ABOS Part I Orthopedic Deformity Analysis & Surgical Planning Comprehensive Review | Part 21921
Key Takeaway
ABOS Part I Orthopedic Deformity Analysis involves comprehensive radiographic assessment for lower limb alignment and surgical planning. Key components include the Mechanical Axis Test (MAT) to measure Mechanical Axis Deviation (MAD), Mechanical Lateral Distal Femoral Angle (mLDFA), Medial Proximal Tibial Angle (MPTA), and Joint Line Convergence Angle (JLCA). Identifying the Center of Rotation of Angulation (CORA) is crucial for precise osteotomy planning, ensuring accurate correction of varus/valgus and multiapical deformities.
ABOS Part I Orthopedic Deformity Analysis & Surgical Planning Comprehensive Review | Part 21921
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 55-year-old male presents with chronic right knee pain and a progressive varus deformity. A standing long-leg alignment radiograph is obtained, and the following measurements are recorded using the Mechanical Axis Test (MAT):
- Mechanical Axis Deviation (MAD): 20 mm medial
- Mechanical Lateral Distal Femoral Angle (mLDFA): 94°
- Medial Proximal Tibial Angle (MPTA): 87°
- Joint Line Convergence Angle (JLCA): 0°
Based on these findings, what is the primary osseous source of the patient's varus malalignment?

Explanation
Correct Answer: C
The normal range for the Mechanical Lateral Distal Femoral Angle (mLDFA) is 85°-90°. An mLDFA greater than 90° indicates a femoral varus deformity, which contributes to medial Mechanical Axis Deviation (MAD). In this patient, the mLDFA is 94°, which is outside the normal range and indicates a distal femoral varus deformity. The Medial Proximal Tibial Angle (MPTA) is 87°, which is within the normal range of 85°-90°, indicating no significant tibial deformity. The Joint Line Convergence Angle (JLCA) is 0°, which is within the normal range of 0°-2° medial convergence, ruling out significant ligamentous laxity or cartilage loss as the primary source of the osseous malalignment. Therefore, the primary osseous source of the varus malalignment is distal femoral varus.
Question 2
A 62-year-old female presents with severe bilateral knee pain and a progressive valgus deformity. A standing long-leg alignment radiograph of her left lower extremity reveals the following measurements:
- Mechanical Axis Deviation (MAD): 18 mm lateral
- Mechanical Lateral Distal Femoral Angle (mLDFA): 82°
- Medial Proximal Tibial Angle (MPTA): 92°
- Joint Line Convergence Angle (JLCA): 1° lateral
Which of the following best describes the combined sources of her valgus malalignment?

Explanation
Correct Answer: C
The normal range for the Mechanical Lateral Distal Femoral Angle (mLDFA) is 85°-90°. An mLDFA less than 85° indicates a femoral valgus deformity, contributing to lateral Mechanical Axis Deviation (MAD). In this case, the mLDFA is 82°, indicating distal femoral valgus. The normal range for the Medial Proximal Tibial Angle (MPTA) is 85°-90°. An MPTA greater than 90° indicates a tibial valgus deformity, also contributing to lateral MAD. Here, the MPTA is 92°, indicating proximal tibial valgus. The Joint Line Convergence Angle (JLCA) is 1° lateral, which is within the normal range of 0°-2° medial convergence, suggesting no significant medial ligamento-capsular laxity or lateral cartilage loss as a primary source of the osseous malalignment. Therefore, the combined sources of her valgus malalignment are distal femoral valgus and proximal tibial valgus.
Question 3
A resident is performing a Mechanical Axis Test (MAT) on a long-leg radiograph to assess a patient's frontal plane alignment. After drawing the necessary lines, they are measuring the orientation of the distal femur.
Which of the following represents the *normal* range for the Mechanical Lateral Distal Femoral Angle (mLDFA)?

Explanation
Correct Answer: B
The Mechanical Lateral Distal Femoral Angle (mLDFA) is a crucial measurement in assessing frontal plane alignment of the femur. It is formed by the distal femoral joint orientation line and the femoral mechanical axis. According to the provided text, the normal range for the mLDFA is 85°-90°. An mLDFA less than 85° indicates a femoral valgus deformity, while an mLDFA greater than 90° indicates a femoral varus deformity. Options A, C, D, and E represent ranges outside the established normal values.
Question 4
A 30-year-old patient with known internal tibial torsion requires a standing AP long-leg radiograph to accurately assess frontal plane knee alignment. The radiography technologist is preparing to position the patient.
To obtain a true AP view of the knee for accurate alignment assessment, how should the limb be positioned?

Explanation
Correct Answer: B
The text explicitly states that for a true AP view of the knee, the correct method is to orient the patella forward, irrespective of the foot position. This ensures that the knee's frontal plane (or the plane of the knee flexion-extension axis, which is approximately 3° externally rotated to the frontal plane) is perpendicular to the X-ray beam. If the foot is positioned forward in a patient with internal tibial torsion, the patella will point inward, leading to an inaccurate assessment of knee alignment (as shown in Fig. 3-1a and Fig. 3-2a). Palpating the patella and rotating the foot until the patella points forward is the described technique (Fig. 3-2b). Options A, C, D, and E describe incorrect or less accurate positioning methods for assessing true frontal plane knee alignment in the presence of torsional deformities.
Question 5
A 40-year-old patient with a 2.5 cm limb length discrepancy (LLD) due to a previous distal femoral fracture is scheduled for a standing long-leg alignment radiograph. The patient typically compensates for the LLD by flexing the contralateral knee and tilting their pelvis.
What is the most appropriate technique to ensure accurate alignment assessment and prevent compensatory mechanisms from affecting the measurements?

Explanation
Correct Answer: C
The text clearly states that if there is a limb length discrepancy (LLD), the shorter limb should be elevated on blocks adjusted to the approximate discrepancy (Fig. 3-8). This technique prevents the patient from using compensatory mechanisms such as contralateral knee flexion, ipsilateral ankle equinus, pelvic tilt, and scoliosis, which can alter alignment and leg length measurements. These compensatory mechanisms cause uneven loading of the limbs and can lead to inaccurate radiographic assessment. Options A, B, and E describe scenarios where compensatory mechanisms would be present or exacerbated, leading to inaccurate measurements. Option D, while eliminating weight-bearing compensation, does not assess functional standing alignment.
Question 6
A 68-year-old patient presents with chronic medial knee pain and a varus deformity on a standing long-leg radiograph. The Joint Line Convergence Angle (JLCA) is measured at 4° of medial convergence. The surgeon suspects either lateral collateral ligament laxity or significant medial compartment cartilage loss.
What additional radiographic study would be most beneficial to differentiate between these two potential sources of the increased JLCA?

Explanation
Correct Answer: C
The text states that the JLCA should be compared between films obtained with the patient in weight-bearing and non-weight-bearing positions to separate joint line convergence due to loss of cartilage height and ligamentous laxity. Furthermore, stress radiographs can also be used (Chaps. 3, 14, and 16). A varus stress radiograph (Fig. 3-10a) specifically assesses the integrity of the lateral collateral ligament and the stability of the lateral compartment. If the JLCA significantly increases under varus stress compared to a non-weight-bearing film, it indicates lateral collateral ligament laxity. If the JLCA remains similar to the weight-bearing film but is reduced on a non-weight-bearing film, it suggests cartilage loss as the primary factor. A valgus stress radiograph (Option D) would assess the medial collateral ligament, which is not the primary concern for a medially convergent JLCA in varus. Single-leg stance (Option A) and non-weight-bearing (Option B) AP radiographs can provide some information but are less specific than a stress view for differentiating ligamentous laxity from cartilage loss. A lateral view (Option E) assesses sagittal plane alignment and is not relevant for this frontal plane issue.
Question 7
A surgeon is performing a comprehensive deformity analysis of a patient's lower limb using the Mechanical Axis Test (MAT).
Which of the following deformities is *least reliably* identified by the Mechanical Axis Test (MAT)?

Explanation
Correct Answer: D
The text explicitly states that 'Malorientation of the ankle or hip joints usually leads to minimal or no MAD because the deformity apex is at or near the ends of the mechanical axis of the lower limb (center points of ankle and hip) (~Fig. 2-5). Therefore, the MAT does not reliably identify the presence of tibial and femoral deformities around the ankle or hip, respectively.' The MAT is primarily a malorientation test (MOT) of the knee. Distal femoral varus (Option A), proximal tibial valgus (Option B), knee joint subluxation (Option C), and medial compartment cartilage loss (Option E) are all directly assessed or inferred by the various steps of the MAT (mLDFA, MPTA, Addendum 1, and JLCA, respectively).
Question 8
A 28-year-old patient presents with chronic ankle pain and a suspected deformity. As part of a comprehensive deformity analysis, the orientation of the ankle joint is being assessed.
What is the normal range for the Lateral Distal Tibial Angle (LDTA) when measured relative to the tibial mechanical axis?

Explanation
Correct Answer: C
The text specifies the normal orientation of the ankle joint in the frontal plane. It states that 'The LDTA is normally 89±3° to these axes (~Fig. 2-6a).' This angle measures the orientation of the ankle joint line to the tibial mechanical and anatomic axes. Options A, B, D, and E represent incorrect values or refer to other angles (e.g., LPFA, MPFA, MNSA for the hip).
Question 9
A patient with a complex hindfoot deformity requires a radiographic assessment of the calcaneus-tibia alignment in the frontal plane. The surgeon wants a view that clearly shows the body of the calcaneus relative to the tibial diaphysis.
Which specialized radiographic view is described as having the X-ray beam angled 45° to the X-ray plate and foot (with the foot at 90° to the tibia) to achieve this visualization?

Explanation
Correct Answer: C
The text describes the 'long axial' view for assessing the alignment of the calcaneus to the tibia in the frontal plane. It states: 'To obtain this radiograph, the beam is angled 45° to the tibia with the foot at 90° to the tibia (~Fig. 3-16). The 'long axial' view can be obtained with the patient supine (~Fig. 3-16a) or standing (~Fig. 3-16b).' This view projects the tibial shaft onto the film, allowing measurement of the calcaneal axis relative to the tibial mid-diaphyseal line (Fig. 3-15). The Saltzman view (Option D) is an alternative method with a 20° beam and cassette inclination, which shows the ankle joint better but may foreshorten the calcaneus. Mortise (Option A) and Lateral (Option B) views are standard ankle views that do not provide this specific calcaneus-tibia alignment. Oblique view (Option E) is a general term for angled views but not specific to this technique.
Question 10
A 70-year-old patient with a significant knee flexion contracture (e.g., 30° procurvatum of the distal femur) requires an AP long-leg radiograph to assess frontal plane alignment. Standard AP views obtained with the beam perpendicular to the film show overlapped joint surfaces, making accurate measurements impossible.
To obtain a clear AP view of the knee joint surfaces for accurate measurement in this scenario, what modification to the radiographic technique is necessary?

Explanation
Correct Answer: C
The text addresses the challenge of obtaining clear radiographs when a deformity component exists in an orthogonal plane. Specifically, for a sagittal plane deformity affecting an AP view, it states: 'When there is a sagittal plane component of deformity, the AP view radiograph obtained in the usual fashion appears distorted (~Fig. 3-25a). To assess the joint orientation, the radiograph should be obtained inclined by the amount of sagittal plane angulation (~Fig. 3-25b and c).' This means angling the beam to be tangential to the joint surfaces, which in the case of procurvatum (flexion deformity) would involve aiming the beam upward from an anterior-proximal to a posterior-distal position. Options A, B, D, and E either do not address the issue of joint surface overlap, are impractical, or would not yield the desired frontal plane alignment information.
Question 11
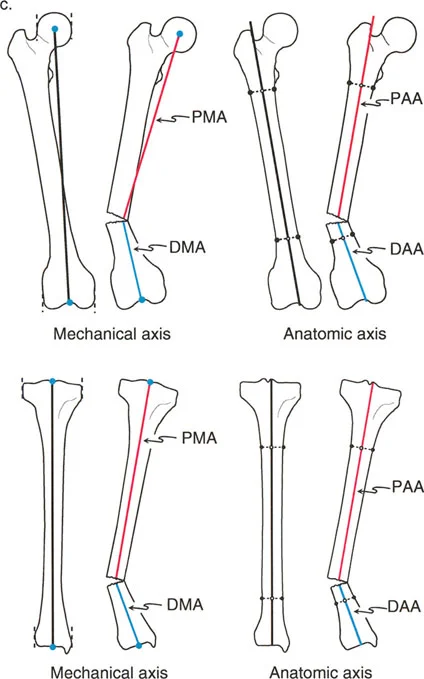
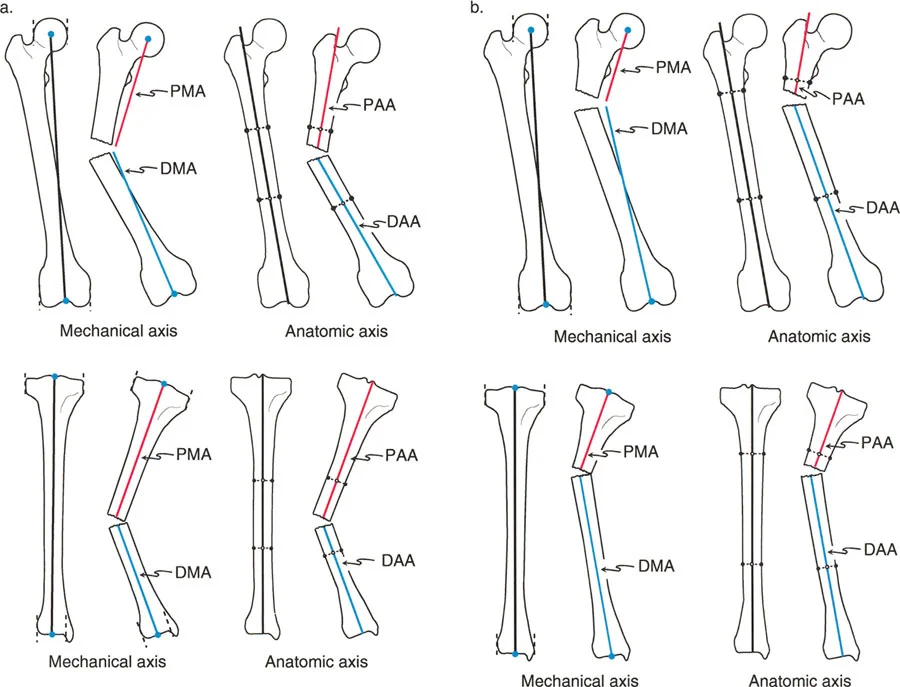
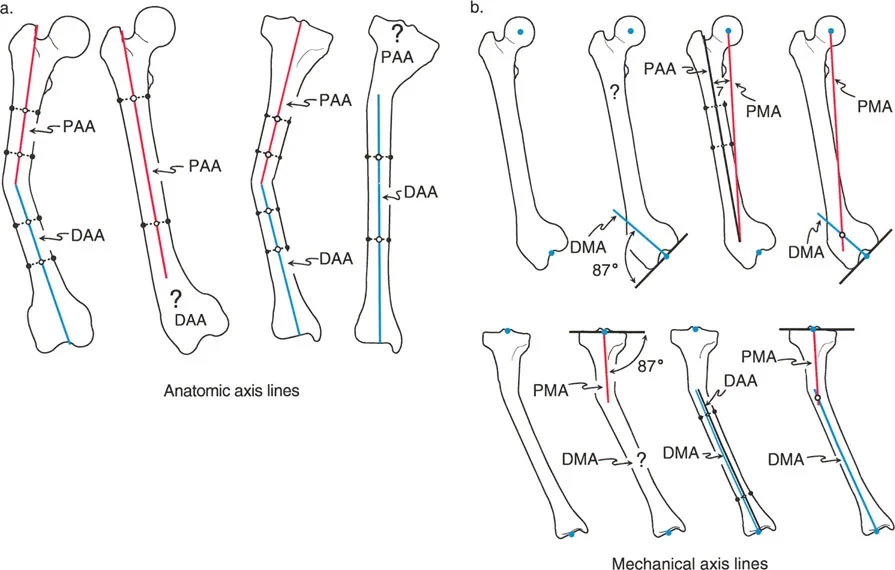
A 35-year-old male presents with a complex post-traumatic deformity of the right femur. During preoperative planning, the surgeon draws the anatomic and mechanical axes of the femur. Which of the following statements accurately describes the relationship between the femoral anatomic and mechanical axes in the frontal plane?
Explanation
Correct Answer: C
The case explicitly states, "in the frontal plane of the femur, the mechanical and anatomic axes diverge by approximately 7 degrees (± 2°). Therefore, the femoral PMA and PAA are distinctly different lines, as are the DMA and DAA. Recognizing this 7-degree divergence is critical when planning distal femoral osteotomies." This divergence is a fundamental concept in lower limb deformity correction.
Option A is incorrect because, while the tibial anatomic and mechanical axes are nearly collinear, the femoral axes are not. Conflating the two is a common pitfall.
Option B is incorrect. The anatomic axis of the femur exits proximally at the tip of the greater trochanter (or piriformis fossa), not through the center of the hip joint. The mechanical axis connects the center of the femoral head to the center of the knee joint.
Option D is incorrect. While the anatomic axis is indeed used for intramedullary nailing, it is not always parallel to the mechanical axis in the femur; they diverge by approximately 7 degrees.
Option E is incorrect. This statement reverses the definitions. The anatomic axis is defined by the mid-diaphyseal line, and the mechanical axis connects the center points of the joints.
Question 12
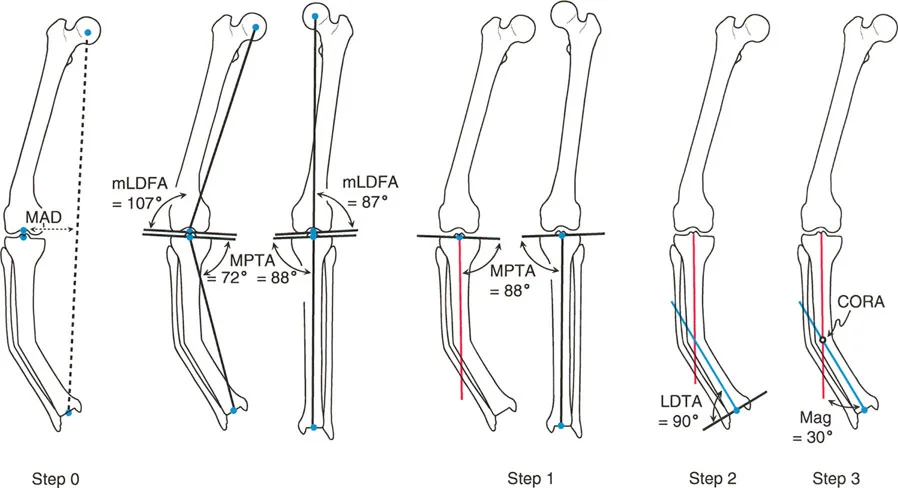
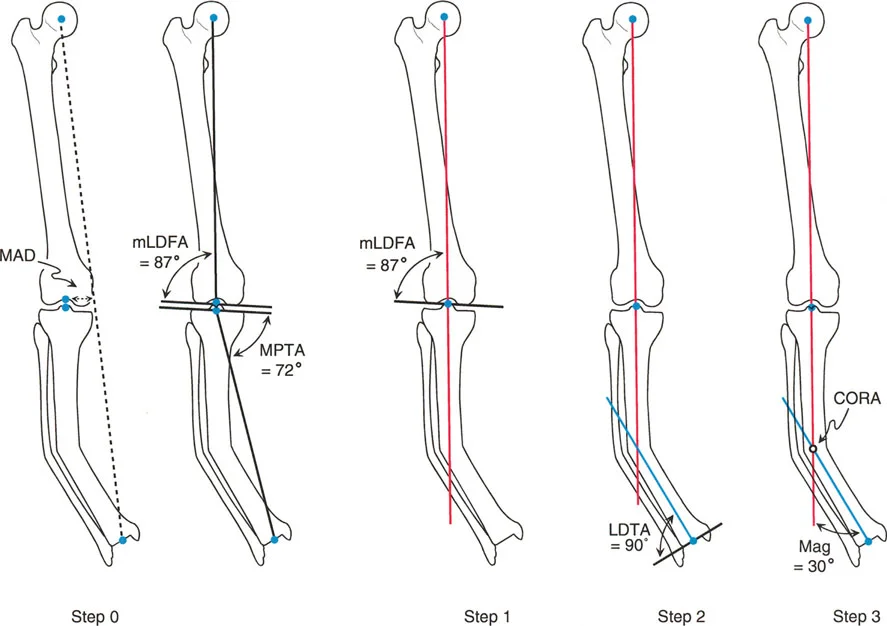
A 28-year-old patient presents with a post-traumatic varus deformity of the mid-diaphyseal tibia. During preoperative planning, the surgeon identifies the intersection point of the proximal and distal mechanical axes of the tibia, as shown in the image. What is the clinical significance of this intersection point, and what is the primary consequence of ignoring it during osteotomy planning?
Explanation
Correct Answer: B
The case defines the Center of Rotation of Angulation (CORA) as "The exact point at which these proximal and distal axis lines intersect." It further states, "The CORA is the holy grail of deformity planning. It dictates precisely where the apex of the deformity lies and, consequently, where the optimal level of the osteotomy (the bone cut) or hinge placement for a dynamic external fixator should be located." The critical consequence of ignoring the CORA is also highlighted: "If a surgeon ignores the CORA and simply cuts the bone wherever it is surgically convenient, they risk violating Paley's Osteotomy Rules. Cutting away from the CORA and simply angulating the bone to correct the axis will introduce iatrogenic translation—a 'dog-leg' deformity where the bone ends no longer line up anatomically."
Option A is incorrect. While the CORA is crucial for osteotomy, it is not directly the ideal location for intramedullary nail insertion, and malunion is a general complication, not the specific iatrogenic translation described.
Option C is incorrect. The angle formed at the CORA indicates the magnitude, but the CORA itself is the location. Ignoring the CORA leads to translation, not primarily nonunion.
Option D is incorrect. The CORA is the intersection of the proximal and distal axis lines (mechanical or anatomic, depending on planning), not where the anatomic and mechanical axes cross each other in a normal bone. Joint stiffness is not the primary consequence of ignoring the CORA.
Option E is incorrect. While the CORA can guide hinge placement for external fixators, it's not specifically for pin placement, and nerve damage is not the direct consequence of ignoring the CORA in terms of alignment.
Question 13
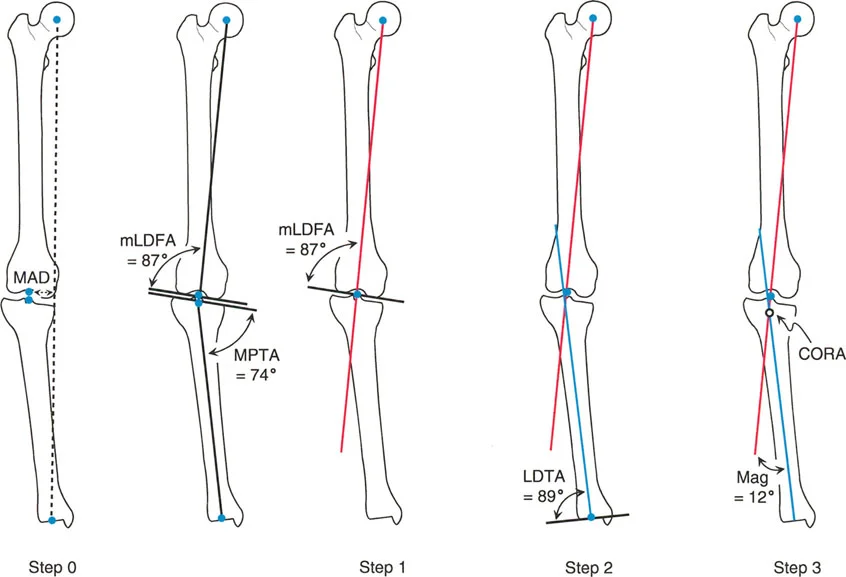
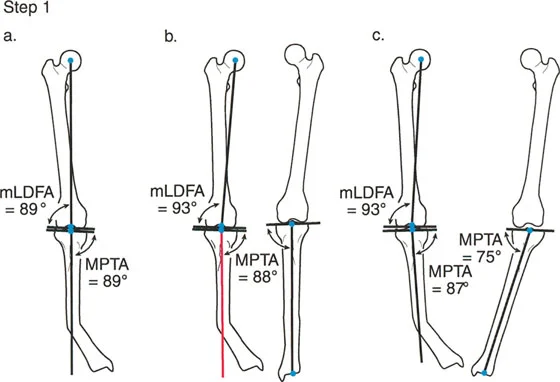
A 60-year-old patient presents with severe knee osteoarthritis and a suspected varus deformity of the right lower extremity. Before proceeding with detailed tibial axis planning, the surgeon performs a Malalignment Test (MAT) as the initial step. Which of the following best describes the primary purpose and components of this crucial prerequisite step?
Explanation
Correct Answer: C
The case explicitly states, "Before drawing any tibial axes, you must assess the entire lower limb macroscopically. This is Step 0—the absolute prerequisite to all localized planning." It then details the components: "1. Draw the Global Mechanical Axes... 2. Measure the Mechanical Axis Deviation (MAD)... 3. Measure Joint Orientation Angles (mLDFA, MPTA, and the Joint Line Convergence Angle (JLCA) on both sides)." The clinical criticality is also explained: "It tells you where the deformity is originating from. Is the massive MAD caused by a tibial deformity, a distal femoral deformity, or a combination of both?"
Option A is incorrect. Bone density assessment is not part of the MAT for deformity planning.
Option B is incorrect. While CORA identification is a later step in planning, the MAT is a global assessment, and a CT scan is not the primary tool for initial MAT.
Option D is incorrect. Limb length measurement is a separate assessment, not the primary purpose of the MAT.
Option E is incorrect. Soft tissue evaluation is important but not the core component of the radiographic MAT.
Question 14
A 40-year-old patient presents with a severe bilateral Blount's disease deformity affecting both tibias and femurs. The surgeon is planning a proximal tibial osteotomy on the right leg. After performing the Malalignment Test (MAT), it is determined that both the ipsilateral (right) femoral mechanical axis and the contralateral (left) proximal tibial mechanical axis are abnormal. In this specific scenario, how should the Proximal Tibial Mechanical Axis (PMA) be accurately drawn?
Explanation
Correct Answer: C
This question describes Scenario C for drawing the Proximal Tibial Mechanical Axis (PMA): "Abnormal Ipsilateral mLDFA and Abnormal Contralateral MPTA." The case states, "If the ipsilateral femur is deformed, AND the contralateral leg is also deformed... you have no patient-specific templates available. You must default to the population average normal MPTA, which is 87°. Draw the PMA starting from the center of the knee, extending distally at exactly an 87° angle to the proximal tibial joint line."
Option A is incorrect because this applies to Scenario A (Normal Ipsilateral mLDFA), which is not the case here.
Option B is incorrect because this applies to Scenario B (Abnormal Ipsilateral mLDFA, but Normal Contralateral MPTA), which is also not the case here as the contralateral MPTA is abnormal.
Option D is incorrect. While the anatomic axis uses mid-diaphyseal lines, the mechanical axis planning for the proximal tibia relies on the joint center and the MPTA, especially when the segment is short or deformed.
Option E is incorrect. This describes the global mechanical axis of the entire lower limb, not the PMA of the tibia.
Question 15
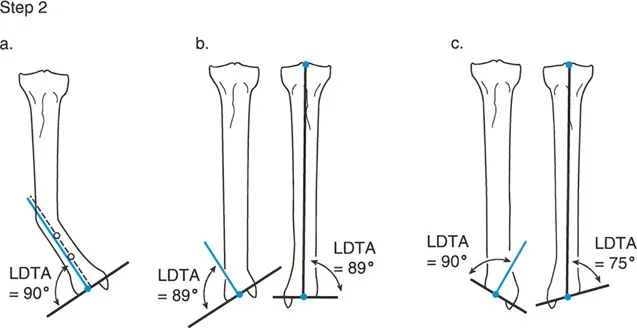
A 55-year-old patient presents with a tibial deformity primarily located in the proximal metaphysis. The distal tibia appears grossly straight on the full-length standing radiograph. When planning the Distal Tibial Mechanical Axis (DMA), the surgeon initially draws a line from the center of the ankle joint, extending proximally, parallel to the mid-diaphyseal line of the distal segment. What crucial additional step, as highlighted in the case, must the surgeon perform even if the distal tibia appears straight, and why?
Explanation
Correct Answer: B
The case specifically includes a "Surgical Pearl" under Scenario A for drawing the Distal Tibial Mechanical Axis (DMA): "Even if the distal tibia looks perfectly straight to the naked eye, you must perform the Malorientation Test (MOT) of the ankle. Draw the ankle plafond line and measure the LDTA. If it falls outside the 86-92° range, a hidden juxta-articular deformity is lurking, and your mid-diaphyseal line will lead to a malaligned ankle post-operatively." This emphasizes that a visually straight diaphysis does not preclude a subtle, but critical, juxta-articular deformity.
Option A is incorrect. While limb length discrepancy is important, it's not the specific additional step required for accurate DMA drawing in this context.
Option C is incorrect. The prerequisite for all planning is a full-length standing weight-bearing film, so this is assumed to be already done.
Option D is incorrect. While fibular alignment can be relevant in some complex cases, the immediate and crucial step for tibial DMA accuracy is the ankle MOT.
Option E is incorrect. In the tibia, the mechanical and anatomic axes are considered parallel, so comparing them for divergence is not the primary concern here; the concern is the joint orientation itself.
Question 16
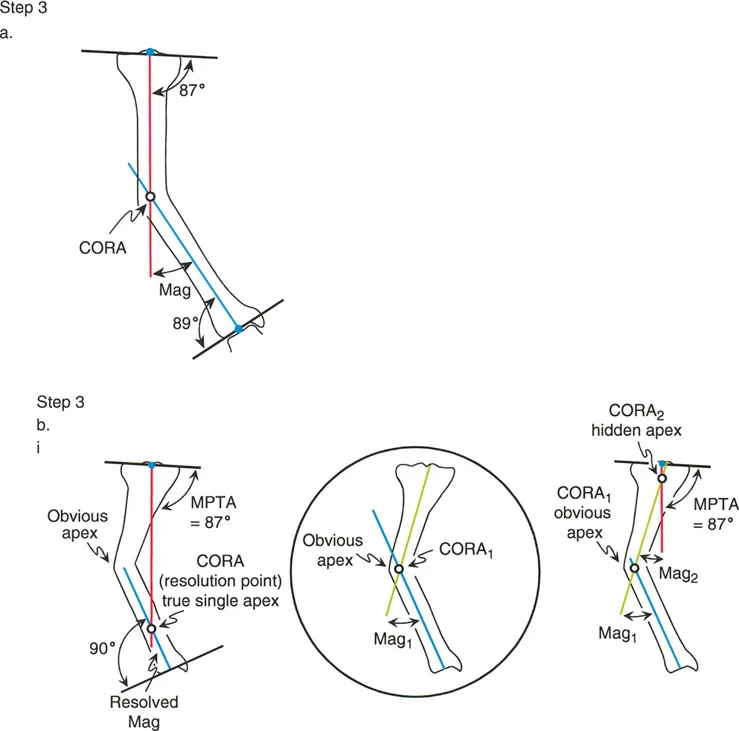
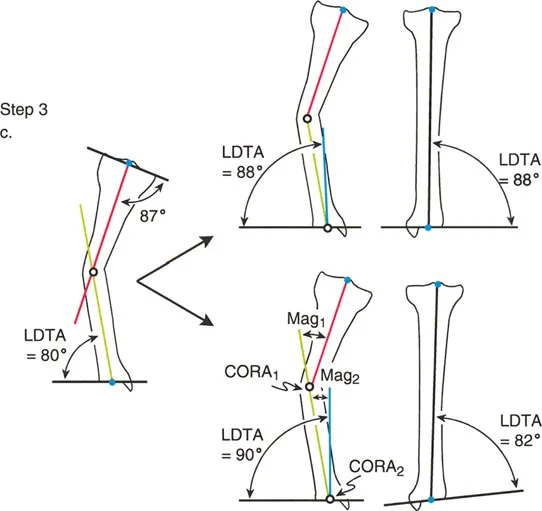
A 16-year-old patient presents with a complex tibial deformity following a physeal injury, exhibiting a sweeping curvature rather than a sharp angulation. After drawing the Proximal Mechanical Axis (PMA) and Distal Mechanical Axis (DMA), the surgeon finds that their intersection (the 'resolved CORA') falls significantly outside the bone cortex, and the single CORA does not correspond to the obvious anatomical apex of the bone's curvature. What does this finding indicate, and what is the appropriate next step in planning?
Explanation
Correct Answer: C
The case explicitly addresses this scenario under "Step 3b & 3c: Multiapical Deformities and Translation": "What if the CORA you mapped out falls completely outside the bone cortex, or does not match the obvious anatomical apex of the deformity? This is a critical diagnostic moment... It means one of two things is occurring: 1. There is a translation deformity present in addition to the angulation... 2. There is more than one apex of angulation (a multiapical deformity, such as a sweeping bow)." The solution is then provided: "To solve a multiapical deformity, you must break the bone down further by drawing a third line: the mechanical axis of the middle segment of the bone... You now have the precise locations and individual magnitudes (Mag 1 and Mag 2) for a double-level osteotomy." Performing a single osteotomy at a resolved CORA in a multiapical deformity will lead to a "dog-leg" deformity.
Option A is incorrect. Complex deformities are often correctable with advanced planning.
Option B is incorrect. This describes a uniapical deformity. The scenario explicitly states the CORA falls outside the bone and doesn't match the apex, indicating it's not a simple uniapical deformity.
Option D is incorrect. While CT can be helpful, the case describes a method for resolving this on a frontal plane radiograph.
Option E is incorrect. While rotational deformities exist and require different imaging, the described issue (CORA outside bone, not matching apex) specifically points to multiapical or translational deformity in the frontal plane.
Question 17
A 22-year-old patient requires a distal femoral osteotomy for valgus deformity. The surgeon is meticulously planning the correction using mechanical axis principles. Which of the following represents the normal average Mechanical Lateral Distal Femoral Angle (mLDFA) that should be targeted for correction?
Explanation
Correct Answer: B
The "High-Yield Joint Orientation Angles (Frontal Plane)" table in the case explicitly lists the normal average for the Mechanical Lateral Distal Femoral Angle (mLDFA) as 87°, with a normal range of 85° - 90°. This is a critical value to memorize for board exams and clinical planning.
Options A, C, D, and E are incorrect as they do not match the specified normal average for the mLDFA.
Question 18
A surgeon is planning a complex osteotomy for a patient with a severe multiapical tibial deformity. Due to the complexity and the need for gradual, multi-planar correction, the surgeon opts for a hexapod circular external fixator. According to Paley's Osteotomy Rules, if the surgeon places both the osteotomy and the hinge of the fixator away from the true CORA(s) of the deformity, what is the most likely outcome?
Explanation
Correct Answer: C
The case outlines "Rule of Osteotomy 3": "When the hinge and the osteotomy are both placed away from the CORA, a massive translation deformity is created, and the mechanical axis will not be fully corrected. This is a surgical failure." This rule highlights the critical importance of CORA-based planning to achieve both anatomic and mechanical axis correction.
Option A is incorrect. This describes Rule of Osteotomy 1, where both the osteotomy and hinge are at the CORA.
Option B is incorrect. This describes Rule of Osteotomy 2, where the hinge is at the CORA, but the osteotomy is at a different level.
Option D is incorrect. Placing the osteotomy and hinge away from the CORA leads to instability and poor alignment, which would hinder, not accelerate, healing.
Option E is incorrect. While overcorrection is a risk, the primary and most severe consequence of violating Rule 3 is uncorrected mechanical axis and massive translation, which is a fundamental failure of the correction.
Question 19
A 48-year-old patient presents with a long-standing varus deformity of the right lower extremity. To accurately plan the correction, the orthopedic surgeon requires a specific type of radiograph. Which of the following is the absolute prerequisite for accurate Mechanical Axis Deviation (MAD) calculation and overall frontal plane planning?
Explanation
Correct Answer: B
The case explicitly states this as a "Crucial Prerequisite" for the step-by-step masterclass: "This process must be performed meticulously on a high-quality, full-length, standing, weight-bearing AP radiograph of both lower extremities. Supine films or short knee-to-ankle films are entirely useless for accurate MAD calculation, as they eliminate the effect of gravity, ligamentous laxity, and the hip joint's contribution to alignment."
Option A is incorrect because the case specifically states these are "entirely useless" for accurate MAD calculation.
Option C is incorrect. A lateral radiograph is essential for sagittal plane planning but not for frontal plane MAD calculation.
Option D is incorrect. While a CT scan can provide detailed bony anatomy, it is typically performed supine and is not the primary or initial prerequisite for global frontal plane mechanical axis planning, which relies on weight-bearing films.
Option E is incorrect. An MRI is excellent for soft tissue and cartilage assessment but does not provide the full-length bony alignment required for mechanical axis planning.
Question 20
A 30-year-old patient has a severe juxta-articular varus deformity of the distal tibia, making it impossible to draw an accurate mid-diaphyseal line on the short distal segment. The contralateral limb is also affected by a similar deformity. When planning the Distal Tibial Mechanical Axis (DMA), the surgeon must reference the ankle joint orientation line. What is the population average normal Lateral Distal Tibial Angle (LDTA) that should be used in this scenario?
Explanation
Correct Answer: B
This scenario falls under "Step 2: Drawing the Distal Tibial Mechanical Axis (DMA) and Ankle MOT," specifically Scenario C: "Distal Tibial Deformity with Abnormal Contralateral LDTA." The case states, "If the deformity is distal and the opposite leg is also abnormal (or amputated), you must use the population average normal LDTA, which is 90° (though ranges from 86-92° exist, 90° is the standard, safe planning fallback). Draw the DMA from the center of the ankle, extending proximally at exactly 90° to the ankle joint line."
Option A (87°) is incorrect; this is the normal MPTA and mLDFA.
Options C, D, and E are incorrect as they do not represent the standard population average normal LDTA for planning in this specific scenario.
Question 21
A 50-year-old patient presents with a complex varus deformity of the proximal tibia, with the apex of the deformity located very close to the knee joint line (juxta-articular). The remaining proximal tibial segment is too short to reliably draw a mid-diaphyseal line. According to the principles of anatomic axis planning, what is the critical approach for drawing the axis line of such a short juxta-articular segment?
Explanation
Correct Answer: B
The case addresses this challenge under "Principles of Axis Planning - Anatomic Axis Planning - Metaphyseal and Juxta-Articular Deformities": "When the CORA is located very near the joint line, the remaining bone segment is too short, and the metaphysis flares out widely. You physically cannot draw an accurate mid-diaphyseal line on the articular side because there is no 'diaphysis' left to measure. To draw the axis line of a short juxta-articular segment, you must reference it off the joint line itself. If you know the normal intersection point and the normal population angle of the anatomic axis relative to the joint line, you can mathematically reconstruct the anatomic axis of that short segment."
Option A is incorrect. Extrapolating from a distal segment for a proximal juxta-articular deformity is not the correct method and would likely lead to error.
Option C is incorrect. Ignoring a significant part of the deformity will lead to incomplete correction and malalignment.
Option D is incorrect. While the femoral mechanical axis is used in some scenarios for the proximal tibial mechanical axis, this question specifically asks about anatomic axis planning for a short juxta-articular segment, which requires referencing the joint line itself.
Option E is incorrect. While MRI can show the medullary canal, the planning principles described rely on radiographic measurements and known angles relative to the joint line for reconstruction, not direct MRI drawing for this specific problem.
Question 22
A surgeon is planning a tibial osteotomy for a diaphyseal varus deformity. The osteotomy is planned exactly at the Center of Rotation of Angulation (CORA), and the axis of correction of angulation (ACA) will pass through the CORA. What is the expected geometric outcome of this correction?
Explanation
Question 23
A patient requires a distal femoral osteotomy for a valgus deformity. The surgeon plans the osteotomy proximal to the Center of Rotation of Angulation (CORA) due to poor bone quality at the CORA, but places the hinge (ACA) exactly at the CORA. Which of the following best describes the resulting correction?
Explanation
Question 24
During correction of a tibial shaft deformity, the osteotomy and the hinge (axis of correction of angulation, ACA) are both placed distal to the true Center of Rotation of Angulation (CORA). What is the primary mechanical consequence of this technical error?
Explanation
Question 25
When analyzing sagittal plane alignment of the femur and tibia on a full-length lateral radiograph, which of the following angle ranges best represents the normal Posterior Proximal Tibial Angle (PPTA)?
Explanation
Question 26
In a normal lower extremity, the mechanical axis of the femur deviates from the anatomic axis of the femur. What is the normal angle between the femoral mechanical axis and the femoral anatomic axis?
Explanation
Question 27
A patient presents with a tibial deformity consisting of 15 degrees of varus on the AP radiograph and 20 degrees of apex anterior (procurvatum) angulation on the lateral radiograph. Using the principles of deformity analysis, how should this deformity be fundamentally conceptualized for correction with a single hinge?
Explanation
Question 28
A 45-year-old patient has a significant genu varum deformity. On the standing AP long-leg radiograph, the Joint Line Convergence Angle (JLCA) is measured at 6 degrees, opening laterally. What is the most likely primary contributor to this abnormal JLCA?
Explanation
Question 29
A surgeon is planning a proximal tibial osteotomy for a varus deformity. Compared to an opening wedge osteotomy, a closing wedge osteotomy at this location will most likely result in which of the following?
Explanation
Question 30
During limb lengthening via distraction osteogenesis, what is the most universally accepted optimal rate and rhythm of distraction to promote high-quality regenerate bone while minimizing soft tissue complications?
Explanation
Question 31
What is the primary purpose of the latency period (typically 5-7 days) between the osteotomy and the initiation of distraction in limb lengthening?
Explanation
Question 32
In Paley's terminology of lower limb deformity, which of the following best defines /"malorientation/"?
Explanation
Question 33
A 6-year-old child presents with symptomatic genu valgum. The surgeon elects to perform guided growth using a tension band plate construct. Where should the plate be positioned to correct the deformity if the pathology is localized to the distal femur?
Explanation
Question 34
The Taylor Spatial Frame (TSF) utilizes the mathematical principles of a Stewart platform to correct complex deformities simultaneously. Which of the following is NOT one of the six degrees of freedom addressed by this hexapod system?
Explanation
Question 35
A patient has a distal femoral fracture that has healed with internal rotation malunion. How will this rotational deformity primarily affect the measurement of the Mechanical Lateral Distal Femoral Angle (mLDFA) on a standard anteroposterior (AP) radiograph?
Explanation
Question 36
When analyzing a tibia with a multi-apical deformity using the mechanical axis method, how are the multiple Centers of Rotation of Angulation (CORAs) typically identified?
Explanation
Question 37
A 12-year-old patient undergoing 5 cm of femoral lengthening with an external fixator develops decreased active and passive knee flexion and extension over 4 weeks. What is the most critical management strategy to prevent irreversible joint damage?
Explanation
Question 38
Which of the following is the primary mechanical advantage of utilizing a dome (cylindrical) osteotomy for the correction of a metaphyseal angular deformity compared to an opening wedge osteotomy?
Explanation
Question 39
A patient undergoes a proximal tibial osteotomy for a varus deformity. The center of rotation of angulation (CORA) is determined to be at the metaphyseal-diaphyseal junction. The surgeon plans an osteotomy distal to the CORA but places the hinge (axis of correction) exactly at the CORA. Which of the following describes the resulting correction?
Explanation
Question 40
In evaluating a lower extremity deformity, a standing full-length radiograph
reveals a mechanical axis deviation (MAD) of 30 mm medial to the knee center. The mechanical lateral distal femoral angle (mLDFA) is 87° and the medial proximal tibial angle (MPTA) is 78°. The joint line convergence angle (JLCA) is 2°. Which of the following is the primary location of the deformity?
Explanation
Question 41
During a comprehensive deformity analysis, the mechanical axis of the entire lower extremity must be determined. This axis is defined by a straight line connecting which of the following anatomical landmarks?
Explanation
Question 42
A 25-year-old male has a malunited tibial fracture with an apex anterolateral deformity. To achieve full correction of both the angulation and translation simultaneously using a single cut, the osteotomy and the hinge (axis of correction) must be placed at which of the following locations?
Explanation
Question 43
When evaluating the sagittal plane alignment of the normal lower extremity, the posterior distal femoral angle (PDFA) and posterior proximal tibial angle (PPTA) are expected to be approximately:
Explanation
Question 44
A 40-year-old female presents with a varus knee and a medial mechanical axis deviation (MAD). Her MPTA is 87°, mLDFA is 87°, and JLCA is 8°. A stress radiograph shows correction of the JLCA to 2°. What is the primary cause of her varus malalignment?
Explanation
Question 45
A surgeon is planning a distal femoral osteotomy for a valgus deformity. A lateral opening wedge osteotomy is chosen over a medial closing wedge. What is an expected biomechanical and dimensional consequence of this specific choice?
Explanation
Question 46
During deformity analysis using the anatomic axis method, the surgeon notes an angle of 7 degrees between the anatomic and mechanical axes of the normal femur (AMA). If a midshaft femoral deformity is corrected based solely on properly aligning the proximal and distal anatomic axes, what will be the effect on the mechanical axis?
Explanation
Question 47
An 18-year-old male with a shortened limb and a valgus deformity requires correction. A dome osteotomy is planned at the distal femur. What is the primary geometric advantage of a dome osteotomy in this scenario?
Explanation
Question 48
A patient requires a large angular correction of the proximal tibia for Blount's disease. During planning, the axis of correction (hinge) is placed on the convex (lateral) cortex. This placement of the hinge will mathematically result in:
Explanation
Question 49
A 30-year-old male presents with a multi-apical tibial diaphyseal deformity
. How is the mechanical axis analysis of a multi-apical deformity best approached?
Explanation
Question 50
A patient requires correction of a uniapical tibial deformity. The osteotomy is planned distant to the center of rotation of angulation (CORA), but the hinge axis is placed exactly on the CORA. According to Paley's osteotomy rules, what is the expected outcome of this correction?
Explanation
Question 51
A 16-year-old male presents with a mid-diaphyseal tibial varus deformity. During preoperative planning, the Center of Rotation of Angulation (CORA) is determined. According to Paley's osteotomy rules, if the osteotomy is performed at a level different from the CORA, but the hinge (axis of rotation) is placed exactly at the CORA, what is the expected outcome of the correction?
Explanation
None
