Mastering Lower Extremity Deformity Correction & Biomechanics: ABOS Review | Part 9
Key Takeaway
Lower extremity deformity correction involves precise analysis of alignment using angles like mLDFA, MPTA, and MAD. Principles by Paley guide interventions such as guided growth for pediatric cases and osteotomies or TKA for adults. Key aspects include understanding biomechanics, gait, and balancing soft tissues to restore optimal function and prevent long-term complications.
Question 1
According to the principles of deformity correction popularized by Paley, what is the most important radiographic line for assessing lower extremity alignment and planning correction?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis, a straight line from the center of the femoral head to the center of the ankle talus, is the cornerstone of lower extremity alignment analysis. The goal of deformity correction is to realign this axis so it passes through the center of the knee joint, thereby normalizing joint loading.
Question 2
A 10-year-old boy has a predicted leg length discrepancy of 4 cm at skeletal maturity, with the right leg being shorter. His skeletal age is 11 years. According to the Paley multiplier method, what is the most appropriate management strategy?
View Answer & Explanation
Correct Answer: D
Rationale: A predicted 4 cm LLD is significant and warrants intervention. The Paley multiplier method is used to calculate the precise timing for an epiphysiodesis of the longer (contralateral) limb to arrest its growth, allowing the shorter limb to catch up by skeletal maturity. Performing it too early (C) would result in overcorrection (making the left leg shorter).
Question 3
A surgeon is performing a medial distal femoral hemiepiphysiodesis for genu valgum. After inserting the metaphyseal screw, what is the most critical step to ensure proper placement of the epiphyseal screw?
View Answer & Explanation
Correct Answer: C
Rationale: The most critical aspect of the technique is to avoid iatrogenic injury to the physis. Both screws must be confirmed to be purely metaphyseal and epiphyseal, respectively, without crossing or damaging the growth plate. This is typically confirmed with AP and lateral fluoroscopic views. Angling away from the joint (B) is also important, but avoiding physeal damage is paramount.
Question 4
An 11-year-old girl undergoes guided growth for genu valgum. Six months postoperatively, her alignment is corrected to neutral. Her parents ask when the plates should be removed.
View Answer & Explanation
Correct Answer: B
Rationale: Due to the phenomenon of "rebound growth," where the deformity tends to recur after implant removal, it is common practice to slightly overcorrect the alignment before removing the hardware. For genu valgum, correcting to neutral and then allowing it to drift into a few degrees of varus helps ensure the final alignment at maturity will be neutral. Removing immediately at neutral (A) risks recurrence of valgus.
Question 5
What is the most common complication associated with the use of eight-Plates for guided growth?
View Answer & Explanation
Correct Answer: C
Rationale: While all are potential complications, hardware-related issues are the most frequently reported. Screw breakage, loosening, or pullout can occur due to the dynamic forces across the physis. Physeal bar formation (A) is rare with this technique compared to older methods like stapling. Rebound (E) is a phenomenon, not a direct complication of the implant itself.
Question 6
A 14-year-old boy is noted to have a 2.5 cm leg length discrepancy. His skeletal age is 15.5 years. His physes are still open but will close soon. What is the most appropriate treatment to equalize leg lengths at maturity?
View Answer & Explanation
Correct Answer: C
Rationale: For a 2.5 cm discrepancy in a patient with limited but remaining growth, a contralateral (longer leg) epiphysiodesis is the treatment of choice. It is a relatively minor procedure that can correct discrepancies between 2 and 5 cm by arresting the growth of the longer limb. Lengthening (B) is too invasive for this amount of LLD. A shoe lift (E) is a non-operative option but does not correct the underlying discrepancy.
Question 7
The Paley multiplier method for predicting limb length at maturity is based on which of the following principles?
View Answer & Explanation
Correct Answer: B
Rationale: The multiplier method simplifies LLD prediction by using multipliers derived from the known, predictable percentages of growth remaining in the femur and tibia at different skeletal ages. By multiplying the current LLD by the appropriate multiplier, one can project the LLD at maturity. It relies on skeletal age, not chronological age (C), and acknowledges that growth is not linear (A).
Question 8
A 10-year-old boy presents with bilateral genu varum. A standing full-length radiograph is obtained. To assess the overall limb alignment, a line is drawn from the center of the femoral head to the center of the ankle. In this patient, the line passes 25 mm medial to the center of the knee. What does this measurement represent?
View Answer & Explanation
Correct Answer: D
Rationale: The Mechanical Axis Deviation (MAD) is defined as the distance between the mechanical axis (femoral head center to ankle center) and the center of the knee. A medial deviation indicates varus alignment. The other options are specific joint orientation angles or biomechanical points, not the overall limb alignment measurement.
Question 9
A 12-year-old girl is evaluated for genu valgum. Her full-length standing radiograph reveals a Mechanical Lateral Distal Femoral Angle (mLDFA) of 78°. The Medial Proximal Tibial Angle (MPTA) is 88°. Based on these findings, what is the primary anatomical source of her deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The normal mLDFA is 85-90°. An angle less than 85° indicates distal femoral valgus. Her MPTA of 88° is within the normal range (85-90°), ruling out a primary tibial deformity. Therefore, the source of her genu valgum is the distal femur.
Question 10
A 9-year-old boy presents with bowlegs. Radiographic analysis shows a Mechanical Axis Deviation (MAD) of 30 mm medial. His mLDFA is 89°, and his MPTA is 80°. Which guided growth procedure would most appropriately address the apex of his deformity?
View Answer & Explanation
Correct Answer: D
Rationale: The patient has genu varum. The MPTA of 80° is less than the normal 85-90°, indicating tibial varus. The mLDFA of 89° is normal. To correct tibial varus, growth on the lateral side of the proximal tibial physis must be tethered. Medial tethering (C) would worsen the varus deformity.
Question 11
According to the principles outlined by Dr. Dror Paley, where is the Center of Rotation of Angulation (CORA) typically located in developmental angular deformities of the pediatric lower limb?
View Answer & Explanation
Correct Answer: C
Rationale: A critical anatomical principle for guided growth is that in developmental deformities, the CORA is located at the level of the physis. This allows a hemi-epiphysiodesis implant, which acts as a hinge at the physis, to correct the deformity without inducing translation.
Question 12
A surgeon is planning a guided growth procedure for a 7-year-old with 15° of genu valgum originating from the distal femur. The width of the distal femoral physis (r) is measured to be 60 mm. Using the formula ε = (r * α) / 57, how much longitudinal growth (ε) is required on the untethered side of the physis to achieve full correction?
View Answer & Explanation
Correct Answer: C
Rationale: The calculation is ε = (60 mm * 15°) / 57. This equals 900 / 57, which is approximately 15.8 mm. This formula is essential for predicting the amount of growth needed for correction, which in turn helps time the hardware removal.
Question 13
A 13-year-old girl with significant genu valgum is evaluated. Her standing radiograph shows that the distal femoral joint line and the proximal tibial joint line are not parallel, converging medially by 4°. What is this measurement called, and what might it suggest?
View Answer & Explanation
Correct Answer: C
Rationale: The Joint Line Convergence Angle (JLCA) is the angle between the distal femoral and proximal tibial joint lines. A normal JLCA is 0-2°. An angle greater than 2° can indicate issues within the joint itself, such as ligamentous laxity or cartilage wear, rather than a primary bony deformity.
Question 14
A senior surgeon is mentoring a resident on timing a permanent epiphysiodesis for a 14-year-old boy. The senior surgeon pulls out a set of charts plotting remaining growth against skeletal age. Which historical method is being referenced?
View Answer & Explanation
Correct Answer: C
Rationale: The foundational work by Anderson, Green, and Messner, later adapted into nomograms by Bowen and others, established the use of growth remaining charts based on skeletal age. The image displays these classic charts. The Paley Multiplier Method was developed to replace this system.
Question 15
A major advantage of the Paley Multiplier Method over historical growth prediction models is its elimination of the need for which of the following?
View Answer & Explanation
Correct Answer: D
Rationale: The Paley Multiplier Method uses age- and gender-specific coefficients, eliminating the need for subjective and variable skeletal age assessments (e.g., Greulich and Pyle atlas). This significantly improves the accuracy and reproducibility of growth prediction.
Question 16
Paley's Osteotomy Rule #1 states that to correct an angular deformity without inducing a secondary translation, the hinge of correction must be placed at the CORA. How does a properly placed hemi-epiphysiodesis plate (e.g., an 8-plate) adhere to this rule?
View Answer & Explanation
Correct Answer: B
Rationale: The genius of guided growth for developmental deformities is that the CORA is at the physis. By placing an implant across the physis, the implant's hinge of action is perfectly aligned with the deformity's CORA, allowing for pure angular correction without iatrogenic translation.
Question 17
An 11-year-old girl presents with knock-knees. A standing radiograph is ordered to assess her lower extremity alignment. To ensure an accurate measurement of her mLDFA and MPTA, what is the most critical aspect of patient positioning for the radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: Rotational malalignment can significantly alter the projected angles on a 2D radiograph, potentially masking or exaggerating an angular deformity. Ensuring the patellae are pointing straight ahead provides a true anteroposterior view of the knee, which is essential for accurate measurement of joint orientation angles.
Question 18
A 6-year-old boy is undergoing guided growth for 20° of proximal tibial varus. The surgeon has calculated that 18 mm of lateral physeal growth is required for correction. The Paley Multiplier Method is used to predict that this will take 18 months. What is the most critical clinical question this method helps answer for this young patient?
View Answer & Explanation
Correct Answer: D
Rationale: A key limitation of historical methods was their focus on permanent epiphysiodesis. The Paley Multiplier Method is exceptionally useful for temporary guided growth in young children because it allows for precise prediction of when to remove the hardware to halt the correction at neutral, avoiding an iatrogenic overcorrection into valgus.
Question 19
In the geometric model of guided growth, the process is analogized to a circular sector. What anatomical structure or implant component represents the center of the circle in this model?
View Answer & Explanation
Correct Answer: C
Rationale: In the geometric model, the implant (staple or plate) tethers one side of the physis, creating a fixed hinge. This hinge acts as the center of the circle around which the untethered side of the physis grows, creating a wedge of new bone.
Question 20
A resident is calculating the required growth (ε) for a deformity correction using the formula ε = (r * α) / 57. The constant '57' is a clinically simplified value. From what mathematical expression is this constant derived?
View Answer & Explanation
Correct Answer: D
Rationale: The full formula for arc length is ε = 2πr(α/360). This can be rearranged to ε = (r * α) * (2π/360). The term (2π/360) simplifies to approximately 1/57.3. For clinical ease, the formula is written as ε = (r * α) / 57. Therefore, 57 is derived from 360 / 2π.
Question 21
An 8-year-old girl with the clinical appearance of knock-knees is being evaluated. Her standing radiograph shows a mechanical axis that passes 20 mm lateral to the center of the knee. What is the correct terminology for this finding?
View Answer & Explanation
Correct Answer: B
Rationale: Genu valgum (knock-knees) is characterized by a mechanical axis that passes lateral to the center of the knee. The distance of this deviation is the Mechanical Axis Deviation (MAD). Therefore, a lateral MAD corresponds to a valgus deformity. A medial MAD (distractor E) corresponds to varus.
Question 22
A 14-year-old boy has a 10° varus deformity originating from the proximal tibia. The surgeon plans a lateral proximal tibial hemi-epiphysiodesis. If the surgeon misplaces the implant and creates the corrective hinge in the metaphysis instead of at the physis, what iatrogenic deformity is likely to occur in addition to the angular correction?
View Answer & Explanation
Correct Answer: C
Rationale: This question tests Paley's Osteotomy Rule #1. The CORA for this deformity is at the physis. By placing the hinge of correction (the implant) away from the CORA (in the metaphysis), a secondary translational deformity will be created as the angular correction occurs.
Question 23
A surgeon measures the Medial Proximal Tibial Angle (MPTA) on a standing radiograph. Which two lines are used to form this angle?
View Answer & Explanation
Correct Answer: B
Rationale: The MPTA is a critical joint orientation angle that defines the alignment of the proximal tibia. It is measured as the medial angle between the mechanical axis of the tibia and the joint line of the proximal tibia (the tibial plateau).
Question 24
A 10-year-old boy has a valgus deformity of his left knee. Radiographic measurements are: mLDFA = 76°, MPTA = 92°, JLCA = 1°. Where are the sites of deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The normal mLDFA is 85-90°; 76° indicates significant femoral valgus. The normal MPTA is 85-90°; 92° indicates tibial valgus. Since both angles are outside the normal range and contribute to the overall valgus alignment, the deformity originates from both the distal femur and proximal tibia.
Question 25
One of the major limitations of the historical growth charts, such as those by Anderson and Green, was their reliance on growth percentiles. Why was this a clinical problem?
View Answer & Explanation
Correct Answer: C
Rationale: The standard curves on the charts represented the average (50th percentile) grower. A child on a lower or higher growth percentile has significantly different amounts of growth remaining than the average, making predictions based on the standard curves inaccurate for these outliers.
Question 26
A surgeon is planning to correct a 10° varus deformity in a proximal tibia with a physeal width (r) of 55 mm. Using the formula ε = (r * α) / 57, the required growth (ε) is calculated to be 9.6 mm. If the patient's predicted growth rate at the proximal tibia is 6 mm/year, approximately how long should the implant remain in place?
View Answer & Explanation
Correct Answer: D
Rationale: This is a two-step problem. First, the required growth is 9.6 mm. Second, the time required is the total growth needed divided by the growth rate: Time = 9.6 mm / 6 mm/year = 1.6 years. 1.6 years is approximately 19 months (1.6 * 12).
Question 27
What is the primary biomechanical consequence of a varus malalignment where the mechanical axis passes medial to the knee?
View Answer & Explanation
Correct Answer: C
Rationale: In varus (bow-legged) alignment, the weight-bearing line is shifted medially. This concentrates mechanical stress on the medial compartment of the knee, which can lead to accelerated cartilage wear and early-onset medial compartment osteoarthritis.
Question 28
A 10-year-old girl has a 12° valgus deformity of the knee. The surgeon determines the deformity is entirely within the distal femur (mLDFA = 77°). To correct this, where should a hemi-epiphysiodesis plate be placed?
View Answer & Explanation
Correct Answer: A
Rationale: A valgus deformity of the femur means the medial side of the physis is growing faster or is longer than the lateral side. To correct this, the growth on the medial side must be tethered or slowed, allowing the lateral side to "catch up" and straighten the limb. Placing the plate laterally (B) would worsen the valgus.
Question 29
The landmark used to define the proximal point of the lower extremity mechanical axis is the center of which structure?
View Answer & Explanation
Correct Answer: B
Rationale: The mechanical axis of the lower extremity, representing the true weight-bearing line, is defined by a straight line from the center of the femoral head to the center of the ankle (tibial plafond). The anatomical axis of the femur, in contrast, follows the intramedullary canal.
Question 30
A 9-year-old boy has a varus deformity. His mLDFA is 94° and his MPTA is 88°. What is the source of his deformity?
View Answer & Explanation
Correct Answer: A
Rationale: The normal mLDFA is 85-90°. An angle greater than 90° indicates distal femoral varus. The MPTA of 88° is within the normal range. Therefore, the deformity originates from the distal femur.
Question 31
A 58-year-old male presents with worsening left medial knee pain and a varus thrust gait. Physical examination reveals tenderness over the medial joint line and stable ligaments. A standing long-leg radiograph demonstrates isolated medial compartment osteoarthritis (MCOA) with a mechanical axis deviation (MAD) of 20 mm medial to the center of the knee. When planning a high tibial osteotomy (HTO), what is the typical target for postoperative alignment to optimize outcomes for MCOA?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that for medial compartment osteoarthritis (MCOA), the alignment is typically overcorrected into some degree of valgus to offload the diseased medial compartment. In contrast, lateral compartment osteoarthritis (LCOA) is corrected only to a neutral MAD. Neutral correction for MCOA would be insufficient to unload the medial compartment effectively.
Question 32
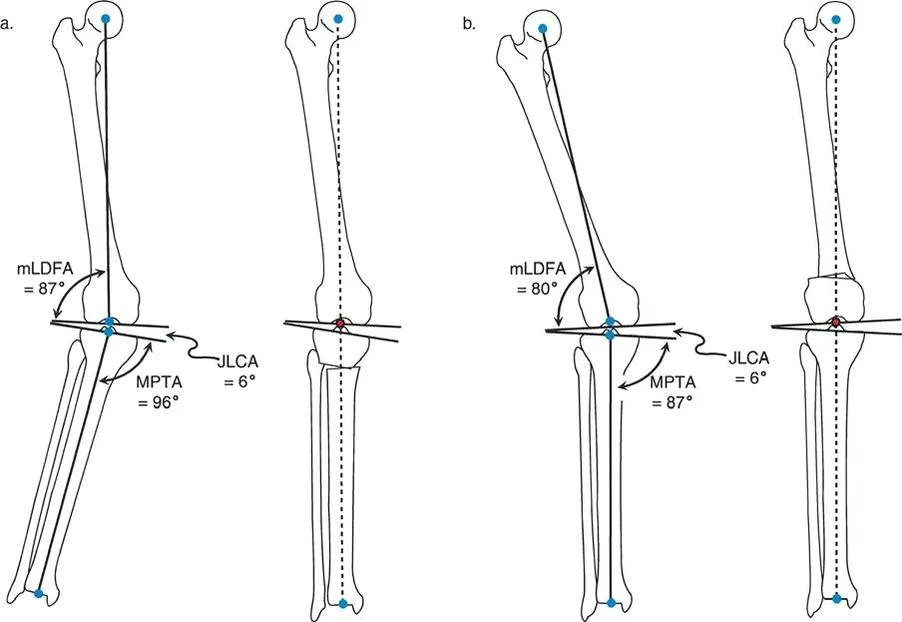
A 52-year-old female with lateral compartment osteoarthritis (LCOA) and a valgus deformity is scheduled for a realignment osteotomy. Her preoperative mLDFA is 80° and MPTA is 87°. The surgeon plans a distal femoral varus osteotomy. What is the recommended postoperative mechanical axis deviation (MAD) for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that LCOA should be corrected to a neutral MAD only (MAD of 0 mm). This is in contrast to MCOA, which is overcorrected into valgus. Overcorrecting LCOA into varus would overload the medial compartment, which is undesirable.
Question 33
A 48-year-old male undergoes a 12° acute closing wedge proximal tibial osteotomy to correct a valgus deformity associated with LCOA. Intraoperatively, the surgeon notes tension on the peroneal nerve after correction. According to the provided text, what is the most appropriate next step to mitigate the risk of nerve injury?
View Answer & Explanation
Correct Answer: C
Rationale: The text advises that for larger acute valgus-to-varus corrections of the tibia, prophylactic peroneal nerve decompression and anterior compartment fasciotomy are advisable to decrease the risk of peroneal nerve palsy and compartment syndrome. Simply monitoring postoperatively ignores a significant intraoperative warning sign.
Question 34
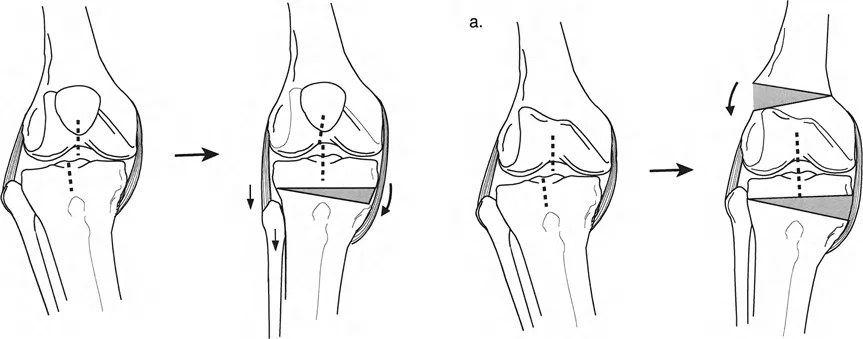
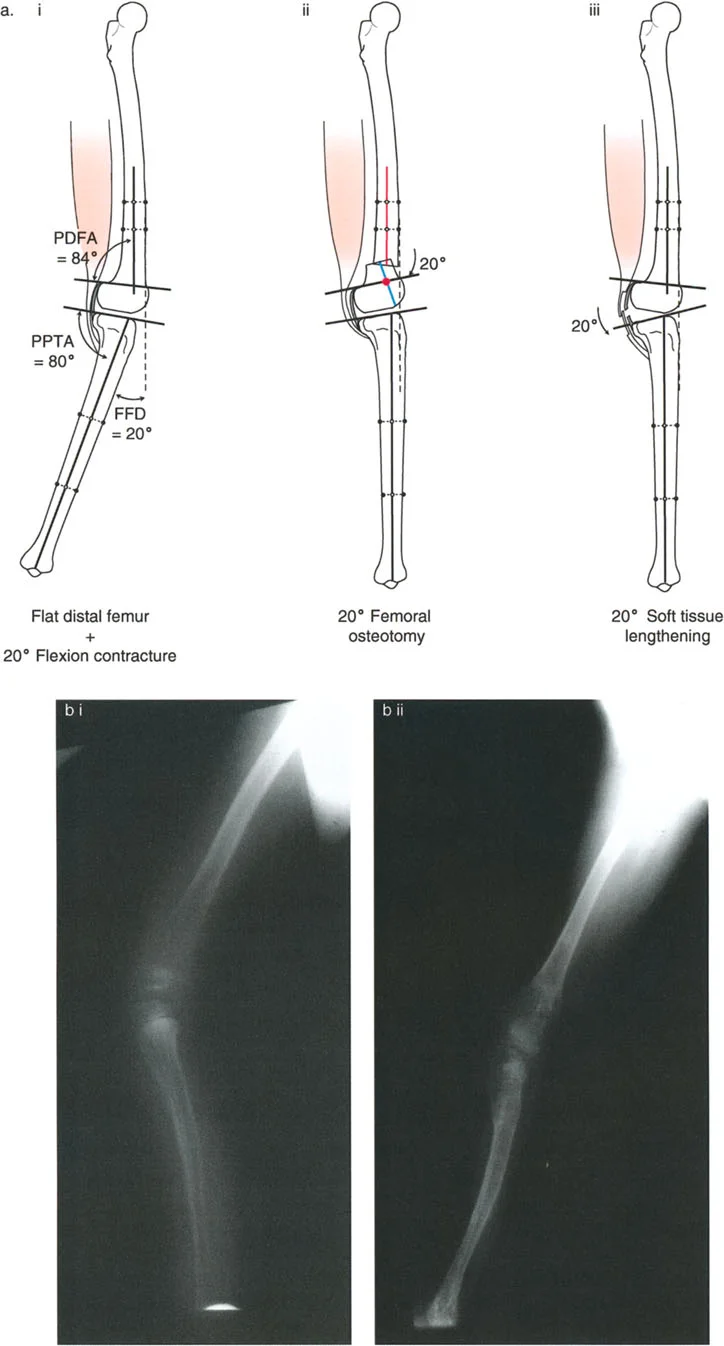
A 60-year-old female with MCOA presents with a varus deformity and a concomitant 15° fixed flexion deformity (FFD). A long lateral radiograph reveals a proximal posterior tibial angle (PPTA) of 71°. The surgeon plans a valgus-producing opening wedge HTO. What is the target postoperative PPTA to correct the FFD?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that when correcting a varus deformity associated with procurvatum (flexion deformity), the tibia may be corrected to a PPTA of up to 90°. Overcorrection beyond 90° is not recommended because it eliminates the natural bone stop to deceleration of the femur during gait. The image provided shows a case where the PPTA was overcorrected to 90° to fully correct the flexion deformity.
Question 35
A 55-year-old male with MCOA has a varus deformity and a significant external tibial torsion deformity, causing patellofemoral maltracking. The surgeon plans a valgus and internal rotation osteotomy of the proximal tibia. To facilitate rotational correction, which osteotomy configuration is most useful?
View Answer & Explanation
Correct Answer: C
Rationale: The text indicates that it is difficult to rotate the bone ends when the osteotomy is above the tuberosity due to the large surface area. To facilitate rotation and maximize room for fixation, an L-shaped osteotomy is useful. This type of osteotomy, as shown in the associated figure, allows for both realignment and rotational correction.
Question 36
A 65-year-old male presents with MCOA, varus deformity, and lateral tibial subluxation. Radiographs reveal a valgus distal femur (mLDFA 81°) and a varus proximal tibia (MPTA 83°), consistent with a "bad pattern." According to the text, what is the preferred surgical strategy to reduce the subluxation and realign the limb?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that "probably the best way to treat lateral subluxation is varus osteotomy of the femur combined with valgus osteotomy of the tibia." This combination of osteotomies is indicated by the "bad pattern" deformity and effectively reduces the subluxation by creating a "good pattern" of an inclined knee joint.
Question 37
A 22-year-old patient presents with a 20° fixed flexion deformity (FFD) of the knee. A long lateral radiograph shows a posterior distal femoral angle (PDFA) of 64° and a proximal posterior tibial angle (PPTA) of 80°. Based on these measurements, where is the primary source of the deformity?
View Answer & Explanation
Correct Answer: B
Rationale: A normal PDFA is approximately 83-84°. A PDFA of 64° indicates a 20° procurvatum (flexion) deformity of the distal femur. Since the PPTA is normal (80°), the entire 20° FFD is attributable to the bony deformity in the distal femur. A soft tissue contracture would be present if the joint orientation angles were normal.
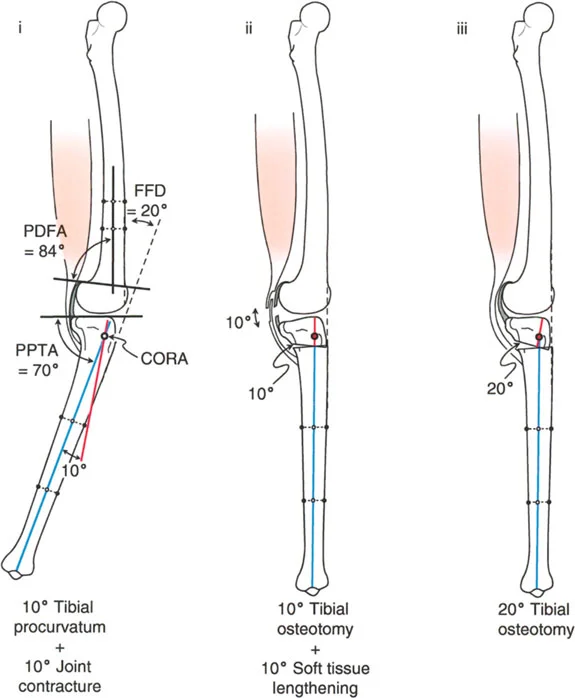
Question 38
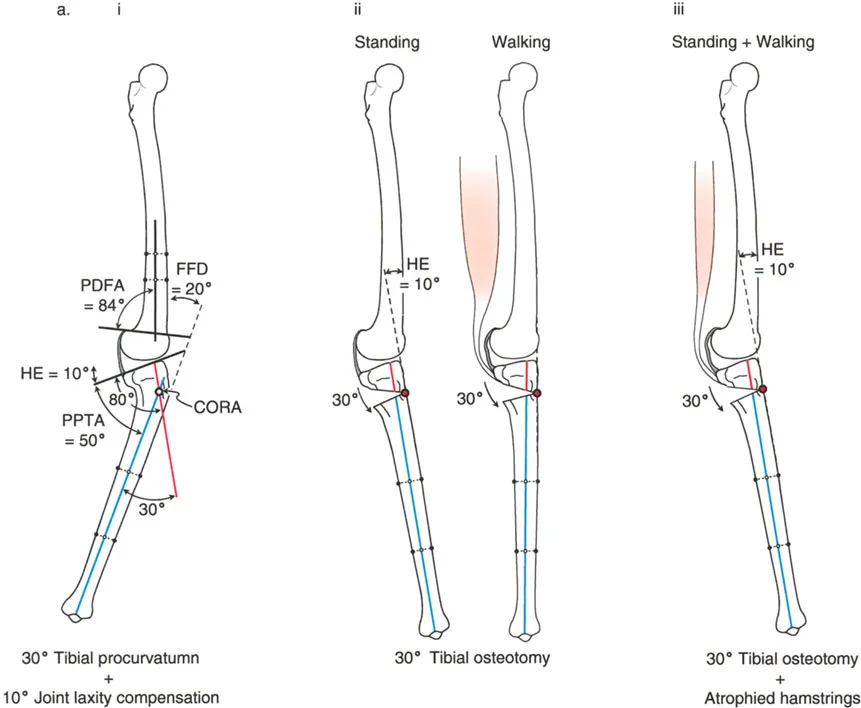
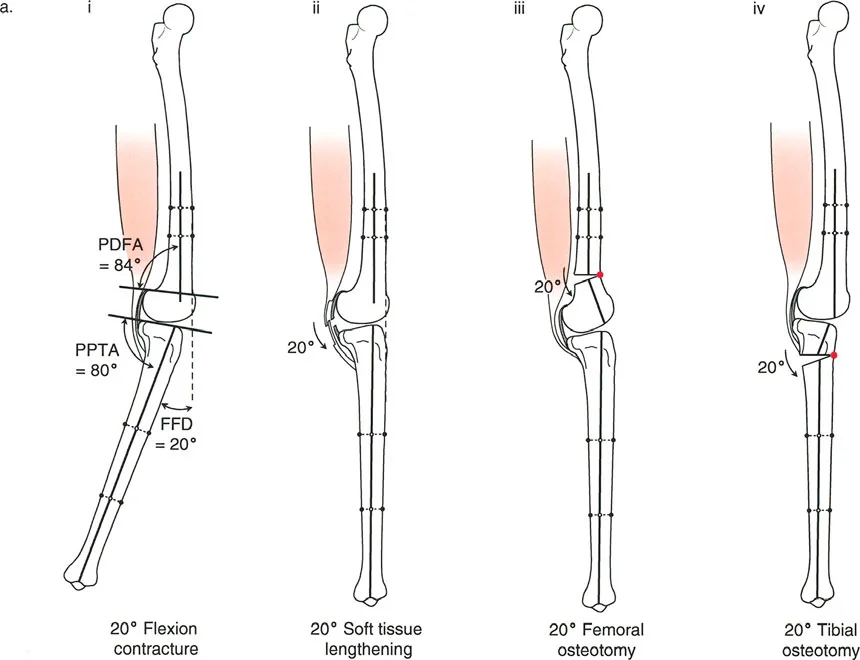
A 19-year-old male has a 20° knee flexion deformity secondary to a proximal tibial procurvatum (PPTA = 60°). The surgeon considers correcting this with a 20° extension osteotomy of the distal femur. What is the primary disadvantage of this approach?
View Answer & Explanation
Correct Answer: C
Rationale: The text and accompanying figure (Fig. 17-2a) explicitly state that correcting a tibial deformity with a femoral osteotomy is not preferred because the osteotomy is far from the Center of Rotation of Angulation (CORA). This results in an undesirable forward translation of the tibia and knee.
Question 39
A 62-year-old woman with MCOA and varus deformity is being treated with a closing wedge high tibial osteotomy. She also has a mild fixed flexion deformity. To avoid exacerbating patellar baja, where should the closing wedge osteotomy be performed?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that a closing wedge osteotomy proximal to the tibial tuberosity moves the tuberosity closer to the joint line, which can cause or worsen patella baja. Therefore, when a closing wedge osteotomy is chosen in the setting of a flexion deformity, it is preferable to perform it distal to the tuberosity to avoid altering the patellar tendon insertion level relative to the joint.
Question 40
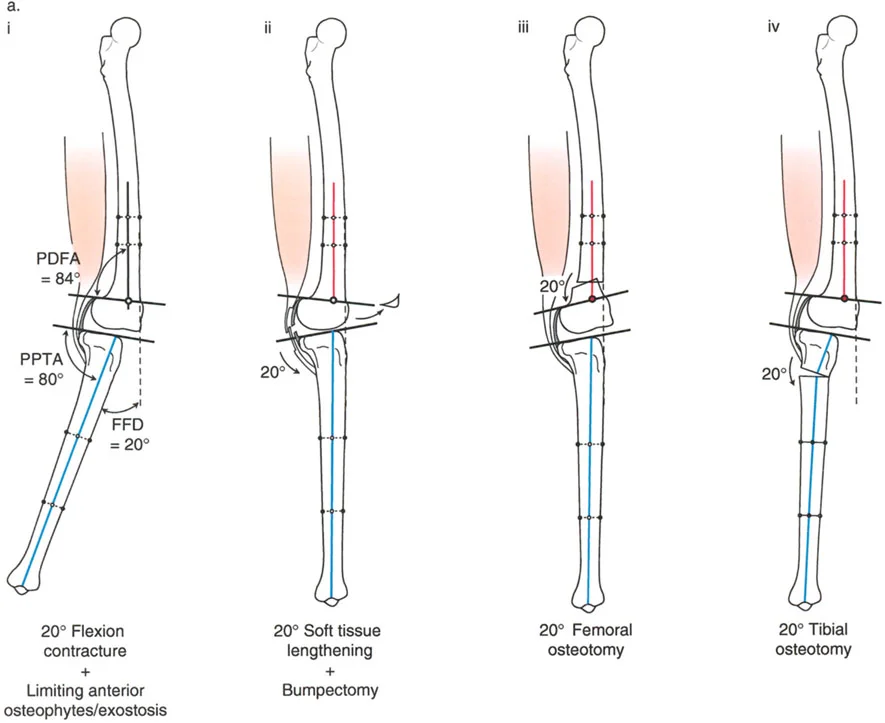
A 30-year-old patient has a 20° fixed flexion deformity (FFD) of the knee. Sagittal plane analysis reveals a normal PDFA of 84° and a normal PPTA of 80°. According to the principles outlined, what is the ideal treatment?
View Answer & Explanation
Correct Answer: C
Rationale: When the FFD exists with normal bony alignment (normal PDFA and PPTA), the deformity is due to a joint contracture. The text identifies the ideal treatment in this scenario as soft tissue lengthening. While a femoral osteotomy is a reasonable alternative, soft tissue procedures directly address the pathology.
Question 41
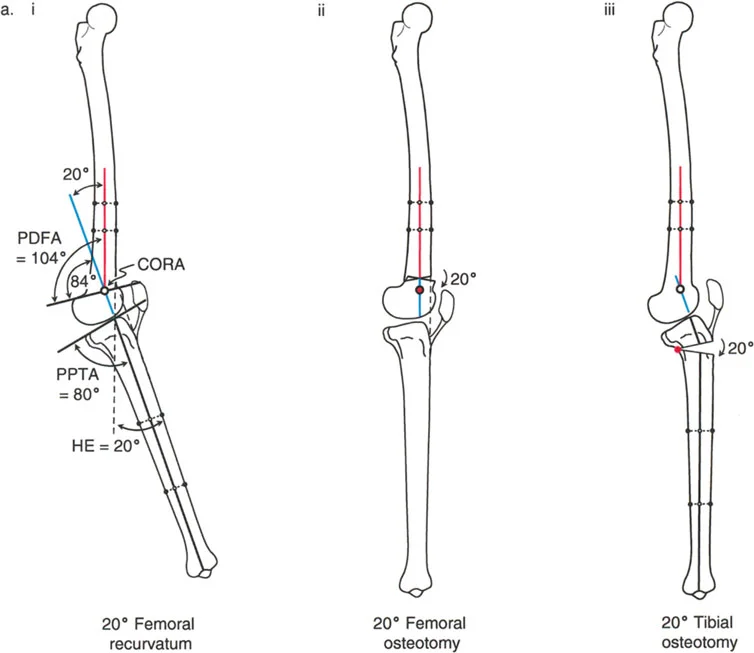
A 25-year-old male presents with knee hyperextension (recurvatum). A long lateral radiograph in maximum extension shows a PPTA of 100° and a PDFA of 83°. What is the primary clinical concern associated with this specific bony deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The text specifies that tibial recurvatum (increased PPTA) is usually more symptomatic than femoral recurvatum because the anterior deceleration stop to the femur is lost. This leads to compensatory quadriceps firing to pull the tibia forward, increasing stress on the patellofemoral joint and often causing anterior knee pain. Loss of flexion is characteristic of femoral recurvatum.
Question 42
A 66-year-old male with MCOA, varus deformity, and lateral subluxation has significant medial tibial plateau depression. What surgical technique is specifically designed to address both the plateau depression and the associated subluxation?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that in the presence of medial plateau depression, lateral subluxation is corrected by medial plateau elevation. This procedure directly addresses the intra-articular bone loss, which helps to reduce the knee subluxation. A standard metaphyseal osteotomy would not correct the articular depression.
Question 43
A 14-year-old female with a history of polio and absent quadriceps function has a 12° fixed flexion deformity (FFD). Radiographs show a distal femoral procurvatum (PDFA = 65°). What is the primary goal of performing a femoral extension osteotomy in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that in patients with absent quadriceps function (e.g., polio), it is essential to fully extend the knee with an osteotomy. This allows the ground reaction force line to pass in front of the knee, enabling the patient to "lock" the knee passively and maintain a stable stance without active quadriceps control.
Question 44
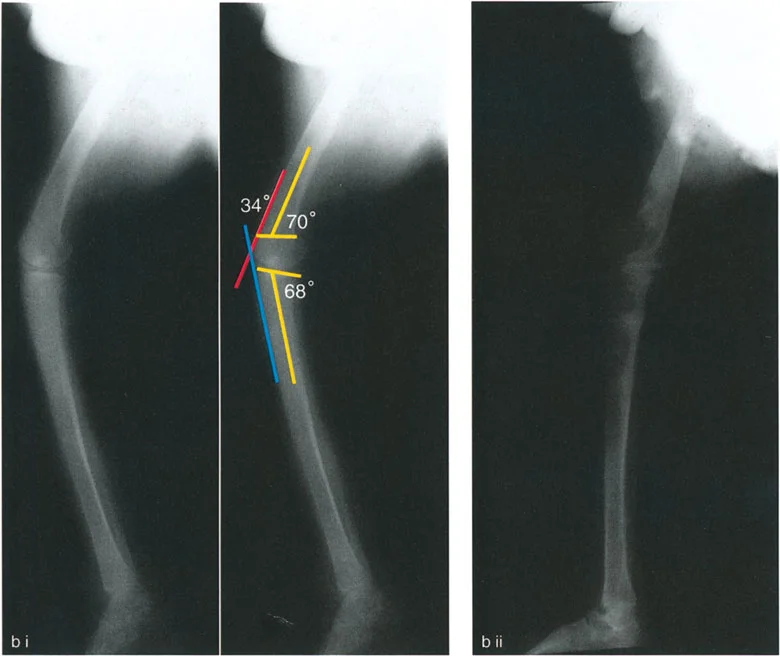
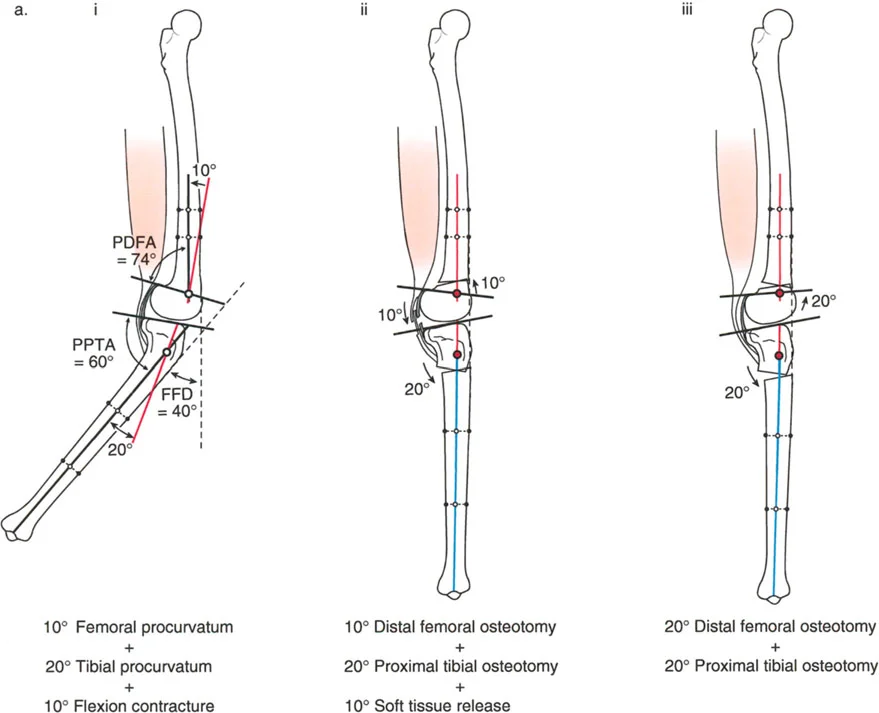
A patient has a 20° fixed flexion deformity (FFD) that is determined to be a combination of 10° of distal femoral procurvatum and a 10° soft tissue contracture. The surgeon elects to perform a 20° distal femoral extension osteotomy to correct the entire deformity. What is the main advantage of this approach over a combined osteotomy and soft tissue release?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes this exact scenario (Fig. 17-5) and states that performing the entire correction in the bone is a "very reasonable option that avoids an extensive soft tissue procedure and decreases the risk of recurrence." Correcting the contracture via an extra-articular osteotomy can be preferable to intra-articular releases that may lead to stiffness or recurrence.
Question 45
A 59-year-old male with MCOA has a varus deformity and a recurvatum deformity. The patellar tendon insertion is noted to be at a normal level relative to the knee joint line. To correct both deformities, where should the osteotomy be made?
View Answer & Explanation
Correct Answer: B
Rationale: As shown in Figure 16-22a, when a varus plus recurvatum deformity is present and the patellar tendon is at a normal level, the osteotomy is made distal to the tibial tuberosity. This allows for an oblique plane correction to address both deformities without altering patellar height unfavorably.
Question 46
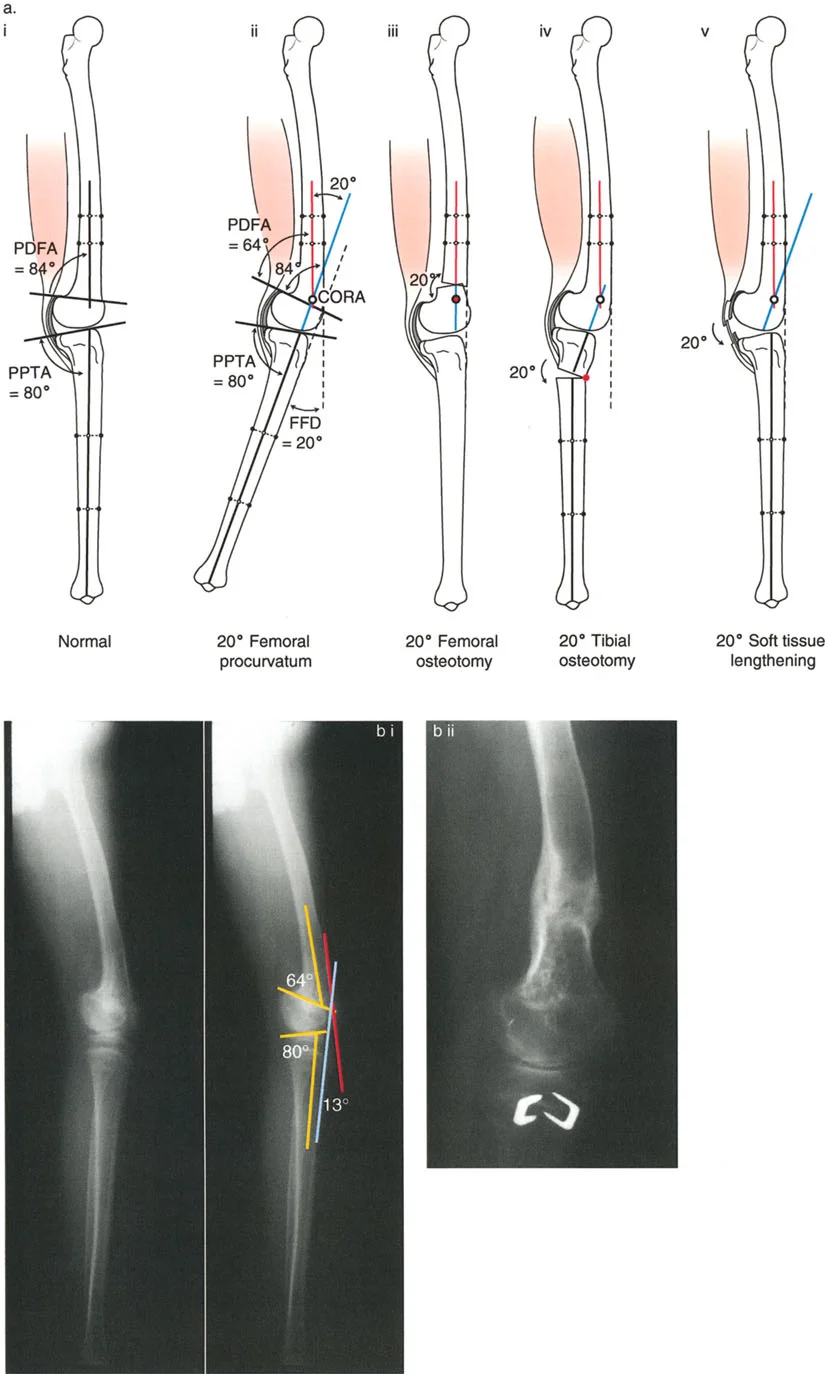
A patient presents with a 20° knee flexion deformity. Sagittal plane analysis reveals a 10° distal femoral procurvatum (PDFA=74°) and a 10° proximal tibial procurvatum (PPTA=70°). The surgeon plans to correct the entire 20° deformity with a proximal tibial extension osteotomy. What is the primary concern with this strategy?
View Answer & Explanation
Correct Answer: B
Rationale: The text (Fig. 17-3) explicitly states that correcting a combined femoral and tibial deformity entirely in the tibia is "not a good alternative because it eliminates the important posterior tilt of the proximal tibia." The posterior slope is crucial for normal knee kinematics and the deceleration mechanism of the femur.
Question 47
A 68-year-old male with a history of a healed, malunited femoral shaft fracture presents with debilitating knee pain and a significant varus deformity. A standing hip-to-ankle radiograph is obtained for preoperative planning. According to the principles of deformity analysis, what is the primary purpose of drawing a line from the center of the femoral head to the center of the ankle mortise?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the mechanical axis is a straight line drawn from the center of the femoral head to the center of the ankle mortise. This line is the foundation for assessing Mechanical Axis Deviation (MAD) and overall limb alignment. The anatomical axis follows the intramedullary canal of the bone, which is different.
Question 48
A 72-year-old female presents with severe valgus knee deformity and end-stage lateral compartment osteoarthritis. Preoperative planning using a full-length standing radiograph reveals a Mechanical Lateral Distal Femoral Angle (mLDFA) of 98 degrees. What is the most accurate interpretation of this finding?
View Answer & Explanation
Correct Answer: D
Rationale: The normal mLDFA is approximately 87-88 degrees. A value of 98 degrees is significantly abnormal and indicates a valgus deformity originating from the distal femur. An abnormal Medial Proximal Tibial Angle (MPTA) would point to a tibial deformity.
Question 49
A 65-year-old male with a history of a proximal tibial fracture treated non-operatively presents with severe varus deformity and medial knee pain. His full-length radiograph shows a Medial Proximal Tibial Angle (MPTA) of 75 degrees. The mLDFA is 88 degrees. This deformity pattern indicates that the malalignment is located in the:
View Answer & Explanation
Correct Answer: B
Rationale: The normal MPTA is approximately 87-88 degrees. A value of 75 degrees indicates significant tibial varus. Since the mLDFA is normal, the deformity is isolated to the proximal tibia. This information is critical for deciding whether an osteotomy is needed in conjunction with the TKA.
Question 50
During preoperative planning for a TKA in a patient with a severe varus deformity, the surgeon measures the angle formed by extending the lines of the distal femoral and proximal tibial joint surfaces. This angle is found to be 12 degrees. What is this measurement called and what does it signify?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the Joint Line Convergence Angle (JLCA) as the angle formed by extending the joint surface lines. A large JLCA (normal is 0-2 degrees) indicates an intra-articular problem, such as severe asymmetric cartilage wear or significant ligamentous laxity, which contributes to the overall malalignment.
Question 51
A surgeon is planning a TKA for a patient with a 25-degree varus deformity secondary to a healed diaphyseal tibial fracture. The surgeon plans to correct the entire limb malalignment solely with asymmetric intra-articular bone cuts during the TKA. According to the provided text, what is the most likely biomechanical consequence of this strategy?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly warns against this strategy, stating it is a "grave biomechanical error." Attempting to correct a large, remote extra-articular deformity with intra-articular cuts creates a trapezoidal flexion and extension gap, leading to severe collateral ligament imbalance, edge-loading, and early failure.
Question 52
A 70-year-old female undergoes a TKA for a severe valgus knee. During the trial reduction, the surgeon finds the knee is perfectly balanced and stable in 90 degrees of flexion. Upon bringing the knee into full extension, it is found to be excessively tight. According to the systematic balancing algorithm described, what is the next most appropriate step?
View Answer & Explanation
Correct Answer: B
Rationale: The text outlines a clear algorithm: balance in flexion first. If the knee is then too tight in extension, it necessitates more resection of bone from the distal femur. Changing the tibial insert (Option A) would unbalance the flexion gap, which was already correct.
Question 53
During a complex TKA, the surgeon has balanced the knee in flexion using an appropriate tibial insert. When the knee is brought into extension, it is found to be unstable and loose. What is the correct surgical maneuver to address this specific problem?
View Answer & Explanation
Correct Answer: D
Rationale: Following the "flexion first" principle, if the knee is balanced in flexion but loose in extension, the extension gap must be filled. This is achieved by advancing (distalizing) the femoral component, typically with augments. Resecting more distal femur (Option A) would worsen the extension laxity.
Question 54
A surgeon is performing a TKA and prioritizes balancing the extension gap first. After achieving stability in extension, the knee is found to be excessively tight in flexion. Why is this "extension first" approach considered less efficient and more complex than the "flexion first" method described in the text?
View Answer & Explanation
Correct Answer: C
Rationale: The text emphasizes prioritizing flexion balancing because any change to the tibial insert thickness affects both flexion and extension. By establishing the flexion gap first, the surgeon isolates the extension gap as a single variable that can be adjusted with the distal femoral cut or augmentation, simplifying the process from nine possibilities to three.
Question 55
A 69-year-old male with a severe varus deformity has a preoperative plan that includes a corrective osteotomy. During the planning phase, the surgeon identifies the point where the proximal and distal mechanical axis lines of the deformed tibia intersect. What is this critical geometric point called?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the Center of Rotation of Angulation (CORA) as the geometric point where the proximal and distal mechanical axis lines of a deformed bone intersect. The CORA represents the true apex of the deformity and is the fundamental point around which a corrective osteotomy is planned.
Question 56
According to the core principles for ligament balancing outlined in the text, what is the relative contribution of soft tissue releases versus the use of more constrained prostheses in achieving a well-balanced knee in complex TKA?
View Answer & Explanation
Correct Answer: B
Rationale: The text provides a clear core principle: "Recognize that greater than 95% of ligament balancing requires soft tissue releases." It further states that less than 5% involves advancements or more constrained prostheses, emphasizing the primacy of soft tissue work over implant constraint.
Question 57
A 75-year-old patient presents with severe knee osteoarthritis and a significant valgus deformity. Preoperative radiographic analysis reveals a normal MPTA of 87 degrees and a normal JLCA of 2 degrees. The mLDFA is measured at 96 degrees. Based on this "deformity map," where is the primary source of the patient's malalignment?
View Answer & Explanation
Correct Answer: C
Rationale: The systematic analysis shows normal tibial (MPTA) and intra-articular (JLCA) parameters. The only abnormal value is the mLDFA (normal ~87-88°), which at 96° indicates a significant valgus deformity originating in the distal femur. This precise localization is the goal of the Paley method of analysis.
Question 58
A surgeon is performing a TKA on a patient with a fixed flexion contracture and severe varus. After making the initial bone cuts and performing medial releases, the trial components are placed. The knee is stable in flexion but remains tight in extension. Which of the following adjustments is most likely to correct the residual tightness in extension without affecting the flexion gap?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that varying the thickness of the distal femoral cut affects stability *only* in extension. Since the flexion gap is already balanced, resecting more distal femur will loosen the tight extension gap without altering the flexion stability. Resecting posterior condyles (Option C) would loosen the flexion gap.
Question 59
What is the normal physiological value for the Medial Proximal Tibial Angle (MPTA) as described in the provided text?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that the normal value for the Medial Proximal Tibial Angle (MPTA) is approximately 87 to 88 degrees. This value represents a slight varus alignment of the proximal tibia relative to its mechanical axis.
Question 60
A 62-year-old patient has a large varus deformity originating from the femoral diaphysis. The surgeon ignores this and proceeds with a standard TKA, making large, asymmetric bone cuts to align the limb. This results in significant elevation of the medial joint line. What is a direct consequence of this iatrogenic joint line elevation?
View Answer & Explanation
Correct Answer: C
Rationale: Correcting a remote, extra-articular deformity at the joint level forces the joint line to become oblique to the mechanical axis and creates a trapezoidal gap. This inherently leads to severe collateral ligament imbalance, as one side becomes tight while the other becomes lax, leading to instability and early failure.
Question 61
The fundamental paradigm shift required when treating a patient with end-stage osteoarthritis and severe extra-articular malalignment is best described as moving from:
View Answer & Explanation
Correct Answer: A
Rationale: The introductory paragraph of the text explicitly states, "The surgeon must transition from simple joint resurfacing to comprehensive whole-limb reconstruction." This captures the essence of addressing the entire limb's mechanical environment, not just the articular surfaces.
Question 62
A 71-year-old male undergoes TKA. The trial is performed, and the knee is perfectly balanced in both flexion and extension with a 12mm tibial insert. The surgeon decides to use a 14mm final insert to "make it a little tighter." What is the most likely outcome of this decision?
View Answer & Explanation
Correct Answer: C
Rationale: The text highlights a key principle: "varying the tibial insert thickness affects stability in *both* flexion and extension simultaneously." Increasing the insert thickness from the balanced trial will make both the flexion and extension gaps tighter, potentially leading to stiffness and pain.
Question 63
A preoperative standing radiograph for a complex TKA shows the mechanical axis line passing 35 mm medial to the center of the knee joint. What is the correct term for this measurement?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines Mechanical Axis Deviation (MAD) as "the perpendicular distance in millimeters from the mechanical axis line to the center of the knee joint." This measurement quantifies the overall magnitude of the limb's varus or valgus malalignment.
Question 64
When is a corrective osteotomy considered mandatory in the setting of a TKA for severe malalignment?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that if an extra-articular deformity's apex is far from the joint, attempting to correct it with intra-articular TKR cuts is a grave error. In such cases, a corrective osteotomy is mandatory to realign the bone itself, allowing for a more standard and biomechanically sound TKA.
Question 65
The systematic approach to ligament balancing described in the text simplifies the process by reducing the nine possible alignment outcomes to just three. This simplification is achieved by first establishing a "just right" state in which phase of motion?
View Answer & Explanation
Correct Answer: D
Rationale: The core of the described algorithm is to perform the trial reduction and balancing in flexion first. By adjusting soft tissues and tibial insert thickness to achieve a "just right" state in flexion, the surgeon only has to manage the single variable of the extension gap, reducing the problem to three simple outcomes.
Question 66
A 78-year-old female with severe rheumatoid arthritis has gross instability and bone loss, requiring a TKA. The surgeon is concerned about ligamentous integrity. According to the provided text's core principles, when should a fully constrained (hinged) prosthesis be considered?
View Answer & Explanation
Correct Answer: D
Rationale: A stated core principle is to "Rarely rely on fully constrained (hinged) prostheses unless absolutely necessary." This emphasizes that hinged implants are a last resort, not a routine solution, due to high stress transfer to bone-implant interfaces and other potential complications.
Question 67
What is the normal physiological value for the Mechanical Lateral Distal Femoral Angle (mLDFA) as described in the provided text?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that the normal physiological value for the Mechanical Lateral Distal Femoral Angle (mLDFA) is approximately 87 to 88 degrees. This represents the slight valgus of the distal femoral joint line relative to the femoral mechanical axis.
Question 68
A 35-year-old male is being evaluated for a distal tibial malunion. When assessing the frontal plane alignment on a weight-bearing radiograph, the surgeon notes the relationship between the tibial plafond and the talar dome. According to the principles of normal ankle biomechanics, what is the acceptable amount of joint line convergence angle (JLCA) in a healthy ankle?
View Answer & Explanation
Correct Answer: A
Rationale: The paramount rule of normal ankle alignment is that the superior dome of the talus must be strictly parallel to the tibial plafond, resulting in a JLCA of 0 degrees. This is a critical distinction from the knee, where up to 3 degrees of convergence is considered physiologic.
Question 69
A 28-year-old female presents with chronic ankle pain after a remote tibial fracture. During surgical planning, the surgeon considers the three-dimensional anatomy of the talus in the sagittal plane. As described by Inman and Stiehl, the 3D shape of the talar dome is best characterized as which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The 3D shape of the talar dome is a frustum, which is a section of a cone. This conical geometry dictates that the true axis of ankle rotation is oblique, not a simple hinge parallel to the joint line.
Question 70
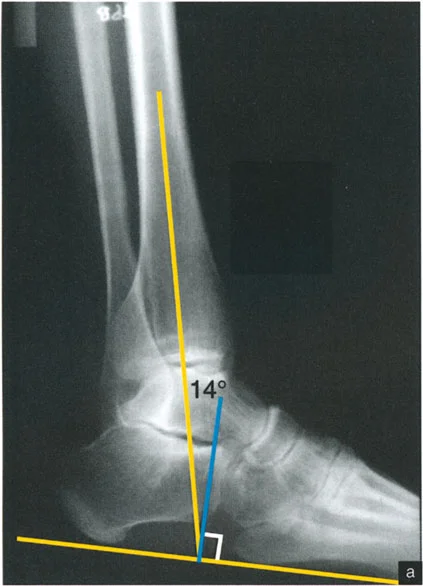
A 45-year-old male is being evaluated for a sagittal plane deformity of the distal tibia. A true lateral radiograph is obtained with the plantar aspect of the foot at 90° to the tibia. The surgeon measures the angle between the mid-diaphyseal line of the tibia and the tibial plafond. What is the normal value for this Anterior Distal Tibial Angle (ADTA)?
View Answer & Explanation
Correct Answer: C
Rationale: The normal tibial plafond is tilted anteriorly, resulting in an Anterior Distal Tibial Angle (ADTA) of exactly 80°. An angle greater than 80° indicates procurvatum, while an angle less than 80° indicates recurvatum.
Question 71
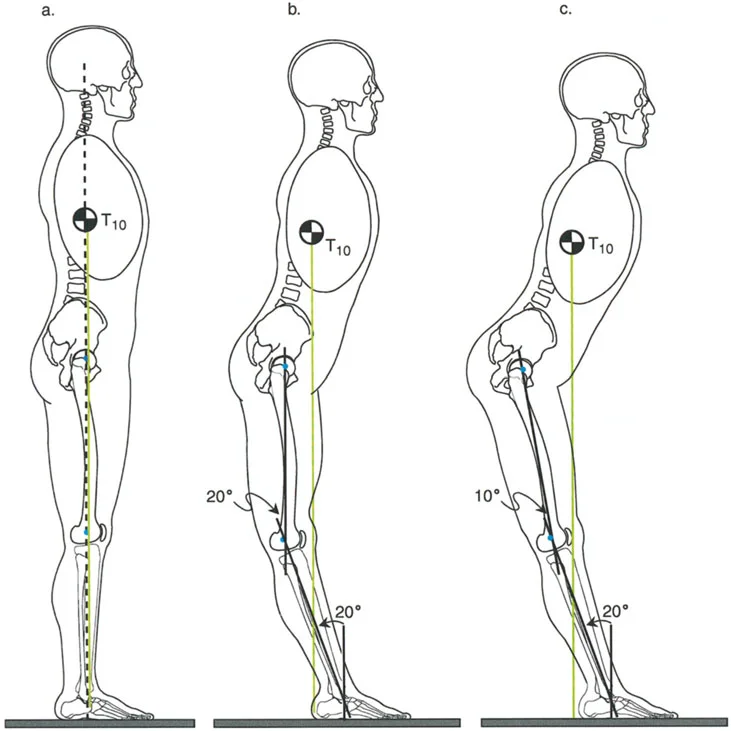
A 50-year-old female is evaluated for ankle pain. Biomechanical analysis of her single-leg stance reveals the position of the Ground Reaction Force Vector (GRV). In a normal individual, the GRV passes anterior and lateral to the center of the ankle joint. This creates which combination of moments on the hindfoot and ankle?

View Answer & Explanation
Correct Answer: D
Rationale: During single-leg stance, the GRV passes lateral to the ankle center, creating a valgus moment, and anterior to the ankle center, creating a dorsiflexion moment. This explains why the anterolateral aspect of the tibiotalar joint is under the greatest stress.
Question 72
A 62-year-old male presents with anterolateral ankle pain consistent with early osteoarthritis. His gait analysis shows normal alignment. Given the inherent valgus and dorsiflexion moments created by the Ground Reaction Force Vector (GRV) during single-leg stance, which two muscle groups must remain highly active to dynamically counter these forces?
View Answer & Explanation
Correct Answer: B
Rationale: The tibialis posterior (a powerful inverter) must fire to counteract the valgus moment from the GRV. The gastro-soleus complex (powerful plantar flexors) must fire to counteract the dorsiflexion moment. These muscles are critical for dynamic ankle stability.
Question 73
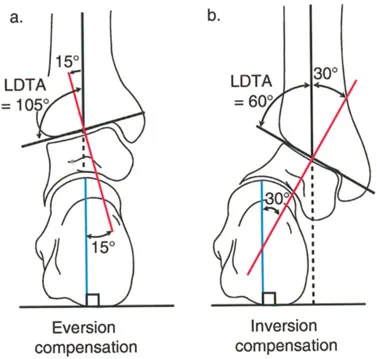
A 40-year-old female has a post-traumatic distal tibial deformity. The surgeon is explaining the compensatory capacity of the hindfoot. The subtalar joint has an asymmetrical range of motion that dictates its ability to compensate for tibial malalignment. What are the normal maximum ranges for subtalar inversion and eversion, respectively?
View Answer & Explanation
Correct Answer: B
Rationale: The subtalar joint has a much greater range of inversion (30°) than eversion (15°). This is why the hindfoot can compensate for a much larger valgus deformity (which requires inversion) than a varus deformity (which requires eversion).
Question 74
A 33-year-old male presents with a 20-degree varus deformity of the distal tibia. On clinical examination, his foot is plantigrade. Which joint is primarily responsible for compensating for this deformity to keep the foot flat on the floor?
View Answer & Explanation
Correct Answer: B
Rationale: The subtalar joint acts as a universal joint and is the primary driver of compensation for frontal plane tibial malalignment. It will invert or evert to attempt to maintain a plantigrade foot. The ankle joint itself does not have frontal plane motion to compensate.
Question 75
A 55-year-old female with a complex distal tibial valgus deformity is undergoing preoperative planning. The surgeon is concerned about the hindfoot alignment, which is difficult to assess on standard AP and lateral radiographs. Which specialized radiographic view is required to accurately measure the alignment of the calcaneus relative to the mid-diaphyseal line of the tibia?
View Answer & Explanation
Correct Answer: E
Rationale: The Saltzman view is a long axial view radiograph obtained at a 20° inclination to the horizontal. It is the gold standard for radiographically assessing hindfoot alignment by visualizing the relationship between the calcaneal axis and the tibial axis.
Question 76
A 25-year-old male has a 20-degree varus deformity of the distal tibia following a malunion. His subtalar joint has maximally everted by 15 degrees to compensate, but the foot is still not plantigrade. What is the next compensatory mechanism, primarily involving the forefoot, that will occur?
View Answer & Explanation
Correct Answer: B
Rationale: A varus tibial deformity drives the heel into varus. The subtalar joint compensates with eversion. Once eversion is exhausted (at ~15°), the forefoot must pronate to bring the medial side of the foot down to the ground. This is achieved by active plantar flexion of the first ray, creating a rigid cavus foot posture.
Question 77
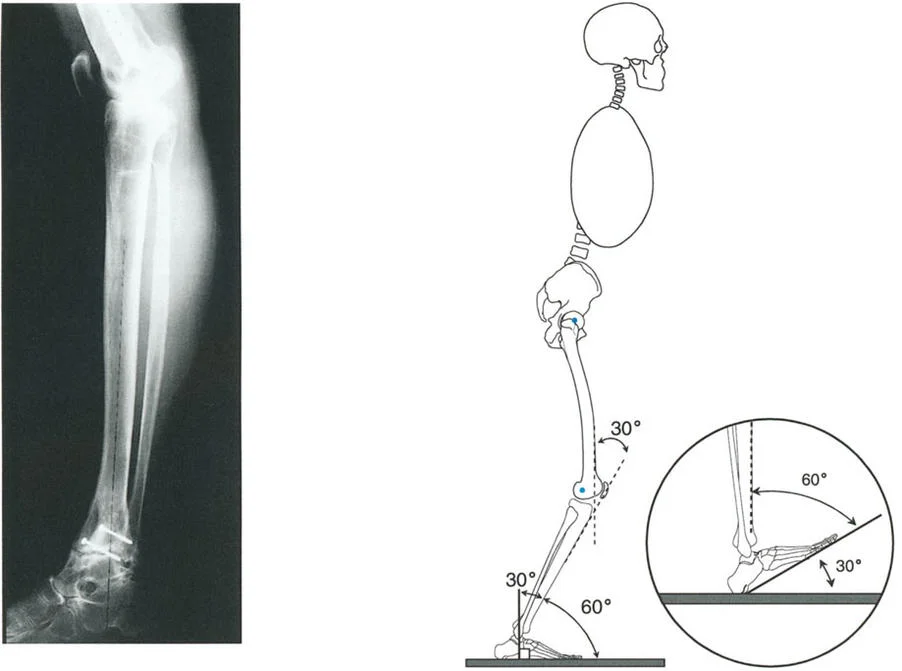
A 48-year-old female presents with a 35-degree valgus deformity of the distal tibia. Her subtalar joint has maximally inverted by 30 degrees, but this is insufficient to make the foot plantigrade. What compensatory mechanism will the forefoot employ to accommodate the remaining deformity?
View Answer & Explanation
Correct Answer: A
Rationale: A valgus tibial deformity drives the heel into valgus. The subtalar joint compensates with inversion. Once inversion is exhausted (at ~30°), the forefoot must supinate to bring the lateral side of the foot down. This is achieved by dorsiflexion of the first ray, contributing to the planovalgus foot posture.
Question 78
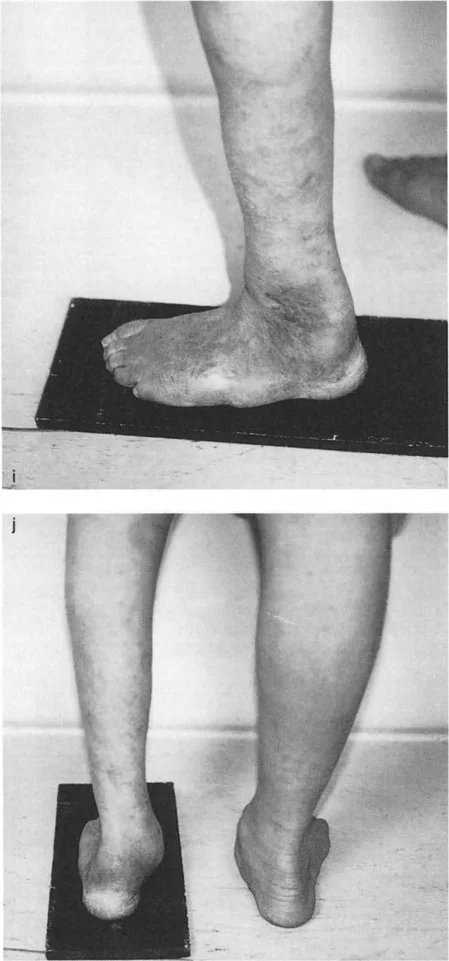
A 30-year-old male presents with lateral foot pain and a history of a healed distal tibia fracture. On examination, he has a high arch and tenderness along the lateral border of his foot. Radiographs confirm a 20-degree varus malunion of the tibia. What is the expected clinical appearance of his foot due to compensation?
View Answer & Explanation
Correct Answer: B
Rationale: A significant varus deformity of the tibia, once subtalar eversion is exhausted, is compensated by forefoot pronation (plantar flexion of the first ray). This creates a rigid, high-arched (cavus) foot posture with the heel in varus, leading to lateral border overload and pain.
Question 79
A 58-year-old female has a long-standing 15-degree varus deformity of her distal tibia but shows surprisingly minimal tibiotalar arthritis on radiographs. What is the primary biomechanical reason that the ankle joint tolerates varus deformities relatively well?
View Answer & Explanation
Correct Answer: A
Rationale: The normal GRV passes lateral to the ankle, loading the anterolateral joint. A varus deformity shifts the mechanical axis and the GRV medially. This unloads the vulnerable lateral joint and transfers the load to the medial facet of the talus and the medial malleolus, which hypertrophies and acts as a buttress. This load transfer is why the joint itself is relatively spared from rapid degeneration.
Question 80
A 42-year-old construction worker with a 25-degree distal tibial varus malunion presents with debilitating pain. His ankle joint space is well-preserved. What is the most likely source of his pain?
View Answer & Explanation
Correct Answer: D
Rationale: While the ankle joint itself tolerates varus well, the compensatory mechanisms are highly pathologic for the foot. The development of a rigid cavovarus foot drastically decreases the weight-bearing surface area, concentrating force on the lateral border of the foot. This is the primary source of pain in patients with uncorrected tibial varus.
Question 81
A 39-year-old male has a 25-degree valgus malunion of his distal tibia. He presents with severe lateral ankle pain and radiographic evidence of advanced tibiotalar and fibulotalar arthritis. Which of the following is the primary reason the ankle joint tolerates valgus deformity so poorly?
View Answer & Explanation
Correct Answer: B
Rationale: The lateral aspect of the ankle is already physiologically overloaded by the normal GRV. A valgus deformity shifts the GRV even further laterally, which dramatically increases the bending moment and stress on the lateral tibiotalar joint and fibula. This leads to rapid cartilage wear and degenerative arthritis.
Question 82
A 29-year-old female sustains a distal tibia fracture that heals in 20 degrees of valgus. During gait, this deformity places immense shear stress on the fibula and its articulation with the tibia. This chronic stress most commonly leads to which of the following pathologic changes?
View Answer & Explanation
Correct Answer: A
Rationale: Valgus deformity creates significant shear stress on the fibula and the syndesmosis. Over time, this chronic load causes the syndesmotic ligaments to stretch and fail, leading to a widening of the syndesmosis and lateral shift of the talus, which accelerates arthritis.
Question 83
A surgeon is planning a corrective osteotomy for a patient with a valgus malunion. The surgeon recalls the work of Yablon et al. regarding talar stability. According to this research, what is the biomechanical consequence of just a 1mm lateral shift of the talus within the mortise?
View Answer & Explanation
Correct Answer: B
Rationale: The work by Yablon et al. is foundational to understanding ankle stability. It demonstrated that even a 1mm lateral shift of the talus dramatically decreases the contact area between the tibia and talus. This concentrates the entire body weight over a much smaller surface, leading to extremely high contact pressures and rapid cartilage destruction.
Question 84
A 41-year-old female presents with a flexible planovalgus foot deformity and lateral ankle pain. Radiographs reveal a 25-degree valgus malunion of the distal tibia. What is the expected clinical appearance of her foot due to compensation?
View Answer & Explanation
Correct Answer: B
Rationale: A valgus deformity of the tibia is compensated first by subtalar inversion, and then by forefoot supination (dorsiflexion of the first ray). This combination leads to a collapse of the medial longitudinal arch, resulting in a flexible planovalgus (flatfoot) posture.
Question 85
A surgeon is analyzing a post-traumatic deformity in a 30-year-old male. The Center of Rotation of Angulation (CORA) is located in the mid-diaphysis of the tibia. According to Paley's principles, how will this deformity affect the joint orientation angles of the knee and ankle?
View Answer & Explanation
Correct Answer: C
Rationale: The proximity of the CORA to a joint determines its effect. A CORA near the knee primarily affects the Medial Proximal Tibial Angle (MPTA). A CORA near the ankle primarily affects the Lateral Distal Tibial Angle (LDTA). A mid-diaphyseal CORA is equidistant and will therefore affect both joint orientation angles, though to a lesser magnitude than a juxta-articular deformity.
Question 86
A 45-year-old male is being evaluated in a gait laboratory. During the initial contact phase of the gait cycle, which muscle group is primarily responsible for eccentrically contracting to control plantarflexion and prevent an audible "foot slap"?
View Answer & Explanation
Correct Answer: C
Rationale: The pretibial muscles (tibialis anterior, EHL, EDL) eccentrically contract to control the descent of the foot to the ground after heel strike. This is the key function of the first (heel) rocker. Weakness of these muscles leads to uncontrolled plantarflexion, or "foot slap."
Question 87
A 52-year-old female is observed walking after recovery from an Achilles tendon rupture. During midstance, her tibia seems to collapse forward rapidly, and she demonstrates poor knee stability. This observation suggests a deficiency in the primary function of which phase of the stance cycle?
View Answer & Explanation
Correct Answer: B
Rationale: The second (ankle) rocker is controlled by the eccentric contraction of the triceps surae, which acts as a brake to prevent the tibia from collapsing forward too quickly. A deficient triceps surae compromises this function, leading to instability.
Question 88
A 68-year-old male with severe hallux rigidus presents with a complaint of a "weak" and shuffling gait. His primary difficulty is with propulsion at the end of the stance phase. This gait abnormality is due to the disruption of which biomechanical event?
View Answer & Explanation
Correct Answer: D
Rationale: The third (forefoot) rocker uses the metatarsophalangeal (MTP) joints as a fulcrum for the concentric contraction of the calf muscles to generate propulsive force. Hallux rigidus (stiffness of the first MTP joint) directly impairs this mechanism, weakening toe-off.
Question 89
An orthopedic surgeon is reviewing post-operative radiographs of a tibial deformity correction. The surgeon's primary goal, beyond achieving perfect static alignment, should be the restoration of which functional outcome?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text emphasizes that the ultimate goal of deformity correction is not a "pretty picture" on a radiograph but a patient who walks well. A smooth, efficient, and painless gait represents the successful restoration of dynamic function.
Question 90
A 58-year-old male is evaluated for a gait disturbance. On observation, his head has an excessive vertical displacement of approximately 10 cm with each step. This finding, known as vaulting, is a classic compensation for a failure of which fundamental process?
View Answer & Explanation
Correct Answer: C
Rationale: Vaulting is a compensation for a functionally long limb, which occurs when the smooth, energy-conserving progression through the three foot rockers is lost (e.g., due to an ankle fused in equinus). The patient must rise up on the contralateral toes to clear the stiff limb, causing excessive vertical head motion.
Question 91
A 49-year-old male underwent a tibiotalar arthrodesis fused in 10 degrees of equinus. To compensate for the loss of the second rocker and allow for forward progression during midstance, which of the following gait deviations is most likely to develop at the ipsilateral knee?
View Answer & Explanation
Correct Answer: B
Rationale: With a fixed equinus deformity, the ankle cannot dorsiflex during midstance. To allow the body's center of mass to pass over the foot, the patient compensates by forcing the knee into hyperextension (genu recurvatum). This is a common secondary pathology following ankle fusion in equinus.
Question 92
A 22-year-old patient with a common peroneal nerve palsy is observed to have a high-stepping, or "steppage," gait. This is a compensatory mechanism for the failure of which muscle group's function during the first rocker?
View Answer & Explanation
Correct Answer: B
Rationale: Peroneal nerve palsy causes weakness of the pretibial muscles (dorsiflexors). This leads to a foot drop during swing phase and an inability to control plantarflexion at initial contact (failure of the first rocker). The steppage gait is a compensation to clear the dropped foot during swing.
Question 93
The stance phase of the normal gait cycle is primarily characterized by a series of three biomechanical pivots that allow for a smooth, rolling transition of weight. What is the correct sequence of these pivots (rockers)?
View Answer & Explanation
Correct Answer: D
Rationale: The stance phase progresses sequentially from the first rocker (heel), to the second rocker (ankle), and finally to the third rocker (forefoot) for propulsion. This sequence ensures metabolic efficiency.
Question 94
A 60-year-old woman with a history of an iatrogenic anterior translation of her distal tibia during a deformity correction reports a jarring sensation with every step. A loud foot slap is audible on exam. This gait pathology is a direct result of the failure of which rocker?
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that a loud "slap" at initial contact indicates a failure of the first rocker. This can be caused by anterior compartment weakness or an iatrogenic anterior translation deformity, which functionally weakens the pretibial muscles' ability to control plantarflexion.
Question 95
During the second (ankle) rocker, the powerful triceps surae complex contracts eccentrically. What is the primary biomechanical purpose of this specific muscle action?
View Answer & Explanation
Correct Answer: C
Rationale: The eccentric (lengthening) contraction of the calf muscles during the second rocker is crucial for decelerating the forward momentum of the tibia over the fixed talus. This controlled movement prevents a sudden collapse into dorsiflexion and maintains knee stability.
Question 96
A 70-year-old male with end-stage ankle arthritis undergoes an ankle arthrodesis. To best preserve the second and third rockers and facilitate a more normal gait, what is the ideal position of the foot and ankle for fusion?
View Answer & Explanation
Correct Answer: C
Rationale: While an ankle fusion eliminates the ankle rocker, fusing in a plantigrade (neutral dorsiflexion) and slightly valgus position allows the patient to "roll over" the foot through the midfoot and forefoot, best simulating the second and third rockers. Equinus or calcaneus positions create significant gait compensations.
Question 97
A 14-year-old boy with the deformity seen in the clinical photograph presents with medial knee pain and a lateral thrust during gait. The deformity disrupts the normal mechanical axis of the lower extremity. Which rocker is most likely to be overloaded and dysfunctional due to the compensatory gait?
View Answer & Explanation
Correct Answer: B
Rationale: The image shows significant tibial vara (bowing). This coronal plane deformity shifts the mechanical axis medially, causing a varus thrust at the knee and altering the forces across the ankle during midstance. This directly impacts the function and loading of the second (ankle) rocker.
Question 98
The propulsive force for "toe-off" is generated by the explosive concentric contraction of the calf muscles during the third rocker. Which anatomical structures serve as the fulcrum for this critical action?
View Answer & Explanation
Correct Answer: C
Rationale: In terminal stance, as the heel lifts, the body's weight pivots over the heads of the metatarsals. The MTP joints therefore act as the final fulcrum for the propulsive third rocker.
Question 99
A 35-year-old patient has an isolated paralysis of the tibialis anterior muscle. Which specific phase of the gait cycle will be most profoundly affected?
View Answer & Explanation
Correct Answer: C
Rationale: The tibialis anterior is the primary muscle of the first rocker. Its eccentric contraction controls plantarflexion during the loading response immediately following initial contact. Its paralysis leads to foot slap, the hallmark of first rocker failure.
Question 100
A surgeon performs a triple arthrodesis on a patient with a severe flatfoot deformity, as suggested by the clinical photo. By fusing the subtalar, talonavicular, and calcaneocuboid joints, the surgeon aims to restore a stable arch. However, this procedure inherently sacrifices motion, which will most significantly impair which rocker functions?
View Answer & Explanation
Correct Answer: B
Rationale: A triple arthrodesis stiffens the entire hindfoot and midfoot. This rigidity prevents the foot from adapting to surfaces and smoothly transferring weight from the ankle to the forefoot, thus impairing the transition from the second (ankle) to the third (forefoot) rocker.
