Comprehensive ABOS Review: Lower Limb Deformity Analysis, Biomechanics & Surgical Planning | Part 14

Key Takeaway
Orthopedic deformity correction involves precise radiographic analysis of lower limb alignment, understanding biomechanics, and applying principles like CORA and Paley's rules for osteotomy planning. It addresses conditions like genu varum, coxa vara, and limb length discrepancy, often utilizing intramedullary nailing or external fixation to restore normal mechanical axis and function.
Question 1
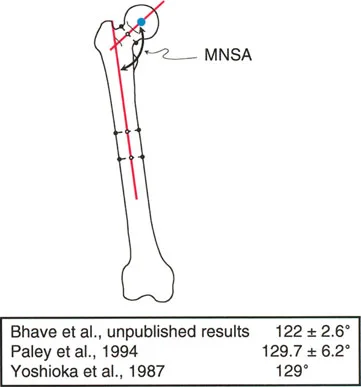
A 28-year-old male is being evaluated for a post-traumatic femoral neck malunion. The surgeon measures the angle between the mechanical axis of the femur and the axis of the femoral neck. What is this measurement?
View Answer & Explanation
Correct Answer: B
Rationale: The Mechanical Neck Shaft Angle (MNSA) is defined as the angle between the mechanical axis of the femur and the axis of the femoral neck. This is distinct from the LPFA (A), which uses a line from the greater trochanter tip to the femoral head center.
Question 2
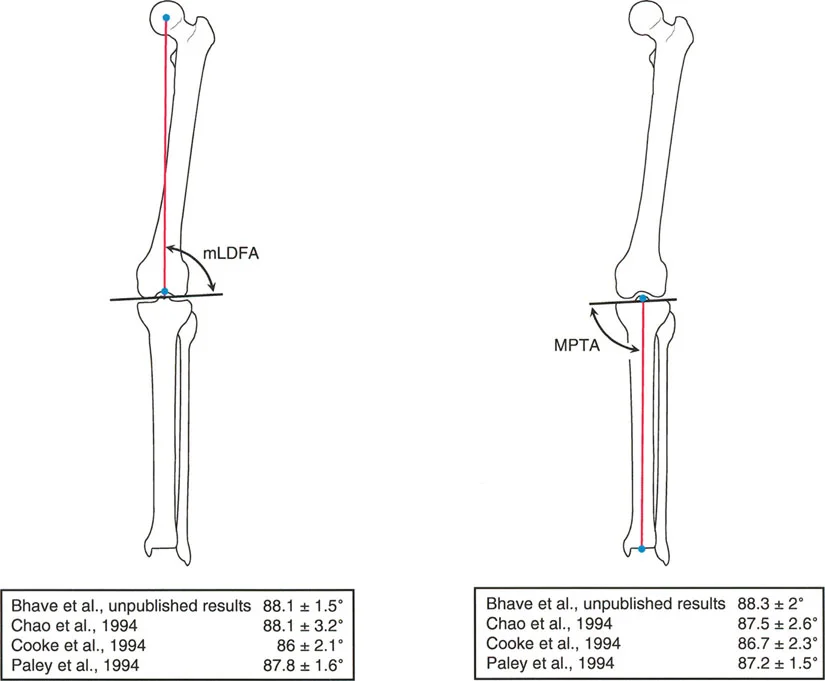
A surgeon is performing an open reduction and internal fixation of a supracondylar femur fracture. To ensure proper alignment and avoid post-traumatic arthritis, what is the target value for the mechanical Lateral Distal Femoral Angle (mLDFA)?
View Answer & Explanation
Correct Answer: B
Rationale: The accepted normal mLDFA is 87.5° ± 2°. This means the distal femur is in slight valgus relative to its mechanical axis. Achieving a 90° angle (C) would be incorrect and would create a varus deformity at the knee.
Question 3
A 55-year-old male has a post-traumatic deformity of the distal femur. His standing alignment film shows a mechanical Lateral Distal Femoral Angle (mLDFA) of 93°. How would this deformity be characterized?
View Answer & Explanation
Correct Answer: B
Rationale: The normal mLDFA is 87.5°, indicating slight valgus. An angle greater than this, such as 93°, indicates a loss of the normal valgus and a shift into varus. Distal femoral valgus (A) would be represented by an mLDFA less than 87.5°.
Question 4
A resident is asked to measure the mechanical Medial Proximal Tibial Angle (MPTA) on a preoperative radiograph for a high tibial osteotomy. Which landmarks are used to define this angle?
View Answer & Explanation
Correct Answer: D
Rationale: The MPTA is defined as the medial angle formed between the mechanical axis of the tibia and the proximal tibial joint line. All other options describe different angles (e.g., B describes the LDTA).
Question 5
A 60-year-old male is being planned for a medial opening wedge high tibial osteotomy for varus malalignment and medial compartment osteoarthritis. What is the accepted normal value for the mechanical Medial Proximal Tibial Angle (MPTA)?
View Answer & Explanation
Correct Answer: C
Rationale: The text provides an accepted normal MPTA of 87° ± 2°. This indicates that the proximal tibia is normally in slight varus relative to its mechanical axis. An MPTA of 90° (D) would be perpendicular, which is not the normal state.
Question 6
A 30-year-old patient has a post-traumatic deformity of the proximal tibia with a measured mechanical Medial Proximal Tibial Angle (MPTA) of 94°. This finding indicates which type of deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The normal MPTA is 87°, indicating slight varus. An angle greater than this, such as 94°, represents a deformity in the valgus direction. Proximal tibial varus (A) would be indicated by an MPTA less than 87°.
Question 7
A 58-year-old male presents with progressive right medial knee pain and a noticeable bow-legged deformity. During single-leg stance, the ground reaction vector (GRV) passes significantly medial to the center of his knee joint. According to the principles of joint loading, what is the primary biomechanical consequence of this GRV position?
View Answer & Explanation
Correct Answer: B
Rationale: When the GRV passes medial to the knee center, it increases the lever arm for the adductor moment, which exponentially amplifies the compressive forces on the medial compartment. This is the fundamental mechanism of overload in varus deformity. Increased lateral compartment compression (D) would occur in a valgus deformity.
Question 8
A 62-year-old female is being evaluated for a high tibial osteotomy (HTO). A standing full-length radiograph is obtained. The surgeon draws a line from the center of the femoral head to the center of the ankle plafond. The perpendicular distance from this line to the center of the knee joint is measured. What is this critical measurement called?
View Answer & Explanation
Correct Answer: C
Rationale: The Mechanical Axis Deviation (MAD) is defined as the perpendicular distance from the mechanical axis (femoral head center to ankle center) to the center of the knee. It is the single most important measurement for quantifying coronal plane alignment.
Question 9
A 65-year-old man has a severe varus deformity of his right knee, as depicted in Diagram C of the provided image. His mechanical axis falls entirely medial to the knee joint. What is the approximate load distribution across his medial and lateral tibial compartments during single-leg stance?
View Answer & Explanation
Correct Answer: E
Rationale: As described in the text and shown in the diagram, when a severe varus deformity causes the mechanical axis to fall completely medial to the knee joint, 100% of the joint load is borne by the medial compartment. This catastrophic overload state guarantees accelerated cartilage wear. A 75/25 distribution (A) is seen in physiologic varus (Diagram B).
Question 10
A 55-year-old female presents with debilitating medial knee pain and is observed to have a dynamic varus thrust during gait. She has no ligamentous instability on examination. When planning a corrective osteotomy, which of the following is the most crucial radiographic parameter to restore?
View Answer & Explanation
Correct Answer: C
Rationale: The ultimate goal of a coronal plane deformity correction around the knee is to restore the normal mechanical axis, thereby normalizing the load distribution across the joint. While other parameters are important, the mechanical axis is the primary determinant of joint loading and the main target of correction.
Question 11
A surgeon is planning a high tibial osteotomy for a patient with varus malalignment and medial compartment arthritis. The goal is to shift the mechanical axis slightly lateral to the center of the knee to unload the medial compartment. The ideal postoperative location for the mechanical axis to pass through the tibial plateau is often referred to as what?
View Answer & Explanation
Correct Answer: B
Rationale: The Fujisawa point is the target point for overcorrection in a high tibial osteotomy, typically located at 62-66% of the tibial plateau width from the medial edge. Passing the mechanical axis through this point effectively unloads the diseased medial compartment. The CORA (A) is the center of the deformity, not the target for correction.
Question 12
A 48-year-old male is observed to walk with a prominent lateral trunk shift over his left leg during the stance phase of gait. He has a history of left medial knee pain and radiographic evidence of a varus deformity. What is the primary purpose of this gait modification?
View Answer & Explanation
Correct Answer: D
Rationale: This gait pattern is a Duchenne (or compensated Trendelenburg) gait. By lurching the torso laterally, the patient shifts their center of gravity, which moves the ground reaction force vector closer to the center of the knee. This shortens the adductor moment arm and significantly reduces the painful compressive forces on the overloaded medial compartment.
Question 13
A 67-year-old female with a painful varus left knee is evaluated. Her standing radiographs show a significant varus deformity, but during clinical gait analysis, her varus thrust appears minimal. She does, however, have a pronounced lurch of her torso to the left with each step. What is the most important implication of this finding for the surgeon?
View Answer & Explanation
Correct Answer: C
Rationale: The Duchenne gait is a dynamic compensation that can make the underlying varus deformity appear less severe during casual observation. The surgeon must rely on the standing radiographs to appreciate the true magnitude of the Mechanical Axis Deviation, as the compensatory trunk shift is actively reducing the dynamic thrust.
Question 14
A 22-year-old male presents with anterior knee pain and a persistent flexed-knee gait after a remote tibial fracture. On examination, he has a 25-degree knee flexion posture when standing, but his passive knee extension is full (0 degrees) when examined on the table. A lateral radiograph reveals a Posterior Proximal Tibial Angle (PPTA) of 65 degrees. What is the most accurate diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The key finding is the discrepancy between the flexed posture during weight-bearing and the full passive extension on the exam table. This, combined with the abnormal (decreased) PPTA, indicates an extra-articular bony deformity (procurvatum) is forcing the knee into an obligate flexed position to get the foot plantigrade. A true FFD (A) would mean the knee cannot be passively extended to 0 degrees.
Question 15
A patient has a proximal tibial procurvatum deformity with a PPTA of 60°, as shown in the provided image. To achieve a plantigrade foot, the patient must maintain a 30° knee flexion posture. Which of the following surgical procedures would be a disastrous error in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The patient's flexed-knee posture is an obligate compensation for an extra-articular bony deformity, not a soft-tissue contracture. Attempting to treat this with soft-tissue releases (hamstring lengthening, capsular release) would fail to address the underlying osseous problem and could lead to significant knee instability. The correct treatment is a bone-level correction (A).
Question 16
A 35-year-old patient has a 10-degree recurvatum deformity of the distal tibia (abnormal ADTA). To compensate and achieve a plantigrade foot, the patient walks with 10 degrees of compensatory ankle plantar flexion. What is the most significant biomechanical consequence of this compensation on the ankle joint?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that compensatory plantar flexion to accommodate a distal tibial recurvatum uncovers the talar dome. As little as 5° of recurvatum can reduce the tibiotalar contact area by 30%. This drastically increases the stress per unit area, leading to accelerated ankle arthrosis.
Question 17
A 50-year-old female presents with a stiff ankle and knee pain. On examination, she has a rigid 15-degree equinus contracture of her right ankle. During gait, she is observed to snap her knee into hyperextension during the mid-stance phase. What is the term for this compensatory knee deformity?
View Answer & Explanation
Correct Answer: D
Rationale: A rigid equinus contracture prevents the necessary ankle dorsiflexion for the tibia to advance over the foot during stance. To compensate and allow forward progression, the body's only option is to force the knee backward into hyperextension, which is termed genu recurvatum. This places immense stress on the posterior soft tissues of the knee.
Question 18
A 70-year-old male with severe knee osteoarthritis has a 24-degree fixed flexion deformity (FFD) of his right knee, as shown in the image. Which phase of the normal gait cycle is completely eliminated by this deformity?
View Answer & Explanation
Correct Answer: C
Rationale: Normal gait begins with heel strike, where the heel makes initial contact with the ground while the knee is in near-full extension. A patient with a significant FFD has a functionally shortened limb and cannot reach the ground with their heel first. They are forced into a "flat-foot" or "forefoot" strike, completely eliminating the heel rocker mechanism.
Question 19
A patient with a 20-degree knee fixed flexion deformity (FFD) complains of rapid fatigue when walking. What is the primary reason for the increased metabolic energy cost associated with this gait pattern?
View Answer & Explanation
Correct Answer: B
Rationale: The elimination of the heel strike and heel rocker mechanism due to an FFD drastically reduces the limb's ability to absorb shock upon weight acceptance. This abrupt, uncontrolled loading is biomechanically inefficient and skyrockets the metabolic energy cost of walking, leading to rapid fatigue.
Question 20
According to Paley's principles, what is the first and most critical step in the preoperative planning for any angular limb deformity correction?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that locating the CORA is the absolute cornerstone and the "first, non-negotiable step" in preoperative planning. The CORA defines the true epicenter of the deformity, and all subsequent decisions about osteotomy location and hinge placement revolve around this geometric point.
Question 21
A surgeon is evaluating a standing full-length AP radiograph. An angle is measured between the mechanical axis of the femur and the joint line of the knee. What is this angle, and what is its normal average value?
View Answer & Explanation
Correct Answer: B
Rationale: The Mechanical Lateral Distal Femoral Angle (mLDFA) defines the relationship between the femoral mechanical axis and the distal femoral joint line in the coronal plane. Its normal average value is 87° (range 85-90°). The MPTA (A) relates to the tibia.
Question 22
During preoperative planning for a high tibial osteotomy, the Medial Proximal Tibial Angle (MPTA) is measured to be 78°. What does this value indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The normal MPTA is 85-90°. An angle less than 85° indicates a varus deformity originating from the proximal tibia. An angle greater than 90° would indicate valgus. Procurvatum (E) is a sagittal plane deformity measured by the PPTA.
Question 23
A standing AP radiograph of a patient with a varus knee deformity shows that the femoral and tibial joint lines are not parallel, converging medially by 4 degrees. What is this measurement called, and what does it most likely represent?
View Answer & Explanation
Correct Answer: C
Rationale: The Joint Line Convergence Angle (JLCA) measures the non-parallelism of the knee joint lines and is normally 0-2°. An elevated JLCA (greater than 2°) indicates an intra-articular contribution to the overall deformity, typically from asymmetric medial compartment cartilage loss or lateral collateral ligament laxity.
Question 24
A patient presents with a flexed-knee gait. A standing lateral radiograph is obtained to assess sagittal alignment. The angle measured between the anterior cortex of the proximal tibia and the tibial plateau is found to be 68°. What is this angle, and what deformity does it signify?
View Answer & Explanation
Correct Answer: B
Rationale: The angle described is the Posterior Proximal Tibial Angle (PPTA), which evaluates sagittal alignment of the proximal tibia. The normal value is approximately 81° (range 77-84°). A value less than 77°, such as 68°, indicates an anterior bow, or procurvatum deformity.
Question 25
According to Paley's first rule of osteotomy, what is the result when the osteotomy cut is made at the CORA and the axis of correction (hinge) is also placed at the CORA?
View Answer & Explanation
Correct Answer: D
Rationale: Paley's first rule describes the ideal scenario for simple angular deformities. When both the osteotomy and the corrective hinge are located precisely at the CORA, the bone segments pivot perfectly around the deformity's epicenter, resulting in pure angular correction without any associated translation.
Question 26
A 14-year-old boy presents with progressive bilateral leg bowing and knee pain. On examination, he has a lateral thrust during gait. Radiographs are shown. Based on Paley's principles, the varus deformity shown significantly increases the external moment arm acting on the knee. What is this moment called?
View Answer & Explanation
Correct Answer: C
Rationale: In genu varum, the ground reaction force passes medial to the center of the knee joint, creating an external adduction moment. This moment tends to open the lateral side of the knee and compress the medial side, leading to increased stress on the medial compartment and lateral ligaments. The knee abduction moment (distractor D) is increased in genu valgum.
Question 27
A 16-year-old female presents with bilateral knock-knees and lateral knee pain, especially with running. A clinical photograph is shown. This deformity results in a dysfunctional lever arm for which of the following structures during single-limb stance?
View Answer & Explanation
Correct Answer: D
Rationale: Genu valgum causes the ground reaction force to pass lateral to the knee, creating an external abduction (valgus) moment. This moment must be counteracted by internal adduction (varus) forces generated by the lateral soft tissue structures, primarily the lateral collateral ligament (LCL) and the iliotibial (IT) band. This chronic tension overload can lead to lateral-sided pain and instability.
Question 28
A 12-year-old boy with the deformity seen in the radiograph is evaluated for gait disturbance. The medial deviation of the mechanical axis in genu varum leads to a compensatory gait pattern to reduce the knee adduction moment. Which of the following gait modifications is most commonly observed?
View Answer & Explanation
Correct Answer: C
Rationale: To decrease the high external knee adduction moment in genu varum, patients often sway their trunk laterally over the stance limb. This shifts the body's center of mass closer to the knee joint center, reducing the lever arm of the ground reaction force and thus decreasing the adduction moment and medial compartment load. Increased hip adduction (distractor B) would worsen the varus alignment and increase the adduction moment.
Question 29
A 25-year-old male presents with a painful right foot deformity following a crush injury 2 years ago. His clinical and radiographic images are shown. During the terminal stance phase of gait, this equinovarus posture most significantly impairs the function of which muscle group by shortening its lever arm?
View Answer & Explanation
Correct Answer: C
Rationale: The peroneus longus and brevis are the primary evertors of the foot and also contribute to plantarflexion. In a fixed varus deformity, the foot is already inverted, placing the peroneal tendons at a mechanical disadvantage and shortening their effective lever arm for eversion. This dysfunction impairs their ability to stabilize the lateral side of the foot and contribute to a balanced push-off. The gastrocnemius-soleus complex (distractor B) is a powerful plantarflexor, but its primary lever arm is not as compromised by the varus alignment as the everters are.
Question 30
A 17-year-old female is evaluated for a right limb length discrepancy (LLD) and associated deformities. A scanogram is provided. The observed pelvic obliquity is a common compensation for LLD. This compensation effectively shortens the lever arm of which muscle group on the longer (left) side, leading to a Trendelenburg gait?
View Answer & Explanation
Correct Answer: C
Rationale: To compensate for the shorter right leg, the patient drops the pelvis on the right side (adduction of the left hip) when standing on the left leg. This adduction of the stance limb (the longer leg) decreases the horizontal distance between the greater trochanter and the center of the femoral head, effectively shortening the lever arm of the hip abductors (gluteus medius and minimus). This makes them less efficient, requiring more force to stabilize the pelvis, which can manifest as a Trendelenburg gait.
Question 31
A 10-year-old boy presents with a complex left lower extremity deformity. Radiographs demonstrate a significant tibial malunion or congenital pseudarthrosis. In planning a corrective osteotomy, the intersection of the proximal and distal axial lines of the tibia defines what critical parameter?
View Answer & Explanation
Correct Answer: C
Rationale: The Center of Rotation of Angulation (CORA) is a fundamental principle in deformity correction. It is the point where the proximal anatomical (or mechanical) axis of a deformed bone intersects with the distal anatomical (or mechanical) axis. Placing an osteotomy at the CORA allows for correction of the angulation without introducing translation. The MAD (distractor A) is the distance from the mechanical axis to the center of the knee, not a point within the bone itself.
Question 32
A 15-year-old female with the deformity shown in the radiograph complains of patellofemoral pain and instability. The genu valgum alignment alters the Q-angle and patellar tracking. This malalignment creates a dysfunctional lever arm that results in what primary deforming force on the patella?
View Answer & Explanation
Correct Answer: B
Rationale: Genu valgum increases the Q-angle, which is the angle between the line of pull of the quadriceps (approximated by a line from the ASIS to the center of the patella) and the line of pull of the patellar tendon (center of the patella to the tibial tubercle). A larger Q-angle increases the lateral vector force on the patella during knee extension, predisposing it to lateral subluxation, dislocation, and patellofemoral pain due to altered contact pressures.
Question 33
A 13-year-old boy with severe bilateral genu varum is shown. From a biomechanical standpoint, the primary goal of a corrective proximal tibial osteotomy is to realign the limb and restore a normal lever arm relationship. What is the primary objective of this realignment in relation to the ground reaction force?
View Answer & Explanation
Correct Answer: B
Rationale: The goal of a valgus-producing proximal tibial osteotomy for genu varum is to shift the mechanical axis from medial to the knee to a point that passes through the center or slightly lateral to the center of the knee. This neutralizes or slightly reverses the external adduction moment, thereby offloading the overloaded medial compartment and distributing forces more evenly across the joint. Shifting it far medial (distractor A) would worsen the pathology.
Question 34
A 9-year-old girl presents with a right limb length discrepancy and pelvic obliquity as seen in the clinical photo. To maintain a level gaze and upright posture, she may develop a compensatory deformity in the spine. What is the most likely spinal deformity to develop as a result of this uncorrected LLD?
View Answer & Explanation
Correct Answer: D
Rationale: A limb length discrepancy causes the pelvis to tilt down on the shorter side. To bring the torso back to a vertical position, the lumbar spine curves. This compensatory curve is typically flexible and convex toward the side of the shorter limb. This is a non-structural scoliosis because it will correct when the pelvic obliquity is corrected (e.g., by having the patient sit or by using a shoe lift). A curve convex to the long side (distractor E) would exacerbate the trunk imbalance.
Question 35
A 22-year-old male presents with the post-traumatic right ankle and foot deformity shown. The fixed equinovarus position alters the foot's function as a lever during gait. Specifically, it compromises the foot's ability to function as a rigid lever for propulsion. Which joint complex is critical for "locking" the midfoot to create this rigid lever?
View Answer & Explanation
Correct Answer: B
Rationale: During normal gait, as the heel rises and the subtalar joint inverts, the axes of the transverse tarsal joint (talonavicular and calcaneocuboid joints) become non-parallel. This "locks" the midfoot, transforming the foot from a flexible shock absorber into a rigid lever for efficient push-off. In a fixed varus (inverted) deformity, this dynamic locking mechanism is disrupted, impairing propulsive efficiency. The subtalar joint (distractor E) is key to initiating this process, but the transverse tarsal joint is what provides the midfoot rigidity.
Question 36
A 14-year-old boy is diagnosed with adolescent Blount's disease based on the radiographs shown. The characteristic depression and beaking of the posteromedial tibial physis leads to a multiplanar deformity. Besides varus, what other two deformities are typically present at the proximal tibia?
View Answer & Explanation
Correct Answer: C
Rationale: Blount's disease is a developmental disorder of the posteromedial proximal tibial physis. The growth suppression in this region leads to a characteristic triplanar deformity consisting of varus (frontal plane), procurvatum (flexion deformity in the sagittal plane), and internal tibial torsion (transverse plane). Understanding this multiplanar nature is crucial for complete surgical correction.
Question 37
A 16-year-old female with severe genu valgum undergoes a corrective distal femoral osteotomy. The goal is to realign the mechanical axis to pass through the center of the knee. This realignment primarily reduces the chronic tensile stress on which structure?
View Answer & Explanation
Correct Answer: C
Rationale: In genu valgum, the knee joint line is tilted, causing the lateral side to be compressed and the medial side to be under tension. The primary static stabilizer resisting this valgus force on the medial side is the Medial Collateral Ligament (MCL). A corrective varus-producing distal femoral osteotomy levels the joint line and neutralizes the valgus moment, thus reducing the chronic tensile strain on the MCL. The LCL (distractor D) is under tension in genu varum.
Question 38
A 10-year-old boy presents with the complex left tibial deformity shown. An external fixator is planned for gradual correction. According to Paley's principles, if an osteotomy is performed distal to the CORA and then angulated, what type of secondary deformity will be induced?
View Answer & Explanation
Correct Answer: C
Rationale: A fundamental rule of deformity correction is that angular correction at the level of the CORA results in pure angular correction without translation. If the osteotomy is performed away from the CORA, angulation will induce a secondary translational deformity. The farther the osteotomy is from the CORA, the greater the induced translation for a given amount of angular correction. This principle is critical for accurate surgical planning.
Question 39
A 17-year-old female with a 4 cm right tibial shortening is evaluated. She compensates with pelvic obliquity and right-sided equinus. This compensatory equinus posture alters ankle biomechanics during the stance phase. How does it affect the lever arm of the gastrocnemius-soleus complex?
View Answer & Explanation
Correct Answer: A
Rationale: A fixed equinus posture means the ankle is already plantarflexed at initial contact. The gastrocnemius-soleus complex is already in a shortened position, which places it on an unfavorable portion of the length-tension curve, reducing its force-generating capacity. Furthermore, the already-plantarflexed position reduces the available range of motion for powerful push-off, effectively impairing the function of the calf as a lever for propulsion.
Question 40
A 25-year-old male with a post-traumatic right foot equinovarus deformity is shown. This deformity creates an inefficient lever for push-off because the weight-bearing forces are concentrated on the lateral border of the foot. Which metatarsal is subjected to the highest stress and is most at risk for a stress fracture?
View Answer & Explanation
Correct Answer: E
Rationale: In an equinovarus foot, the hindfoot is inverted and the forefoot is adducted and supinated. During weight-bearing and push-off, the forces are transmitted along the lateral column of the foot instead of being distributed across the metatarsal heads. This concentrates significant stress on the base and shaft of the fifth metatarsal, predisposing it to stress fractures (e.g., Jones fracture) and chronic pain.
Question 41
A 14-year-old boy presents with the severe genu varum seen in the radiograph. The chronic medial compartment overload caused by the altered lever arm of the ground reaction force can lead to which of the following long-term consequences if left untreated?
View Answer & Explanation
Correct Answer: C
Rationale: Genu varum shifts the mechanical axis medially, concentrating joint reaction forces onto the medial tibial plateau and medial femoral condyle. This chronic overload, as described by the Hueter-Volkmann principle in skeletally immature patients and by mechanical wear in adults, leads to accelerated degeneration of the articular cartilage and the development of premature medial compartment osteoarthritis. The LCL (distractor A) is under increased tension but osteoarthritis occurs in the compressed compartment.
Question 42
A 16-year-old female with the genu valgum shown is being evaluated. In deformity analysis, a line is drawn from the center of the femoral head to the center of the ankle. In this patient, where would this line, representing the mechanical axis of the lower limb, pass relative to the knee joint?
View Answer & Explanation
Correct Answer: C
Rationale: The definition of genu valgum (knock-knee) is a condition where the mechanical axis of the lower extremity passes lateral to the center of the knee joint. This creates a valgus moment at the knee, compressing the lateral compartment and placing the medial structures under tension. A line passing medial to the knee (distractor A) defines genu varum.
Question 43
A 9-year-old girl with a right limb length discrepancy is shown. A common compensatory mechanism is vaulting, where the patient rises up on the toes of the contralateral (longer) limb during its swing phase. What is the primary purpose of this maneuver?
View Answer & Explanation
Correct Answer: C
Rationale: Vaulting is a gait compensation for relative or absolute limb length discrepancy. The patient performs an exaggerated plantarflexion of the stance limb (the longer or contralateral limb) during the swing phase of the affected (shorter) limb. This maneuver effectively lengthens the stance limb, raising the pelvis on that side to provide adequate clearance for the swinging limb to pass through without dragging its toe.
Question 44
A 15-year-old male presents with a progressive limp and right hip pain. Radiographs reveal a coxa vara deformity. An orthopedic surgeon explains that this deformity will have significant downstream effects. What is the most predictable consequence of an uncorrected proximal femoral varus deformity on the ipsilateral knee?
View Answer & Explanation
Correct Answer: B
Rationale: Coxa vara causes the femoral head to be displaced medially relative to the shaft. This shifts the entire mechanical axis of the limb medially, resulting in a medial Mechanical Axis Deviation (MAD) and subsequent overloading of the medial compartment of theknee, leading to premature osteoarthritis. Lateral compartment overloading (A) is characteristic of a coxa valga deformity.
Question 45
A 17-year-old female with cerebral palsy is evaluated for a scissoring gait. Radiographs demonstrate bilateral coxa valga. How does this proximal femoral deformity alter the mechanical axis of the lower extremity?
View Answer & Explanation
Correct Answer: B
Rationale: In coxa valga, the femoral head is displaced laterally relative to the femoral shaft. This pathological shift moves the entire mechanical axis laterally, creating a lateral Mechanical Axis Deviation (MAD) and overloading the lateral compartment of the knee. A medial MAD (A) is seen in coxa vara.
Question 46
During preoperative planning for a proximal femoral osteotomy, a surgeon is measuring key radiographic parameters. Which of the following is considered the cornerstone angle for surgical planning in the Paley method and has a normal value of approximately 90°?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that the Lateral Proximal Femoral Angle (LPFA) is the "absolute cornerstone angle for surgical planning in the Paley method." Its normal value is 90° (range 85° to 95°). The MPFA (B) is a useful adjunct, and the NSA (A) is a traditional but less precise measure for total limb alignment.
Question 47
A 12-year-old boy is diagnosed with developmental coxa vara. On physical examination, he demonstrates a significant Trendelenburg lurch. Which radiographic measurement best correlates with the clinical finding of abductor insufficiency?
View Answer & Explanation
Correct Answer: C
Rationale: A negative Articulo-Trochanteric Distance (ATD) signifies that the greater trochanter has migrated proximally to the level of the femoral head's superior articular surface. This reduces the lever arm and resting tension of the gluteus medius, leading to profound abductor insufficiency and a Trendelenburg lurch. While a decreased NSA (A) and LPFA (E) are characteristic of coxa vara, the ATD is the most direct indicator of abductor biomechanics.
Question 48
A surgeon is planning a proximal femoral osteotomy for a patient with a complex, multi-apical femoral deformity, making the mechanical axis difficult to delineate accurately. Which angle, based on the femoral anatomical axis, serves as a reliable secondary measure for planning the correction?
View Answer & Explanation
Correct Answer: B
Rationale: The text identifies the Medial Proximal Femoral Angle (MPFA) as a "highly useful adjunct measurement when the mechanical axis is difficult to determine." It is based on the femoral anatomical axis and has a normal value of 84° (range 80° to 89°). The LPFA (C) is the primary angle but relies on an identifiable mechanical axis.
Question 49
According to the principles of deformity correction outlined by Paley, what is the precise geometric definition of the Center of Rotation of Angulation (CORA)?
View Answer & Explanation
Correct Answer: B
Rationale: The CORA is rigorously defined as the geometric apex of the deformity, which is the exact point where the Proximal Mechanical Axis (PMA) and the Distal Mechanical Axis (DMA) intersect. While the CORA is in the center of the femoral head for developmental coxa vara (E), this is not true for all proximal femoral deformities, such as coxa valga.
Question 50
A pediatric orthopedist is explaining the etiology of developmental coxa vara to a resident. What is the underlying pathomechanical cause related to the proximal femoral physis?
View Answer & Explanation
Correct Answer: B
Rationale: Developmental coxa vara is caused by differential growth where the medial side (the femoral head physis) grows significantly slower than the lateral side (greater trochanteric physis). This leads to a relative overgrowth of the greater trochanter, driving the proximal femur into varus. Accelerated medial growth (A) would cause a valgus deformity.
Question 51
A 14-year-old is being treated for developmental coxa vara. For the purposes of surgical planning using the Paley method, where is the CORA for this deformity located?
View Answer & Explanation
Correct Answer: B
Rationale: As described in the text and shown in Figure (a) of the provided image, the CORA for developmental coxa vara is located in the center of the femoral head. This is because the deformity originates from a growth disturbance at the medial femoral neck physis. The CORA at the base of the greater trochanter (A) is characteristic of developmental coxa valga.
Question 52
A surgeon is planning a varus-producing osteotomy to correct a developmental coxa valga deformity in a 16-year-old. Based on the principles of physeal growth, where is the CORA for this specific deformity located?
View Answer & Explanation
Correct Answer: C
Rationale: Developmental coxa valga arises from slower growth of the lateral side of the physis (greater trochanteric apophysis). This places the epicenter of the deformity laterally. As shown in Figure (b) of the image, the CORA for developmental coxa valga is located at the base of the greater trochanter. The CORA is in the center of the femoral head (A) for coxa vara.
Question 53
A surgeon plans to perform a proximal femoral osteotomy exactly at the level of the CORA. According to Paley's Osteotomy Rule 1, what is the result of performing a pure angular correction at this specific location?
View Answer & Explanation
Correct Answer: A
Rationale: Paley's Rule 1 states that if an osteotomy is performed exactly at the level of the CORA, pure angular correction (hinging the bone) is sufficient to perfectly realign the mechanical axis without any unintended shifts or the need for translation. However, this is biologically untenable in the proximal femur.
Question 54
All proximal femoral osteotomies are performed distal to the CORA (e.g., intertrochanteric or subtrochanteric). Which of Paley's rules is therefore always in effect, and what does it mandate?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that because proximal femoral osteotomies are performed away from the CORA, Paley's Rule 2 is always in effect. This rule states that to prevent malalignment, the surgeon *must* introduce a deliberate translation at the osteotomy site simultaneously with the angulation. Translation is described as a "mandatory, mathematically required component."
Question 55
A 13-year-old with coxa vara is scheduled for a corrective valgus-producing osteotomy at the subtrochanteric level. To properly realign the mechanical axis, what translational maneuver must be performed on the distal femoral segment in addition to the angular correction?
View Answer & Explanation
Correct Answer: B
Rationale: To correct coxa vara, a valgus osteotomy is performed. The CORA is in the femoral head, and the osteotomy is far distal to it. According to the principles outlined, to realign the mechanical axis, the distal segment must be angulated into valgus and translated laterally. Medial translation (A) is required when correcting coxa valga.
Question 56
A 16-year-old with coxa valga undergoes a varus-producing intertrochanteric osteotomy. To achieve a neutral mechanical axis, what is the required direction of translation for the distal fragment?
View Answer & Explanation
Correct Answer: C
Rationale: The correction of coxa valga requires a varus-producing osteotomy. The CORA is at the base of the greater trochanter. Since the osteotomy is performed distal to this CORA, the distal segment must be angulated into varus and translated medially to restore the mechanical axis. Lateral translation (A, B) is used for correcting coxa vara.
Question 57
A surgeon is planning two separate proximal femoral osteotomies. The first is a subtrochanteric osteotomy for severe coxa vara. The second is an intertrochanteric osteotomy for mild coxa valga. Which statement accurately compares the magnitude of translation required for these two procedures?
View Answer & Explanation
Correct Answer: B
Rationale: The text states a key geometric rule: "the farther the osteotomy is from the CORA, the greater the magnitude of translation required." The CORA for coxa vara is high in the femoral head, making a subtrochanteric osteotomy very far away, thus requiring substantial lateral translation. The CORA for coxa valga is lower at the trochanteric base, making an intertrochanteric osteotomy relatively close, requiring less medial translation.
Question 58
What is the inherent effect of a valgus-producing proximal femoral osteotomy on overall femoral length?
View Answer & Explanation
Correct Answer: B
Rationale: A valgus osteotomy, used to correct coxa vara, takes a more horizontal femoral neck and makes it more vertical. This geometric shift inherently lengthens the femur. Conversely, a varus osteotomy (A) shortens the femur.
Question 59
A surgeon is performing a varus-producing osteotomy to correct coxa valga. What is the inherent effect of this specific osteotomy on femoral length?
View Answer & Explanation
Correct Answer: A
Rationale: A varus osteotomy, used to correct coxa valga, takes a more vertical femoral neck and makes it more horizontal. This geometric change inherently shortens the femur. A valgus osteotomy (B) lengthens the femur.
Question 60
A 16-year-old with cerebral palsy and coxa valga is scheduled for a corrective osteotomy. The surgeon plans a varus-producing osteotomy proximal to the lesser trochanter (intertrochanteric). What is the expected effect of this procedure on the iliopsoas tendon?
View Answer & Explanation
Correct Answer: B
Rationale: A varus osteotomy for coxa valga inherently shortens the femur and requires medial translation of the distal fragment. When performed intertrochanterically, the iliopsoas remains on the distal fragment. Both the shortening and the medial translation work together to relax the iliopsoas tendon, which is why this level is preferred for varus corrections.
Question 61
Based on the biomechanical principles of iliopsoas tension, what is the optimal level for performing a varus-producing osteotomy for the correction of coxa valga?
View Answer & Explanation
Correct Answer: B
Rationale: Varus osteotomies are best performed proximal to the lesser trochanter (intertrochanteric). This is because the procedure shortens the femur and medially translates the distal fragment, both of which relax the iliopsoas tendon (which remains attached to the distal fragment), preventing it from resisting the correction. A subtrochanteric level (A) is not ideal for this specific correction.
Question 62
A 14-year-old with developmental coxa vara requires a valgus-producing osteotomy. The surgeon considers an intertrochanteric osteotomy. What is the primary biomechanical disadvantage of performing this specific osteotomy at this level?
View Answer & Explanation
Correct Answer: B
Rationale: A valgus osteotomy for coxa vara inherently lengthens the femur and requires massive lateral translation of the distal fragment. If performed intertrochanterically, the iliopsoas remains on the distal fragment. Both the lengthening and the extreme lateral translation severely stretch the iliopsoas tendon, creating a powerful deforming force that can inhibit correction or cause displacement.
Question 63
To mitigate the deforming force of the iliopsoas tendon during the correction of coxa vara, what is the optimal level for performing the required valgus-producing osteotomy?
View Answer & Explanation
Correct Answer: A
Rationale: Valgus osteotomies are best performed distal to the lesser trochanter (subtrochanteric). At this level, the iliopsoas is attached to the proximal fragment. While the valgus angulation stretches the tendon, the proximal fragment's lesser trochanter moves medially, which offsets the stretch. The large lateral translation of the distal fragment has no effect on the tendon. The net effect is no change in psoas tension.
Question 64
A surgeon performs a subtrochanteric valgus osteotomy for coxa vara. How does this specific osteotomy level neutralize the tension of the iliopsoas tendon?
View Answer & Explanation
Correct Answer: C
Rationale: In a subtrochanteric osteotomy, the iliopsoas is on the proximal fragment. When this fragment is angulated into valgus, the lesser trochanter (its insertion point) moves medially. This medial shift counteracts the stretch caused by the verticalization of the neck (lengthening). The lateral translation of the distal fragment (B) does not affect the tendon. The osteotomy lengthens, not shortens (D).
Question 65
A 16-year-old male with a history of a healed slipped capital femoral epiphysis presents with right knee pain. On examination, he has a fixed varus deformity of the hip. Radiographs confirm a coxa vara with a mechanical Lateral Proximal Femoral Angle (mLPFA) of 75°. How does this proximal femoral deformity affect the mechanical axis at the level of the knee?
View Answer & Explanation
Correct Answer: B
Rationale: Coxa vara (decreased neck-shaft angle) lowers the femoral head relative to the shaft, which shifts the entire mechanical axis of the lower extremity medially. This medial shift overloads the medial compartment of the knee, resulting in a varus deformity downstream. Coxa valga would cause a lateral shift (valgus thrust).
Question 66
A 22-year-old female with a history of developmental dysplasia of the hip underwent a valgus-producing proximal femoral osteotomy. Two years later, she develops lateral knee pain. A standing long-leg radiograph reveals a mechanical axis that passes lateral to the center of the knee. Which proximal femoral deformity is the most likely cause of this finding?
View Answer & Explanation
Correct Answer: B
Rationale: Coxa valga, characterized by an increased neck-shaft angle, elevates the femoral head. This shifts the mechanical axis of the lower extremity laterally, causing a valgus deformity at the knee and overloading the lateral compartment. Coxa vara would cause a medial shift of the axis.
Question 67
A 45-year-old male is being evaluated for a complex lower extremity malalignment. The surgeon is performing a deformity analysis based on Paley's principles. What is the correct definition of the mechanical axis of the lower extremity?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis represents the true weight-bearing line of the lower extremity. By definition, it is the straight line drawn from the center of the femoral head to the center of the ankle mortise. The anatomic axis (A) follows the intramedullary canal and is different, especially in the femur.
Question 68
An orthopedic resident is planning a corrective osteotomy for a proximal femoral deformity. The attending surgeon emphasizes the importance of identifying the CORA. What is the geometric definition of the Center of Rotation of Angulation (CORA)?
View Answer & Explanation
Correct Answer: B
Rationale: The CORA is the geometric apex of a deformity. It is precisely located at the intersection of the axis of the bone proximal to the deformity and the axis of the bone distal to the deformity. Identifying the CORA is the critical first step in planning an accurate correction.
Question 69
A surgeon performs a subtrochanteric osteotomy to correct a varus deformity. The CORA was located in the intertrochanteric region, but the osteotomy was performed 4 cm distally. The correction hinge was placed at the osteotomy site, not at the CORA. According to Paley's principles, what is the most likely outcome?
View Answer & Explanation
Correct Answer: D
Rationale: This scenario describes a violation of Paley's osteotomy rules, specifically Rule 3, where both the osteotomy and the hinge are remote from the CORA. This always induces an unplanned and uncorrected secondary translation, creating a new deformity (often a "zigzag" deformity) and failing to properly realign the mechanical axis.
Question 70
A 30-year-old patient is being evaluated for hip pain. A standing AP radiograph of the pelvis and proximal femurs is obtained. The surgeon measures the angle between the mechanical axis of the femur and the joint line of the proximal femur. What is the name of this angle and its normal range?
View Answer & Explanation
Correct Answer: C
Rationale: The Mechanical Lateral Proximal Femoral Angle (mLPFA) is the primary angle for assessing varus or valgus of the proximal femur. It relates the mechanical axis to the proximal joint line, and its normal value is approximately 90° (range 85-95°). The NSA (B) relates the neck axis to the anatomic shaft axis.
Question 71
A 14-year-old with Blount's disease is undergoing a full lower extremity alignment assessment. Radiographic analysis of the left femur reveals a mechanical Lateral Proximal Femoral Angle (mLPFA) of 80°. What does this finding indicate?
View Answer & Explanation
Correct Answer: B
Rationale: The normal range for the mLPFA is 85° to 95°. A value less than 85°, such as 80°, indicates a varus deformity of the proximal femur, also known as coxa vara. A value greater than 95° would indicate coxa valga.
Question 72
A 50-year-old male has a malunion of a proximal femur fracture. When planning a corrective osteotomy, the surgeon measures the mechanical Lateral Proximal Femoral Angle (mLPFA). Which axes must be used to measure this angle accurately?
View Answer & Explanation
Correct Answer: B
Rationale: The mLPFA is defined by the angle between the mechanical axis of the femur (center of head to center of knee) and the joint orientation line of the proximal femur (a line across the base of the femoral head). Using the anatomic axis (C) would result in measuring the aLPFA, which can be misleading in a bowed femur.
Question 73
A 25-year-old female is evaluated for hip dysplasia. As part of the workup, the surgeon measures the Neck Shaft Angle (NSA) on an AP radiograph. What is the normal range for the NSA in an adult?
View Answer & Explanation
Correct Answer: D
Rationale: The Neck Shaft Angle (NSA), also known as the caput-collum-diaphyseal (CCD) angle, relates the axis of the femoral neck to the anatomic axis of the femoral shaft. The accepted normal range in adults is 124° to 136°, with a mean of approximately 130°.
Question 74
A 12-year-old patient with cerebral palsy presents with a scissoring gait and difficulty with perineal care. Radiographs demonstrate a Neck Shaft Angle (NSA) of 145°. This finding is best described as which deformity?
View Answer & Explanation
Correct Answer: D
Rationale: A Neck Shaft Angle greater than the normal upper limit (around 136°) is defined as coxa valga. This condition is common in non-ambulatory patients, such as those with cerebral palsy, due to the lack of normal physiologic varus stress on the proximal femur during development.
Question 75
A 55-year-old male with a severe proximal femoral varus deformity is being evaluated. The surgeon obtains a full-length standing radiograph and measures the Joint Line Convergence Angle (JLCA) of the knee. What is the primary clinical significance of an abnormal JLCA in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The JLCA measures the parallelism of the knee's articular surfaces. A normal JLCA is 0-2°. An increased JLCA indicates that the joint is "opening up" on one side due to ligamentous laxity or cartilage wear. This signals that the overall limb malalignment is not solely from the proximal femur but also has a component at the knee joint, which must be considered in the surgical plan.
Question 76
An orthopedic surgeon is reviewing a set of radiographs for a patient with multi-level lower limb deformity. To accurately assess the contribution of knee joint laxity to the overall malalignment, the Joint Line Convergence Angle (JLCA) must be measured. Which radiographic view is essential for a valid JLCA measurement?
View Answer & Explanation
Correct Answer: B
Rationale: The JLCA is a measure of joint space opening under load. Therefore, it must be measured on a weight-bearing radiograph to be valid. A non-weight-bearing view (A) would not demonstrate the effects of ligamentous laxity and would give a falsely normal or underestimated JLCA.
Question 77
A 40-year-old female presents with a painful gait and a suspected leg length discrepancy following a femoral fracture treated non-operatively 20 years ago. According to the principles of deformity analysis, what is the mandatory first step before drawing any lines on the femur?
View Answer & Explanation
Correct Answer: C
Rationale: The pelvis provides the foundational horizontal reference for the entire lower extremity. Establishing a reliable pelvic horizontal is the first and most critical step. A tilted pelvis can create an apparent limb malalignment or LLD that can mislead the entire surgical plan if not accounted for first.
Question 78
A 35-year-old patient with a history of a triple innominate osteotomy for hip dysplasia as a child is being evaluated for a femoral malunion. The surgeon needs to establish the most reliable horizontal reference line on a standing AP pelvis radiograph. Which landmarks are considered the gold standard in this scenario?
View Answer & Explanation
Correct Answer: D
Rationale: The inferior margins of the sacroiliac joints are considered the most stable and reliable landmarks for establishing the pelvic horizontal. They are robust and less likely to be affected by congenital dysplasia or prior pelvic osteotomies, which can significantly alter the height and shape of the iliac crests (A).
Question 79
A surgeon is planning a complex femoral osteotomy on a patient with developmental dysplasia of the hip (DDH). The surgeon notes that the iliac wings are asymmetric. Why is using a line connecting the top of the iliac crests to establish the pelvic horizontal potentially unreliable in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Pathologies like congenital pelvic dysplasia, as well as previous pelvic osteotomies, can lead to asymmetric growth and shape of the iliac wings. This asymmetry renders a line connecting the iliac crests inaccurate and unreliable for establishing a true horizontal reference for the pelvis.
Question 80
An 8-year-old child with a proximal femoral deformity is being evaluated. The surgeon is having difficulty visualizing the inferior SI joints clearly on the radiograph. Assuming no prior pelvic surgery, what is the most useful alternative landmark for establishing the pelvic horizontal in this pediatric patient?
View Answer & Explanation
Correct Answer: A
Rationale: In pediatric patients, the triradiate cartilages of the acetabulum are excellent, reliable landmarks for establishing the pelvic horizontal, provided no pelvic osteotomy has altered their relationship. Sacral foramina (E) are also a valid alternative, but the triradiate cartilages are often more distinct and centrally located in this age group.
Question 81
A 28-year-old patient presents with a chief complaint of a "short leg." On a standing AP radiograph, the line connecting the inferior SI joints is parallel to the floor, but the right femoral head is 2 cm lower than the left. This finding is most consistent with which condition?
View Answer & Explanation
Correct Answer: D
Rationale: When the pelvic horizontal line is parallel to the floor, the pelvis is level. If the legs are of unequal length in this state, it indicates a true, structural leg length discrepancy originating from the bones of the lower extremity. If the pelvis were tilted (B), it would be a compensatory obliquity to level the head and shoulders.
Question 82
A 50-year-old male is evaluated for back pain and a limp. On physical examination, he has a fixed adduction contracture of his right hip. A standing radiograph shows that the pelvis is tilted down on the left side. What is the most likely cause of this pelvic obliquity?
View Answer & Explanation
Correct Answer: C
Rationale: A fixed adduction contracture of the hip forces the pelvis to tilt upwards on the affected side to allow the foot to be placed on the ground, resulting in an apparent lengthening of that limb. This is a form of fixed pelvic obliquity driven by a soft tissue contracture, not by a true LLD (B), which would cause the pelvis to tilt down on the short side.
Question 83
A 45-year-old male is undergoing correction of a tibial malunion. The surgeon is deciding between external fixation and intramedullary nailing (IMN). According to the principles of modern deformity correction, which of the following is a primary advantage of choosing IMN over a fine-wire external fixator?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that intramedullary nailing offers profound advantages, including the "complete elimination of pin-tract infections," which is a major source of morbidity with external fixation. Postoperative adjustments (A) are a key feature of external fixators, not IMN. IMN requires more rigorous preoperative planning (D), not less.
Question 84
A 28-year-old female has a femoral varus malunion corrected with an intramedullary nail. Postoperatively, a small residual varus deformity is noted. Compared to a correction performed with a Taylor Spatial Frame (TSF), what is the primary limitation in managing this residual deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that with IMN, the correction is dictated entirely by preoperative planning and the rigid trajectory of the hardware. Unlike an external fixator where residual deformities can be "tweaked and dialed in postoperatively," the alignment achieved with an IMN is fixed once the surgery is complete. IMN provides robust stability (A).
Question 85
A 33-year-old male undergoes an osteotomy and intramedullary nailing for a tibial valgus deformity. During the procedure, the nail is passed across the osteotomy site. Which principle best describes the mechanism by which the bone segments achieve their final alignment?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text states, "The nail acts as an internal template; the bone will inevitably conform to its shape." This is the fundamental principle of IMN in deformity correction. The other options describe factors that are either secondary or incorrect for this specific mechanism.
Question 86
A surgeon is performing preoperative planning for a femoral malunion that will be corrected with an intramedullary nail. To determine the Center of Rotation of Angulation (CORA) for this procedure, which method is considered mandatory?
View Answer & Explanation
Correct Answer: B
Rationale: The text is unequivocal: "when planning for IMN fixation, the anatomic axis method is vastly superior and absolutely mandatory." This is because the nail physically occupies and follows the anatomic axis (the medullary canal). The mechanical axis method (A) is used for overall limb alignment planning, especially with external fixators, but not for determining the IMN trajectory.
Question 87
A 50-year-old male presents with a tibial malunion. A resident asks why the anatomic axis method is preferred over the mechanical axis method for planning the correction with an intramedullary nail. What is the most accurate explanation?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that an intramedullary nail is a physical object that "must follow the path of least resistance within the medullary canal—it inherently follows the mid-diaphysis (the anatomic axis)." Therefore, all planning must be based on the path the nail will actually take.
Question 88
A 22-year-old female is being evaluated for genu varum. Preoperative planning requires identification of the mechanical axis of the lower limb. How is this axis correctly defined?
View Answer & Explanation
Correct Answer: C
Rationale: The text provides a precise definition: "The mechanical axis of the lower limb is a straight line drawn from the center of the femoral head to the center of the ankle joint (the center of the tibial plafond)." The other options describe the anatomic axis (A, B) or are incorrect definitions.
Question 89
A 41-year-old male has a femoral malunion. During preoperative planning for intramedullary nailing, the surgeon identifies the anatomic axis of the femur. What does this axis represent?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the anatomic axis as "the mid-diaphyseal line of the bone. It is the physical center of the medullary canal." The line of weight-bearing (A) refers to the mechanical axis.
Question 90
A surgeon is planning an osteotomy and intramedullary nailing for a proximal tibial varus deformity. What is the geometric relationship between the mechanical and anatomic axes in the tibia?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "In the tibia, the mechanical axis and the anatomic axis are parallel (though not collinear...)." This is a crucial distinction from the femur, where the axes are angled relative to each other.
Question 91
A 30-year-old patient undergoes a 4 cm tibial lengthening using the Lengthening Over Nail (LON) technique. Based on the biomechanical principles of the tibia, what is the expected effect of this procedure on the overall mechanical alignment of the limb?
View Answer & Explanation
Correct Answer: C
Rationale: Because the anatomic and mechanical axes of the tibia are parallel, lengthening the tibia along its anatomic axis (the path of the nail) does not alter the mechanical alignment. The text confirms this: "correcting a deformity or lengthening the tibia strictly along its anatomic axis does not alter the overall mechanical alignment of the limb."
Question 92
A 25-year-old female requires a 5 cm femoral lengthening. The surgeon is explaining the biomechanical challenges to the resident. What is the fundamental geometric difference between the femur and the tibia that makes femoral lengthening more complex?
View Answer & Explanation
Correct Answer: C
Rationale: The text highlights this as the critical difference: "In the femur, the biomechanics are vastly different and far more complex. The anatomic axis of the femur sits at an angle—typically 6 to 9 degrees—to the mechanical axis." This angle, the AMA, is the source of alignment changes during femoral lengthening.
Question 93
During preoperative planning for a femoral deformity correction, the surgeon measures the angle between the mid-diaphyseal line of the femur and the line from the center of the femoral head to the center of the knee. What is this angle called?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines the angle between the anatomic axis (mid-diaphyseal line) and the mechanical axis of the femur as the "Anatomic-Mechanical Angle (AMA)." This is a key concept in understanding the effects of femoral nailing and lengthening.
Question 94
A 38-year-old male is scheduled for a femoral osteotomy and intramedullary nailing. The surgeon notes a normal Anatomic-Mechanical Angle (AMA). What is the primary implication of this angle when lengthening the femur along the path of an intramedullary nail?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that due to the AMA, "If you lengthen a femur along its anatomic axis (the path of the IMN), the distal fragment will translate laterally relative to the proximal fragment's mechanical axis line." This lateral translation of the knee joint creates a valgus effect.
Question 95
A 42-year-old patient develops an iatrogenic valgus malunion after intramedullary nailing of a femur fracture. According to the principles discussed, what is the single most common cause of such a failure?
View Answer & Explanation
Correct Answer: C
Rationale: The text is explicit: "The single most common cause of failure, malunion, or iatrogenic deformity in IMN deformity correction is the selection of incorrect starting (entry) and ending (terminal) points." The other options are potential technical errors but are not cited as the most common cause of malalignment.
Question 96
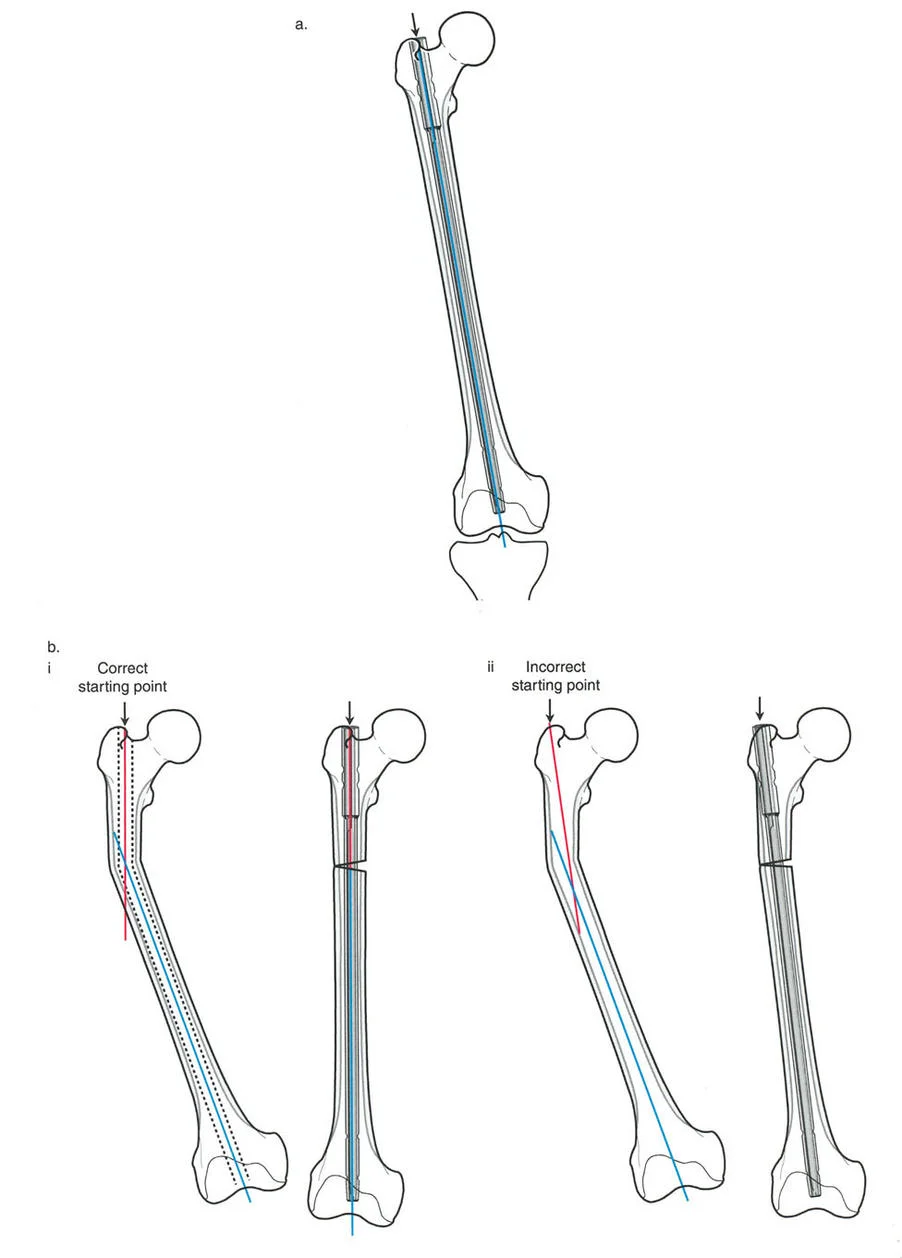
A surgeon is preparing to perform an antegrade intramedullary nailing for a mid-shaft femoral deformity. To ensure a trajectory that is collinear with the true anatomic axis of the femoral shaft, what is the correct starting point for a standard nail?
View Answer & Explanation
Correct Answer: C
Rationale: The text and the accompanying image clearly state that for a standard antegrade femoral nail, the correct starting point is the piriformis fossa, as it "offers a more collinear trajectory with the true anatomic axis of the femoral shaft." A lateral starting point (A) is explicitly shown to be incorrect for this type of nail and will induce a varus deformity.
Question 97
A 35-year-old male with a femoral shaft fracture is treated with an antegrade intramedullary nail designed for piriformis entry. However, the surgeon initiates the entry portal on the lateral tip of the greater trochanter. What is the most likely iatrogenic deformity that will result?
View Answer & Explanation
Correct Answer: B
Rationale: As illustrated in the provided image and explained in the text, a starting point that is too lateral forces the proximal segment into varus relative to the nail. When the nail is then passed distally, this results in an overall residual varus malalignment of the limb.
Question 98
A 29-year-old patient has a 10-degree varus malunion of the proximal femur. The surgeon plans correction with an osteotomy and a piriformis-entry intramedullary nail. During the procedure, the starting point is inadvertently made on the greater trochanter. The nail is passed and locked. What is the most probable postoperative outcome?
View Answer & Explanation
Correct Answer: C
Rationale: The incorrect lateral starting point induces a varus force on the proximal fragment. This iatrogenic varus counteracts the intended corrective effect of the procedure. Therefore, the preoperative varus deformity will not be fully corrected, and a residual varus will remain.
Question 99
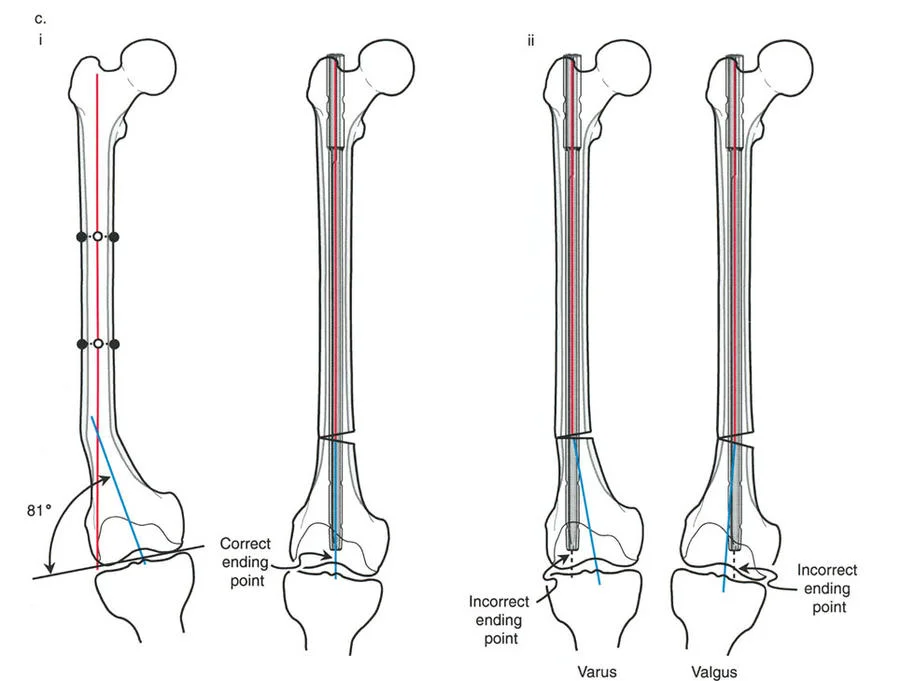
A surgeon is performing an intramedullary nailing for a distal third femoral deformity. To achieve a normal mechanical lateral distal femoral angle (mLDFA), where should the tip of the nail be positioned on the AP fluoroscopic view?
View Answer & Explanation
Correct Answer: C
Rationale: The text and image emphasize that the correct ending point for a femoral nail is "at the exact center of the femoral condyles (in both the coronal and sagittal planes)." On an AP view, this corresponds to the center of the intercondylar notch. This ensures the distal anatomic axis is correctly aligned.
Question 100
A 48-year-old female undergoes correction of a distal femoral valgus deformity with an intramedullary nail. Intraoperatively, the surgeon notes on the final AP fluoroscopy that the nail tip is positioned in the center of the medial femoral condyle. What is the expected final alignment?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "If the nail ends too medially, it forces the distal segment into varus." By ending in the medial condyle instead of the center, the nail pushes the distal fragment medially, creating an iatrogenic varus deformity.
