Lower Extremity Deformity Correction: Paley's Principles & Surgical Planning | Part 1
Key Takeaway
Orthopedic deformity correction involves restoring normal mechanical and anatomic axes using principles like CORA and specific osteotomy techniques. Planning requires full-length radiographs and understanding joint orientation angles. Surgical methods range from acute fixation to gradual correction with hexapod fixators, addressing malunions, knee, and hip deformities.
Question 1
A 45-year-old male presents with knee pain 2 years after a distal femur fracture treated with a plate. Radiographs reveal a valgus malunion. During preoperative planning, you identify the proximal and distal mechanical axes. According to Paley's principles, what is the definition of the Center of Rotation of Angulation (CORA)?
View Answer & Explanation
Correct Answer: B
Rationale: The CORA is the foundational concept in Paley's methodology and is defined as the point where the proximal and distal axes of a deformed bone intersect. The other options describe incorrect anatomical or conceptual points.
Question 2
A 28-year-old female presents with a tibial malunion characterized by pure medial translation of the distal segment by 15 mm, with no angular deformity. On radiographic analysis, what is the expected location of the CORA?
View Answer & Explanation
Correct Answer: D
Rationale: In a pure translation deformity, the proximal and distal axes are parallel and, by definition, never intersect. Therefore, the CORA is considered to be at infinity. This is a key biomechanical principle distinguishing it from angular deformities.
Question 3
A 50-year-old male has a femoral malunion with significant varus angulation and medial translation. A surgeon performs an osteotomy at the CORA and places the hinge of correction at the CORA. According to Paley's Osteotomy Rules, what is the expected outcome?
View Answer & Explanation
Correct Answer: C
Rationale: This scenario describes Paley's Rule 1. When the osteotomy and the hinge are both located at the CORA, a pure angular correction realigns the bone completely without inducing any secondary translation. This is the ideal but not always clinically achievable scenario.
Question 4
A 33-year-old construction worker has a tibial malunion where the CORA is located in the diaphysis. Due to poor soft tissue in the diaphysis, the surgeon decides to perform the corrective osteotomy in the proximal metaphysis. To achieve perfect realignment, what must be done at the osteotomy site according to Paley's principles?
View Answer & Explanation
Correct Answer: B
Rationale: This is a direct application of Paley's Rule 2. When the osteotomy is performed at a level different from the CORA, both angulation and translation are required at the osteotomy site to achieve a pure angular correction at the true CORA and restore the mechanical axis.
Question 5
A surgeon is correcting a femoral varus deformity. The CORA is identified in the diaphysis. The surgeon performs the osteotomy at the CORA but inadvertently places the corrective hinge on the medial cortex, away from the CORA. What is the most likely consequence of this action, as described by Paley's Rule 3?
View Answer & Explanation
Correct Answer: D
Rationale: Paley's Rule 3 states that if the hinge of correction is placed away from the CORA, the correction will induce an iatrogenic translation deformity, which will offset the mechanical axis. This is a common technical error if the hinge placement is not precise.
Question 6
A 35-year-old male presents with a painful left tibial malunion one year post-trauma. Radiographic analysis reveals a complex deformity. The AP view shows varus angulation and medial translation. The lateral view shows procurvatum angulation and posterior translation. What is the most likely classification of this deformity according to Paley's system?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of both angulation and translation on both orthogonal views is characteristic of an oblique plane deformity (Variant 2). In this type, the deformity exists in a single plane that is oblique to the standard AP and lateral radiographic beams.
Question 7
A surgeon is analyzing the radiographs of a patient with a tibial malunion, as shown in the image. The AP view shows varus and the lateral view shows procurvatum. What single radiographic finding is the most definitive proof that this is a Variant 2 oblique plane deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the definitive radiographic proof of a Variant 2 oblique plane deformity is that the CORA is located at the exact same horizontal (proximal-distal) level on both orthogonal views. This confirms that the apex of angulation and the point of translation are in the same plane.
Question 8
A 40-year-old motorcyclist sustained a femoral fracture that healed with a malunion. On the AP view, there is 30° of valgus. On the lateral view, there is 40° of procurvatum. Using the Pythagorean theorem, what is the magnitude of the true angulation in the oblique plane?
View Answer & Explanation
Correct Answer: D
Rationale: The true magnitude of a deformity in an oblique plane is calculated using the Pythagorean theorem: True Magnitude = √(AP component² + Lateral component²). In this case, √(30² + 40²) = √(900 + 1600) = √2500 = 50°.
Question 9
A 29-year-old patient has a tibial malunion. Preoperative planning using the graphic method reveals that the angulation vector and the translation vector perfectly overlap on the same line of action. What does this finding confirm?
View Answer & Explanation
Correct Answer: C
Rationale: The graphic method is used to visualize the relationship between deformity components. When the vectors for angulation and translation lie on the same line, it confirms they share the same plane of action, which is the definition of a Variant 2 oblique plane deformity.
Question 10
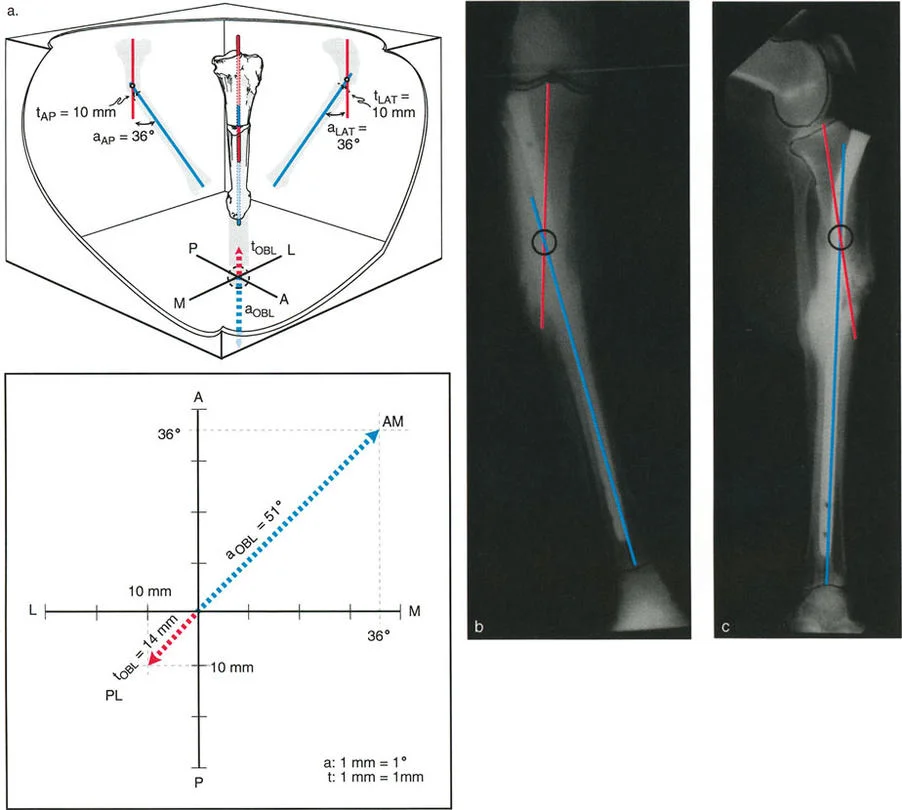
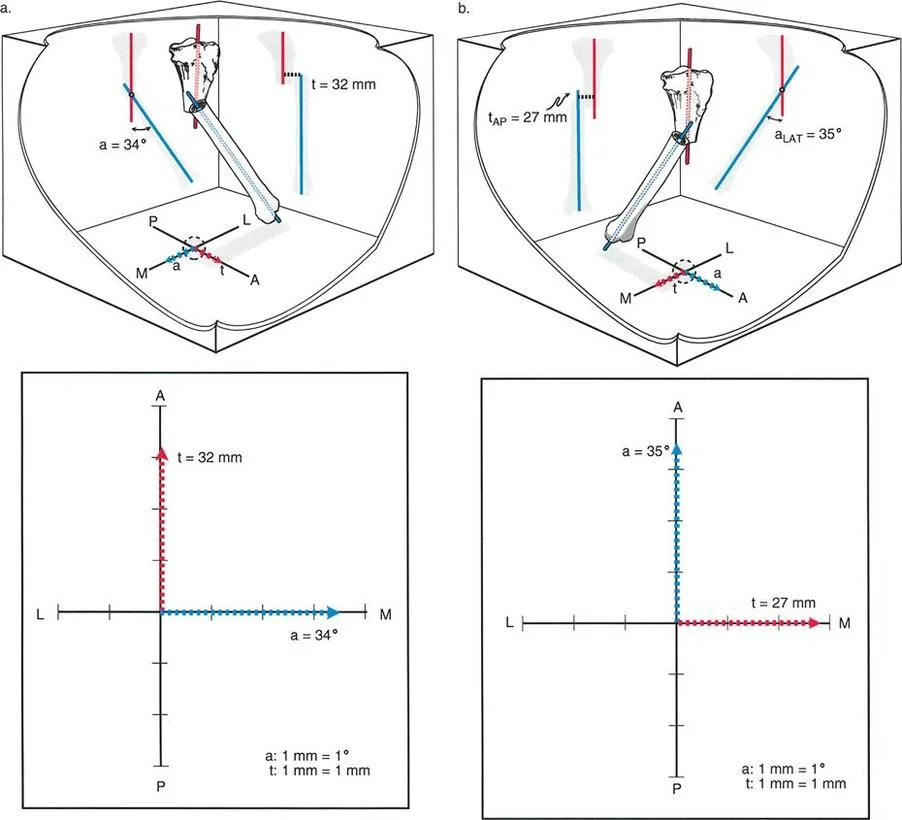
A 38-year-old female presents with a femoral malunion. The AP radiograph shows 34° of varus angulation with no medial or lateral translation. The lateral radiograph shows no procurvatum or recurvatum, but a 32 mm posterior translation of the distal segment. How is this deformity best classified?
View Answer & Explanation
Correct Answer: B
Rationale: This clinical picture perfectly describes a Type 2, Variant 1 deformity. One view (AP) shows pure angulation, while the orthogonal view (lateral) shows pure translation. This indicates the plane of angulation and the plane of translation are separated by exactly 90 degrees.
Question 11
A patient has a Type 2, Variant 1 tibial malunion with pure varus on the AP view and pure posterior translation on the lateral view. Where is the CORA for this specific type of deformity located?
View Answer & Explanation
Correct Answer: E
Rationale: Unlike an oblique plane deformity where the CORA is shifted, in a Type 2, Variant 1 deformity (orthogonal planes), the CORA is located exactly at the level of the malunion. This is because one view shows pure angulation, defining the apex at the fracture site.
Question 12
When using the graphic method to plan a correction for a Type 2, Variant 1 deformity (e.g., pure AP angulation, pure lateral translation), how would the angulation and translation vectors appear on the X-Y coordinate graph?
View Answer & Explanation
Correct Answer: C
Rationale: The graphic method for a Type 2, Variant 1 deformity will show one vector entirely on the horizontal (mediolateral) axis and the other entirely on the vertical (anteroposterior) axis. This creates a 90-degree separation, visually confirming the orthogonal nature of the deformity.
Question 13
A surgeon is planning an acute correction of a tibial malunion with both angulation and translation. An intramedullary nail is chosen for fixation. To prevent the bone from sliding back into its translated position during nail insertion, what adjunct is most critical?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically highlights the use of Poller (blocking) screws when using an intramedullary nail to correct a translated malunion. They act as a fulcrum to direct the nail and, more importantly, block the bone from shifting back into the translated deformity as the nail is passed.
Question 14
A 17-year-old has a severe, complex tibial angulation-translation deformity with significant soft tissue scarring from the initial injury. The surgeon is concerned about the risk of neurovascular compromise with an acute correction. What is the gold standard surgical approach in this scenario?
View Answer & Explanation
Correct Answer: D
Rationale: For severe or complex deformities, especially where acute correction poses a risk to the soft tissue envelope or neurovascular structures, gradual correction with a hexapod external fixator is considered the gold standard. This allows for slow, controlled realignment, minimizing risk.
Question 15
What is the primary advantage of using a hexapod external fixator for correcting an angulation-translation deformity where the osteotomy is performed away from the CORA?
View Answer & Explanation
Correct Answer: C
Rationale: The text emphasizes that hexapod systems use a virtual hinge. The surgeon inputs the deformity parameters, and the software calculates a strut adjustment schedule that simultaneously corrects angulation and translation, effectively performing a perfect, gradual Paley Rule 2 correction in 3D space without needing a physical hinge.
Question 16
A surgeon is treating a distal femoral valgus malunion. They misidentify the CORA and perform a medial opening wedge osteotomy in the metaphysis, ignoring a translational component. The postoperative AP radiograph shows a straight mechanical axis. What is the most common complication of this error?
View Answer & Explanation
Correct Answer: B
Rationale: The text identifies iatrogenic joint malorientation as the most common complication. By ignoring the translation and correcting the axis at the wrong level, the surgeon straightens the bone but tilts the joint line (altering the mLDFA), leading to abnormal joint mechanics and future arthritis.
Question 17
According to the provided surgical pearls, what is the most critical imaging requirement for accurately planning a lower extremity deformity correction?
View Answer & Explanation
Correct Answer: D
Rationale: The "Do's and Don'ts" table explicitly states to "DO obtain full-length, weight-bearing AP and LAT radiographs" and "DON'T rely on short, localized X-rays." This is because the mechanical axis can only be assessed by seeing the hip, knee, and ankle centers on a single image.
Question 18
A surgeon is performing an osteotomy for gradual correction with an external fixator. To maximize the potential for bone healing, what is the recommended technique for creating the bone cut?
View Answer & Explanation
Correct Answer: D
Rationale: The surgical pearls table recommends a low-energy, multi-drill hole osteotomy (corticotomy) to preserve the periosteal blood supply. This is contrasted with a high-speed saw, which can cause thermal necrosis and inhibit healing, a major concern in deformity correction.
Question 19
A 42-year-old patient has a tibial malunion with 20 mm of pure lateral translation. The surgeon corrects the translation but does not address the joint orientation angles. What is the primary consequence of this isolated correction?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that pure translation shifts the mechanical axis parallel to itself without altering joint orientation angles. Correcting only the translation at the bone level without considering the overall axis will simply move the entire malaligned axis back to the center, but the axis itself remains parallel to its deformed state.
Question 20
If a surgeon only corrects the angulation of a combined angulation-translation deformity and ignores the translation, what will be the persistent clinical problem?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly explains this pitfall: "If a surgeon only corrects the angulation and ignores the translation, the joint orientation angles may be restored, but the limb will remain mechanically malaligned (a persistent MAD)." The goal is to restore both joint orientation and mechanical axis.
Question 21
A 31-year-old patient has an oblique plane tibial deformity. If a special radiograph were taken perfectly perpendicular to the true plane of deformity, what would be observed regarding the measured angulation and translation?
View Answer & Explanation
Correct Answer: D
Rationale: The text explains that an X-ray beam perpendicular to the oblique plane reveals the true, maximum deformity. The apparent deformities on the AP and lateral views are merely projections (or "shadows") of this true deformity and will always be of lesser magnitude.
Question 22
Conversely, if a radiograph of an oblique plane deformity is taken perfectly in-line with (parallel to) the plane of deformity, what would the radiograph show?
View Answer & Explanation
Correct Answer: B
Rationale: This is the conceptual opposite of the previous question. The text states, "a radiograph taken perfectly in-line with the oblique plane will show a perfectly straight bone with zero deformity." This is because you are looking "down the barrel" of the deformity plane, making it invisible.
Question 23
A 45-year-old male presents with medial-sided knee pain and a varus deformity of his left lower extremity. A long-leg standing radiograph is obtained for preoperative planning. According to the principles of deformity correction, what is the primary biomechanical goal of surgical intervention?
View Answer & Explanation
Correct Answer: C
Rationale: The primary objective of lower limb deformity correction is to restore the Mechanical Axis Deviation (MAD) to normal, ensuring the ground reaction force vector passes through the center of the knee. This optimizes load distribution. Restoring the anatomic axis (A) is the goal of IM nailing but not the primary biomechanical goal for the limb. The other options are incorrect geometric goals.
Question 24
A 30-year-old patient has a femoral malunion after a motorcycle accident. During preoperative planning, the surgeon defines the mechanical axis of the femur. Which of the following correctly defines this axis?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis of a bone is defined as a line connecting the center points of the proximal and distal joints. For the femur, this is from the center of the femoral head to the center of the knee. The line bisecting the medullary canal (A) is the anatomic axis.
Question 25
A 28-year-old female has a tibial malunion with varus deformity. The surgeon is planning a correction with an intramedullary nail. Which of the following best describes the anatomic axis of the tibia, which is critical for this type of planning?
View Answer & Explanation
Correct Answer: B
Rationale: The anatomic axis is a line that bisects the medullary canal (the mid-diaphyseal line). This is particularly relevant for intramedullary fixation. The line from the center of the knee to the center of the ankle (C) describes the mechanical axis of the tibia.
Question 26
A surgeon is evaluating a normal femur on a long-leg radiograph. When comparing the mechanical and anatomic axes of the femur, what is the expected relationship between these two lines?
View Answer & Explanation
Correct Answer: D
Rationale: In the femur, the anatomic axis (mid-diaphyseal line) is not parallel to the mechanical axis (hip center to knee center). The angle between them, the Anatomic-Mechanical Angle (AMA), is approximately 7 degrees. In the tibia, the axes are essentially parallel and superimposed (A).
Question 27
A 55-year-old female is being evaluated for a distal femoral varus deformity. Preoperative planning requires knowledge of normal joint orientation angles. What is the average normal value for the Mechanical Lateral Distal Femoral Angle (mLDFA)?
View Answer & Explanation
Correct Answer: C
Rationale: The average normal mLDFA is 87° (Range 85°–90°). This angle is formed by the mechanical axis of the femur and the distal femoral joint line. An mLDFA of 81° (A) is the average for the anatomic LDFA (aLDFA).
Question 28
A 62-year-old male is undergoing planning for a high tibial osteotomy to correct varus malalignment. The surgeon measures the angle between the tibial mechanical axis and the proximal tibial joint line. What is the average normal value for this angle, the Mechanical Proximal Tibial Angle (MPTA)?
View Answer & Explanation
Correct Answer: C
Rationale: The average normal MPTA is 87° (Range 85°–90°). It is a critical reference angle for assessing tibial deformity. An angle less than 85° indicates a varus deformity of the proximal tibia.
Question 29
A 25-year-old patient with a history of a subtrochanteric fracture malunion presents for corrective osteotomy. The surgeon is evaluating the orientation of the proximal femur. What is the average normal value for the Lateral Proximal Femoral Angle (LPFA)?
View Answer & Explanation
Correct Answer: D
Rationale: The average normal LPFA is 90° (Range 85°–95°). This angle is formed by the proximal femoral mechanical axis and a line from the tip of the greater trochanter to the center of the femoral head. It is used to assess for proximal femoral (hip) joint malorientation.
Question 30
A 35-year-old patient has a history of a pilon fracture with subsequent valgus malunion of the distal tibia. When performing deformity analysis, the surgeon measures the Lateral Distal Tibial Angle (LDTA). What is the average normal value for this angle?
View Answer & Explanation
Correct Answer: D
Rationale: The average normal LDTA is 89° (Range 86°–92°). This angle assesses the orientation of the ankle joint relative to the tibial axis. A value greater than 92° would indicate a valgus deformity at the ankle.
Question 31
A surgeon is performing anatomic axis planning for a femoral malunion that will be treated with an intramedullary nail. The surgeon needs to assess the distal femoral joint orientation relative to the anatomic axis. What is the average normal value for the Anatomic Lateral Distal Femoral Angle (aLDFA)?
View Answer & Explanation
Correct Answer: A
Rationale: The average normal aLDFA is 81° (Range 79°–83°). This is different from the mLDFA (87°) because it is measured relative to the anatomic axis, which is angled 7° valgus relative to the mechanical axis in the diaphysis.
Question 32
A 68-year-old female with severe medial compartment osteoarthritis presents with a varus thrust gait. On a standing long-leg radiograph, the angle between the distal femoral joint line and the proximal tibial joint line is measured to be 4 degrees, with the lines converging medially. What is the significance of this increased Joint Line Convergence Angle (JLCA)?
View Answer & Explanation
Correct Answer: C
Rationale: A normal JLCA is 0°–2°. A JLCA greater than 2° is a red flag indicating that the knee joint itself is opening up, which can be due to severe cartilage wear (intra-articular deformity) or ligamentous stretching (e.g., LCL laxity in varus). It complicates planning because the tibia and femur cannot be planned in isolation.
Question 33
A 40-year-old carpenter sustained a tibial shaft fracture that healed in 15 degrees of varus. He is scheduled for a corrective osteotomy and fixation with a long intramedullary nail. Which deformity planning method is most practical and directly applicable to this surgical plan?
View Answer & Explanation
Correct Answer: C
Rationale: Anatomic axis planning is highly practical for tibial deformities treated with an intramedullary nail because the nail will dictate the alignment of the medullary canal (the anatomic axis). This method allows the surgeon to accurately predict the postoperative alignment based on the hardware. Mechanical axis planning (B) is also valid but less direct when an IM nail is used.
Question 34
A surgeon is performing anatomic axis planning for a mid-diaphyseal tibial malunion. According to Paley's principles, what is the first step in this process?
View Answer & Explanation
Correct Answer: B
Rationale: The first step in anatomic axis planning for a diaphyseal deformity is to define the anatomic axes of the bone segments involved. This is done by drawing lines that bisect the medullary canal in the proximal and distal segments relative to the deformity.
Question 35
During anatomic axis planning for a tibial deformity, the surgeon measures the Mechanical Proximal Tibial Angle (MPTA) and finds it to be 78° (normal 87°). How should the proximal anatomic axis line be correctly drawn for deformity analysis?
View Answer & Explanation
Correct Answer: B
Rationale: If the MPTA is abnormal, it indicates a second, juxta-articular deformity. The existing proximal mid-diaphyseal line cannot be used as the reference axis. A new, "correct" anatomic axis must be drawn based on the joint line, using either the contralateral normal MPTA or the population average of 87° as the target.
Question 36
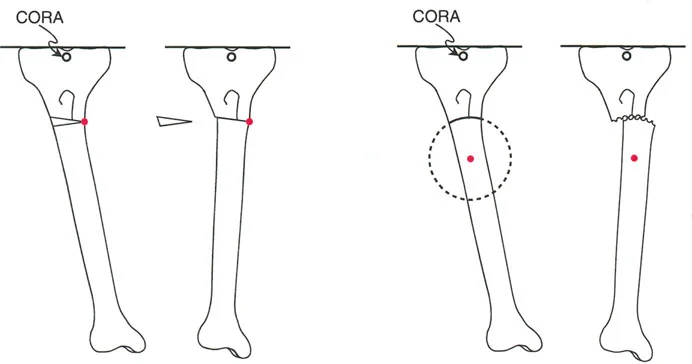
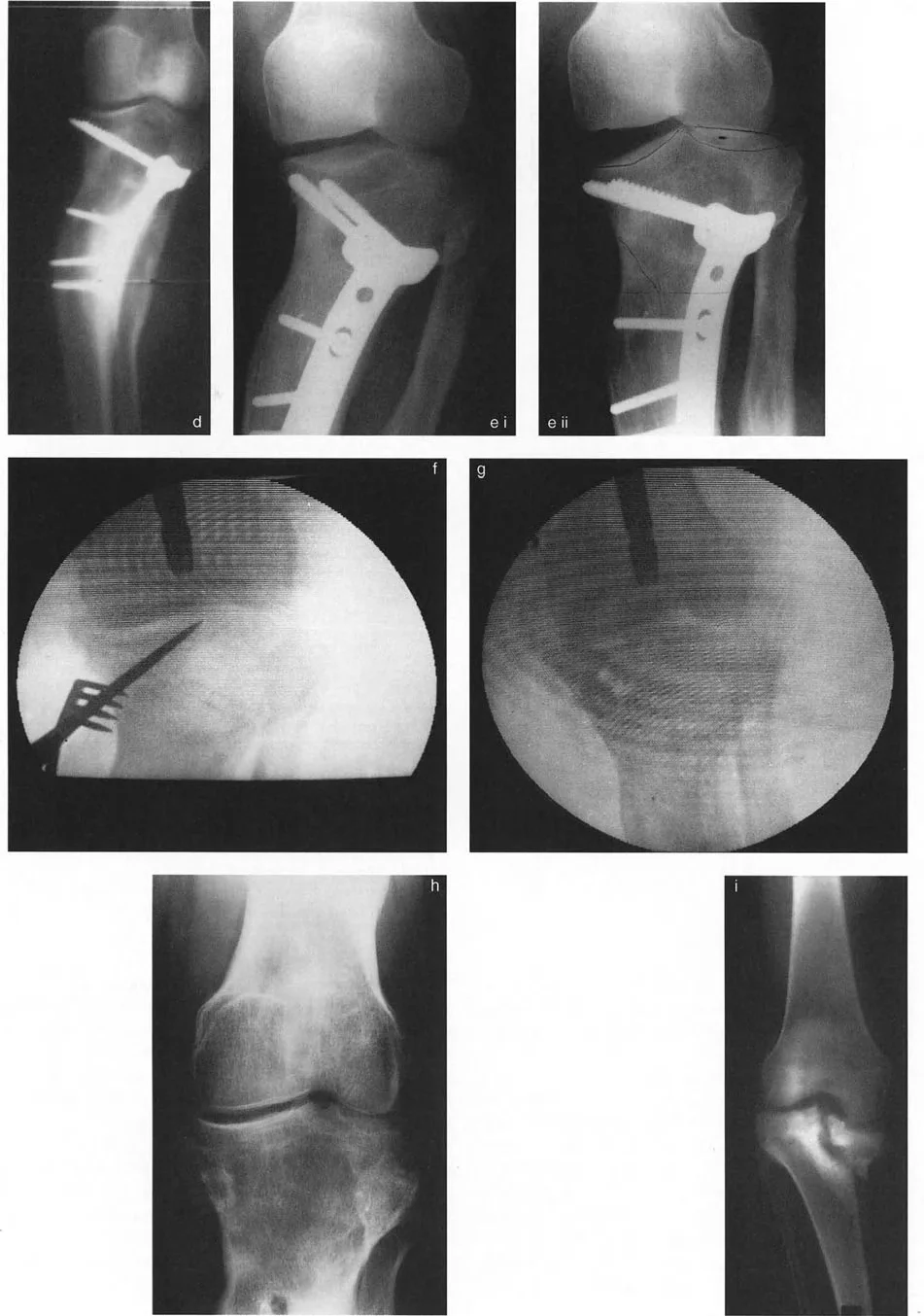
A 33-year-old patient has a uniapical varus deformity of the tibia. The surgeon performs anatomic axis planning as shown in the image. What does the intersection point of the proximal and distal anatomic axis lines represent?
View Answer & Explanation
Correct Answer: B
Rationale: The intersection of the proximal and distal axis lines (whether mechanical or anatomic) defines the Center of Rotation of Angulation (CORA). This is the apex of the deformity. While the osteotomy is often performed at the CORA (A), the point itself is defined as the CORA.
Question 37
A 29-year-old patient has a tibial malunion with 15 degrees of varus and 30 degrees of external rotation. The surgeon is concerned about the accuracy of planning on a standard AP radiograph. In cases of severe rotational deformity, which planning method is generally preferred for its accuracy?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text states that anatomic axis planning can be less accurate because its starting points are sensitive to tibial rotation. It explicitly mentions that if severe rotational deformity exists, mechanical axis planning is preferred. While CT-based planning (C) is an excellent modern tool, based on the provided text, mechanical axis planning is the preferred 2D radiographic method.
Question 38
A resident is learning femoral mechanical axis planning for a varus deformity. What is the critical difference in the starting point of this process compared to tibial planning?
View Answer & Explanation
Correct Answer: B
Rationale: A key principle highlighted is that femoral mechanical axis planning starts *distally* at the knee by establishing the Distal Mechanical Axis (DMA). In contrast, tibial planning typically starts proximally at the knee. Starting at the hip (A) is the second step of femoral planning.
Question 39
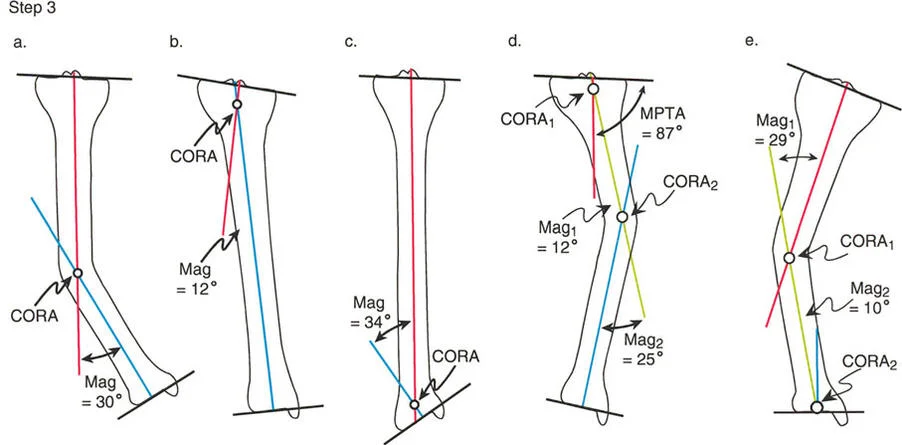
A 22-year-old male presents with a 15-degree varus deformity of the proximal tibia. Preoperative planning identifies the Center of Rotation of Angulation (CORA) in the metaphysis. The surgeon performs a transverse osteotomy and places the axis of correction (hinge) exactly at the CORA. According to Paley's Osteotomy Rules, what is the expected geometric outcome?
View Answer & Explanation
Correct Answer: A
Rationale: This scenario describes Paley's Osteotomy Rule 1. When the osteotomy and the hinge are both placed at the CORA, pure angulation occurs, and the mechanical axes of the proximal and distal segments become perfectly collinear. Rule 2 involves the osteotomy being at a different level than the CORA, which causes angulation and translation at the bone ends.
Question 40
A 35-year-old female undergoes a distal femoral osteotomy for a valgus deformity. The surgeon intentionally performs the osteotomy 3 cm proximal to the CORA to achieve better bone contact but places the hinge of correction at the CORA. To achieve a collinear mechanical axis, what additional maneuver is required?
View Answer & Explanation
Correct Answer: B
Rationale: This is a clinical application of Paley's Osteotomy Rule 2, the basis for the angulation-translation (a-t) osteotomy. When the osteotomy is performed at a level different from the CORA (but the hinge remains at the CORA), the bone ends must be translated relative to each other to make the mechanical axes collinear. Failure to translate results in a secondary deformity.
Question 41
A 40-year-old male is evaluated 6 months after a tibial osteotomy for varus malunion. Postoperative radiographs show that the angular deformity is corrected, but the mechanical axis remains deviated medially. The surgeon's notes indicate the osteotomy and hinge were both performed 4 cm distal to the true CORA. This outcome is a classic example of violating which of Paley's Osteotomy Rules?
View Answer & Explanation
Correct Answer: C
Rationale: Paley's Osteotomy Rule 3 states that if both the osteotomy and the hinge are placed at a level different from the CORA, a secondary translation deformity will be induced. This results in parallel but non-collinear mechanical axes and a persistent mechanical axis deviation (MAD), as described in the vignette.
Question 42
A surgeon plans a proximal tibial osteotomy for a 20-degree varus deformity. The CORA is located in a region with poor soft tissue coverage. To mitigate wound healing risks, the surgeon decides to perform the osteotomy in the more muscular diaphysis. What is the primary biomechanical advantage of performing an angulation-translation (a-t) osteotomy in this scenario?
View Answer & Explanation
Correct Answer: C
Rationale: A key reason to perform an a-t osteotomy (moving the cut away from the CORA) is to improve bone contact. By translating the fragments, the cortical corner of one segment can be impacted into the medullary canal of the other, creating a "dovetail" effect that significantly increases intrinsic stability and the surface area for healing.
Question 43
A 28-year-old female with a 25-degree proximal tibia valgus deformity is scheduled for an acute corrective osteotomy. During the procedure, which neurovascular structure is at the highest risk of a traction injury if a lateral opening wedge technique is used?
View Answer & Explanation
Correct Answer: D
Rationale: In a valgus (knock-knee) deformity, the lateral side is convex. An opening wedge on the lateral side will place maximum stretch on the structures on this convex side. The common peroneal nerve is located laterally and is tethered at the fibular neck, making it highly susceptible to traction injury during acute valgus correction.
Question 44
A surgeon is planning an opening wedge osteotomy. The biomechanical principle of "convex side peril" dictates that neurovascular structures are most vulnerable to stretch when they are located on the convex side of the deformity. Why is this the case?
View Answer & Explanation
Correct Answer: C
Rationale: As the angular correction occurs, the convex side of the bone travels along the longest arc. This results in the greatest excursion and stretch on the soft tissue envelope on that side. Nerves, with their limited elasticity, are particularly at risk when located on the convex side of an acute correction.
Question 45
A 19-year-old male presents with a 15-degree tibia vara deformity and a 2.5 cm limb length discrepancy (LLD), with the affected leg being shorter. Which of the following osteotomy techniques would be most appropriate to address both deformities simultaneously?
View Answer & Explanation
Correct Answer: C
Rationale: An opening wedge osteotomy inherently lengthens the bone. For a tibia vara (bowleg) deformity, a medial opening wedge corrects the varus alignment while simultaneously increasing the length of the limb, making it the ideal choice to address both the angular deformity and the LLD.
Question 46
A 55-year-old female with severe medial compartment knee osteoarthritis undergoes a high tibial osteotomy using a medial opening wedge technique and a locking plate. For optimal biomechanical stability and load sharing, where should the plate be placed?
View Answer & Explanation
Correct Answer: B
Rationale: The biomechanically superior location for a plate in an opening wedge osteotomy is the concave side. This placement utilizes the tension band principle. The intact cortical hinge on the convex side absorbs compressive forces, while the plate on the concave side resists tensile forces, creating a stable, load-sharing construct.
Question 47
A surgeon places a plate on the convex side of an opening wedge osteotomy without using a structural bone graft. What is the most likely mechanism of hardware failure?
View Answer & Explanation
Correct Answer: C
Rationale: Placing a plate on the convex side makes it a load-bearing device. Without a structural support (like an intact hinge or bone graft) on the concave side to absorb compression, the plate is subjected to massive bending forces with every step. This cyclic loading leads to metal fatigue and eventual plate breakage.
Question 48
A 30-year-old patient has a complex, multiplanar 45-degree tibial deformity with poor overlying soft tissues. The surgeon desires the most accurate correction possible with minimal risk to the soft tissue envelope. Which of the following strategies is most appropriate?
View Answer & Explanation
Correct Answer: C
Rationale: Gradual correction with an external fixator is the safest and most accurate method for large, complex deformities, especially with compromised soft tissues. It avoids the acute stretch on neurovascular structures and allows for postoperative adjustments based on weight-bearing radiographs to achieve a perfect mechanical axis. The principle of distraction osteogenesis allows the soft tissues to adapt gradually.
Question 49
During an acute opening wedge osteotomy of the femur, the surgeon uses an oscillating saw to perform the bone cut. To minimize the risk of non-union, what is the most critical intraoperative step to prevent thermal necrosis?
View Answer & Explanation
Correct Answer: C
Rationale: The friction from a saw blade generates significant heat, which can cause thermal necrosis of the bone ends and lead to non-union. The most effective way to prevent this is to use a sharp blade (which cuts with less friction) and to dissipate heat continuously with copious chilled saline irrigation directly on the cutting surface.
Question 50
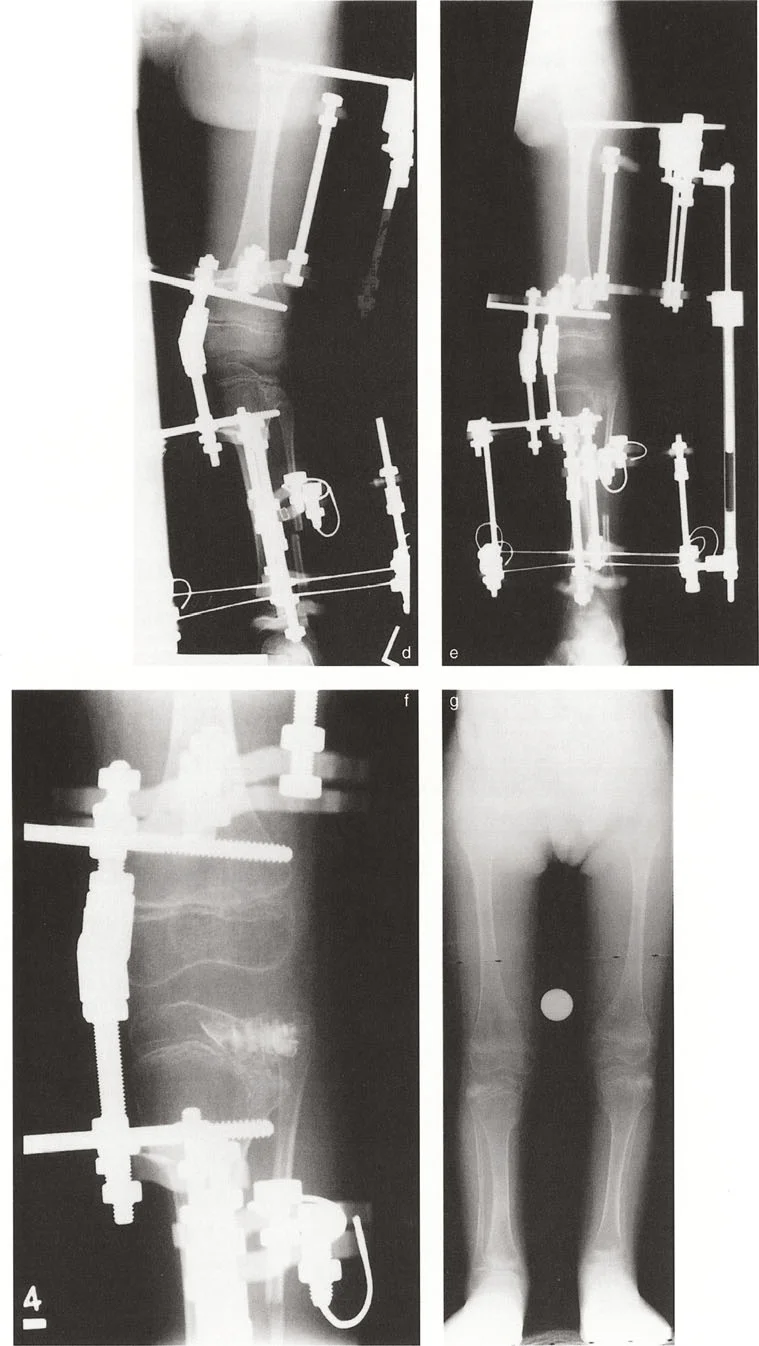
A surgeon is performing a Fixator-Assisted Nailing (FAN) for a diaphyseal tibial deformity. A temporary external fixator is applied prior to the osteotomy. What is the primary purpose of this temporary fixator?
View Answer & Explanation
Correct Answer: D
Rationale: In FAP and FAN techniques, the temporary external fixator is a reduction tool. After the osteotomy, it is used to "dial in" the perfect angular and translational correction and hold it rigidly. Once the mechanical axis is perfectly restored, the definitive internal fixation (plate or nail) is applied, and the fixator is then removed.
Question 51
The "dome osteotomy" used for deformity correction in long bones is geometrically best described as having what shape?
View Answer & Explanation
Correct Answer: D
Rationale: Despite its name, the dome osteotomy in long bones is not a true spherical dome. It is a cylindrical (or barrel vault) cut. This geometry allows for rotation around the central axis of the cylinder, enabling large angular corrections while maintaining excellent bone-to-bone contact.
Question 52
For a focal dome osteotomy to achieve pure angular correction without inducing a secondary translation of the mechanical axis, what geometric condition must be met?
View Answer & Explanation
Correct Answer: B
Rationale: The geometric principle of the focal dome osteotomy is that it behaves like a Rule 2 correction. To ensure the mechanical axes become collinear without a secondary shift, the pivot point of the correction—which is the central axis of the cylindrical cut—must be perfectly aligned with the preoperatively determined CORA.
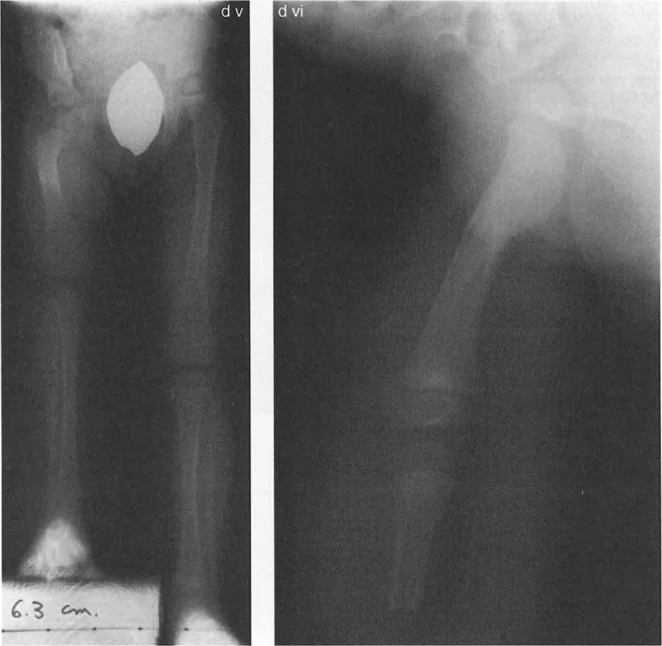
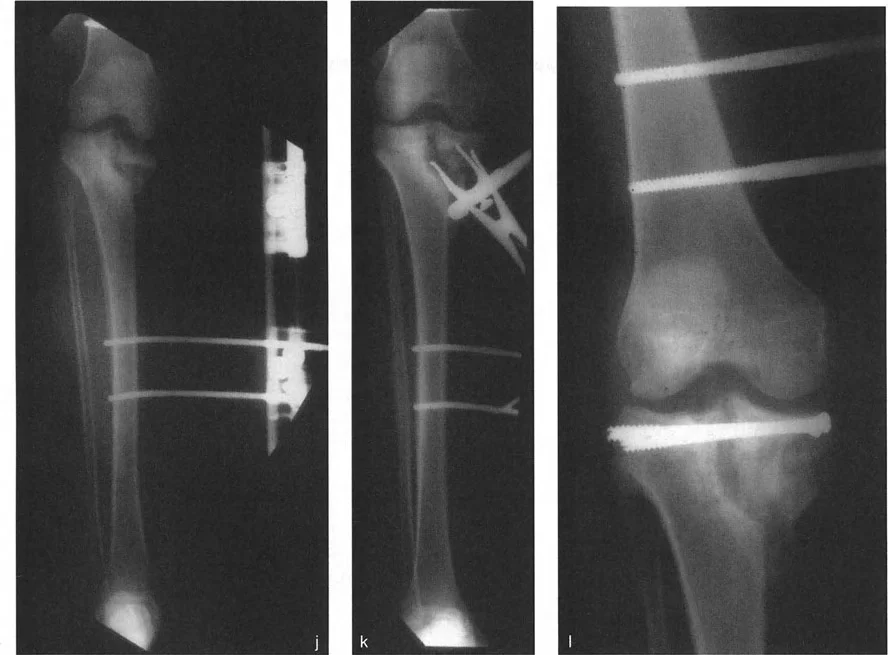
Question 53
A 17-year-old male undergoes an acute correction of a 30-degree tibial recurvatum deformity using a focal dome osteotomy and an intramedullary nail, as shown in the image. Due to the significant lengthening of the anterior soft tissues, what prophylactic surgical procedure is mandatory to prevent a serious postoperative complication?
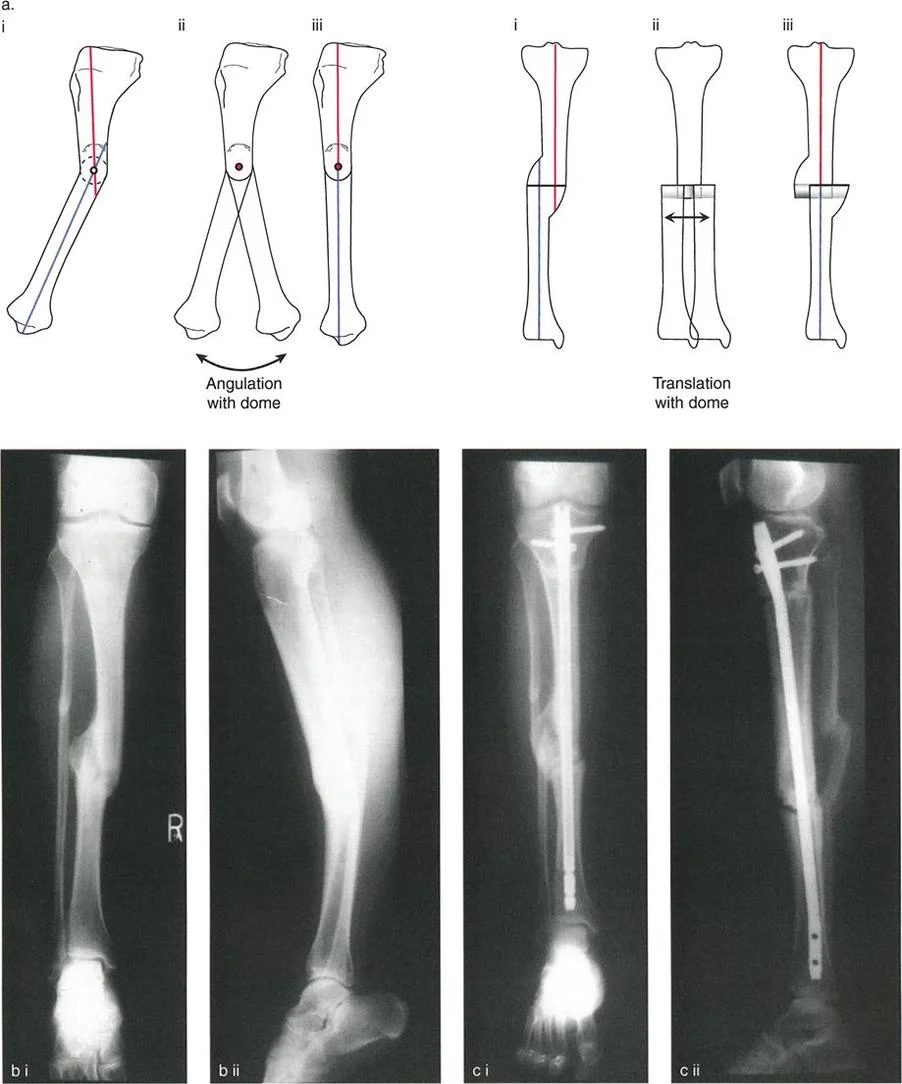
View Answer & Explanation
Correct Answer: D
Rationale: Correcting a recurvatum (hyperextension) deformity involves acutely lengthening the anterior aspect of the limb. This places significant tension on the muscles and fascia of the anterior compartment, dramatically increasing intra-compartmental pressure. A prophylactic anterior compartment fasciotomy is required to prevent acute compartment syndrome.
Question 54
What is the primary biomechanical advantage of a focal dome osteotomy compared to a simple transverse opening wedge osteotomy for large angular corrections?
View Answer & Explanation
Correct Answer: C
Rationale: The cylindrical shape of the dome osteotomy allows the bone ends to rotate along the arch, maintaining a massive surface area of contact throughout the correction. This provides excellent intrinsic stability against shear forces and promotes rapid healing, unlike a simple wedge osteotomy which creates a large gap.
Question 55
A surgeon is preparing to perform a focal dome osteotomy on a large adult tibia. What is the standard technique for creating the precise, large-radius cylindrical cut?
View Answer & Explanation
Correct Answer: E
Rationale: For large bones like the femur or tibia, creating a custom, large-radius dome is technically demanding. The standard and most precise method is the multiple drill hole technique. A central K-wire acts as a pivot, and a guide is used to make a series of parallel drill holes in a perfect arc, which are then connected to complete the osteotomy.
Question 56
A 25-year-old patient presents with a complex 3D deformity of the femur, including 20 degrees of varus and 30 degrees of internal rotation malunion. The surgeon wishes to correct both deformities acutely through a single osteotomy with maximal bone contact. What is the primary limitation of using a standard cylindrical dome osteotomy for this case?
View Answer & Explanation
Correct Answer: C
Rationale: The primary limitation of a standard cylindrical dome osteotomy is its inability to correct axial rotation. The bone ends are constrained by the walls of the cylinder, and any attempt to twist them results in incongruence and loss of contact. Advanced modifications like the inclined or helical dome are required for combined angular and rotational corrections.
Question 57
A surgeon is treating a patient with severe femoral anteversion combined with a valgus deformity. To achieve simultaneous acute correction of both angulation and rotation with maximal bony apposition, which specialized osteotomy technique is most appropriate?
View Answer & Explanation
Correct Answer: D
Rationale: The Nishio helical dome osteotomy is specifically designed to address combined angular and rotational deformities. By creating a helical or spiral cut, the osteotomy surfaces can slide along each other, allowing for simultaneous, coupled correction of angulation and axial rotation while maintaining excellent bone contact.
Question 58
During a Fixator-Assisted Nailing (FAN) procedure for a proximal tibial varus deformity, the surgeon notes that after inserting the nail, the deformity tends to recur because the nail sits in the wide metaphyseal canal. What adjunct fixation can be used to prevent this loss of reduction?
View Answer & Explanation
Correct Answer: B
Rationale: Poller, or blocking, screws are used to solve this exact problem. By placing a screw on the concave side of the deformity (in this case, medially), the surgeon artificially narrows the medullary canal. This forces the nail to follow the desired corrected mechanical axis and prevents it from shifting back into the original deformed position.
Question 59
A 60-year-old male undergoes a distal femoral osteotomy with a "Step Plate" fixation. What is the primary biomechanical function of the step-cut in the bone that matches the plate?
View Answer & Explanation
Correct Answer: C
Rationale: The "Step Plate" concept is designed to protect the screws from shear stress. The bony step abuts the plate directly, creating a path of least resistance for axial load to be transferred from the bone into the plate itself. This offloads the screws, reducing the risk of toggling, back-out, or breakage.
Question 60
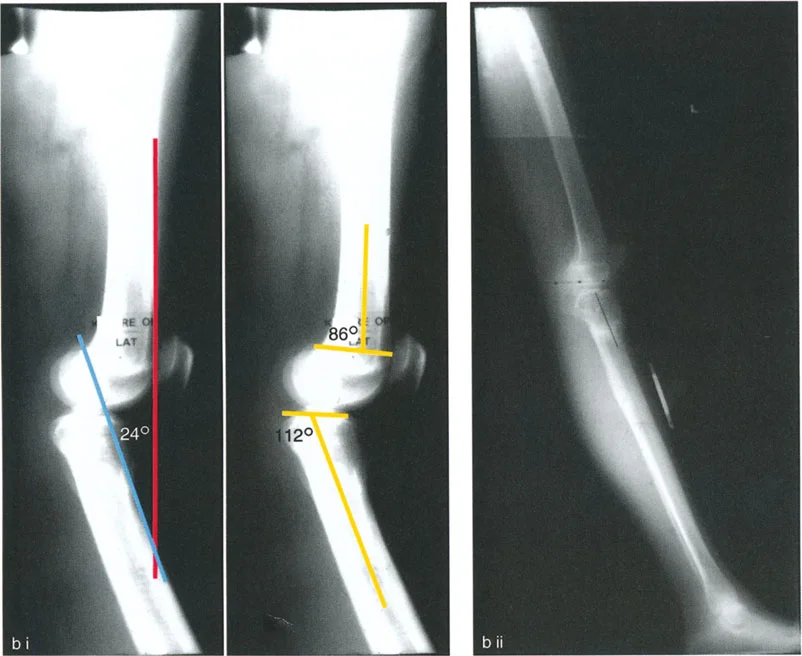
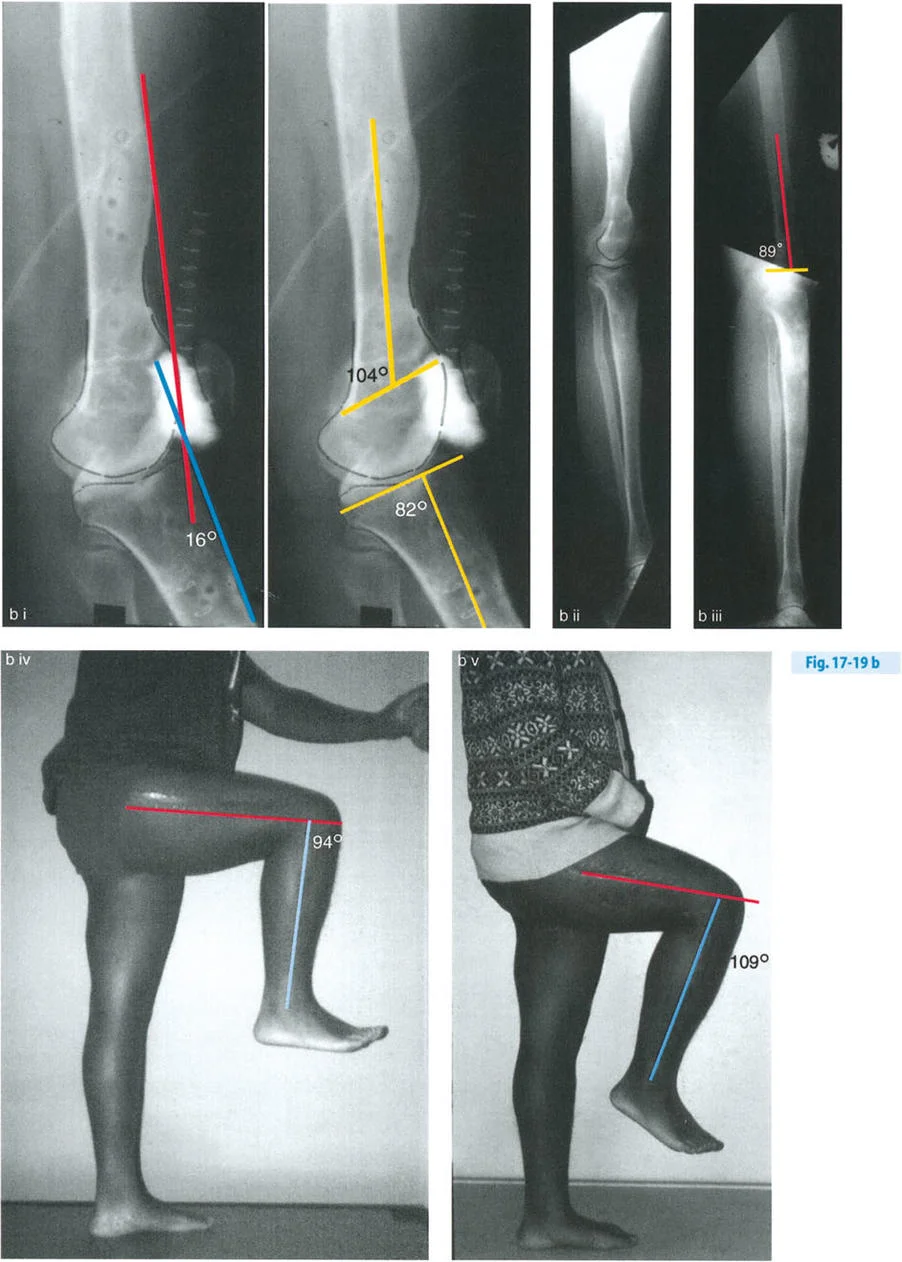
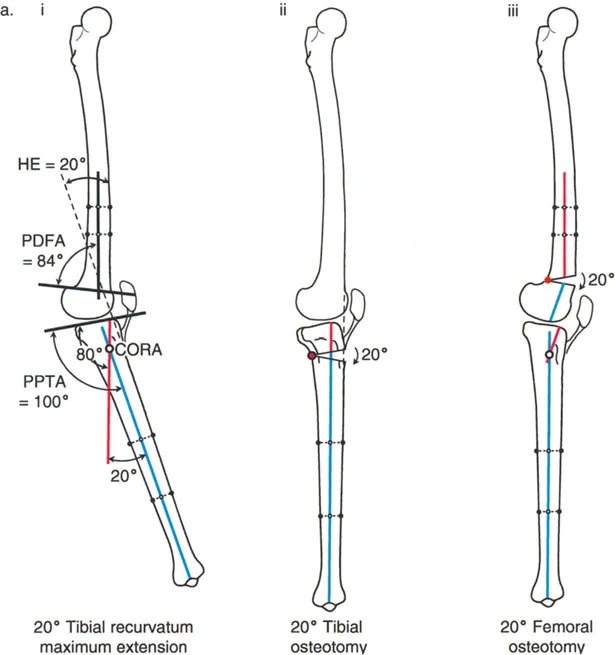
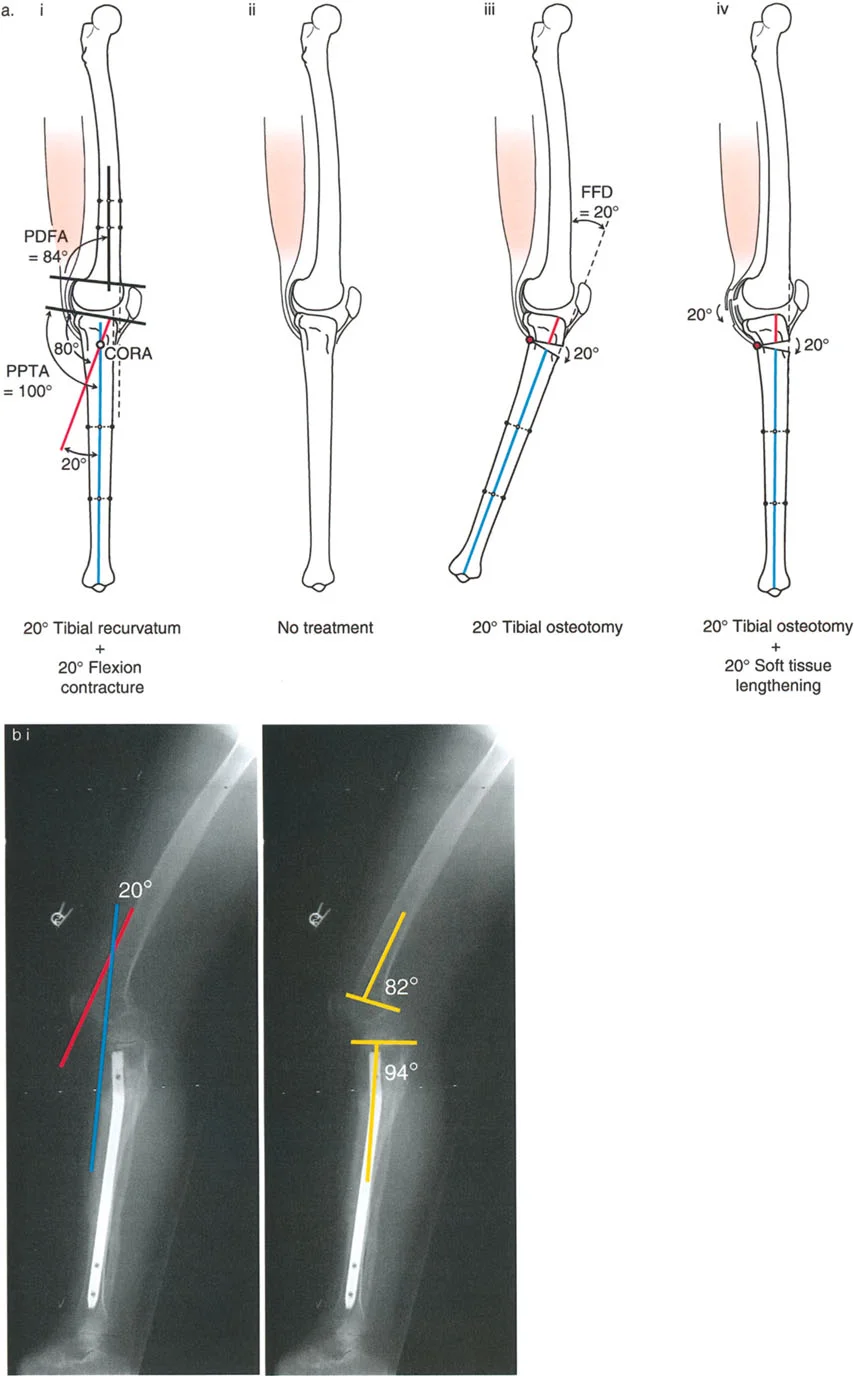
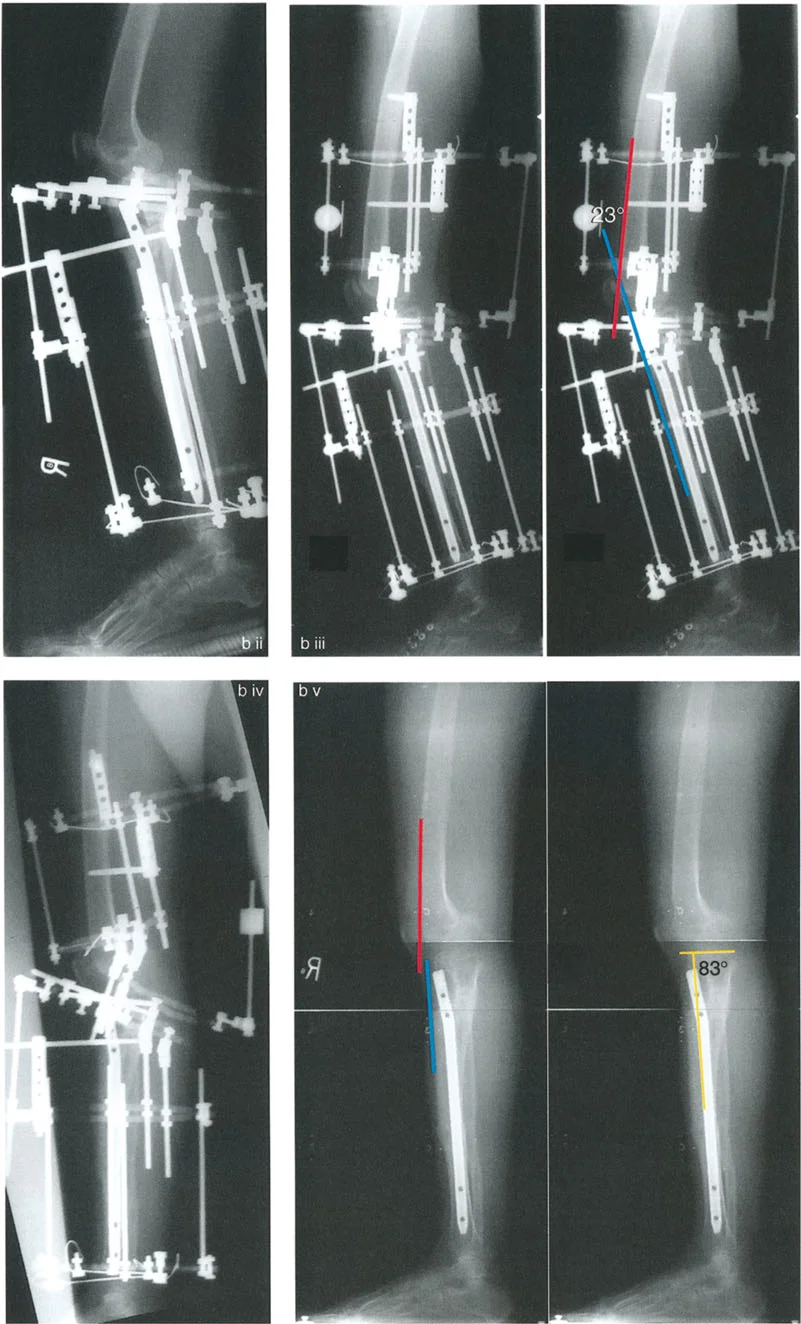
A 19-year-old male with a history of a distal femur physeal injury presents with knee hyperextension (HE). On examination, he has 20° of knee HE. A standing lateral radiograph shows a posterior distal femoral angle (PDFA) of 104° and a posterior proximal tibial angle (PPTA) of 80°. Based on the provided diagram, what is the source of his deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The normal PDFA is approximately 83°. A PDFA of 104° indicates a 21° distal femoral recurvatum deformity (104°-83° ≈ 20°). The PPTA of 80° is within the normal range. Since the clinical HE of 20° matches the bony femoral deformity, the source is isolated distal femoral recurvatum. Tibial recurvatum would be indicated by an abnormally high PPTA.
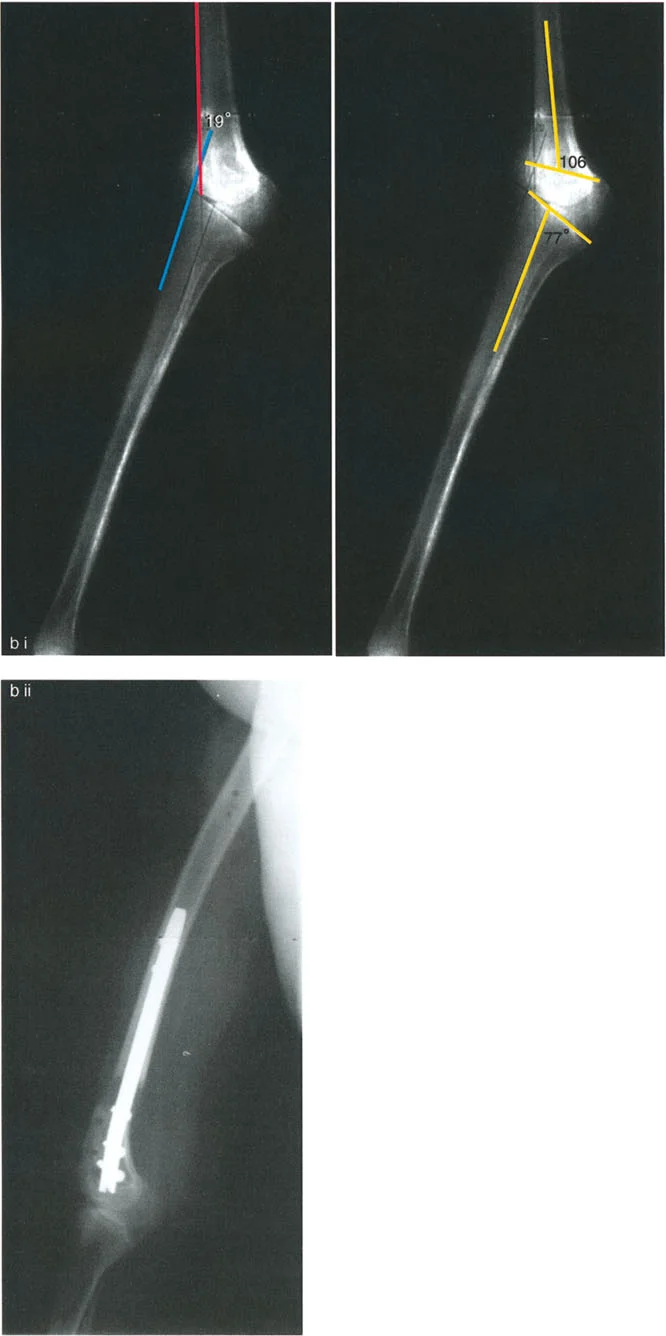
Question 61
A 22-year-old female with a history of poliomyelitis presents with symptomatic knee recurvatum. Examination reveals 19° of hyperextension. Radiographs show a PDFA of 106° and a PPTA of 77°. What is the most appropriate treatment to correct her deformity and maintain neutral knee extension?
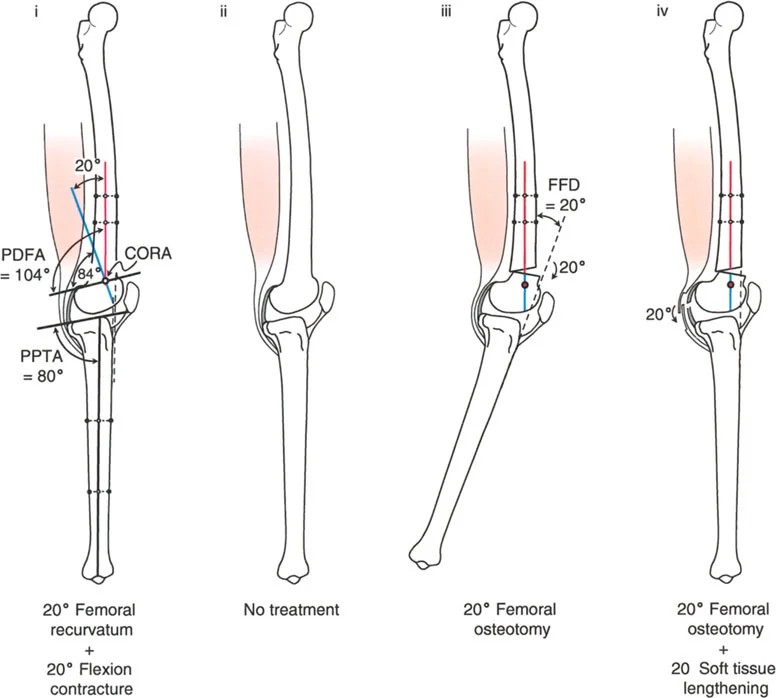
View Answer & Explanation
Correct Answer: B
Rationale: The deformity is located in the distal femur, as indicated by the abnormal PDFA of 106° (normal ~83°), representing approximately 23° of recurvatum. The PPTA is normal. The principle of deformity correction is to perform the osteotomy at the level of the Center of Rotation of Angulation (CORA), which is in the distal femur. A distal femoral flexion osteotomy will correct the alignment. A tibial osteotomy would create a compensatory deformity.
Question 62
A patient has a 20° knee hyperextension deformity secondary to distal femoral recurvatum (PDFA = 104°, PPTA = 80°). If the surgeon incorrectly performs a 20° proximal tibial flexion osteotomy instead of a femoral osteotomy, what is the most likely clinical and radiographic outcome?
View Answer & Explanation
Correct Answer: D
Rationale: Correcting a femoral deformity with a tibial osteotomy creates a new, compensatory deformity. While the overall limb alignment and knee extension may become neutral, the joint orientation will be abnormal. The combination of femoral recurvatum and iatrogenic tibial flexion will make the tibia appear translated anteriorly relative to the femur, altering joint kinematics. Patella baja is a risk of tibial osteotomies proximal to the tubercle, not the primary outcome of this specific mismatch.
Question 63
A 30-year-old patient is evaluated for an abnormal gait. On examination, the knee has a full range of motion from 0° to 120°. A lateral radiograph reveals a PDFA of 104° and a PPTA of 80°. Despite the significant femoral recurvatum, the patient does not exhibit clinical hyperextension. What is the most likely explanation for this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The patient has a 21° femoral recurvatum deformity (PDFA 104°). The absence of clinical hyperextension (HE=0°) indicates that the bony deformity is perfectly balanced by an equal and opposite soft tissue knee flexion contracture of 21°. This is a common compensatory mechanism. If there were no flexion contracture, the patient would exhibit 21° of clinical HE.
Question 64
A patient has a 20° distal femoral recurvatum deformity that is fully compensated by a 20° soft tissue flexion contracture, resulting in 0° of maximum knee extension. If a surgeon performs a 20° distal femoral flexion osteotomy to normalize the PDFA, what is the most probable postoperative outcome?
View Answer & Explanation
Correct Answer: B
Rationale: This scenario is described as the "worst of all possible treatment choices." Correcting the bony deformity without addressing the co-existing soft tissue flexion contracture will "unmask" the contracture. The osteotomy removes the bony block to flexion (the recurvatum), and the knee's maximum extension will now be limited by the soft tissues, resulting in a 20° fixed flexion deformity.
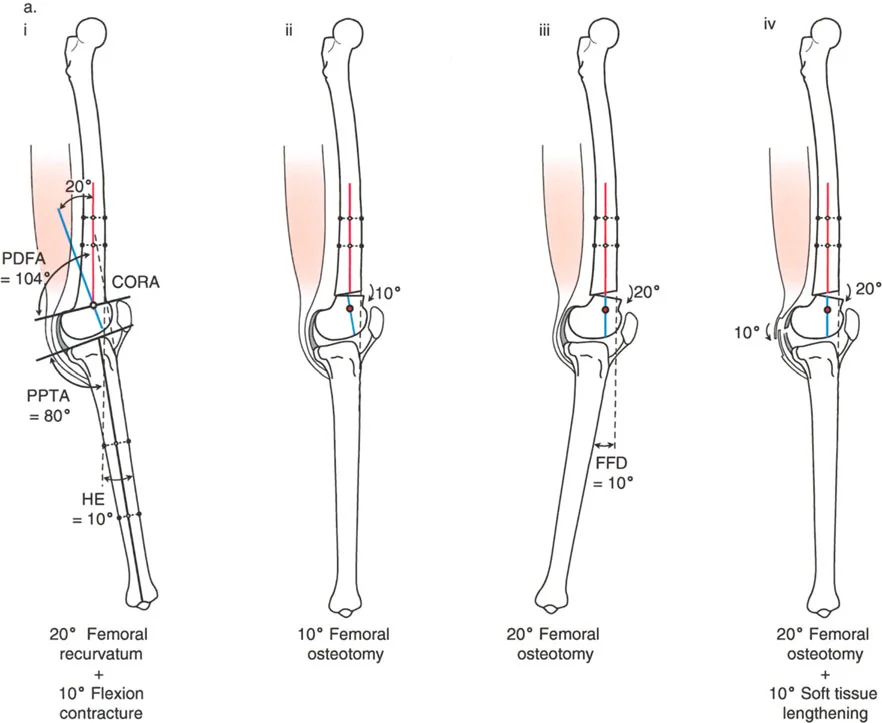
Question 65
A 16-year-old presents with 10° of knee hyperextension (HE). Radiographs show a PDFA of 104° and a PPTA of 80°. What is the magnitude of the associated soft tissue knee flexion contracture?
View Answer & Explanation
Correct Answer: B
Rationale: The total bony deformity is a 21° femoral recurvatum (PDFA 104°). The clinical presentation is only 10° of HE. The relationship is: Clinical HE = Bony Recurvatum - Flexion Contracture. Therefore, 10° = 21° - Flexion Contracture. The flexion contracture must be approximately 11° (closest answer is 10°). This represents a partially compensated deformity.
Question 66
For the 16-year-old patient with 10° of clinical HE, a 20° femoral recurvatum, and a 10° flexion contracture, what is the ideal surgical treatment to achieve a final maximum knee extension of 0° without requiring soft tissue procedures?
View Answer & Explanation
Correct Answer: C
Rationale: The ideal treatment is a compromise that corrects only the amount of the clinical hyperextension. A 10° distal femoral flexion osteotomy will reduce the 20° bony recurvatum to 10°. This remaining 10° of bony recurvatum will be perfectly balanced by the pre-existing 10° soft tissue flexion contracture, resulting in a knee that extends to 0°. This avoids creating a new flexion deformity while eliminating the clinical HE.
Question 67
A patient with a partial growth arrest of the distal femur has 16° of clinical hyperextension. Radiographs show a PDFA of 104° and PPTA of 82°. This indicates a 21° femoral recurvatum and an associated 5° flexion contracture. If the surgeon performs a full 21° distal femoral flexion osteotomy, what will be the resulting knee alignment?
View Answer & Explanation
Correct Answer: C
Rationale: Fully correcting the 21° bony deformity will unmask the underlying 5° soft tissue flexion contracture. The knee's maximum extension will now be limited by this contracture, resulting in a 5° fixed flexion deformity. The ideal compromise would have been a 16° osteotomy to match the clinical HE.
Question 68
A patient with a distal femoral recurvatum deformity has limited knee flexion to 90°. The primary goal of surgery is to improve the flexion range. The patient has 16° of clinical HE and a 24° femoral recurvatum deformity. How can a distal femoral flexion osteotomy increase the total arc of motion?
View Answer & Explanation
Correct Answer: B
Rationale: In recurvatum, the knee starts in a hyperextended position. A flexion osteotomy of the distal femur effectively "pre-flexes" the distal articular segment. If the total articular arc is, for example, 120°, starting from -16° (hyperextension) would limit flexion to 104°. By performing a 16° flexion osteotomy, the starting position becomes 0°, allowing the knee to potentially reach the full 120° of flexion, thereby increasing the functional range of motion.
Question 69
A 25-year-old male presents with 20° of knee hyperextension. A lateral radiograph shows a PDFA of 84° and a PPTA of 100°. Based on the provided diagram, what is the source of his deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The normal PPTA is approximately 80°. A PPTA of 100° indicates a 20° proximal tibial recurvatum deformity (100°-80° = 20°). The PDFA of 84° is within the normal range. Since the clinical HE of 20° matches the bony tibial deformity, the source is isolated proximal tibial recurvatum. Femoral recurvatum would be indicated by an abnormally high PDFA.
Question 70
A 14-year-old who sustained a proximal tibial traction pin injury presents with 24° of knee hyperextension. Radiographs reveal a PPTA of 112° and a PDFA of 86°. What is the most appropriate surgical intervention?
View Answer & Explanation
Correct Answer: B
Rationale: The deformity is located in the proximal tibia, as indicated by the abnormal PPTA of 112° (normal ~80°), representing approximately 32° of recurvatum. The clinical HE is 24°, suggesting a small concomitant flexion contracture. However, the CORA is in the proximal tibia. The fundamental principle is to correct the deformity at its source. Therefore, a proximal tibial flexion osteotomy is the ideal treatment.
Question 71
A patient has a 20° knee hyperextension deformity secondary to proximal tibial recurvatum (PPTA = 100°, PDFA = 84°). If the surgeon incorrectly performs a 20° distal femoral flexion osteotomy, what is the most likely adverse consequence?
View Answer & Explanation
Correct Answer: C
Rationale: Correcting a tibial deformity with a femoral osteotomy creates an abnormal joint orientation. The combination of iatrogenic femoral flexion and native tibial recurvatum results in an altered patellar tracking mechanism and increased contact pressures on the patella. Patients with this combination frequently complain of patellofemoral pain and instability. The knee may also appear subluxed.
Question 72
A patient's lateral knee radiograph shows a PPTA of 100° and a PDFA of 84°. Clinically, the patient's knee extends to exactly 0° and flexes to 110°. What is the underlying pathology?
View Answer & Explanation
Correct Answer: B
Rationale: A PPTA of 100° indicates a 20° proximal tibial recurvatum deformity. The fact that the knee only extends to 0° (and not into hyperextension) means there must be an equal and opposite 20° soft tissue flexion contracture that is masking the bony deformity. This is a fully compensated deformity.
Question 73
A 14-year-old boy with a history of Legg-Calvé-Perthes disease presents with limited hip motion. On examination, his hip has a fixed flexion contracture and limited adduction. The surgeon notes that the limitation in adduction is primarily due to soft tissues surrounding the joint rather than the joint capsule or articular surface itself. Which of the following is the most likely cause of this extra-articular limitation?
View Answer & Explanation
Correct Answer: D
Rationale: The text distinguishes between intra-articular and extra-articular causes of limited range of motion. Muscle contracture and heterotopic ossification are listed as extra-articular causes. Capsular contracture, adhesions, and articular deformity are intra-articular causes.
Question 74
A 12-year-old girl is being evaluated for developmental coxa vara. Preoperative planning for a proximal femoral osteotomy is undertaken. According to the principles of deformity correction, where is the Center of Rotation of Angulation (CORA) for this type of deformity typically located?
View Answer & Explanation
Correct Answer: B
Rationale: As stated in the text and shown in Figure 19-5a, the CORA for a developmental varus deformity of the hip is at the center of the femoral head. The CORA for a valgus deformity is at the base of the greater trochanter.
Question 75
A 15-year-old boy with cerebral palsy has a progressive, painful valgus hip deformity. A varus-producing proximal femoral osteotomy is planned. To correctly restore the mechanical axis, the surgeon must understand the location of the deformity's CORA. Where is the CORA for a developmental valgus deformity of the hip located?
View Answer & Explanation
Correct Answer: D
Rationale: The text and Figure 19-5b indicate that for a developmental valgus deformity, the CORA is located at the lateral end of the physis of the greater trochanter, which corresponds to the base of the greater trochanter. The CORA for a varus deformity is at the center of the femoral head.
Question 76
A 10-year-old child with congenital coxa vara is scheduled for a 40-degree valgus osteotomy of the proximal femur. The parents are concerned about potential limb length discrepancy. What is the expected effect of this procedure on the length of the femur?

View Answer & Explanation
Correct Answer: B
Rationale: As described in the text and illustrated in Figure 19-7, a valgus osteotomy lengthens the femur because it makes the femoral neck more vertical. Conversely, a varus osteotomy shortens the femur by making the neck more horizontal.
Question 77
A 16-year-old with a painful hip due to coxa valga is undergoing a varus osteotomy. During preoperative counseling, the surgeon discusses the expected biomechanical changes. What effect will the varus osteotomy have on the overall length of the femur?
View Answer & Explanation
Correct Answer: A
Rationale: A varus osteotomy shortens the femur because it makes the femoral neck more horizontal, decreasing the overall vertical height of the proximal femur. This is illustrated in Figure 19-7. A valgus osteotomy has the opposite effect, lengthening the femur.
Question 78
A surgeon is performing a valgus osteotomy for a 30-degree varus deformity of the hip. Preoperative examination reveals that maximum hip adduction is limited to 10 degrees due to extra-articular soft tissue tightness. Which muscle group is the primary extra-articular restraint to adduction of the proximal femoral segment?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that for a valgus osteotomy, "The major extra-articular limitations to adduction of the proximal segment of the femur after osteotomy are the tensor fascia lata and the gluteus medius and minimus muscles." The adductors would be relaxed by this maneuver, not tightened.
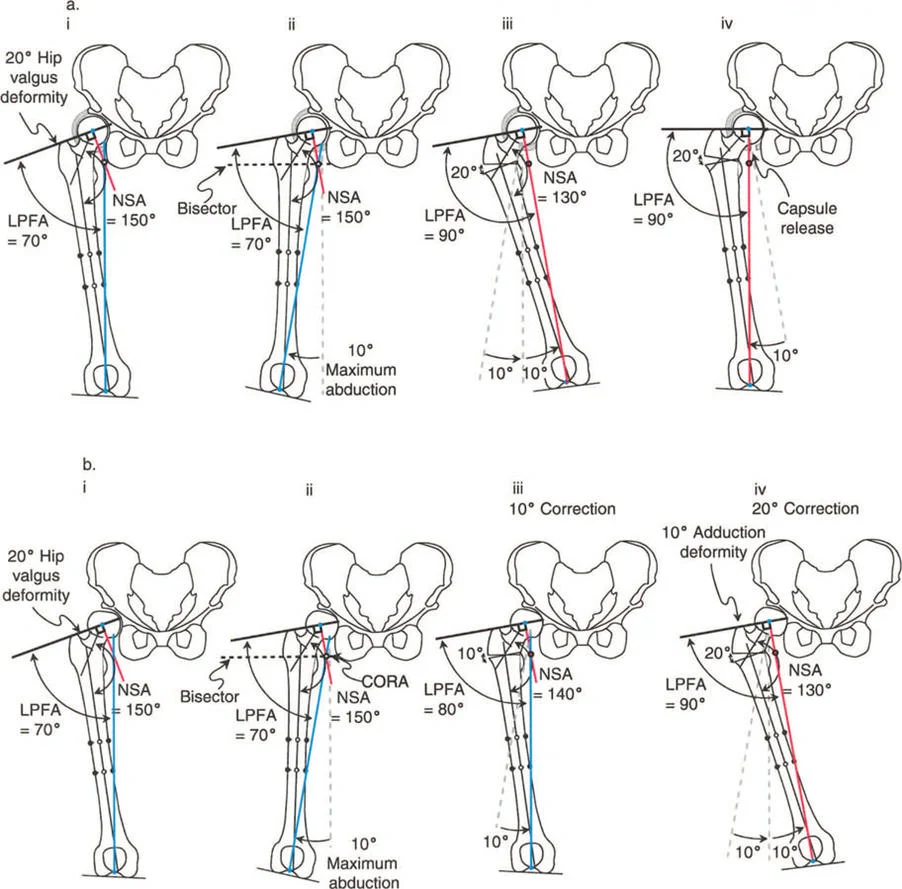
Question 79
A 9-year-old with congenital coxa vara undergoes a 30-degree valgus osteotomy. Preoperatively, the hip had limited adduction due to tight abductors. If this abductor tightness is not addressed intraoperatively, what is the most likely immediate postoperative clinical finding?
View Answer & Explanation
Correct Answer: B
Rationale: As shown in Figure 19-1b, if a valgus osteotomy is performed in the presence of tight abductors that do not allow sufficient adduction of the proximal fragment, the limb will be held in abduction. This results in a fixed abduction contracture immediately after correction.
Question 80
A 13-year-old patient undergoes a valgus osteotomy for coxa vara. After the correction, the surgeon notes that passive hip abduction is significantly limited. The diagram illustrates the biomechanical changes. What is the rationale for performing an adductor tenotomy in this situation?

View Answer & Explanation
Correct Answer: C
Rationale: The text explains that valgus osteotomy has a lengthening effect, which can make the adductor muscles tight. As shown in Figure 19-1a, an adductor tenotomy may be required to improve postoperative hip abduction and relieve pressure on the femoral head caused by this increased tension.
Question 81
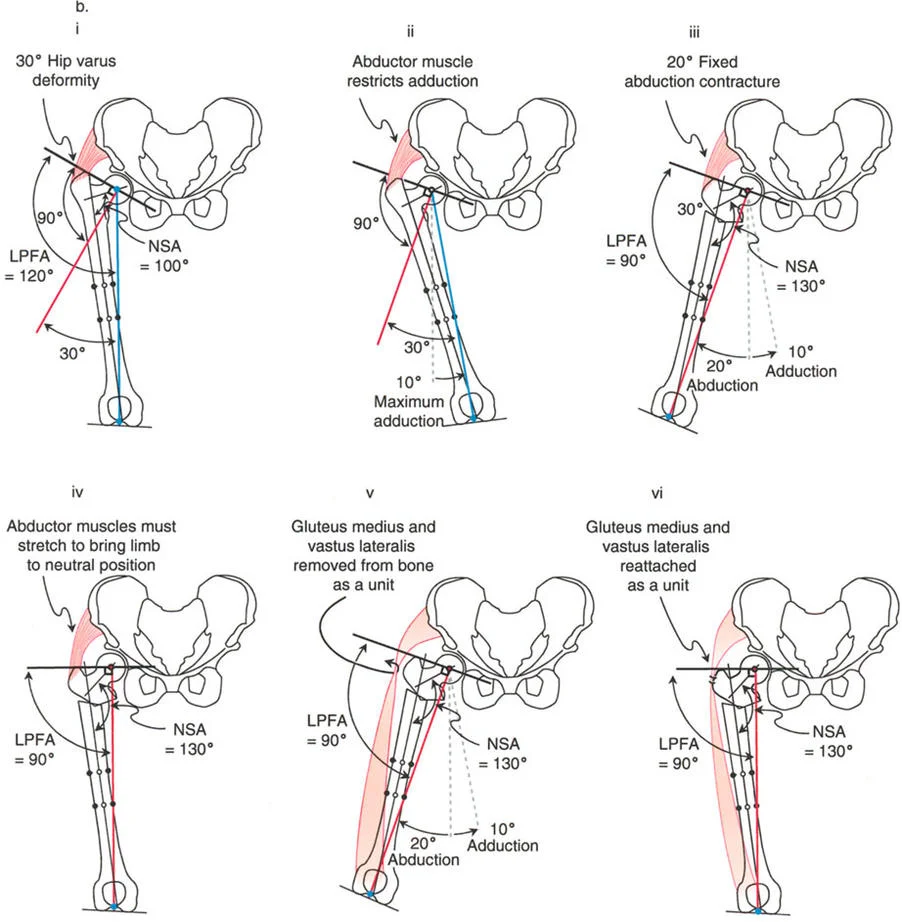
A 7-year-old child with congenital femoral deficiency has severe coxa vara and a significant abduction contracture that prevents adequate adduction for a valgus osteotomy. The surgeon plans a procedure to release the abductor mechanism while preserving its function. Which surgical step is central to this technique?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes a specific procedure for this scenario, based on the Harding approach. It involves "removal of the entire insertion of the gluteus medius and minimus in continuity with the quadriceps (vastus lateralis)." This allows the proximal femur to be adducted without weakening the abductors, which are reattached after the correction.
Question 82
During a valgus-extension osteotomy for congenital coxa vara, a surgeon performs a release of the gluteus medius and minimus in continuity with the vastus lateralis. To achieve full correction, the surgeon notes that release of an additional muscle is necessary to improve internal rotation, extension, and adduction. Which muscle is most likely to require release?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "It is also necessary to release the piriformis muscle, which can restrict internal rotation, extension, and adduction." The piriformis is a primary external rotator and can act as an abductor and extensor, thus its release is crucial in complex corrections.
Question 83
A 15-year-old has a 20-degree varus deformity of the hip with a spherical femoral head. Examination reveals that maximum passive adduction is only 10 degrees due to intra-articular restrictions. A 20-degree valgus osteotomy is performed. What additional procedure is required to achieve a neutral limb alignment without creating a new deformity?
View Answer & Explanation
Correct Answer: C
Rationale: As shown in Figure 19-3a, when a valgus osteotomy is performed for a varus deformity with a round head but intra-articular adduction limitation, full correction will result in a residual valgus deformity. A capsular release is required to allow the proximal fragment to adduct fully, bringing the limb into neutral alignment.
Question 84
A 16-year-old with a history of SCFE has a 20-degree varus deformity and a non-spherical, deformed femoral head. Maximum passive adduction is 10 degrees. If the surgeon performs a 20-degree valgus osteotomy, what is the most likely outcome?
View Answer & Explanation
Correct Answer: B
Rationale: The text and Figure 19-3b explain that if the femoral head is non-spherical and blocks adduction, full angular correction cannot be obtained. Performing a 20-degree valgus osteotomy when only 10 degrees of adduction is available will result in a 10-degree valgus deformity, as the proximal fragment cannot be fully adducted into the corrected position.
Question 85
A 62-year-old male presents with worsening right knee pain and a varus thrust. Weight-bearing radiographs demonstrate significant medial compartment joint space narrowing. An orthopedic resident is asked to define the Joint Line Congruency Angle (JLCA) as part of the deformity analysis. What is the correct definition of the JLCA?
View Answer & Explanation
Correct Answer: C
Rationale: The Joint Line Congruency Angle (JLCA) is the cornerstone of intra-articular deformity analysis. It is defined as the angle between a line drawn across the distal femoral condyles and a line drawn across the tibial plateaus. In a normal knee, these lines are parallel, resulting in a JLCA near 0 degrees.
Question 86
A 25-year-old female presents for a routine physical exam with no knee complaints. Her lower extremity alignment is assessed on a standing AP radiograph. Her knee joint lines appear parallel and the joint space is symmetric. What is the typical measurement for a normal Joint Line Congruency Angle (JLCA)?

View Answer & Explanation
Correct Answer: B
Rationale: In a healthy, congruent knee, the joint lines of the femur and tibia are nearly parallel. This relationship results in a normal JLCA that is typically measured between 0 and 2 degrees. An angle greater than this suggests intra-articular pathology such as cartilage loss or dysplasia.
Question 87
A 58-year-old female with a history of knee pain presents with a weight-bearing radiograph showing an increased Joint Line Congruency Angle (JLCA) and a varus mechanical axis. The surgeon must determine the etiology of the increased JLCA. Which of the following is a primary diagnostic dilemma that must be resolved?
View Answer & Explanation
Correct Answer: C
Rationale: An increased JLCA on a static weight-bearing film can be caused by true physical loss of cartilage and bone on one side, or by the joint "opening up" on the contralateral side due to ligament laxity. These two causes must be strictly distinguished during preoperative planning, as their management is different.
Question 88
A 65-year-old male with a varus knee deformity is being evaluated for a high tibial osteotomy. His standing AP radiograph shows an increased JLCA. To differentiate between medial cartilage loss and lateral collateral ligament (LCL) laxity, what is the gold standard assessment tool?
View Answer & Explanation
Correct Answer: C
Rationale: Standard weight-bearing films are insufficient to differentiate cartilage loss from ligamentous laxity. Varus and valgus stress radiographs, ideally under fluoroscopy, are the gold standard. They allow for measurement of the minimum cartilage space under compression and the maximum opening under tension, which reveals ligamentous competence.
Question 89
A 60-year-old patient with a valgus knee deformity undergoes stress radiography. The surgeon applies a varus stress to the knee. What is the primary purpose of this specific maneuver?
View Answer & Explanation
Correct Answer: B
Rationale: Applying stress to compress the side of the deformity reveals the true remaining cartilage height. In a valgus knee, the deformity is on the lateral side, but the question asks about applying varus stress. Varus stress compresses the medial compartment, allowing measurement of the minimum cartilage space and true cartilage height on the medial side. Valgus stress would be used to assess the lateral compartment.
Question 90
A surgeon is planning a high tibial osteotomy for a 55-year-old with varus malalignment. The preoperative analysis reveals a significant JLCA of 7 degrees due to confirmed medial cartilage loss. If the surgeon performs a standard extra-articular osteotomy to correct the mMPTA to 87 degrees but fails to account for the intra-articular angulation from the JLCA, what is the most likely outcome?
View Answer & Explanation
Correct Answer: C
Rationale: This is a common pitfall. The angulation from the JLCA must be incorporated into the total magnitude of angular correction. Failing to account for this intra-articular "wedge" will result in under-correction of the overall mechanical axis, even if the bone angles (mMPTA) are corrected perfectly.
Question 91
A 45-year-old patient has a severe varus deformity secondary to a depressed medial tibial plateau. The distal femur is anatomically normal. When planning a corrective tibial osteotomy, the deformed tibial articular surface is an unreliable reference. According to Paley's Rule of Joint Line Substitution, what should be used as the surrogate "knee joint line" for planning?
View Answer & Explanation
Correct Answer: B
Rationale: Paley's Rule of Joint Line Substitution states that if one side of the joint is deformed but the other is normal, the normal side can be used as the reference for planning. In this case, with a deformed tibia and a normal femur, the distal femoral joint line serves as the reliable horizontal reference for planning the tibial correction.
Question 92
A 16-year-old presents with a valgus knee. Radiographs show a hypoplastic lateral femoral condyle from a prior infection, but the proximal tibia is normal. The surgeon is planning a distal femoral osteotomy. To ensure an accurate correction, which reference line should be used to represent the knee joint for calculating the desired mLDFA?
View Answer & Explanation
Correct Answer: A
Rationale: This is the corollary to Paley's Rule of Joint Line Substitution. When there is an isolated femoral deformity with joint surface involvement and a normal tibia, the proximal tibial joint line should be used as the reference horizontal for planning the femoral correction. This prevents over- or under-correction.
Question 93
A surgeon is planning a correction for a patient with a depressed lateral tibial plateau. The surgeon decides to perform an extra-articular proximal tibial osteotomy and will not surgically alter the joint surface itself. In this scenario, what is the most appropriate method for representing the proximal tibial joint line during templating?
View Answer & Explanation
Correct Answer: B
Rationale: The knee joint line should be treated as a single "best fit" line *only* if there is no intention to surgically alter the shape of the joint line itself (i.e., an extra-articular correction is planned). In this case, the preferred single best-fit line is often to adopt the normal femoral condylar line (Paley's Rule of Substitution).
Question 94
A 14-year-old with severe adolescent Blount's disease presents with a varus deformity and clinical instability. The surgeon plans to directly elevate the depressed medial tibial plateau to restore joint congruity. What is the correct approach for characterizing the tibial joint surface during preoperative planning for this intra-articular procedure?
View Answer & Explanation
Correct Answer: C
Rationale: If an intra-articular correction (like a plateau elevation) is planned, the articular surface must be characterized by two separate lines—one for the medial plateau and one for the lateral. This is the only way to accurately calculate the required millimeters of elevation and degrees of angular tilt for the depressed segment.
Question 95
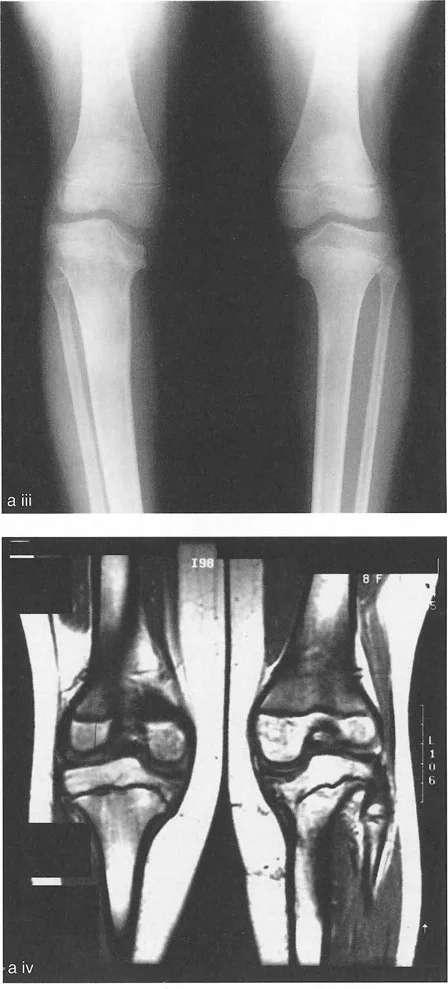
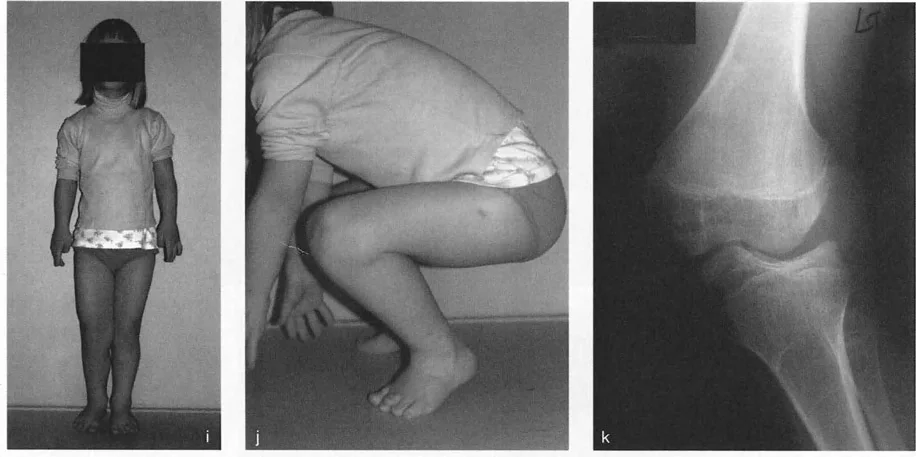
A 15-year-old patient with adolescent Blount's disease is shown in the provided image. Based on the typical pathophysiology of this condition, what is the characteristic deformity of the proximal tibial joint line?
View Answer & Explanation
Correct Answer: C
Rationale: Blount's disease (tibia vara) is characterized by pathology of the posteromedial proximal tibial physis, leading to a severe depression and medial (varus) sloping of the medial tibial plateau. This creates an acute angle between the medial and lateral plateau joint lines.
Question 96
A 9-year-old patient with Ellis-van Creveld syndrome presents with a severe valgus knee deformity. The radiograph is shown. What is the pathognomonic feature of the proximal tibial joint line in this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Ellis-van Creveld syndrome (chondroectodermal dysplasia) leads to a distinct "step" depression in the lateral tibial plateau. A key feature is that the medial and lateral plateau lines often remain parallel to each other, but they are at different horizontal levels, creating a large step-off and severe valgus.
Question 97
A 17-year-old patient has a valgus deformity due to a hypoplastic lateral femoral condyle. Despite the malalignment, he has a smooth range of motion and no clinical instability. What is the primary biomechanical reason that femoral condyle malorientation is often better tolerated than a tibial plateau step-off?
View Answer & Explanation
Correct Answer: C
Rationale: The fundamental geometric difference is key. The tibial plateaus are relatively flat, so a step-off creates immediate incongruity and point-loading. Conversely, the femoral condyles are round. A round surface can still roll and glide effectively on the flat tibia even if its height or orientation is altered, making the joint more "forgiving" of this type of deformity.
Question 98
A 14-year-old is evaluated for a knee deformity. The AP radiograph reveals that both distal femoral condyles are maloriented and incline toward the intercondylar notch, creating the appearance shown in the image. What is the name of this deformity and its typical cause?
View Answer & Explanation
Correct Answer: B
Rationale: The classic "fishtail" appearance on an AP radiograph is caused by a growth arrest in the exact center of the distal femoral physis. This tethers the central portion while the medial and lateral peripheries continue to grow, causing both condyles to malorient and incline toward the middle.
Question 99
A 16-year-old patient has a significant valgus mechanical axis deviation due to a post-traumatic malunion of a distal femoral fracture that resulted in a maloriented lateral condyle. The joint itself is stable and has good motion. What is the most appropriate surgical strategy to realign the limb?

View Answer & Explanation
Correct Answer: C
Rationale: Because of the geometric tolerance of the round femoral condyles, malalignment due to femoral unicondylar displacement or malorientation can frequently be realigned using an extra-articular distal femoral supracondylar osteotomy. A high-risk intra-articular procedure is often unnecessary if the joint is stable and functional.
Question 100
A 40-year-old patient has a varus deformity and significant clinical instability due to a 1 cm step-off of the medial tibial plateau from a chronic, non-united fracture. What is the most appropriate surgical approach to address both the malalignment and the instability?
View Answer & Explanation
Correct Answer: C
Rationale: In stark contrast to femoral deformities, the severe instability and incongruity caused by a tibial plateau step-off almost always mandates a true intra-articular osteotomy (plateau elevation). An extra-articular correction would not address the instability and would lead to rapid joint destruction.
