Mastering Lower Limb Deformity, LLD & Biomechanics: ABOS Board Review | Part 2

Key Takeaway
This ABOS board review covers comprehensive lower limb deformity analysis, leg length discrepancy (LLD) management, and gait biomechanics. It details Shapiro's classification, Moseley graph, Paley Multiplier Method, and Paley's osteotomy rules for surgical correction, alongside TKA alignment principles. Essential for orthopedic exam preparation.
Mastering Lower Limb Deformity, LLD & Biomechanics: ABOS Board Review | Part 2
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
According to Paley's principles of deformity correction, what is the expected result when both the osteotomy and the hinge axis are placed exactly at the Center of Rotation of Angulation (CORA)?
Explanation
Question 2
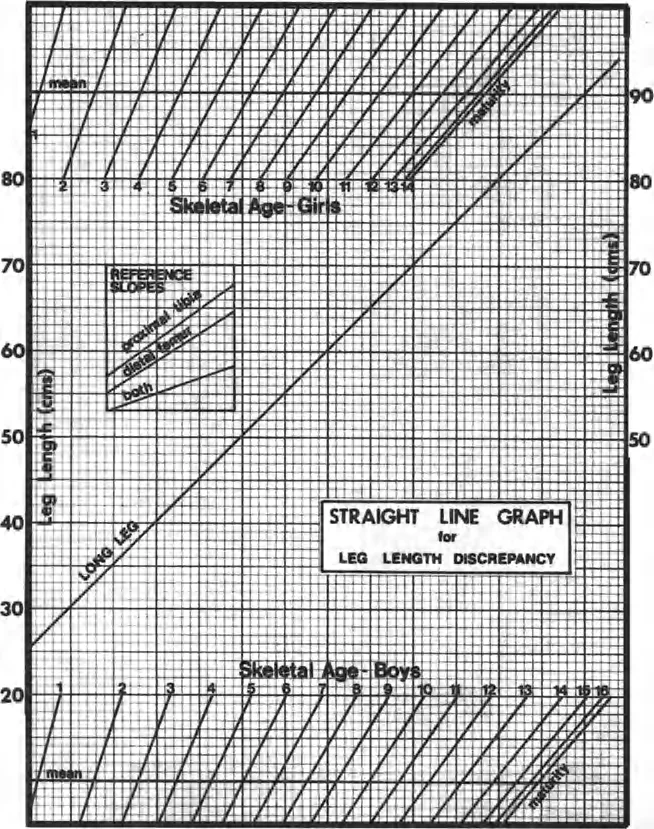
A girl with a 3 cm right leg length discrepancy (LLD) has a skeletal bone age of 11 years. Assuming skeletal maturity at age 14, what is the most appropriate management to achieve limb equality at maturity based on the Menelaus method?
Explanation
Question 3
A patient with severe genu varum presents with a Mechanical Axis Deviation (MAD) measuring 30 mm medial to the center of the knee. What is the expected biomechanical consequence in the knee joint?
Explanation
Question 4
A 45-year-old male undergoes a medial opening wedge high tibial osteotomy (HTO) for medial compartment arthritis. Postoperatively, what predictable biomechanical change regarding the extensor mechanism is most likely to occur?
Explanation
Question 5
When planning a deformity correction using an external fixator for distraction osteogenesis, a latency period of 7 to 10 days is typically observed. What is the primary biological purpose of this phase?
Explanation
Question 6
A surgeon plans an osteotomy for a diaphyseal tibial deformity. The osteotomy is performed proximal to the CORA due to poor soft tissues, but the hinge of the frame is placed exactly on the CORA. According to Paley's rules, what is the expected outcome?
Explanation
Question 7
A patient's lower extremity radiographs reveal a mechanical lateral distal femoral angle (mLDFA) of 81 degrees and a medial proximal tibial angle (MPTA) of 87 degrees. The joint line convergence angle (JLCA) is 2 degrees. What is the primary source of the deformity?
Explanation
Question 8
During gradual femoral lengthening using an Ilizarov external fixator, the patient develops a progressive knee flexion and hip abduction contracture. Increased tension in which of the following structures is most likely responsible?
Explanation
Question 9
An 18-month-old child presents with bilateral symmetric genu varum. Standing AP radiographs show a metaphyseal-diaphyseal angle (Drennan's angle) of 8 degrees bilaterally. What is the most appropriate management?
Explanation
Question 10
Using the multiplier method for limb length discrepancy (LLD), what is the estimated final LLD at skeletal maturity for a 4-year-old girl who currently has a congenital LLD of 2.5 cm?
Explanation
Question 11
An 8-year-old girl has a predicted leg length discrepancy of 3.5 cm at maturity due to a prior distal femoral physeal fracture. What is the most appropriate definitive management?
Explanation
Question 12
According to the principles of lower limb deformity correction, if an osteotomy is performed exactly at the Center of Rotation of Angulation (CORA) and the mechanical axis lines are aligned around a hinge at this same location, what is the biomechanical outcome?
Explanation
Question 13
During gradual distraction osteogenesis for lower limb lengthening, what is the primary mode of bone formation observed within the distraction gap?
Explanation
Question 14
A patient undergoes a medial opening-wedge high tibial osteotomy (HTO) for varus gonarthrosis. How does this procedure typically affect patellar height and posterior tibial slope if the anterior gap is opened the exact same amount as the posterior gap?
Explanation
Question 15
A newborn is diagnosed with complete fibular hemimelia. Which of the following associated lower extremity anomalies is most universally expected in this patient?
Explanation
Question 16
A 12-year-old boy is undergoing a 4-cm tibial lengthening using a circular frame. Two months into distraction, the physician notes increasing difficulty with ankle dorsiflexion. What is the primary cause of this complication?
Explanation
Question 17
When using the Paley Multiplier method to predict leg length discrepancy at skeletal maturity for a congenital discrepancy, the multiplier for a girl at age 3 is approximately 2.0. What underlying assumption does this mathematical method rely on?
Explanation
Question 18
In the evaluation of an 18-month-old child with significant genu varum, which of the following radiographic parameters most strongly predicts progression to infantile Blount disease rather than resolution of physiologic bowing?
Explanation
Question 19
According to Paley's first rule of osteotomy for lower limb deformity, if the osteotomy is performed exactly at the Center of Rotation of Angulation (CORA) and the correction hinge is placed on the transverse bisector line, what is the geometric result?
Explanation
Question 20
A surgeon applies Osteotomy Rule 2 for a proximal tibial deformity. The osteotomy is performed at a level distinct from the CORA, but the hinge is maintained on the bisector line of the CORA. What is the expected outcome of this correction?
Explanation
Question 21
In a skeletally mature adult with normal coronal alignment, where does the mechanical axis of the lower extremity (Mikulicz line) typically pass in relation to the center of the knee joint?
Explanation
Question 22
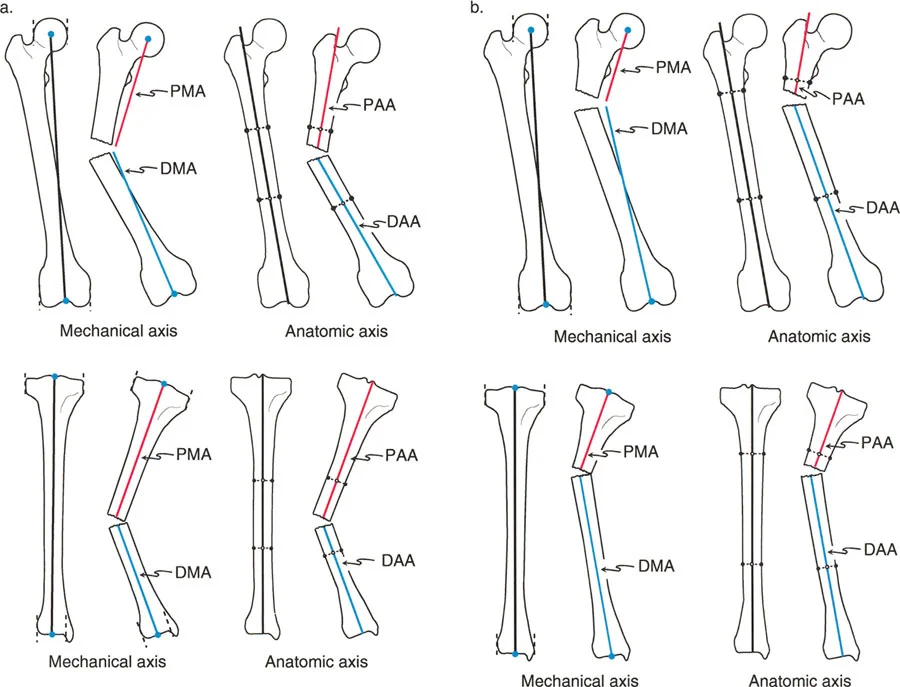
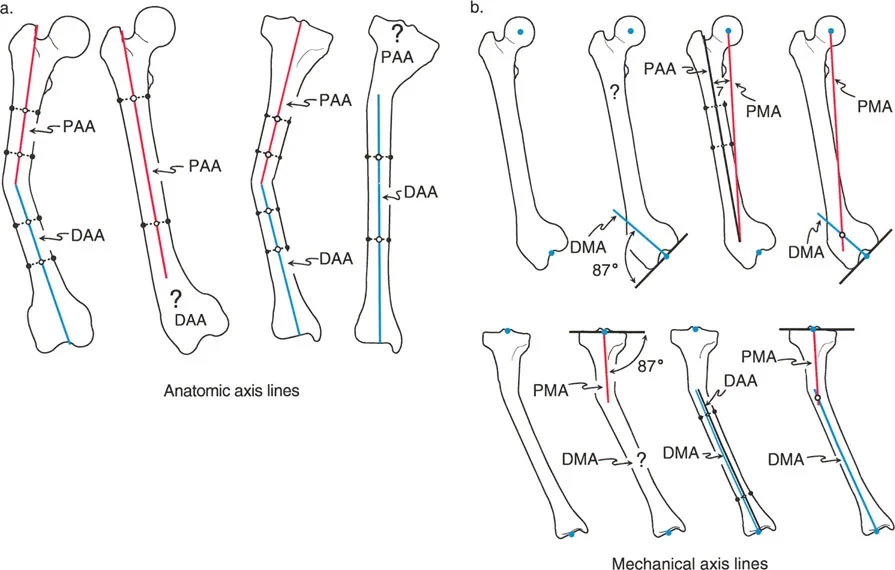
When planning a distal femoral corrective osteotomy, understanding the relationship between the mechanical and anatomic axes of the femur is critical. In a normal femur, the angle between the anatomic and mechanical axes (AMA angle) typically measures:
Explanation
Question 23
An 11-year-old girl with a skeletal age of 11 presents with a projected leg length discrepancy (LLD) of 3 cm. Assuming standard growth rates, how much length correction can be anticipated if a contralateral distal femoral epiphysiodesis is performed today?
Explanation
Question 24
A patient presents with a projected leg length discrepancy at maturity of 1.5 cm due to a mild congenital hemihypertrophy. What is the most appropriate management recommendation?
Explanation
Question 25
During preoperative planning for a varus distal femoral deformity, the surgeon measures the mechanical lateral distal femoral angle (mLDFA). What is the accepted normal population average for the mLDFA?
Explanation
Question 26
The Taylor Spatial Frame (TSF) relies on a specific biomechanical concept to correct complex multi-planar lower limb deformities simultaneously. Which mechanical principle forms the basis of the TSF?
Explanation
Question 27
A surgeon seeks to maximize the biomechanical bending and torsional stiffness of a circular Ilizarov frame for tibial lengthening. Which combination of modifications is most effective?
Explanation
Question 28
A 25-year-old male undergoing tibial distraction osteogenesis at a rate of 1 mm/day is noted on 4-week follow-up radiographs to have premature consolidation of the regenerate. What is the most appropriate next step in management?
Explanation
Question 29
When performing a diaphyseal tibial corticotomy for Ilizarov distraction osteogenesis in an adult, what is the standard recommended latency period before initiating distraction?
Explanation
Question 30
A surgeon is performing a medial opening-wedge high tibial osteotomy (HTO). If the anterior aspect of the osteotomy gap is inadvertently opened wider than the posterior aspect, what is the biomechanical consequence on the sagittal alignment?
Explanation
Question 31
A 40-year-old patient presents with a symptomatic valgus deformity of 15 degrees originating entirely within the distal femur. To restore the mechanical axis while avoiding leg length discrepancy, which procedure is mechanically most sound if lengthening is strictly avoided?
Explanation
Question 32
During normal human gait, the joint reaction force across the knee is highest during which specific phase?
Explanation
Question 33
According to Paley's Rule 3, if a corrective osteotomy is performed outside the CORA and the hinge is placed at the osteotomy site rather than on the bisector line, what is the geometric consequence?
Explanation
Question 34
A 6-year-old child presents with severe bowing of the proximal tibia. Radiographs demonstrate depression of the medial tibial plateau with a physeal bar, consistent with Langenskiöld stage VI infantile Blount disease. What is the most appropriate surgical intervention?
Explanation
Question 35
During a 5 cm proximal tibial lengthening using a circular fixator, the patient complains of dorsal foot numbness and new-onset weakness in the extensor hallucis longus. What is the most appropriate initial management step?
Explanation
Question 36
When planning a deformity correction, an osteotomy is performed at a level different from the center of rotation of angulation (CORA), but the mechanical axis is realigned. According to Paley's rules of osteotomy, what is the expected outcome at the osteotomy site?
Explanation
Question 37
A 4-year-old girl has a congenital femoral deficiency with a current leg length discrepancy of 3 cm. Using the Paley multiplier method, what is the predicted discrepancy at skeletal maturity?
Explanation
Question 38
During tibial lengthening using distraction osteogenesis, the standard protocol involves a distraction rate of 1 mm per day. If serial radiographs reveal premature consolidation of the regenerate, which modification is most appropriate?
Explanation
Question 39
An obese 3-year-old boy presents with progressive bilateral genu varum. Radiographs show a medial metaphyseal beak and a Drennan's angle (metaphyseal-diaphyseal angle) of 20 degrees. What is the primary biomechanical derangement leading to this condition?
Explanation
Question 40
When evaluating a long-leg standing radiograph for a suspected lower limb deformity, the mechanical axis deviation (MAD) is measured. In a normal lower extremity, where does the mechanical axis line pass relative to the knee joint center?
Explanation
Question 41
A 7-year-old child undergoes lateral tension band plating (guided growth) of the distal femur for genu valgum. Three months post-operatively, radiographs show backing out of the diaphyseal screw. What is the most likely surgical cause?
Explanation
Question 42
A 12-year-old boy is undergoing a 6 cm tibial lengthening over an Ilizarov frame. During the consolidation phase, he develops a fixed 20-degree equinus contracture. Which biomechanical factor primarily drives this complication?
Explanation
Question 43
The Taylor Spatial Frame (TSF) utilizes the principles of a Stewart platform to correct complex multiplanar deformities. How many degrees of freedom does this hexapod system allow for simultaneous correction?
Explanation
Question 44
A 14-year-old male presents with a leg length discrepancy. A scanogram confirms the right femur is 3.5 cm shorter than the left. He is at Risser 4, and his bone age matches his chronologic age. Which of the following is the most appropriate management?
Explanation
Question 45
When performing fixator-assisted nailing (FAN) for distal femoral deformity correction, what is the primary advantage of placing the external fixator before reaming and nail insertion?
Explanation
Question 46
A patient presents with severe osteoarthritis and a significant varus deformity. The Joint Line Convergence Angle (JLCA) measures 6 degrees (medial convergence). What does this abnormal JLCA indicate about the deformity?
Explanation
Question 47
An infant with Proximal Focal Femoral Deficiency (PFFD) is evaluated. Radiographs show a severely dysplastic proximal femur with no radiographic evidence of a femoral head or acetabulum. According to the Aitken classification, what is the grade of this deformity?
Explanation
Question 48
A surgeon is planning a lateral opening wedge osteotomy of the distal femur to correct a valgus deformity. To prevent unintended sagittal plane deformity (flexion or extension), where should the mechanical hinge be aligned?
Explanation
Question 49
During a massive femoral lengthening procedure, a patient develops paresthesias in the anterolateral thigh and knee, alongside isolated weakness in knee extension. Which nerve is most likely experiencing a stretch injury?
Explanation
Question 50
A patient with a 4 cm structural right leg length discrepancy stands barefoot. To maintain truncal balance and visual gaze, which compensatory mechanism is primarily utilized by the pelvis and hips?
Explanation
Question 51
In the context of distraction osteogenesis, what does the Bone Healing Index (BHI) objectively measure?
Explanation
Question 52
When evaluating sagittal alignment of the femur, the mechanical posterior distal femoral angle (mPDFA) is assessed. Which of the following values represents the normal anatomical range for the mPDFA?
Explanation
Question 53
According to Paley's rules of deformity correction, if an osteotomy is performed at a level different from the Center of Rotation of Angulation (CORA), but the hinge is placed exactly at the CORA (Rule 2), what is the expected biomechanical outcome?
Explanation
Question 54
According to the White-Menelaus rule of thumb for estimating remaining growth, what is the expected annual longitudinal growth from the distal femoral and proximal tibial physes, respectively?
Explanation
Question 55
During distraction osteogenesis of the tibia using a circular fixator, a patient develops premature consolidation of the regenerate bone. What is the most appropriate initial management?
Explanation
Question 56
A 9-year-old obese male presents with progressive bowing of the left leg. Radiographs reveal a prominent step-off and depression of the medial tibial plateau with an osseous bridge, consistent with Langenskiöld Stage VI late-onset Blount's disease. Which is the most appropriate definitive surgical intervention?
Explanation
Question 57
In assessing lower limb coronal alignment using standard nomenclature, the normal mechanical lateral distal femoral angle (mLDFA) and medial proximal tibial angle (MPTA) are approximately:
Explanation
Question 58
When correcting a complex uniplanar deformity, if the osteotomy and the hinge are both placed away from the Center of Rotation of Angulation (CORA) (Paley's Rule 3), what is the inevitable biomechanical outcome?
Explanation
Question 59
Which of the following physical exam findings best differentiates a structural from a compensatory hindfoot varus in a patient with a rigid plantarflexed first ray (cavovarus foot)?
Explanation
Question 60
A 14-year-old male presents with anterior knee pain and an out-toeing gait. Examination shows hip internal rotation of 10 degrees and external rotation of 80 degrees. The mechanical axis is neutral. What deformity is most likely present and what is the optimal correction?
Explanation
Question 61
When planning a single-stage correction of an oblique plane deformity (combined varus and recurvatum) in the proximal tibia, the true axis of the deformity is determined by:
Explanation
Question 62
A patient undergoing tibial lengthening with a circular fixator develops erythema, induration, and purulent discharge around a proximal wire site. Radiographs show no lucency around the wire. According to the Checketts-Otburn classification, what is the appropriate management for this Grade 2 pin site infection?
Explanation
Question 63
In utilizing a hexapod circular fixator (e.g., Taylor Spatial Frame) for lower limb deformity correction, the concept of "chronic automation" relies primarily on which of the following mathematical principles?
Explanation
Question 64
During distraction osteogenesis, the optimal rate and rhythm of distraction established by Ilizarov to promote woven bone formation and minimize tissue ischemia is:
Explanation
Question 65
A 14-year-old boy is undergoing correction of a severe varus deformity in the tibial diaphysis. The Center of Rotation of Angulation (CORA) is correctly identified. The surgeon performs the osteotomy 4 cm distal to the CORA but places the hinge axis of the external fixator exactly on the CORA. According to Paley's Rule 2 of deformity correction, what is the expected geometric outcome once angular correction is achieved?
Explanation
Question 66
A surgeon is planning to correct a tibial deformity. According to Paley's Rule 2 of deformity correction, if the hinge axis is placed exactly on the Center of Rotation of Angulation (CORA) but the osteotomy is performed at a different level (proximal or distal to the CORA), what is the expected geometric outcome at the osteotomy site?
Explanation
Question 67
What is the foundational principle underlying the Paley Multiplier method for predicting limb length discrepancy (LLD) in patients with congenital femoral deficiency?
Explanation
Question 68
A 45-year-old male presents with severe varus gonarthrosis. Standing long leg radiographs reveal a mechanical axis deviation (MAD) of 45 mm medial to the center of the knee. The mechanical lateral distal femoral angle (mLDFA) is 88 degrees and the medial proximal tibial angle (MPTA) is 80 degrees. The joint line convergence angle (JLCA) is 1 degree. What is the primary source of the varus deformity and the most appropriate site for osteotomy?
Explanation
Question 69
A 25-year-old male is undergoing tibial lengthening via distraction osteogenesis. The distraction rate was conservatively set at 0.5 mm per day (0.25 mm twice daily). During the distraction phase, radiographs at 3 weeks show dense, bridging trabeculae across the entire regenerate gap. What is the most likely complication of this protocol, and what is the appropriate initial intervention?
Explanation
Question 70
A patient presents with a severe procurvatum deformity of the proximal tibia (apex anterior angulation) due to a prior unreduced fracture. Which of the following compensatory gait abnormalities is mechanically most likely to be observed?
Explanation
Question 71
When utilizing a hexapod external fixator (e.g., Taylor Spatial Frame) to correct a multiplanar deformity, accurate input of mounting parameters is critical. Which of the following best defines the 'rotary frame offset' parameter?
Explanation
Question 72
A 12-year-old boy presents with a 2.5 cm leg length discrepancy due to a prior left femoral shaft fracture. His skeletal age is identical to his chronological age. Based on the Menelaus approximation of the Green-Anderson charts, and assuming skeletal maturity at age 16, which intervention will most accurately achieve limb length equality at maturity?
Explanation
Question 73
A 10-year-old patient is undergoing a 5 cm tibial lengthening using a circular external fixator. At the 4-week follow-up, the patient develops lateral ankle pain. Radiographs reveal proximal migration of the lateral malleolus and widening of the distal tibiofibular clear space. What critical technical step was likely omitted during the initial frame application?
Explanation
Question 74
According to Paley's principles of deformity correction, if the osteotomy is performed at a different level than the Center of Rotation of Angulation (CORA) but the hinge is placed exactly on the CORA, what is the geometric result after correction?
Explanation
Question 75
A surgeon is planning a corrective osteotomy for a tibial diaphyseal deformity. According to Paley's principles (Rule 2), if the hinge axis is placed exactly at the Center of Rotation of Angulation (CORA) but the osteotomy is performed at a different level, what is the expected biomechanical outcome?
Explanation
Question 76
A 16-year-old male presents with lateral mechanical axis deviation (MAD) of the lower extremity. Standing alignment radiographs reveal a mechanical lateral distal femoral angle (mLDFA) of 81° and a medial proximal tibial angle (MPTA) of 87°. The joint line convergence angle (JLCA) is 1°. What is the primary anatomic source of his malalignment?
Explanation
Question 77
A 15-year-old male undergoes gradual correction of a severe proximal tibial valgus and procurvatum deformity using a circular hexapod frame. On postoperative day 14, he develops weakness in ankle dorsiflexion and decreased sensation in the first web space. Which nerve is most likely compromised?
Explanation
Question 78
When evaluating a sagittal plane deformity of the distal tibia using standard lateral radiographs, what is the generally accepted normal value for the mechanical posterior distal tibial angle (mPDTA)?
Explanation
Question 79
A 10-year-old girl (skeletal age 10) presents with a 2.5 cm leg length discrepancy (LLD) secondary to a prior left distal femur fracture. Using the Menelaus method, at what age should a right distal femoral epiphysiodesis be performed to achieve limb length equality at skeletal maturity?
Explanation
Question 80
A surgeon applies Paley's Rule 3 during a deformity correction, placing both the osteotomy and the hinge axis at a location distant from the Center of Rotation of Angulation (CORA). What is the expected biomechanical consequence of this configuration?
Explanation
Question 81
A 35-year-old patient is undergoing tibial lengthening via distraction osteogenesis (Ilizarov technique) at a standard rate of 1 mm/day. Radiographs at 6 weeks reveal a central radiolucent fibrous interzone of 9 mm with poor regenerate bone formation. What is the most appropriate next step in management?
Explanation
None
