ABOS Part I & OITE Orthopedic Board Review: Deformity Correction, Paley's Principles, MCQs | Part 22017
Key Takeaway
Orthopedic deformity correction involves meticulous surgical planning using principles like Paley's rules to address malalignment, angulation, and translation. It utilizes tools such as the Center of Rotation of Angulation (CORA) and external fixators to restore the mechanical axis and achieve collinearity, crucial for preventing osteoarthritis and ensuring optimal limb function. Advanced radiographic assessment is mandatory for precise correction.
ABOS Part I & OITE Orthopedic Board Review: Deformity Correction, Paley's Principles, MCQs | Part 22017
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old male presents with chronic knee pain and progressive varus deformity following a distal femoral fracture treated non-operatively 5 years prior. A full-length weight-bearing radiograph reveals a mechanical axis deviation (MAD) of 25mm medial to the center of the knee joint. Further analysis shows a mechanical Lateral Distal Femoral Angle (mLDFA) of 80° and a Medial Proximal Tibial Angle (MPTA) of 87°. Based on Paley's principles, which of the following statements best describes the primary source of the patient's malalignment?
Explanation
Correct Answer: C
The patient presents with a medial MAD, which indicates a varus deformity of the limb. The normal range for the mechanical Lateral Distal Femoral Angle (mLDFA) is 85° to 90°, with an average of 88°. The patient's mLDFA of 80° is significantly less than the normal range, indicating a varus deformity originating in the distal femur. Conversely, the Medial Proximal Tibial Angle (MPTA) is 87°, which falls within the normal range of 85° to 90° (average 87°), thus excluding the proximal tibia as the primary source of the angular deformity. Therefore, the primary deformity is located in the femur, causing a varus malalignment.
Option A is incorrect because while the limb has a varus malalignment, the MPTA is normal, indicating the tibia is not the primary source of the angular deformity. Option B is incorrect because the mLDFA of 80° indicates a varus, not valgus, deformity of the femur. Option D is incorrect because the limb has a varus, not valgus, malalignment, and the tibia is not the primary source. Option E is incorrect as the analysis of joint orientation angles clearly points to the femur as the primary source, not an equal distribution.
Question 2
A 45-year-old male presents with a chronic tibial malunion following a high-energy trauma. Clinical examination reveals a significant valgus deformity of the lower limb. A full-length weight-bearing radiograph is obtained for preoperative planning. The image below illustrates the initial step in identifying the geometric center of the angular deformity. Based on Paley's principles, what does the black circle in the provided image represent?

Explanation
Correct Answer: C
The image provided (Panel c from the teaching case) explicitly illustrates the process of identifying the Center of Rotation of Angulation (CORA). The red line represents the proximal anatomical axis, and the blue line represents the distal anatomical axis. The black circle highlights the intersection point of these two lines. According to Paley's principles, the CORA is the geometric pivot point of the deformity, located at the intersection of the proximal and distal anatomical axes. This point is crucial for planning corrective osteotomies.
Option A is incorrect; MAD is a linear distance from the knee center to the mechanical axis, not a point identified by intersecting anatomical axes. Option B is incorrect; the red line represents the proximal anatomical axis, but the black circle is the intersection of both axes. Option D is incorrect; while the osteotomy is often planned near the CORA, the black circle specifically denotes the CORA itself, not necessarily the osteotomy site, especially in cases with translation. Option E is incorrect; the CORA is a point of angulation, and while translation may be present, the black circle does not represent the point of maximal translation.
Question 3
A 58-year-old patient presents with a tibial malunion characterized by a varus angulation and a significant medial translation at the fracture site. Preoperative planning identifies the CORA to be located 3 cm distal to the actual fracture site. The surgeon plans to correct this deformity using an external fixator. According to Paley's principles, which of the following surgical strategies will result in a perfect correction of both angulation and translation without creating a new deformity?
Explanation
Correct Answer: C
This scenario describes a combined angulation and translation deformity, where the CORA is displaced from the fracture site. According to Paley's Rule 2: 'If the hinge is placed at the CORA but the osteotomy is performed at a different level (e.g., at the physical apex of the deformity or fracture site), then angulation is corrected AND a translation is created at the osteotomy site.' In this case, the pre-existing medial translation has displaced the CORA distally. By placing the mechanical hinge of the frame at the true CORA (3 cm distal to the fracture site) and performing the osteotomy at the original fracture site, the corrective rotation around the hinge will simultaneously correct the angulation and induce a translation that is exactly equal and opposite to the original medial translation, resulting in a perfectly collinear bone axis.
Option A describes a scenario that would correct angulation but leave a residual translation (Rule 3 if the fracture site is not the CORA). Option B describes Paley's Rule 1, which is for pure angulation deformities where the CORA is at the osteotomy site, not applicable here due to translation. Options D and E involve arbitrary osteotomy or hinge placements that would likely lead to new, iatrogenic deformities (Rule 3).
Question 4
A 28-year-old patient presents with a pure angular valgus deformity of the proximal tibia, with the CORA precisely located at the metaphyseal apex of the deformity. The surgeon plans a corrective osteotomy and fixation with a circular external fixator. According to Paley's principles, which of the following approaches will achieve a perfect correction without creating any secondary translation?
Explanation
Correct Answer: C
This scenario describes a pure angular deformity where the CORA is located at the apex of the deformity. According to Paley's Rule 1: 'If the osteotomy is performed at the CORA and the hinge is placed at the CORA, then angulation is perfectly corrected without creating any secondary translation.' This is the ideal, straightforward scenario for simple angular deformities, where the bone segments pivot around their natural geometric center, resulting in perfectly collinear proximal and distal anatomical axes.
Options A, B, and D describe situations where either the osteotomy or the hinge (or both) are not at the CORA, which, according to Paley's Rule 3, would result in the creation of a new, secondary translation deformity (a 'residual bump'). Option E is incorrect because applying a translational force would be unnecessary and potentially detrimental in a pure angular deformity corrected according to Rule 1.
Question 5
A 62-year-old patient undergoes a corrective osteotomy for a tibial malunion. During the procedure, the surgeon performs the osteotomy at the original fracture site, which is 4 cm distal to the calculated CORA. The external fixator hinge is also inadvertently placed at the fracture site, rather than at the true CORA. Postoperatively, the limb's mechanical axis is straightened, but the patient develops a prominent bony prominence on the medial aspect of the tibia. Which of Paley's Osteotomy Rules best explains this outcome?
Explanation
Correct Answer: C
This clinical scenario perfectly illustrates Paley's Rule 3: 'If both the osteotomy and the hinge are placed at a location that is NOT the CORA, then angulation is corrected, but a new, secondary translation deformity is created.' In this case, both the osteotomy and the hinge were placed at the fracture site, which was 4 cm distal to the true CORA. While the overall angulation was corrected (straightening the mechanical axis), the misalignment of the hinge and osteotomy relative to the CORA resulted in a new translational deformity, clinically manifesting as a prominent bony prominence or 'residual bump' (a bayonet or offset position).
Option A (Rule 1) describes the ideal correction for pure angulation without translation. Option B (Rule 2) describes the method for correcting combined angulation and translation by placing the hinge at the CORA and the osteotomy elsewhere. Option D (The Rule of Halves) is a planning principle for drawing anatomical axes, not an osteotomy rule. Option E (distraction osteogenesis) is a biological process, not one of Paley's geometric osteotomy rules.
Question 6
A 35-year-old male presents with a complex tibial malunion involving angulation, translation, and significant internal rotational deformity. The surgeon is planning a multiplanar correction using a circular external fixator. Regarding the rotational component, which of the following statements is true based on the provided case material?
Explanation
Correct Answer: D
The case states: 'Rotational osteotomy correction around the mechanical axis of the femur does not produce MAD. However, performing a proximal femoral osteotomy around the mechanical axis produces significant displacement (translation) of the diaphysis of the femur, making it biologically and technically impractical.' This directly supports option D.
Option A is incorrect. The case states: 'Rotational osteotomy correction around the anatomic axis of the femur produces MAD.' Option B is incorrect. The case states: 'Rotational osteotomies around the anatomic or mechanical axis of the tibia do not produce any MAD in the frontal plane.' Option C is incorrect. The case states: 'Clinical assessment has been shown to be essentially equivalent in accuracy to complex radiographic methods for rotational deformities.' Option E is incorrect. The case states: 'The direction of a rotation deformity is described by convention as the distal joint relative to the proximal joint.'
Question 7
A 50-year-old patient presents with a severe, multiplanar tibial malunion, as depicted in the clinical image below. The deformity includes significant angulation, translation, and a rotational component. The surgeon is preparing for a complex deformity correction. According to the teaching case, what is the absolute minimum requirement for initial radiographic assessment in this scenario?

Explanation
Correct Answer: C
The teaching case explicitly states under 'Preoperative Planning Masterclass: A Step-by-Step Guide': 'High-quality, standing, weight-bearing, full-length anteroposterior (AP) and lateral radiographs of the entire lower extremity are the absolute minimum requirement. These images must be well-calibrated (usually with a 50mm scaling ball) and show the hip, knee, and ankle on a single continuous film to prevent parallax error.'
Options A and B (CT/MRI) are advanced imaging modalities that may be used for further detail but are not the 'absolute minimum requirement' for initial geometric planning. Option D (stress radiographs) assesses stability, not the primary deformity geometry. Option E (bilateral radiographs) is often helpful for comparison but the case specifies the 'absolute minimum requirement' for the affected limb's assessment.
Question 8
A 40-year-old patient presents with a complex tibial malunion, exhibiting both valgus angulation and anterior translation in the sagittal plane. The surgeon has meticulously identified the AP CORA and the LAT CORA. What is the next critical step in preoperative planning to ensure a single corrective motion simultaneously fixes both the valgus and the recurvatum without inducing unwanted rotation?
Explanation
Correct Answer: B
The teaching case emphasizes the importance of addressing oblique plane deformities: 'Deformities rarely exist purely in the cardinal coronal or sagittal planes. A malunion with valgus (AP plane) and recurvatum (LAT plane) is, in reality, a single deformity existing in an oblique plane. The true magnitude and orientation of this oblique deformity must be calculated using trigonometric principles or specialized software. The axis of the corrective hinge must be placed perfectly perpendicular to this calculated oblique plane. This ensures that a single corrective motion simultaneously fixes both the valgus and the recurvatum without inducing any unwanted rotation or creating a new deformity.'
Option A is incorrect as it suggests multiple osteotomies, which is less ideal than a single oblique correction. Option C is incorrect because placing the hinge only at the AP CORA would not account for the sagittal plane deformity and would likely induce new deformities. Option D is too vague and does not follow the systematic planning approach. Option E is a redundant step at this stage, as MAD would have been quantified earlier.
Question 9
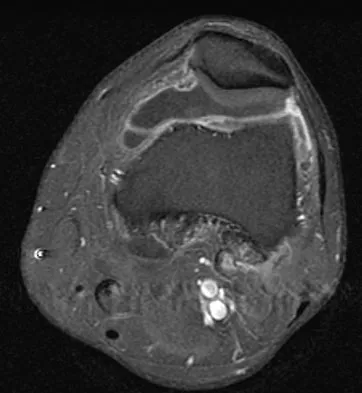
A 25-year-old patient presents with a tibial shaft malunion, as seen in the clinical image below, resulting in a significant foot progression angle during gait. The orthopedic surgeon is assessing the rotational component of the deformity. According to the teaching case, what is the most practical and accurate clinical method for assessing tibial torsion?

Explanation
Correct Answer: C
The teaching case states: 'Tibial torsion is more accurately assessed by observing the orientation of the long axis of the sole of the foot relative to the knee forward position. This can best be achieved using the thigh-foot axis with the patient prone and the knees flexed to 90 degrees.' It also cautions that 'the foot progression angle may appear normal, even in the presence of a severe torsional deformity, because of compensatory mechanisms at the hip or knee.'
Option A is incorrect because, as stated in the case, the foot progression angle can be misleading due to compensatory mechanisms. Option B is a general assessment but less specific and accurate for tibial torsion than the thigh-foot axis. Option D (CT scan) is a radiographic method, and while accurate, the question asks for the 'most practical and accurate clinical method.' Option E assesses hip rotation, not specifically tibial torsion.
Question 10
A 48-year-old patient with a history of open tibial fracture and subsequent malunion, complicated by poor soft tissue coverage and a history of infection, requires a complex multiplanar deformity correction. Given these specific patient factors, which surgical method is highlighted in the teaching case as the 'undisputed gold standard' for such complex deformities?
Explanation
Correct Answer: C
The teaching case explicitly states: 'For these multiplanar, complex deformities, especially those with compromised soft tissues, poor bone biology, or active infection, circular external fixation based on the Ilizarov method remains the undisputed gold standard.' This directly addresses the patient's specific factors (complex deformity, compromised soft tissues, history of infection).
Options A, B, D, and E all represent forms of internal fixation or simpler external fixation, which are generally contraindicated or less ideal in the presence of compromised soft tissues, poor bone biology, or active infection due to increased risk of infection, nonunion, or hardware failure. The Ilizarov method, with its external nature and ability for gradual correction and distraction osteogenesis, is uniquely suited for such challenging cases.
Question 11
A 32-year-old male presents with a malunited tibial shaft fracture following a high-energy motor vehicle accident. Radiographs reveal both angular deformity and a significant parallel shift of the distal segment relative to the proximal segment. He complains of increasing knee pain and difficulty with ambulation. Which of the following best describes the primary biomechanical consequence of this combined deformity on his lower extremity?
Explanation
Correct Answer: C
The case describes an angulation-translation deformity. The text explicitly states, 'When an angulation-translation deformity is present, the MAD is invariably altered. This shift concentrates immense mechanical forces onto one compartment of the knee, hip, or ankle. Over time, this abnormal load distribution leads to rapid cartilage wear, capsular stretching, joint instability, and the predictable, early onset of severe osteoarthritis.' Therefore, an altered Mechanical Axis Deviation (MAD) leading to abnormal load distribution is the primary biomechanical consequence.
Option A is incorrect because the deformity is described as both angular and translational, not purely angular. While joint line obliquity can occur, the overarching issue is the MAD.
Option B is incorrect because a pure translational shift without angulation is rare in malunions and would not typically lead to significant knee pain and difficulty ambulation due to altered joint loading in the same way an angulation-translation deformity does. The text defines pure translation as a parallel displacement without angular deviation, which is not the full picture here.
Option D is incorrect because while rotational deformities can coexist, the description focuses on angulation and translation. The text notes that plain films cannot accurately quantify torsion, and rotational deformities must be assessed clinically or via CT, making it less likely to be the 'primary biomechanical consequence' described by the given radiographic findings.
Option E is incorrect as abnormal loading typically leads to cartilage wear and osteoarthritis, not increased bone density at the fracture site, which would be a secondary effect of healing rather than the primary biomechanical consequence of the malalignment.
Question 12
A 55-year-old patient presents with a malunited distal femoral fracture. Preoperative planning involves assessing the coronal alignment of the distal femur. Which of the following joint orientation angles is most critical for evaluating this specific aspect of the deformity and planning a distal femoral osteotomy (DFO)?
Explanation
Correct Answer: D
The text explicitly states: 'Mechanical Lateral Distal Femoral Angle (mLDFA) ... Defines the coronal alignment of the distal femur. An abnormal value indicates a femoral deformity. Crucial for planning distal femoral osteotomies (DFO).' This directly addresses the question's focus on distal femoral coronal alignment and DFO planning.
Option A (MPTA) is incorrect because it defines the coronal alignment of the proximal tibia, not the distal femur, and is essential for high tibial osteotomies (HTO).
Option B (LDTA) is incorrect because it defines the coronal alignment of the ankle mortise relative to the tibial axis, relevant for ankle deformities.
Option C (PPTA) is incorrect because it defines the sagittal alignment (posterior slope) of the proximal tibia, critical for knee sagittal stability.
Option E (JLCA) is incorrect because it measures the angle between femoral condyles and tibial plateau, suggesting intra-articular deformity or cartilage loss, rather than the primary coronal alignment of the distal femur itself.
Question 13
A 40-year-old patient presents with a complex tibial malunion exhibiting both angulation and translation. The surgeon is meticulously planning the correction using Paley's principles. The CORA for this angulation-translation deformity is identified. Which statement accurately describes the location of the angulation-translation CORA compared to a pure angular deformity?
Explanation
Correct Answer: C
The text states: 'In a simple, pure angular deformity, the CORA lies directly within the bone itself, exactly at the apex of the bend. However, the introduction of translation changes the geometry entirely. In an angulation-translation deformity, the translational shift causes the intersection of the proximal and distal axes to occur at a new, displaced point, which we call the angulation-translation CORA. Because of the parallel shift of the bone segments, this point may lie far outside the physical confines of the bone itself.'
Option A is incorrect because this describes the CORA for a pure angular deformity, not an angulation-translation deformity.
Option B is incorrect as the CORA's location is determined by the intersection of axes, which can be anywhere, not necessarily in the joint space.
Option D is incorrect because the text emphasizes that 'Understanding the location of the angulation-translation CORA is the single most critical step in preoperative planning. Its location dictates exactly where the osteotomy must be placed...'
Option E is incorrect because the CORA is the intersection of proximal and distal mechanical axes of the deformed bone, while MAD is the perpendicular distance from the center of the knee joint to the overall mechanical axis line of the limb. They are distinct concepts.
Question 14
A 28-year-old patient has a malunited femoral shaft fracture with angulation and translation in an oblique plane. Preoperative radiographs show an AP angulation of 26° and a lateral angulation of 14°, along with AP translation of 8 mm and lateral translation of 16 mm. The surgeon uses the graphical method to determine the true oblique plane deformity. Based on the principles described in the case and the provided image, what would be the approximate true oblique plane angulation and translation?

Explanation
Correct Answer: C
The question provides the same values as the example in the text and the image: 'an AP angulation of 26° and a lateral angulation of 14° are drawn as two lines at a 90° angle originating from a zero point. The resultant vector (the hypotenuse of the right triangle formed) represents the true magnitude of the oblique plane angulation.' The image's bottom right panel clearly shows aAP = 26°, aLAT = 14°, resulting in aOBL = 30°. Similarly, for translation, tAP = 8 mm and tLAT = 16 mm, resulting in tOBL = 18 mm. The text explicitly states: 'By identifying this true plane, a surgeon can perfectly orient the hinges of a circular external fixator (like a Taylor Spatial Frame) or the cut of an osteotomy to correct both AP and lateral deformities simultaneously in one smooth motion.'
Options A, B, D, and E are incorrect as they do not match the calculated true oblique angulation and translation derived from the graphical method illustrated and described in the text.
Question 15
A 60-year-old patient requires correction of a pure angular deformity in the tibia. The surgeon plans an osteotomy and places the Angulation Correction Axis (hinge) precisely at the CORA. According to Paley's Osteotomy Rules, what is the expected outcome of this surgical approach?
Explanation
Correct Answer: C
This scenario perfectly describes Paley Osteotomy Rule One: 'The Pure Angular Correction'. The text states: 'Condition: The osteotomy is performed exactly AT the CORA, and the Angulation Correction Axis (hinge) is placed exactly AT the CORA. Result: Pure angular correction. The proximal and distal anatomical axes become perfectly collinear with no induced translation. Clinical Application: This is the ideal scenario for a pure angular deformity. By cutting at the apex and hinging at the apex, the bone straightens perfectly.'
Option A is incorrect as this describes the outcome of Paley's Rule Three, where both the osteotomy and hinge are away from the CORA.
Option B is incorrect as this describes the outcome of Paley's Rule Two, where the osteotomy is away from the CORA but the hinge is at the CORA.
Option D is incorrect as the 'two-bump' problem is associated with strategies that correct angulation and then translate the bone at the osteotomy site, often when the osteotomy is not at the CORA or when dealing with angulation-translation deformities.
Option E is incorrect as this rule describes a successful correction strategy for pure angular deformities.
Question 16
A surgeon is planning to correct a complex angulation-translation deformity of the femur. The CORA is located in an area of poor soft tissue, making an osteotomy at that exact point undesirable. The surgeon decides to perform the osteotomy at a different level, away from the CORA, but still places the Angulation Correction Axis (hinge) precisely at the CORA. Which of Paley's Osteotomy Rules is being applied, and what is the expected outcome?
Explanation
Correct Answer: B
This scenario describes Paley Osteotomy Rule Two: 'The Strategic Correction'. The text states: 'Condition: The Angulation Correction Axis (hinge) is placed AT the CORA, but the osteotomy is performed at a DIFFERENT LEVEL (either proximal or distal to the CORA). Result: The proximal and distal axes still become perfectly collinear. However, at the osteotomy site itself, both angulation and translation will occur. Clinical Application: This is the most powerful rule for treating angulation-translation deformities. By intentionally placing the osteotomy away from the angulation-translation CORA, the induced translation from Rule Two can be used to perfectly cancel out the pre-existing translation of the deformity.'
Option A is incorrect as Rule One applies when both the osteotomy and hinge are at the CORA, resulting in pure angular correction without induced translation.
Option C is incorrect as Rule Three applies when both the osteotomy and hinge are away from the CORA, resulting in iatrogenic translation.
Option D is incorrect as the 'two-bump' problem is a consequence of certain strategies, not a direct result of Rule One, which aims for perfect collinearity.
Option E is incorrect as Rule Three results in iatrogenic translation, not necessarily overcorrection or recurvatum.
Question 17
A 70-year-old patient presents with a complex tibial malunion, as depicted in panel (c) of the image below, showing both angular and translational deviations. The surgeon attempts to correct the deformity by performing an osteotomy and placing the Angulation Correction Axis (hinge) at a location that is neither at the CORA nor at the osteotomy site. What is the most likely outcome of this approach, according to Paley's principles?

Explanation
Correct Answer: C
This scenario describes Paley Osteotomy Rule Three: 'The Common Pitfall'. The text states: 'Condition: Both the osteotomy and the Angulation Correction Axis (hinge) are located AWAY from the CORA. Result: The angulation is corrected, but the proximal and distal axes DO NOT become collinear. A new, iatrogenic translation deformity is created. Clinical Application: This is generally an undesirable outcome and represents a failure of preoperative planning. The bone ends up looking like a bayonet.'
Option A is incorrect as this is the outcome of Rule One.
Option B is incorrect as this is the outcome of Rule Two.
Option D is incorrect as the angulation is corrected, but with an undesirable translational consequence.
Option E is incorrect as Rule Three typically leads to an undesirable 'bayonet' deformity, which is neither cosmetically superior nor avoids translational issues.
Question 18
A 48-year-old patient has a malunited distal tibia fracture with significant angulation and translation in both the coronal and sagittal planes. The surgeon opts to perform an opening wedge osteotomy at the angulation-translation CORA identified strictly on the AP radiograph. What is a common consequence of this specific surgical strategy, as described in the case?
Explanation
Correct Answer: C
The text describes 'Strategy 1: Opening or Closing Wedge at the AP CORA'. It states: 'Technique: An opening or closing wedge osteotomy is performed at this level. This maneuver precisely corrects the coronal plane angulation. The Consequence: Because the correction was based solely on the AP-derived CORA, this action often leaves a residual translation in the sagittal plane (visible on the lateral view). The 'Two-Bump' Problem: To restore the overall mechanical axis, this residual sagittal translation must be corrected by physically shifting the bone at the osteotomy site. This is biomechanically sound but creates an anatomical trade-off: it leaves two distinct bony prominences.'
Option A is incorrect because this strategy focuses on one plane (AP) and typically leaves residual deformity in the other (sagittal).
Option B is incorrect because it's an angulation-translation deformity, and correcting only angulation in one plane will not eliminate all translation, especially in the oblique plane.
Option D is incorrect as the strategy does correct the coronal angulation.
Option E is incorrect as the text explicitly states that residual sagittal translation often requires further shifting at the osteotomy site, leading to the 'two-bump' problem.
Question 19
A 35-year-old patient presents with a complex post-traumatic malunion of the tibia, exhibiting angulation and translation in oblique planes. The surgeon aims for the most anatomic and cosmetically superior result, minimizing bony prominences. Based on the provided teaching case, which surgical strategy is considered the 'Ultimate Solution' for such a deformity?
Explanation
Correct Answer: C
The text describes 'Strategy 4: The Ultimate Solution (Correction Through the Malunion Site)'. It states: 'While the single-plane CORA-based osteotomies are powerful, correcting the deformity directly through the original malunion or nonunion site is often the superior strategy for post-traumatic angulation-translation deformities... When angulation and translation are both present in oblique planes (often approximately 90° apart), performing the correction through the original fracture site yields the most anatomic result. In this advanced series of maneuvers, the angulation is corrected precisely in its oblique plane, and the translation is subsequently corrected in its oblique plane. This strategic approach entirely eliminates the iatrogenic 'bump.''
Options A and B are incorrect as they describe strategies that often lead to the 'two-bump' problem due to residual translation in the unaddressed plane.
Option D is incorrect as while Rule Three can be used for intentional offset, it's generally an undesirable outcome for correcting a malunion and is not the 'ultimate solution' for an anatomic correction.
Option E is incorrect as ignoring the CORA and precise planning would likely lead to suboptimal correction and iatrogenic deformities, contrary to the principles of this masterclass.
Question 20
Preoperative assessment for a complex lower extremity deformity requires standardized, high-quality radiographs. Which of the following is a mandatory characteristic of these radiographs for accurate planning, as emphasized in the case?
Explanation
Correct Answer: D
The text explicitly lists the 'Non-Negotiables: Clinical and Radiographic Assessment': 'Standardized, high-quality, orthogonal AP and lateral radiographs are mandatory. They must be: Full-length: To visualize the entire mechanical axis from the center of the hip to the center of the ankle. Weight-bearing: To assess the limb's alignment under physiological load, which unmasks ligamentous laxity (JLCA alterations). Rotationally controlled: With the patella facing strictly forward (AP view) to eliminate rotational artifact, which can falsely project as coronal or sagittal angulation.'
Option A is incorrect as weight-bearing views are crucial to assess alignment under physiological load.
Option B is incorrect as full-length views are necessary to visualize the entire mechanical axis.
Option C is incorrect as rotationally controlled views are essential to eliminate rotational artifact.
Option E is incorrect as both AP and lateral orthogonal views are mandatory for assessing 3D deformities.
Question 21
A 28-year-old male presents with a mid-diaphyseal tibial malunion characterized by a 20° varus angulation. Preoperative planning identifies the Center of Rotation of Angulation (CORA) at the apex of the deformity. According to Paley's Rule 1 of osteotomy, if the osteotomy and the mechanical hinge are both placed exactly at the CORA, what will be the resulting geometric correction?
Explanation
Question 22
A 35-year-old female requires correction of a distal femoral deformity. The CORA is identified near the articular surface, making an osteotomy at the CORA structurally unfavorable. The surgeon decides to place the hinge at the CORA but performs the osteotomy 4 cm proximal to it. According to Paley's Rule 2, what is the expected outcome?
Explanation
Question 23
During the planning of a deformity correction using an external fixator, a resident incorrectly places both the osteotomy and the hinge at a level 5 cm away from the calculated CORA. Based on Paley's Rule 3, what is the geometric consequence of this technical error?
Explanation
Question 24
A 40-year-old male presents with a valgus knee deformity. Radiographs reveal a mechanical Lateral Distal Femoral Angle (mLDFA) of 81° and a Medial Proximal Tibial Angle (MPTA) of 87°. The Joint Line Convergence Angle (JLCA) is 1°. Where is the primary source of the patient's deformity?
Explanation
Question 25
A patient presents with a severe post-traumatic diaphyseal tibial deformity. A pure translational deformity is noted on the orthogonal radiographs without any angular deviation. When planning the correction, where is the CORA located in a pure translational deformity?
Explanation
Question 26
When evaluating a standing long-leg radiograph of a 55-year-old female with osteoarthritis and a varus knee, the Joint Line Convergence Angle (JLCA) is measured at 6° (opening laterally). What does an abnormal JLCA primarily indicate in the context of deformity planning?
Explanation
Question 27
A 22-year-old patient undergoes an opening wedge high tibial osteotomy (HTO) for a varus deformity. The surgeon makes a geometrically parallel opening wedge gap. What unintended consequence is most likely to occur in the sagittal plane?
Explanation
Question 28
A 45-year-old man requires bone transport for a 6 cm tibial defect using distraction osteogenesis (Ilizarov method). The surgeon performs a corticotomy and begins distraction. What is the standard recommended rate and rhythm of distraction?
Explanation
Question 29
A patient is undergoing distraction osteogenesis for a leg length discrepancy. After the corticotomy, the surgeon instructs the patient to wait 7 days before initiating the distraction protocol. What is the primary biological purpose of this 'latency period'?
Explanation
Question 30
You are reviewing the alignment parameters of a 50-year-old patient.
The patient's mechanical axis deviation (MAD) is perfectly normal (0 mm). However, the knee joint line obliquity is significantly altered relative to the floor. Which of the following best explains this phenomenon?
Explanation
Question 31
Which of the following is the most significant potential complication of distracting a bone segment at a rate faster than 1.5 mm per day during distraction osteogenesis?
Explanation
Question 32
A surgeon is correcting a multi-apical tibial deformity using a Taylor Spatial Frame (TSF). The frame programming utilizes a 'Virtual Hinge'. What does the concept of a virtual hinge represent in six-axis hexapod external fixation?
Explanation
Question 33
A patient with a distal tibial recurvatum deformity presents for preoperative planning. What is the normal anatomic Posterior Distal Tibial Angle (aPDTA) range used as a standard reference in the sagittal plane?
Explanation
Question 34
When calculating the Bone Healing Index (BHI) for a patient who has undergone tibial lengthening via distraction osteogenesis, what formula is strictly utilized?
Explanation
Question 35
A 16-year-old male with Blount's disease undergoes correction of a severe proximal tibial deformity.
Based on Paley's principles of oblique plane deformities, if a patient has both a coronal varus deformity and a sagittal apex posterior (procurvatum) deformity, what is the geometric relationship to the true plane of the deformity?
Explanation
Question 36
Which technique describes Fixator-Assisted Nailing (FAN) in the context of deformity correction?
Explanation
Question 37
A 14-year-old female presents with a 4 cm true leg length discrepancy secondary to physeal arrest, without any angular deformity. Lengthening Over a Nail (LON) is planned. What is the primary advantage of LON compared to classic Ilizarov external fixation lengthening?
Explanation
Question 38
A surgeon evaluates a malunited femur with a mechanical axis deviation (MAD) shifted 40 mm lateral to the center of the knee. The mLDFA is 75° and the MPTA is 87°. An osteotomy is planned. What nerve is at the highest risk of injury if a concomitant proximal fibular osteotomy is performed for a fibular release?
Explanation
Question 39
A 48-year-old male presents with a multi-apical deformity of the femur following a crush injury. When mapping the mechanical axes to determine the CORAs, the surgeon notes that the proximal and distal axes do not intersect with the middle segment axis at the same point. How should this multi-apical deformity be managed conceptually according to Paley's principles?
Explanation
Question 40
During the preoperative planning for a distal tibial deformity correction using a circular frame, you calculate the required angular correction.
What is the mathematical definition of the 'magnitude of deformity'?
Explanation
Question 41
A 28-year-old male sustains a diaphyseal tibial fracture that heals in 15 degrees of varus. A deformity correction is planned. The surgeon places both the osteotomy and the mechanical hinge axis exactly at the Center of Rotation of Angulation (CORA). According to Paley's principles, which of the following best describes the resulting correction?
Explanation
Question 42
A patient with a distal femoral valgus deformity is undergoing a corrective osteotomy.
The surgeon maps the CORA at the level of the joint line, but for soft tissue and biological reasons, chooses to make the osteotomy 4 cm proximal to the CORA. If the mechanical hinge is maintained at the CORA, what is the expected outcome?
Explanation
Question 43
During preoperative planning for a proximal tibial recurvatum deformity, the surgeon plans an osteotomy. By mistake, the surgeon places both the osteotomy cut and the hinge axis 3 cm away from the identified CORA. What is the geometric consequence of this technical error?
Explanation
Question 44
A 40-year-old female presents with medial compartment knee osteoarthritis and a varus thrust. Full-length radiographs show a mechanical axis deviation (MAD) 20 mm medial to the knee center. The mechanical Lateral Distal Femoral Angle (mLDFA) is 87 degrees, and the Medial Proximal Tibial Angle (MPTA) is 80 degrees. What is the primary source of the varus alignment?
Explanation
Question 45
When analyzing lower extremity alignment, the Anatomic Axis of the femur is not collinear with its Mechanical Axis. What is the normal relationship between the anatomic and mechanical axes of the femur?
Explanation
Question 46
A 16-year-old male is undergoing distraction osteogenesis for a tibial leg length discrepancy. After the corticotomy, a latency period is planned before beginning the distraction phase. What is the primary biological purpose of the latency period?
Explanation
Question 47
A 35-year-old male is currently undergoing lengthening of the left tibia using a circular external fixator. The distraction rate is set at 1.0 mm per day, divided into four increments. Three weeks into distraction, he develops an inability to actively dorsiflex his toes and reports decreased sensation in the first web space. What is the most appropriate initial management?
Explanation
Question 48
During the evaluation of a patient with a post-traumatic knee deformity, a weight-bearing radiograph reveals an abnormal Joint Line Convergence Angle (JLCA) of 6 degrees, opening laterally. What does an abnormal JLCA primarily indicate in the context of deformity planning?
Explanation
Question 49
A surgeon is planning to correct a pure translation deformity of the tibial diaphysis resulting from a prior malunion.
When tracing the proximal and distal anatomic axes of the tibia to find the Center of Rotation of Angulation (CORA), what geometric relationship will be observed?
Explanation
Question 50
A 12-year-old girl is undergoing significant lengthening of her tibia. To prevent one of the most common and debilitating joint contracture complications associated with this procedure, the surgeon must either fix the foot in the frame or institute an aggressive physical therapy protocol. Which specific deformity is the surgeon primarily trying to prevent?
Explanation
Question 51
A surgeon uses a Taylor Spatial Frame (TSF) to correct a complex multi-planar deformity of the femur. The mathematical software requires specific parameters to generate a correction schedule. Which of the following best describes the fundamental kinematic mechanism of the TSF?
Explanation
Question 52
When planning an opening wedge osteotomy for a varus deformity of the proximal tibia, the surgeon places the hinge on the lateral cortex. What is the expected biological gap behavior at the medial cortex during correction?
Explanation
Question 53
A patient with a distal tibial malunion has a mechanical Posterior Proximal Tibial Angle (mPPTA) of 81 degrees and an Anterior Distal Tibial Angle (ADTA) of 100 degrees. What sagittal plane deformity does the ADTA value indicate?
Explanation
Question 54
During a 6-cm tibial lengthening using an Ilizarov frame, a surgeon routinely secures the distal tibiofibular syndesmosis with a transverse wire. What is the primary purpose of this specific technical step?
Explanation
Question 55
A 50-year-old male is noted to have a "multi-apical" bowing deformity of his femur following childhood rickets. Preoperative templating reveals two distinct CORAs. If the surgeon decides to perform only a single osteotomy at a "compromise" CORA located between the two true CORAs, what unavoidable consequence will occur upon correcting the mechanical axis?
Explanation
Question 56
A patient undergoing distraction osteogenesis presents to the clinic with erythema and serous drainage around one of the proximal tibial half-pins. There is no pin loosening, and the patient is afebrile. According to the Paley modification of the Checkley-Macaulay classification, what is the best initial management?
Explanation
Question 57
Radiographic evaluation of a regenerate bone column during the consolidation phase of distraction osteogenesis reveals a "concave" or "hourglass" appearance. What is the most likely biomechanical or physiological cause of this regenerate morphology?
Explanation
Question 58
The concept of "tension-stress" in the regeneration of bone and soft tissue was extensively studied and popularized by Gavriil Ilizarov. Which of the following parameters is considered the optimal rhythm for bone distraction to maximize the tension-stress effect?
Explanation
Question 59
When calculating the Mechanical Axis Deviation (MAD) on a standing full-length radiograph, the normal mechanical axis line is drawn from the center of the femoral head to the center of the ankle mortise. Where does this line normally pass in relation to the center of the knee joint?
Explanation
Question 60
A surgeon is evaluating a post-traumatic supracondylar femoral malunion. The Lateral Distal Femoral Angle (mLDFA) is measured using the mechanical axis of the femur. If the surgeon decides to use the anatomic axis of the femur instead to calculate the distal femoral joint orientation, what is the corresponding normal anatomic angle (aLDFA)?
Explanation
Question 61
A 45-year-old female presents with a progressive valgus deformity of her right knee. Standing full-length radiographs reveal a mechanical axis deviation (MAD) of 30 mm lateral to the center of the knee. The mechanical lateral distal femoral angle (mLDFA) is 78°, the medial proximal tibial angle (MPTA) is 87°, and the joint line convergence angle (JLCA) is 1°. Based on Paley's malalignment test, which of the following is the primary source of the deformity?
Explanation
Question 62
A surgeon is planning to correct a diaphyseal tibial angular deformity using a monolateral external fixator. According to Paley's Osteotomy Rule 1, what is the expected outcome if both the osteotomy cut and the mechanical hinge are placed exactly at the Center of Rotation of Angulation (CORA)?
Explanation
Question 63
A 30-year-old male requires correction of a severe mid-diaphyseal varus deformity of the tibia. To promote faster healing, the surgeon performs the osteotomy in the proximal metaphysis but places the hinge of the external fixator exactly at the diaphyseal CORA. According to Paley's principles, what is the biomechanical result of this configuration?
Explanation
Question 64
During a distal femoral osteotomy for a varus deformity, the surgeon places the hinge axis and the osteotomy cut proximal to the actual CORA. What is the expected radiologic outcome of this technical error according to Paley's Osteotomy Rule 3?
Explanation
Question 65
A 55-year-old male with medial compartment knee osteoarthritis presents with a varus thrust. Radiographs show a medial MAD of 40 mm, mLDFA of 87°, MPTA of 86°, and a JLCA of 7° opening laterally. What does the abnormal JLCA primarily signify in the context of deformity planning?
Explanation
Question 66
A patient presents with an obvious clinical deformity of the leg. Radiographic analysis reveals that the proximal and distal anatomical axes of the tibia are perfectly parallel but not collinear. According to Paley's principles, where is the Center of Rotation of Angulation (CORA) located in a pure translational deformity?
Explanation
Question 67
A full-length weight-bearing radiograph demonstrates a complex tibial deformity with two distinct apices of angulation (multi-apical). If the surgeon plans a single osteotomy to correct the entire mechanical axis deviation, what is the most likely consequence?
Explanation
Question 68
When analyzing the sagittal plane alignment of the tibia for deformity correction, which of the following represents the normal Posterior Proximal Tibial Angle (PPTA)?
Explanation
Question 69
A 12-year-old girl with a congenital femoral deficiency has a severe valgus deformity and limb length discrepancy.
When utilizing the anatomical axis for preoperative planning of the femur, the surgeon must account for its normal relationship to the mechanical axis. What is the normal angle between the anatomical and mechanical axes of the femur?
Explanation
Question 70
A patient is evaluated for chronic knee pain. Full-length radiographs reveal an mLDFA of 81° (valgus) and an MPTA of 81° (varus). The mechanical axis deviation (MAD) is exactly 0 mm, passing perfectly through the center of the knee. What is this clinical entity, and what is its primary long-term risk?
Explanation
Question 71
When performing distraction osteogenesis using an Ilizarov circular fixator to treat a limb length discrepancy, what is the primary biological purpose of the 7-to-10 day 'latency period' before initiating distraction?
Explanation
Question 72
According to Ilizarov's principles of distraction osteogenesis for deformity correction and lengthening, what is the most optimal rate and rhythm of distraction to promote regenerate bone formation while avoiding premature consolidation or nonunion?
Explanation
Question 73
To maximize the axial stiffness of a circular external fixator (Ilizarov frame) during a complex deformity correction, which of the following modifications is most effective?
Explanation
Question 74
A surgeon is using a Taylor Spatial Frame (TSF) to correct a complex 6-axis tibial deformity.
To generate an accurate computer prescription, the software requires specific mounting parameters. What do these mounting parameters represent?
Explanation
Question 75
A 10-year-old child presents with a valgus deformity of the left knee. The surgeon opts for guided growth utilizing a tension band plate (eight-Plate) on the medial distal femur. Which of the following laws best describes the principle governing this deformity correction?
Explanation
Question 76
A surgeon is performing a medial opening-wedge high tibial osteotomy for a varus deformity. The preoperative plan indicates a significant correction angle requiring a concomitant fibular osteotomy to prevent tethering. If the surgeon performs the fibular osteotomy at the junction of the middle and distal thirds, which nerve is at the greatest risk of injury?
Explanation
Question 77
During preoperative planning for a distal tibial deformity, the mechanical axis line is found to fall outside the knee joint completely, and the CORA is located 3 cm proximal to the ankle joint. To avoid creating an unexpected translational deformity, how should the external fixator hinges be aligned?
Explanation
Question 78
A 60-year-old male presents with advanced medial compartment gonarthrosis and a varus deformity.
A high tibial osteotomy (HTO) is planned. The patient has a mechanical axis deviation (MAD) of 20 mm medial. If the surgeon aims to deliberately overcorrect the MAD to unload the medial compartment, where should the postoperative mechanical axis ideally pass through the tibial plateau?
Explanation
Question 79
When planning a deformity correction using the magnitude of deformity (angle), the intersection of the proximal and distal axes forms the CORA. Which plane requires the measurement of the Mechanical Lateral Distal Tibial Angle (mLDTA) for standard limb alignment assessment?
Explanation
Question 80
A patient with a distal third tibial malunion has a 15-degree procurvatum deformity and a 10-degree varus deformity. The surgeon plans a single-cut oblique osteotomy to correct both deformities simultaneously. In which plane is the true maximum deformity located?
Explanation
Question 81
A patient has a tibial diaphyseal deformity. Preoperative planning places the osteotomy exactly at the CORA, and the hinge of the external fixator is also placed at the CORA. What is the expected geometric outcome based on Paley's Osteotomy Rule 1?
Explanation
Question 82
A surgeon is planning to correct a distal femoral varus deformity. The CORA is located near the joint line, making an osteotomy at the CORA impossible due to inadequate distal fixation. The surgeon performs the osteotomy proximal to the CORA but places the hinge axis at the CORA. Which of Paley's rules does this describe, and what is the expected outcome?
Explanation
Question 83
A 25-year-old sustains a tibial malunion. An osteotomy is performed 4 cm proximal to the CORA, and the fixation hinge is also placed at the osteotomy site (not at the CORA). Based on Paley's Rule 3, what is the consequence of this construct?
Explanation
Question 84
Evaluating a full-length standing radiograph of a 40-year-old female with bilateral knee pain, the mechanical axis deviation (MAD) is found to be 30mm lateral to the center of the right knee. Which of the following normal radiographic parameter values is most critical for determining if the deformity originates in the distal femur?
Explanation
Question 85
A 30-year-old male with a history of rickets presents with a "windswept" deformity. On the right lower extremity, the joint line convergence angle (JLCA) is measured at 6 degrees. What does an abnormally high JLCA typically indicate in the context of deformity planning?
Explanation
Question 86
During distraction osteogenesis for a post-traumatic tibial length discrepancy using an Ilizarov frame, a patient asks about the optimal timing to begin lengthening after the corticotomy. What is the standard recommended latent period for a healthy adult metaphyseal corticotomy?
Explanation
Question 87
When performing the Malalignment Test to assess the lower extremity, the mechanical axis of the lower limb is drawn from the center of the femoral head to the center of the ankle plafond. In a normally aligned limb, where should this line pass relative to the knee joint?
Explanation
Question 88
A patient undergoes a closing wedge high tibial osteotomy (HTO) for a varus deformity. If the hinge of the osteotomy (the intact lateral cortex) does not perfectly align with the CORA, what compensatory change occurs according to the principles of deformity correction?
Explanation
Question 89
A 45-year-old sustains a tibial shaft fracture that heals in 15 degrees of valgus and 10 degrees of procurvatum.
To accurately locate the CORA for this multiplanar deformity, how should the planning be conducted?
Explanation
Question 90
During correction of a complex foot deformity using a Taylor Spatial Frame, what defines the "origin" of the virtual hinge in the frame's software?
Explanation
Question 91
A 16-year-old presents with a distal femoral valgus deformity. Radiographs show an mLDFA of 75 degrees. The surgeon decides to perform a medial closing wedge osteotomy. What happens to the overall limb length following a closing wedge osteotomy compared to an opening wedge?
Explanation
Question 92
A 28-year-old male with a post-traumatic distal tibial malunion requires correction. Preoperative assessment shows the mechanical Lateral Distal Tibial Angle (mLDTA) is abnormal. What is the generally accepted normal value for the mLDTA?
Explanation
Question 93
When calculating the true magnitude of an angular deformity that is present in both the coronal and sagittal planes, which of the following mathematical principles is commonly utilized?
Explanation
Question 94
A patient with a significant varus deformity of the proximal tibia is planned for a high tibial osteotomy (HTO). Based on the mechanical axis deviation, the CORA is identified exactly at the knee joint line. If an osteotomy is performed at the proximal metaphysis and the hinge is placed laterally at the osteotomy site, what will be the result?
Explanation
Question 95
When performing a corticotomy for distraction osteogenesis in the tibial diaphysis, which of the following techniques is most essential to preserve the endosteal blood supply and optimize the regenerate bone?
Explanation
Question 96
A 50-year-old female undergoes correction of a severe varus knee via a medial opening-wedge high tibial osteotomy. Postoperatively, she is unable to actively extend her great toe and reports numbness in the first web space. What is the most likely cause of this complication?
Explanation
Question 97
During preoperative planning for a distal femoral deformity, the surgeon evaluates the sagittal plane using the mechanical Posterior Distal Femoral Angle (mPDFA). What is the standard normal value for the mPDFA?
Explanation
Question 98
In the application of Paley's rules of deformity correction,
if the mechanical axes of the proximal and distal bone segments are found to be parallel but not collinear, which type of deformity is present?
Explanation
None
