external rotation of the proximal fragment?
Explanation
Question 62
During the ilioinguinal approach for an anterior column acetabular fracture, significant hemorrhage occurs while dissecting over the superior pubic ramus. This bleeding is most likely originating from an anastomosis between the external iliac (or deep inferior epigastric) vessels and which of the following vessels?
Explanation
Question 63
A 55-year-old male is undergoing a total hip arthroplasty (THA) for post-traumatic osteoarthritis 3 years after nonoperative management of a transverse acetabular fracture. Intraoperatively, a nonunion of the posterior column with pelvic discontinuity is identified. Which of the following acetabular reconstruction techniques is most appropriate?
Explanation
Question 64
An 82-year-old female presents with thigh pain and inability to bear weight after a mechanical fall. Radiographs demonstrate a spiral fracture around the stem of her uncemented total hip arthroplasty. The fracture extends just distal to the tip of the stem. Radiographic evaluation shows stem subsidence of 10 mm, but the remaining femoral bone stock is adequate. According to the Vancouver classification, how should this be managed?
Explanation
Question 65
A 68-year-old male sustains a reverse obliquity intertrochanteric femur fracture (AO/OTA 31-A3). Biomechanically, why is a cephalomedullary nail preferred over a sliding hip screw (SHS) for this specific fracture pattern?
Explanation
Question 66
A 35-year-old male falls from a roof and sustains a Schatzker VI tibial plateau fracture. On presentation, his leg is tense, and he has extreme pain with passive stretch of the hallux. If compartment syndrome is confirmed and four-compartment fasciotomies are performed, how should the definitive management of the articular fracture ideally be staged?
Explanation
Question 67
A 22-year-old male presents with a grossly deformed knee following a rugby tackle. Closed reduction of an anterior knee dislocation is performed. The Ankle-Brachial Index (ABI) is calculated to be 0.8. Distal pulses are palpable but slightly asymmetric compared to the contralateral limb. What is the most appropriate next step in management?
Explanation
Question 68
During a Kocher-Langenbeck approach for a posterior wall acetabular fracture, the surgeon elevates the gluteus minimus off the ilium. To prevent iatrogenic denervation of the abductor musculature, dissection superior to the greater sciatic notch should be limited to what distance?
Explanation
Question 69
A 29-year-old male presents with a displaced femoral neck fracture. To preserve the primary blood supply to the femoral head during surgical exposure, the surgeon must be cautious not to injure the deep branch of the medial femoral circumflex artery (MFCA). Where is this vessel consistently located?
Explanation
Question 70
A hemodynamically stable polytrauma patient presents with an ipsilateral closed midshaft femur fracture and a closed midshaft tibia fracture (floating knee). Which of the following describes the most efficient and well-accepted surgical approach for definitive intramedullary nailing of both fractures?
Explanation
None
