ABOS Part I & AAOS OITE Orthopaedic Surgery Exam Prep: Review Questions & Trauma Cases | Part 21576

Key Takeaway
This module offers 41 advanced multiple-choice questions designed to mirror the American Board of Orthopaedic Surgery (ABOS) Part I and AAOS OITE examinations. It covers high-yield clinical topics including sternoclavicular joint injuries, hip fractures, humeral shaft fractures, and open tibial fractures, providing comprehensive preparation for orthopaedic surgery board and in-training exams.
ABOS Part I & AAOS OITE Orthopaedic Surgery Exam Prep: Review Questions & Trauma Cases | Part 21576
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old male presents to the emergency department after a high-speed motor vehicle collision, sustaining a posterior sternoclavicular joint dislocation. During the initial assessment, he reports difficulty swallowing (dysphagia) and a change in voice (hoarseness).
Which of the following vital structures is MOST likely to be directly compressed or injured, contributing to the patient's dysphagia and voice changes?

Explanation
Correct Answer: D
The posterior sternoclavicular joint is in close proximity to several critical mediastinal structures. Dysphagia is directly caused by compression or injury to the esophagus, which lies immediately posterior to the trachea and the SC joint. Voice changes (hoarseness) are typically due to injury to the recurrent laryngeal nerve. The recurrent laryngeal nerve runs in the tracheoesophageal groove, making it highly susceptible to injury when the esophagus or trachea are compressed or displaced by a posterior SC joint dislocation. Therefore, compression in this region can simultaneously affect both the esophagus (leading to dysphagia) and the recurrent laryngeal nerve (leading to voice changes). While the trachea (C) can be compressed leading to airway issues, the esophagus (D) is the more direct cause of dysphagia. The subclavian artery (A) and brachial plexus (B) are vascular and neurological structures, respectively, that would typically present with different symptoms (e.g., diminished pulses, arm paresthesias/weakness). The phrenic nerve (E) controls the diaphragm and its injury would lead to respiratory compromise, not dysphagia or voice changes.
Question 2
A 28-year-old construction worker falls from a height, landing on his right shoulder. He presents with severe pain and a palpable deformity over his right sternoclavicular joint. A standard AP chest X-ray is inconclusive due to bony overlap. Given the high-energy mechanism, there is concern for a posterior dislocation and potential mediastinal involvement.
What is the most appropriate next diagnostic imaging study to accurately characterize the SC joint injury and assess for potential mediastinal involvement?

Explanation
Correct Answer: C
The gold standard for diagnosing and characterizing sternoclavicular (SC) joint dislocations, especially posterior dislocations, is a Computed Tomography (CT) scan with IV contrast. Axial cuts provide detailed information on the direction and degree of displacement relative to the manubrium. For posterior dislocations, a CT angiogram (CT-A) with IV contrast is mandatory to assess for impingement, compression, or laceration of mediastinal vessels and to evaluate the proximity of the clavicle to the trachea, esophagus, and lung apex. While a serendipity view radiograph (A) is helpful for initial screening, it lacks the sensitivity and specificity of CT, particularly for posterior dislocations and assessing vital structures. MRI (B) is useful for soft tissue injuries but less critical than CT for initial bony assessment and mediastinal structures. Ultrasound (D) has limited utility for deep bony and mediastinal structures. A lateral chest radiograph (E) would not provide sufficient detail for the SC joint.
Question 3
A 19-year-old football player sustains an injury during a tackle where he is hit directly on the anterolateral aspect of his shoulder while his arm is adducted and flexed. He immediately reports severe pain and a prominent deformity at his sternoclavicular joint, with the medial clavicle appearing to be displaced posteriorly.
Based on the mechanism described, which type of sternoclavicular joint dislocation is MOST likely to have occurred?

Explanation
Correct Answer: B
The case describes a classic mechanism for a posterior sternoclavicular joint dislocation. This typically results from an indirect force to the anterolateral shoulder, compressing the shoulder and driving the clavicle posteriorly and medially. Examples include dashboard injuries or, as in this case, a direct blow to the top of the shoulder with the arm adducted and flexed. Anterior dislocations (A) most commonly result from an indirect force to the posterolateral aspect of the shoulder, driving the clavicle anteriorly and medially (e.g., fall on an outstretched arm with the shoulder abducted and extended). Superior (C) and inferior (D) dislocations are not standard classifications. While a medial clavicular physeal fracture (E) can mimic a dislocation in skeletally immature patients, the described mechanism is a direct cause of a true posterior dislocation.
Question 4
A 40-year-old recreational athlete presents with an acute anterior sternoclavicular joint dislocation after a fall onto an outstretched arm. Clinical examination confirms an anterior displacement, and plain radiographs (including a serendipity view) show no associated fractures. He has mild pain and full, albeit uncomfortable, shoulder range of motion. There are no signs of neurovascular compromise.
What is the most appropriate initial management strategy for this patient?

Explanation
Correct Answer: C
Acute anterior sternoclavicular (SC) joint dislocations are most commonly managed non-operatively. Even if closed reduction is attempted and initially successful, recurrence is common due to the inherent instability of the joint and the difficulty in maintaining reduction. However, these recurrences are usually asymptomatic and rarely cause significant functional impairment or chronic pain. Initial management involves ice, analgesia, and a sling for comfort for 1-3 weeks, followed by gradual return to activities as tolerated. Emergent closed reduction (A) is often attempted but not strictly necessary if asymptomatic. Open reduction and K-wire fixation (B) is generally avoided for acute anterior dislocations due to the high complication rate of K-wires and the good outcomes with non-operative care. Surgical ligament reconstruction (D) is reserved for chronic, symptomatic instability. A CT angiogram (E) is not indicated for an anterior dislocation without signs of vascular compromise.
Question 5
A 25-year-old male presents to the emergency room after a motorcycle accident. He has an acute posterior sternoclavicular joint dislocation. On examination, he is dyspneic, has stridor, and his ipsilateral radial pulse is diminished compared to the contralateral side. A CT scan confirms posterior displacement of the medial clavicle impinging on the trachea and subclavian artery.
What is the absolute emergent indication for surgical intervention in this patient?

Explanation
Correct Answer: C
For acute posterior sternoclavicular (SC) joint dislocations, the presence of airway compromise (dyspnea, stridor) and neurovascular compromise (diminished pulses, subclavian artery impingement) constitutes an absolute emergent indication for surgical intervention. These symptoms indicate direct pressure on vital mediastinal structures, which can be life-threatening. While persistent pain and cosmetic deformity (A), risk of chronic instability (B), and patient's age/activity level (E) are considerations for surgical intervention in other contexts, they are not emergent absolute indications. Inability to perform closed reduction (D) would lead to open reduction, but the absolute emergent indication is the compromise of vital structures, which necessitates immediate action regardless of reduction method.
Question 6
During a surgical approach to the sternoclavicular joint for chronic instability, the surgeon aims to identify and reconstruct the primary static stabilizer of the joint, which resists superior displacement and provides significant resistance to anterior, posterior, and medial translation.
Which ligament is the surgeon primarily targeting for reconstruction based on its described function?

Explanation
Correct Answer: D
The costoclavicular ligament (rhomboid ligament) is described in the case as the primary static stabilizer of the SC joint. It consists of two laminae extending from the inferior surface of the medial clavicle to the superior surface of the first rib. It strongly resists superior displacement of the clavicle and provides significant resistance to anterior, posterior, and medial translation, as well as axial rotation. Its integrity is paramount for SC joint stability. The anterior (A) and posterior (B) sternoclavicular ligaments primarily resist posterior and anterior translation, respectively. The interclavicular ligament (C) primarily resists inferior displacement. The coracoclavicular ligament (E) stabilizes the acromioclavicular joint, not the sternoclavicular joint.
Question 7
A 16-year-old patient undergoes open reduction and temporary K-wire fixation for an unstable acute posterior sternoclavicular joint dislocation. Six weeks post-operatively, the patient develops sudden onset chest pain, dyspnea, and a new heart murmur.
Based on the provided case information and the known risks of K-wire fixation for SC joint injuries, what is the MOST likely complication this patient is experiencing?

Explanation
Correct Answer: C
The symptoms of sudden onset chest pain, dyspnea, and a new heart murmur in a patient with K-wire fixation across the sternoclavicular joint are highly suggestive of K-wire migration into mediastinal structures. The case explicitly states that K-wires are 'highly discouraged due to significant complication rates, including migration into mediastinal structures (heart, great vessels, lung).' This is a historically significant and potentially fatal complication. Superficial wound infection (A) would present with local signs of inflammation. Recurrent dislocation (B) would typically present with pain and deformity, not acute cardiac/respiratory symptoms. Post-traumatic osteolysis (D) is a chronic, painful condition, not an acute life-threatening event. Supraclavicular nerve neuropraxia (E) would cause sensory deficits in the neck/shoulder, not chest pain or dyspnea.
Question 8
A 14-year-old male presents with a painful, prominent medial clavicle after a wrestling injury. Radiographs appear to show a posterior sternoclavicular joint dislocation. However, the orthopedic surgeon notes that in skeletally immature patients, this presentation can be misleading.
What is the MOST common underlying injury mimicking a true sternoclavicular joint dislocation in this age group?

Explanation
Correct Answer: B
In skeletally immature patients, what appears to be a sternoclavicular (SC) joint dislocation is often a Salter-Harris Type I or II epiphyseal fracture of the medial clavicle. The medial clavicular physis is the last physis to close, typically around 20-25 years of age, making it a common site of injury in adolescents. The epiphysis displaces relative to the metaphysis, mimicking a true joint dislocation. Posterior displacement of the epiphysis requires careful reduction due to the same risks as true posterior dislocations in adults. Acromioclavicular joint separation (A), glenohumeral joint dislocation (C), scapular fracture (D), and first rib fracture (E) are distinct injuries that do not typically mimic an SC joint dislocation in this specific manner.
Question 9
A 55-year-old patient has suffered from chronic, symptomatic anterior sternoclavicular joint instability for over a year, despite extensive non-operative management including physical therapy and injections. She experiences persistent pain, clicking, and functional limitations.
What is the most appropriate surgical intervention for this patient's chronic symptomatic anterior sternoclavicular joint instability?

Explanation
Correct Answer: C
For chronic symptomatic sternoclavicular (SC) joint instability (anterior or posterior) that has failed adequate non-operative management (typically 3-6 months), surgical intervention is indicated. The primary surgical options are medial clavicle resection arthroplasty (especially for degenerative arthritis or persistent pain with some anterior instability) or ligament reconstruction. Ligament reconstruction, often using autograft (e.g., semitendinosus, palmaris longus) in a figure-of-8 pattern, is the mainstay for restoring stability. Emergent closed reduction (A) is for acute injuries. Primary repair of the anterior SC ligament (B) might be attempted in acute settings if the tissue quality is good, but for chronic instability, the ligaments are often attenuated or scarred, making reconstruction more effective. Temporary K-wire fixation (D) is strongly discouraged due to high complication rates. Observation with continued pain medication (E) is not appropriate for debilitating chronic symptoms that have failed conservative care.
Question 10
A patient has just undergone a successful open reduction and ligament reconstruction for a chronic posterior sternoclavicular joint dislocation. The surgeon is discussing the immediate post-operative rehabilitation protocol with the physical therapist.
During the initial 0-6 week post-operative phase, which of the following is a critical precaution or restriction that MUST be strictly adhered to?

Explanation
Correct Answer: C
During the initial 0-6 week post-operative phase following sternoclavicular (SC) joint reconstruction, the primary goal is protection of the surgical repair to allow tissue healing. For posterior repairs, strict avoidance of abduction and external rotation of the ipsilateral arm is a critical precaution. The arm is typically immobilized in a sling or figure-of-8 bandage. Full active range of motion, including overhead activities (A), and immediate return to resistance exercises (B) are contraindicated as they would stress the healing repair. Unrestricted weight-bearing (D) is also not allowed. Discontinuation of pain medication (E) is medically inappropriate and unrelated to rehabilitation precautions.
Question 11
A 78-year-old female presents with an unstable intertrochanteric hip fracture after a ground-level fall. Radiographs demonstrate significant comminution of the posteromedial cortex. During preoperative planning, the orthopedic surgeon reviews the biomechanical principles of proximal femoral stability. Referring to the provided image of the proximal femur, which anatomical structure, when compromised by comminution, is a primary predictor of varus collapse and fixation failure in intertrochanteric fractures?
Explanation
Correct Answer: C
The correct answer is C. The case explicitly states, 'The calcar femorale, a dense vertical plate of bone originating from the posteromedial aspect of the femoral shaft and extending into the posterior femoral neck, is a critical structural landmark. Loss of posteromedial support due to comminution of the calcar is a primary predictor of varus collapse and fixation failure in intertrochanteric fractures.' This structure provides crucial medial buttress support against varus collapse in intertrochanteric fractures.
A. Wards triangle is a relative void in the trabecular network, becoming more prominent in osteoporotic bone, but its comminution is not described as the primary predictor of varus collapse in intertrochanteric fractures. It's more relevant to overall bone quality and screw purchase.
B. The lateral tensile trabeculae are part of the internal architecture, but their disruption is not specifically highlighted as the primary predictor of varus collapse in the context of posteromedial comminution, which is the role of the calcar.
D. The greater trochanter is an attachment site for abductor muscles; while its integrity is important for muscle function, its comminution is not the primary predictor of varus collapse in the same manner as the calcar femorale.
E. The lesser trochanter is the insertion site for the iliopsoas. Its avulsion or comminution can indicate an unstable fracture pattern (e.g., reverse obliquity), but the loss of posteromedial support leading to varus collapse is specifically attributed to the calcar femorale in the case description.
Question 12
A 35-year-old male sustains a Garden IV displaced femoral neck fracture after a high-energy motor vehicle accident. He is taken to the operating room for urgent open reduction and internal fixation. The surgical team is acutely aware of the high risk of avascular necrosis (AVN) in this type of injury. Which of the following arterial structures is considered the dominant contributor to the femoral head's blood supply and is most vulnerable to disruption in displaced femoral neck fractures?
Explanation
Correct Answer: C
The correct answer is C. The case states, 'The primary supply is derived from the medial circumflex femoral artery and the lateral circumflex femoral artery, which form an extracapsular arterial ring at the base of the femoral neck. The medial circumflex femoral artery is the dominant contributor, giving rise to the lateral epiphyseal artery via the retinacular vessels that ascend along the posterosuperior aspect of the femoral neck within the synovial reflection.' Displacement of femoral neck fractures tears or occludes these retinacular vessels, predisposing the femoral head to avascular necrosis.
A. The lateral circumflex femoral artery contributes to the extracapsular ring but is not the dominant contributor to the femoral head's blood supply, especially via the critical retinacular vessels.
B. The obturator artery contributes to the blood supply of the acetabulum and surrounding soft tissues but is not a primary direct supply to the femoral head itself.
D. The artery of the ligamentum teres (foveal artery), a branch of the obturator artery, provides a minor and often inconsistent supply to the femoral head, particularly in adults, and cannot compensate for the loss of the retinacular vessels.
E. The profunda femoris artery is a major artery of the thigh, giving rise to the circumflex femoral arteries, but it does not directly supply the femoral head. Its branches (medial and lateral circumflex) are the direct suppliers.
Question 13
A 42-year-old active male presents with a femoral neck fracture following a fall from a ladder. Radiographs reveal a displaced fracture with a Pauwels angle of 70 degrees. The orthopedic surgeon notes this high angle as a significant concern for fixation failure. Based on the biomechanical principles discussed in the case, what is the primary implication of a high Pauwels angle on the fracture site?
Explanation
Correct Answer: C
The correct answer is C. The case explicitly states, 'The Pauwels classification, based on the angle of the fracture line relative to the horizontal, dictates the ratio of shear to compressive forces. High Pauwels angles inherently have higher shear forces, acting as a strong predictor for nonunion and fixation failure.' A 70-degree angle is a Pauwels Type III, which is characterized by predominantly shear forces.
A. High Pauwels angles lead to increased shear forces, not compressive forces. Increased compressive forces are associated with lower Pauwels angles (Type I) and are generally more favorable for healing.
B. High Pauwels angles are associated with increased shear forces, which decrease, not enhance, stability and predispose to nonunion and failure.
D. The Pauwels classification primarily relates to mechanical stability and the risk of nonunion, not directly to the risk of avascular necrosis, which is more related to initial displacement and disruption of the retinacular vessels.
E. High shear forces at the fracture site make load sharing more challenging and increase the risk of implant failure, rather than improving it.
Question 14
A 68-year-old male presents with an unstable intertrochanteric hip fracture. During preoperative templating, the surgeon measures the lateral wall thickness on the anteroposterior radiograph, as shown in the image. The measurement is found to be 18 mm. Based on the case's guidelines, what is the most appropriate implant choice for this patient?

Explanation
Correct Answer: C
The correct answer is C. The case states, 'The lateral wall thickness must be measured on the anteroposterior radiograph; a thickness of less than twenty point five millimeters is a strong predictor of lateral wall fracture during sliding hip screw insertion, necessitating the use of a cephalomedullary nail.' With a lateral wall thickness of 18 mm (which is less than 20.5 mm), a cephalomedullary nail is indicated to prevent iatrogenic lateral wall fracture and subsequent construct failure.
A. A sliding hip screw (SHS) is contraindicated in this scenario due to the thin lateral wall. Insertion of an SHS would likely lead to a lateral wall fracture, causing the proximal fragment to slide laterally, resulting in massive shortening and construct failure.
B. Cannulated cancellous screws are typically used for femoral neck fractures, not intertrochanteric fractures, and would not provide adequate stability for an unstable intertrochanteric fracture.
D. Hemiarthroplasty is rarely indicated for intertrochanteric fractures, typically reserved for femoral neck fractures in elderly patients or salvage situations with severe pre-existing osteoarthritis and highly comminuted osteoporotic bone.
E. Total hip arthroplasty is also rarely indicated for intertrochanteric fractures, similar to hemiarthroplasty, and is primarily used for femoral neck fractures or severe osteoarthritis.
Question 15
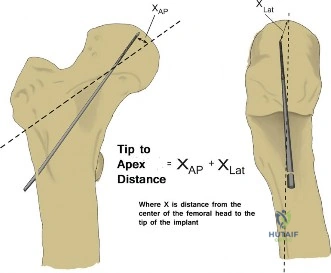
A 55-year-old male undergoes internal fixation with a sliding hip screw for a stable intertrochanteric fracture. Postoperatively, the surgeon reviews the fluoroscopic images and calculates the Tip Apex Distance (TAD). To minimize the risk of lag screw cutout, what is the critical threshold for the Tip Apex Distance that the surgeon should aim to achieve?
Explanation
Correct Answer: C
The correct answer is C. The case explicitly states, 'The concept of Tip Apex Distance, defined as the sum of the distance from the tip of the lag screw to the apex of the femoral head on both views, is critical. A Tip Apex Distance of less than twenty five millimeters has been definitively shown to minimize the risk of lag screw cutout.' This is further reinforced in the 'Summary of Key Literature and Guidelines' section, which highlights Baumgaertner et al.'s work establishing this threshold.
A, B, D, E. These options represent incorrect thresholds. While a smaller TAD is generally better, the established critical threshold for minimizing cutout risk is specifically less than 25 mm, as per the seminal literature and guidelines referenced in the case.
Question 16
An 82-year-old female, 3 months post-sliding hip screw fixation for an intertrochanteric fracture, presents with increasing groin pain and difficulty weight-bearing. Radiographs show the lag screw has migrated superiorly through the femoral head articular surface. The surgeon identifies this as implant cutout. Which of the following is NOT a primary predictor of implant cutout as described in the case?
Explanation
Correct Answer: E
The correct answer is E. The case states, 'Implant cutout is the most common mode of mechanical failure, characterized by the migration of the lag screw through the superior articular surface of the femoral head. Predictors of cutout include a Tip Apex Distance greater than twenty five millimeters, varus malreduction, superior placement of the lag screw, and severe osteoporosis.' Conversely, the case advocates for 'early, safe mobilization' and 'weight-bearing as tolerated immediately following surgery,' noting that 'Restricting weight-bearing in the elderly is often impractical, leads to deconditioning, and does not significantly decrease the rate of mechanical failure.'
A. A Tip Apex Distance (TAD) greater than 25 mm is a well-established primary predictor of cutout, as highlighted in the case.
B. Varus malreduction shifts the weight-bearing axis medially and increases shear forces, drastically increasing the risk of cutout, as described in the case.
C. Superior placement of the lag screw is explicitly listed as a predictor of cutout in the case, as it places the screw in a less dense, more vulnerable part of the femoral head.
D. Severe osteoporosis significantly reduces bone mineral density and architectural integrity, decreasing the pullout strength of screws and increasing the risk of cutout, as mentioned in the case.
Question 17
A 48-year-old male, 18 months after internal fixation of a displaced femoral neck fracture, presents with persistent hip pain and progressive collapse of the femoral head, as depicted in the provided image. Radiographs confirm subchondral collapse and secondary osteoarthritis. The most likely etiology for this complication, as described in the case, is:

Explanation
Correct Answer: C
The correct answer is C. The clinical presentation of persistent hip pain, progressive collapse of the femoral head, and secondary osteoarthritis, occurring months to years after a femoral neck fracture, is classic for avascular necrosis (AVN). The case states, 'Avascular necrosis is a devastating complication primarily associated with femoral neck fractures. It results from the disruption of the retinacular vessels at the time of injury or due to elevated intracapsular pressure. It typically presents months to years after the index procedure with subchondral collapse and secondary osteoarthritis.'
A. Implant cutout typically presents earlier with acute pain and radiographic evidence of screw migration through the articular surface, not progressive collapse over 18 months.
B. Nonunion is a failure of the fracture to heal, often presenting with persistent pain and progressive hardware failure (e.g., screw breakage, telescoping), but not typically with subchondral collapse of the femoral head itself, unless AVN is a contributing factor.
D. Surgical site infection would typically present with signs of inflammation, fever, drainage, and possibly osteolysis, but not primarily with subchondral collapse in this delayed fashion without other infectious signs.
E. Stress shielding can occur with overly rigid implants, potentially leading to bone resorption, but it does not typically cause the specific pattern of subchondral collapse and secondary osteoarthritis characteristic of AVN.
Question 18
A 72-year-old active female presents with a Garden III displaced femoral neck fracture. She has well-controlled hypertension and is otherwise healthy. Concurrently, a 45-year-old male presents with a Garden III displaced femoral neck fracture after a motorcycle accident. Based on the case's indications, what is the most appropriate primary surgical management for each patient, respectively?
Explanation
Correct Answer: B
The correct answer is B. The case provides clear guidelines for femoral neck fractures: 'In the elderly population with displaced femoral neck fractures, arthroplasty is generally preferred due to the unacceptably high rates of fixation failure, nonunion, and avascular necrosis associated with internal fixation.' For the 72-year-old active female with a Garden III (displaced) fracture, arthroplasty (either hemiarthroplasty or total hip arthroplasty, with THA offering superior functional outcomes in active elderly patients as per HEALTH trial) is indicated. The table further specifies 'Displaced fractures (Garden III and IV) in elderly patients' as an indication for arthroplasty. For the 45-year-old male with a displaced femoral neck fracture, the case states, 'Internal fixation is generally indicated to preserve the native joint when the blood supply to the femoral head is presumed intact or when the patient is young enough that arthroplasty would inevitably lead to multiple future revisions.' The table lists 'Displaced fractures in young patients (typically under 60 years)' as an indication for operative fixation.
A. Internal fixation for the 72-year-old is associated with high failure rates. Hemiarthroplasty for the 45-year-old would be premature, as joint preservation is preferred in younger patients.
C. Hemiarthroplasty for the 72-year-old is a reasonable option, but total hip arthroplasty for the 45-year-old is generally avoided as a primary treatment for a salvageable femoral neck fracture due to the high likelihood of future revisions.
D. Non-operative management is reserved for non-ambulatory patients with minimal pain or those with unacceptable anesthetic risk, which does not describe the 72-year-old active female. Internal fixation for the 45-year-old is correct.
E. Internal fixation for the 72-year-old is generally not preferred for displaced fractures. Total hip arthroplasty for the 45-year-old is generally avoided as a primary treatment for a salvageable femoral neck fracture.
Question 19
An 85-year-old male undergoes cephalomedullary nailing for an unstable intertrochanteric hip fracture. Postoperatively, the patient's family asks about the rehabilitation plan and long-term care. Based on the case's recommendations, which of the following statements represents the most appropriate post-operative management strategy?
Explanation
Correct Answer: B
The correct answer is B. The case strongly advocates for 'early, safe mobilization' and states, 'In the vast majority of cases, patients should be allowed weight-bearing as tolerated immediately following surgery.' It also emphasizes, 'Furthermore, a hip fracture is a sentinel event for severe osteoporosis. Secondary fracture prevention must be initiated prior to discharge. This includes a comprehensive endocrinology evaluation, dual energy x-ray absorptiometry scanning, and the initiation of appropriate pharmacological interventions...'
A. Strict non-weight-bearing is generally not recommended for modern hip fracture fixation in appropriately selected patients, as it leads to deconditioning and does not significantly decrease mechanical failure rates.
C. Limited toe-touch weight-bearing is often impractical and unnecessary. VTE prophylaxis is mandatory for a minimum of four weeks postoperatively, regardless of specific risk factors beyond the trauma itself.
D. VTE prophylaxis is typically low molecular weight heparin or direct oral anticoagulants for a minimum of four weeks, not therapeutic anticoagulation for 6 months, unless there are specific indications for long-term therapeutic anticoagulation.
E. Delayed mobilization is contrary to the recommended immediate weight-bearing as tolerated. Restricting weight-bearing does not significantly decrease the rate of mechanical failure and can lead to deconditioning.
Question 20
A hospital system is reviewing its hip fracture care pathway to align with current evidence-based guidelines. They are particularly interested in strategies to reduce mortality and complication rates. Based on the 'Summary of Key Literature and Guidelines' in the case, which two recommendations should be prioritized for implementation?
Explanation
Correct Answer: C
The correct answer is C. The case states, 'The American Academy of Orthopaedic Surgeons clinical practice guidelines strongly recommend early surgery, ideally within twenty four to forty eight hours of admission, to reduce mortality and complication rates. The guidelines also emphasize the necessity of co-management with geriatric or internal medicine services to optimize preoperative medical status and manage postoperative medical complications, reflecting the multidisciplinary approach required to successfully treat this fragile patient population.'
A. Non-operative management is rarely indicated for intertrochanteric fractures, and delayed surgery (beyond 24-48 hours) is contrary to AAOS guidelines and increases mortality/complication rates.
B. While hemiarthroplasty is an option for elderly displaced femoral neck fractures, the HEALTH trial showed THA provides superior functional outcomes in active elderly patients. Restricting weight-bearing is generally not recommended and does not significantly decrease mechanical failure rates.
D. While achieving a TAD of less than 25 mm is crucial, it's not the sole focus for overall hip fracture care pathway improvement. Discontinuing routine VTE prophylaxis is contrary to mandatory guidelines for hip fracture patients.
E. Internal fixation for displaced femoral neck fractures in elderly patients is associated with unacceptably high failure rates, making arthroplasty the preferred option. Bisphosphonate therapy (or other osteoporosis treatment) should be initiated prior to discharge, not delayed for 6 months.
Question 21
A 32-year-old male sustains a closed, isolated mid-diaphyseal humeral shaft fracture after a fall from a bicycle. Initial radiographs confirm a spiral fracture pattern with 15 degrees of varus angulation and 1 cm of shortening. He presents with a new-onset radial nerve palsy, characterized by wrist drop and inability to extend his thumb and fingers. After 3 months of non-operative management with a functional brace, repeat radiographs show early callus formation but no significant change in angulation or shortening. Clinically, there is no improvement in his radial nerve function. What is the MOST appropriate next step in management?
Explanation
Correct Answer: B
The patient presents with a closed humeral shaft fracture and a new radial nerve palsy. The case states that after 3 months of non-operative management, there is no improvement in radial nerve function. According to the teaching case and current literature, for closed humeral shaft fractures with a new radial nerve palsy, initial non-operative management (observation) is generally recommended, with 70-90% spontaneous recovery expected within 3-6 months. However, if there is no sign of recovery after this period (typically 3-6 months), surgical exploration is indicated. Given the 3-month mark with no recovery, and the presence of a fracture that could benefit from fixation (even if angulation is borderline acceptable, the persistent nerve palsy warrants exploration), proceeding with surgical exploration of the radial nerve and internal fixation of the fracture is the most appropriate next step.
Option A is incorrect because while most radial nerve palsies recover spontaneously, waiting another 3 months without any signs of recovery after the initial 3 months would delay potential nerve repair or decompression, especially when surgical fixation of the fracture is also a consideration.
Option C is incorrect because while physical therapy is important, it does not address the lack of nerve recovery. Re-evaluating in 6 months without intervention for a non-recovering nerve at 3 months is a delay in definitive management.
Option D is incorrect because while an EMG/NCS study can provide valuable information about the extent of nerve injury, the clinical absence of recovery after 3 months is a strong enough indication for exploration, especially when combined with the need for fracture fixation. The study might confirm the lack of recovery but would delay surgical intervention.
Option E is incorrect because while a dynamic wrist-hand orthosis is appropriate for supporting the wrist and fingers in radial nerve palsy, scheduling for tendon transfers at 6 months without first exploring the nerve for potential repair or decompression would be premature. Tendon transfers are typically considered for permanent deficits after nerve recovery potential has been exhausted or exploration has confirmed irreparable damage.
Question 22
During an anterolateral approach to the mid-shaft humerus for a comminuted fracture, the surgeon retracts the biceps brachii muscle medially. The image below depicts the next layer of muscle encountered, which is then longitudinally incised to expose the humerus. Which of the following statements regarding the neurovascular structures in this immediate vicinity is MOST accurate?

Explanation
Correct Answer: C
The image depicts the brachialis muscle, which is encountered deep to the biceps brachii after medial retraction. The teaching case explicitly states: 'The musculocutaneous nerve (C5-C7) is located in the fascial plane between the biceps and brachialis. It typically pierces the coracobrachialis and then runs between the biceps and brachialis, supplying both. It then continues as the lateral antebrachial cutaneous nerve. Identify and protect the main trunk of the musculocutaneous nerve, usually by retracting it medially with the biceps.'
Option A is incorrect because the main trunk of the musculocutaneous nerve typically lies superficial to the brachialis (between biceps and brachialis) and enters the brachialis in its mid-belly, not deep to it. Longitudinal incision of the brachialis can injure its distal branches, but the main trunk is usually protected by medial retraction of the biceps.
Option B is incorrect because in the mid-shaft, the radial nerve is located in the spiral groove on the posterior aspect of the humerus. It only becomes more anterior in the distal third of the humerus. Therefore, it is not anterior to the brachialis in the mid-shaft and is not typically identified and protected laterally in the primary dissection plane of the anterolateral approach, though it is at risk from overly long screws or aggressive posterior dissection.
Option D is incorrect because the profunda brachii artery accompanies the radial nerve in the spiral groove, on the posterior aspect of the humerus, not the musculocutaneous nerve, and is not a primary concern during the longitudinal incision of the brachialis muscle itself, unless dissection extends too far posteriorly.
Option E is incorrect because the axillary nerve is a critical structure in the proximal humerus (approximately 5-7 cm distal to the acromion), not typically in the mid-shaft region where the brachialis is being incised. Its risk is primarily during proximal extension of the approach or aggressive deltoid retraction.
Question 23
A 68-year-old female with osteopenia presents with a comminuted mid-diaphyseal humeral fracture after a low-energy fall. She is scheduled for open reduction and internal fixation via an anterolateral approach. During pre-operative templating, the surgeon plans to use a locking compression plate (LCP) and bicortical screws. Which of the following statements regarding screw placement and potential neurovascular injury is MOST critical to consider?
Explanation
Correct Answer: C
The teaching case explicitly highlights the radial nerve as the most commonly injured nerve in humeral shaft fractures and their surgical treatment. It states: 'Though posterior, careless anterior dissection, overly aggressive subperiosteal stripping, or placement of excessively long bicortical screws can endanger the radial nerve.' The radial nerve runs in the spiral groove on the posterior aspect of the humerus in the mid-shaft, making it vulnerable to penetration by screws that are too long.
Option A is incorrect because while the musculocutaneous nerve supplies the brachialis, the primary risk to its main trunk is during the initial dissection between the biceps and brachialis, or if the brachialis split is too lateral. Bicortical screw placement through the brachialis is not the primary mechanism of injury for the musculocutaneous nerve, especially compared to the radial nerve's vulnerability to screw length.
Option B is incorrect because the axillary nerve wraps around the surgical neck of the humerus (proximal humerus), approximately 5-7 cm distal to the acromion. It is not at highest risk from distal bicortical screws; rather, it is at risk during proximal extension of the approach or aggressive deltoid retraction.
Option D is incorrect because the brachial artery and veins are located medial to the biceps and coracobrachialis, generally not directly posterior to the humerus. While aggressive medial retraction could injure them, they are not typically at risk from bicortical screws placed from the anterolateral aspect through the posterior cortex.
Option E is incorrect because the cephalic vein is a superficial vein in the subcutaneous tissue, typically retracted laterally. It is not at risk from bicortical screws placed into the bone, as these screws pass through the bone itself, not the superficial soft tissues where the cephalic vein resides.
Question 24
A 28-year-old male sustains a high-energy segmental humeral shaft fracture with significant comminution and 4 cm of shortening. He is a polytrauma patient with associated pelvic and tibial fractures. He is hemodynamically stable. Which of the following is the MOST compelling indication for operative management of his humeral fracture via an anterolateral approach?
Explanation
Correct Answer: D
While all the options represent valid considerations for operative management, the patient's polytrauma status is often the most compelling indication for early stabilization of long bone fractures, including the humerus. The teaching case lists 'Polytrauma Patient: Early stabilization facilitates nursing care, pulmonary toilet, and overall rehabilitation' as a key indication. In a polytrauma setting, early fracture stabilization helps reduce pain, minimizes blood loss, decreases the risk of fat embolism, and allows for easier patient mobilization, hygiene, and management of other injuries, ultimately improving overall outcomes.
Option A is incorrect because while segmental fractures are often unstable and prone to nonunion, making them an indication for surgery, the polytrauma status often takes precedence in the acute decision-making process for overall patient management.
Option B is incorrect because while young age and high functional demand are factors favoring operative management for faster recovery, they are not as acutely compelling as the polytrauma status in the immediate post-injury phase.
Option C is incorrect because 4 cm of shortening does exceed the generally accepted non-operative limit of 2-3 cm, making it an indication for surgery. However, in a polytrauma patient, the systemic benefits of early stabilization are often prioritized.
Option E is incorrect because comminuted fractures typically benefit from relative stability (bridging plates) rather than absolute stability, which is usually reserved for simple, transverse, or short oblique fractures with lag screw fixation. While comminution is an indication for operative fixation, the statement about absolute stability is incorrect, and the polytrauma status is a stronger overall indication.
Question 25
A 45-year-old construction worker undergoes an anterolateral approach for a mid-diaphyseal humeral fracture. Post-operatively, he develops a new radial nerve palsy. Which of the following is the LEAST likely cause of this iatrogenic injury during the surgical procedure?
Explanation
Correct Answer: D
The teaching case describes the radial nerve's course in the spiral groove on the posterior aspect of the humerus. It explicitly states that 'careless anterior dissection, overly aggressive subperiosteal stripping, or placement of excessively long bicortical screws can endanger the radial nerve.' The radial nerve is vulnerable to direct injury from instruments or screws that extend too far posteriorly.
Option A is incorrect because aggressive subperiosteal stripping on the posterior aspect of the humerus can directly injure the radial nerve, which lies in the spiral groove.
Option B is incorrect because placement of an excessively long bicortical screw from the anterolateral plate is a classic mechanism of iatrogenic radial nerve injury, as the screw can penetrate the posterior cortex and impinge or transect the nerve.
Option C is incorrect because a reduction clamp applied to the posterior cortex, especially if placed blindly or without careful consideration of the radial nerve's location, can directly compress or injure the nerve.
Option D is the correct answer because excessive medial retraction of the biceps brachii muscle is LEAST likely to cause radial nerve injury. The biceps brachii is retracted medially to expose the brachialis. The radial nerve is located posteriorly in the spiral groove in the mid-shaft. Medial retraction of the biceps primarily risks the musculocutaneous nerve (which lies between the biceps and brachialis) or the brachial artery/veins (if retraction is excessively medial and deep), but not the radial nerve directly.
Option E is incorrect because drilling through the far cortex without adequate protection or measurement is a direct precursor to placing an excessively long screw, thus putting the radial nerve at risk.
Question 26
A 55-year-old male undergoes an anterolateral approach for a proximal third humeral shaft fracture. During the approach, the surgeon needs to extend the dissection proximally to ensure adequate plate purchase. Which of the following anatomical considerations is MOST critical when extending the approach proximally?
Explanation
Correct Answer: C
The teaching case specifically addresses the proximal humerus (proximal third) approach: 'The axillary nerve is the most critical structure in this region. It wraps around the surgical neck of the humerus approximately 5-7 cm distal to the acromion, supplying the deltoid and teres minor. Meticulous protection of this nerve is essential, particularly when reflecting the deltoid or extending the approach proximally.'
Option A is incorrect because while the cephalic vein is an important superficial landmark, its identification and protection are generally part of the initial superficial dissection and less critical than the axillary nerve when extending the approach proximally into the deeper structures around the surgical neck.
Option B is incorrect because the musculocutaneous nerve is primarily at risk during the mid-shaft approach, between the biceps and brachialis. While it's important to protect, the axillary nerve is the paramount concern in the proximal third.
Option D is incorrect because the radial nerve pierces the lateral intermuscular septum in the distal third of the humerus to reach the anterior compartment. This is a concern for distal extensions, not proximal.
Option E is incorrect because the brachialis muscle is typically incised in the mid-shaft and distal approaches. While it has dual innervation, the primary concern for proximal extension is the axillary nerve, not the brachialis incision.
Question 27
A 72-year-old female with a history of osteoporosis sustains a comminuted humeral shaft fracture. She is scheduled for plate osteosynthesis via an anterolateral approach. The surgeon plans to use a locking compression plate (LCP). Which biomechanical principle is MOST relevant to the use of an LCP for this fracture pattern?
Explanation
Correct Answer: B
The teaching case states: 'Relative Stability: Achieved with bridging plates (locking or non-locking) for comminuted fractures, allowing for controlled motion at the fracture site to promote indirect bone healing.' It further clarifies: 'In comminuted fractures or osteoporotic bone, locking screws provide angular stability, creating a fixed-angle construct that acts as an internal fixator, primarily providing relative stability.'
Option A is incorrect because absolute stability through interfragmentary compression is typically achieved with lag screws for simple, transverse, or short oblique fractures, not primarily with bridging LCPs for comminuted fractures.
Option C is incorrect because the teaching case states: 'The anterolateral surface is mechanically advantageous for resisting bending forces.' It is also effective against torsional forces, but the statement incorrectly limits its advantage.
Option D is incorrect because LCPs are designed to function as internal fixators with minimal plate-to-bone contact, preserving periosteal blood supply. Extensive periosteal stripping is generally avoided to preserve vascularity.
Option E is incorrect because while LCPs provide stable fixation, the primary goal is to allow for early, safe mobilization and rehabilitation, not immediate full weight-bearing, especially in osteoporotic bone where construct failure is a risk.
Question 28
A 38-year-old male presents with a distal third humeral shaft fracture extending towards the elbow joint. He is scheduled for an anterolateral approach. As the surgeon extends the approach distally, which neurovascular structure requires the MOST vigilant identification and protection due to its changing anatomical course?
Explanation
Correct Answer: C
The teaching case specifically addresses the distal approach: 'As the approach is extended distally, the radial nerve becomes increasingly superficial and anterior. Below the spiral groove, the radial nerve pierces the lateral intermuscular septum to lie between the brachialis and brachioradialis. Careful identification and protection of the radial nerve are critical when dissecting in the distal third. It should be located, mobilized, and protected laterally or posterolaterally.'
Option A is incorrect because the axillary nerve is a proximal structure, wrapping around the surgical neck, and does not become more superficial distally.
Option B is incorrect because while the musculocutaneous nerve does exit the brachialis and continues as the lateral antebrachial cutaneous nerve, its primary risk is in the mid-shaft. The radial nerve's course change in the distal third makes it the most critical structure to protect during distal extension of this approach.
Option D is incorrect because the brachial artery is located medial to the biceps and coracobrachialis. While always important to protect, its course does not change in a way that makes it uniquely vulnerable during distal extension of an anterolateral approach compared to the radial nerve.
Option E is incorrect because the ulnar nerve is located posteromedially in the distal arm and enters the cubital tunnel behind the medial epicondyle. It is not typically encountered or at risk during an anterolateral approach to the humeral shaft.
Question 29
A 22-year-old male sustains an open, comminuted humeral shaft fracture after a motor vehicle accident. He has no neurovascular deficits on presentation. Which of the following is an absolute contraindication to proceeding with immediate open reduction and internal fixation via an anterolateral approach?
Explanation
Correct Answer: C
The teaching case lists 'Absolute Contraindications: Active local infection at the surgical site (relative if debridement and staging are possible)' as a contraindication. Active infection at the surgical site is a critical concern that typically necessitates initial debridement and management of the infection before definitive internal fixation, as implanting hardware into an infected field carries a very high risk of chronic osteomyelitis and implant failure.
Option A is incorrect because significant comminution is listed as a relative contraindication if extensive soft tissue stripping is required, but it is not an absolute contraindication, especially for an open fracture that requires stabilization.
Option B is incorrect because a history of smoking is a risk factor for nonunion but is not an absolute contraindication to surgery. It is a patient factor that needs to be managed, but not a reason to completely avoid surgery.
Option D is incorrect because open fractures are a strong indication for operative management (debridement and stabilization), not a contraindication. While staging may be necessary, the open nature itself is not an absolute contraindication to operative intervention.
Option E is incorrect because a patient's young age is not a contraindication; rather, it often supports operative management for faster recovery and return to high-demand activities. While intramedullary nailing is an alternative, it is not an absolute contraindication to plating.
Question 30
Following an anterolateral approach and plate osteosynthesis for a humeral shaft fracture, a patient is in the immediate post-operative protection phase (Weeks 0-2). Which of the following rehabilitation activities is MOST appropriate during this phase?
Explanation
Correct Answer: D
The teaching case outlines the 'Phase 1 Immediate Post-Operative Protection (Weeks 0-2)' with the goal to 'protect surgical site, initiate gentle distal ROM, prevent shoulder stiffness.' Under exercises, it states: 'Hand, Wrist, Finger ROM: Active flexion/extension, circumduction, grip strengthening. Encourage frequently to prevent stiffness and edema.'
Option A is incorrect because the protocol states: 'Avoid active abduction and external rotation' in Phase 1 to protect the healing fracture and soft tissues.
Option B is incorrect because progressive resistive exercises are introduced in Phase 3 (Weeks 6-12), not in the immediate post-operative phase.
Option C is incorrect because while gentle active and passive elbow ROM is initiated, it is typically within a comfortable range (e.g., 30°-120° initially), avoiding excessive stress on the fracture site. Full active range of motion, especially against gravity, is usually progressed later.
Option E is incorrect because the protocol explicitly states: 'Non-weight-bearing on the affected extremity' during Phase 1.
Question 31
A 40-year-old male undergoes an anterolateral approach for a mid-diaphyseal humeral fracture. During the initial superficial dissection, the surgeon identifies a prominent superficial vein coursing along the lateral aspect of the biceps. What is the MOST appropriate management of this vein during the approach?
Explanation
Correct Answer: C
The teaching case states under 'Superficial Anatomy': 'Cephalic Vein: This superficial vein is a critical landmark, typically found coursing in the deltopectoral groove proximally and then along the lateral aspect of the biceps distally. It should be identified and carefully retracted laterally throughout the approach to minimize bleeding and preserve venous drainage.'
Option A is incorrect because ligating a critical superficial vein like the cephalic vein, especially if it's prominent, can compromise venous drainage of the forearm and hand, leading to edema. Preservation is preferred.
Option B is incorrect because the cephalic vein is typically lateral to the biceps. Retracting it medially would pull it across the surgical field and potentially put it at higher risk of injury or compromise its natural course.
Option D is incorrect because dissecting deep to the vein would place it in the path of deeper dissection, increasing its risk of injury. It should be superficial to the main dissection plane.
Option E is incorrect because the cephalic vein is a significant superficial vein. Ignoring it or assuming it will self-seal if transected is poor surgical practice and can lead to significant bleeding and post-operative complications.
Question 32
A 32-year-old male presents to the emergency department after a high-energy motor vehicle accident with the injury shown in the clinical photograph. He is hemodynamically stable, and a full neurovascular exam reveals intact distal pulses and sensation. After initial ATLS protocol, the most appropriate next step in the management of this open fracture, prior to definitive surgical planning, is:
Explanation
Correct Answer: C
The case explicitly outlines the initial management for an open fracture in the emergency department. After ATLS principles, the specific steps for the open fracture include: performing a full neurovascular examination, removing any obvious contamination, photographing the wound, covering it with a saline-soaked swab, providing analgesia, splinting the limb, obtaining radiographs (if not already done), administering IV antibiotics as per local protocols (e.g., cefuroxime 1.5g IV), and assessing the need for tetanus prophylaxis. This comprehensive approach addresses immediate wound care, pain management, stabilization, and infection prevention.
Option A: While early surgical debridement is important, the '6-hour rule' has been debunked by studies like LEAP, which found no difference in infection rates when managed within 6 or 24 hours. Immediate surgical debridement is not the next step after ATLS but rather the definitive surgical intervention, which requires prior preparation.
Option B: Oral antibiotics are generally insufficient for open fractures, which require intravenous broad-spectrum antibiotics. While a sterile dressing is part of the management, it's not the complete initial picture.
Option D: Direct wound closure is contraindicated in open fractures due to the high risk of trapping bacteria and increasing infection rates. The wound should be debrided and irrigated in the operating room before considering closure or coverage.
Option E: While a vascular injury is a critical concern, the vignette states that a full neurovascular exam revealed intact distal pulses and sensation. Therefore, an immediate CT angiogram is not the most appropriate next step for this specific patient, although it would be indicated if vascular compromise was suspected. The immediate steps focus on wound care and systemic prophylaxis.
Question 33
A 48-year-old construction worker sustains a Gustilo-Anderson Grade II open tibial shaft fracture after a fall from scaffolding. There is no evidence of vascular injury. Based on the current consensus and the LEAP study findings, what is the most appropriate timing for surgical debridement and stabilization?
Explanation
Correct Answer: B
The case explicitly states, 'The current consensus favours prudent early surgery within the first 24 hours. The old '6-hour rule' was based on animal experiments from the 1890s, and the well-known Lower Extremity Assessment Project (LEAP) study found no difference in infection rates when open fractures were managed within 6 hours or 24 hours.' It further recommends that, assuming no vascular injury, the injury is best managed during daytime hours with combined orthopaedic and plastic surgery input.
Option A: This reflects the outdated '6-hour rule' which has been superseded by evidence from the LEAP study.
Option C: Delaying surgery beyond 24 hours for an open fracture increases the risk of infection and is not recommended by current guidelines.
Option D: Open fractures require surgical debridement and stabilization to prevent infection and promote healing, not just observation for infection.
Option E: While urgent, the LEAP study and current guidelines allow for management within 24 hours, suggesting that it can be planned during daytime hours for optimal team availability, unless there's a vascular injury or heavy contamination (which are not present in this vignette).
Question 34
During surgical debridement of a Gustilo-Anderson Grade IIIa open tibial fracture, the orthopedic surgeon encounters muscle tissue that is dark, lacks contractility, and does not bleed when cut. Based on the principles outlined in the case, what is the appropriate management for this muscle tissue?
Explanation
Correct Answer: B
The case states, 'Non-viable skin should be excised, but any skin that is of dubious viability may be left for later assessment/debridement, unlike necrotic muscle which is implicated in infection and must be removed.' The description of the muscle tissue (dark, lacks contractility, no bleeding when cut) aligns with the '4 Cs' (colour, consistency, contractility, cut) used to assess muscle viability, indicating that it is necrotic. Necrotic muscle is a nidus for infection and must be removed during debridement.
Option A: While dubious skin viability might warrant re-assessment, necrotic muscle must be removed immediately due to its high association with infection.
Option C: Irrigation is part of the overall debridement, but it will not render necrotic muscle viable. A VAC device is for wound management after debridement, not a substitute for removing non-viable tissue.
Option D: Clinical assessment using the 4 Cs is the standard for determining muscle viability during debridement; a biopsy would be time-consuming and unnecessary.
Option E: Cauterization is used for hemostasis, not for managing necrotic tissue, and would not address the infection risk posed by non-viable muscle.
Question 35
A 28-year-old male sustains a high-energy open tibial fracture and undergoes surgical debridement and external fixation. Postoperatively, he remains obtunded due to associated head trauma. The nursing staff reports increasing pain medication requirements and a firm anterior compartment. To monitor for the most concerning postoperative complication in this patient, the orthopedic team decides to initiate continuous pressure monitoring. Which of the following findings would be diagnostic of early compartment syndrome in this context?

Explanation
Correct Answer: C
The case states, 'Patients who are unconscious or obtunded warrant continuous pressure monitoring with a slit catheter as used for arterial pressure monitoring. Continuous pressure monitoring of the anterior compartment is a useful adjunct to clinical diagnosis, whereby the ΔP is calculated by subtracting the intracompartmental pressure from the diastolic blood pressure. A persistently low ΔP, that is, <30 mmHg, is diagnostic of early compartment syndrome.'
Option A: An absolute intracompartmental pressure value (e.g., 40 mmHg) can be indicative, but it must be considered in relation to the patient's blood pressure. A single absolute value is less reliable than the ΔP, especially in hypotensive patients.
Option B: With a diastolic BP of 70 mmHg and an intracompartmental pressure of 35 mmHg, the ΔP would be 70 - 35 = 35 mmHg. This value is not less than 30 mmHg, so it would not be diagnostic of early compartment syndrome according to the provided criteria.
Option D: A MAP of 65 mmHg is a general indicator of adequate perfusion but does not directly diagnose compartment syndrome. The critical value is the ΔP.
Option E: An increase, not a decrease, in pain medication requirements would be a clinical sign of worsening compartment syndrome, although this patient is obtunded, making clinical assessment difficult.
Question 36
A 55-year-old farmer sustains an open tibial fracture after being run over by a tractor. The wound is heavily contaminated with farmyard matter, and there is extensive soft tissue loss with exposed bone and periosteal stripping, but no arterial injury requiring repair. Based on the Gustilo and Anderson classification system, how would this injury be classified?

Explanation
Correct Answer: D
The case provides a clear definition for Gustilo-Anderson Grade IIIb: 'An open fracture with extensive soft tissue loss and periosteal stripping'. Additionally, it states that 'Heavy contamination' and 'Farmyard contamination' automatically classify an injury as Grade III. Combining these factors, the presence of farmyard contamination (automatic Grade III) and extensive soft tissue loss with periosteal stripping (specific to IIIb) leads to a classification of IIIb. The absence of an arterial injury requiring repair rules out IIIc.
Option A: Grade I is for clean wounds <1cm.
Option B: Grade II is for wounds >1cm without extensive soft tissue damage or periosteal stripping.
Option C: Grade IIIa is for extensive soft tissue damage but adequate soft tissue coverage. This patient has extensive soft tissue loss and periosteal stripping, which implies inadequate coverage.
Option E: Grade IIIc is specifically for an associated arterial injury requiring repair, which is explicitly stated as absent in the vignette.
Question 37
Following thorough debridement of a Gustilo-Anderson Grade IIIb open tibial fracture, the wound bed reveals exposed bare bone and tendons without paratenon. According to the case discussion on soft tissue coverage, which of the following reconstructive options would be inappropriate for immediate application to this wound?
Explanation
Correct Answer: A
The case explicitly states: 'Bare bone, exposed blood vessels, nerves and tendons (without paratenon) all are harmed by desiccation and do not support granulation tissues and STSG. These tissues should not be left exposed, and should be kept moist with appropriate dressings prior to definitive cover.' Therefore, a split-thickness skin graft (STSG) would be inappropriate for a wound with exposed bare bone and tendons without paratenon.
Options B, C, D, E: Rotational muscle flaps (Gastrocnemius, Soleus) and various free flaps (including fasciocutaneous flaps like the sural artery flap) are all options on the reconstructive ladder designed to provide vascularized soft tissue coverage for complex defects involving exposed bone, vessels, nerves, or tendons, which cannot be covered by STSG.
Question 38
A 22-year-old motorcyclist sustains a Gustilo-Anderson Grade IIIb open fracture of the middle third of the tibia. After initial debridement and stabilization with an external fixator, the plastic surgery team is consulted for definitive soft tissue coverage. Based on the reconstructive options discussed in the case, which flap is most appropriate for this specific defect location?

Explanation
Correct Answer: D
The case provides specific guidance for flap options based on the location of the tibial defect: 'Middle third tibial defect - Soleus rotational flap'.
Option A: A Gastrocnemius rotational flap is indicated for proximal third tibial defects.
Option B: A Latissimus dorsi free flap is typically used for large defects, not specifically for a middle third tibial defect when a local option is available.
Option C: A Radial forearm free flap is indicated for smaller defects, but the soleus flap is a more direct and often preferred option for middle third tibial defects.
Option E: A split-thickness skin graft (STSG) is inappropriate for a Grade IIIb fracture with extensive soft tissue loss and exposed bone, as STSG requires a healthy, vascularized wound bed capable of granulation, which is typically not present in such severe injuries.
Question 39
A resident is presenting a case of a Gustilo-Anderson Grade IIIb open tibial fracture. During the discussion, an attending surgeon challenges the resident on the precise definition of a Grade IIIb injury, specifically regarding the necessity of a flap for classification. Based on the historical context and clarification provided in the case, which statement accurately reflects the definition of a Gustilo-Anderson Grade IIIb open fracture?
Explanation
Correct Answer: D
The case specifically addresses the confusion surrounding the IIIb subtype. It states: 'Type IIIb is described in the previous table and the need for a flap is not part of the classification system.' The definition provided in the table for IIIb is 'An open fracture with extensive soft tissue loss and periosteal stripping.' While Gustilo himself noted that IIIb fractures often need full-thickness soft-tissue coverage, Brumback and Jones clarified that this criterion was not part of the definition of the IIIb subtype published in 1984.
Option A: While Grade III fractures are often high-energy and contaminated, the specific wound size and contamination level are not the sole defining factors for IIIb.
Option B: This describes a Grade IIIa fracture (extensive soft tissue damage but adequate soft tissue coverage), not IIIb, and the need for a flap is not part of the definition for any grade.
Option C: This is incorrect because, as clarified in the case, the need for a flap is not part of the classification definition of IIIb, even though such injuries typically require flaps for coverage.
Option E: This describes a Grade IIIc fracture.
Question 40
A 40-year-old male presents with a Gustilo-Anderson Grade II open tibial fracture after a fall. He has no known allergies. Following initial wound care and splinting in the emergency department, what is the most appropriate antibiotic regimen and duration, according to the BOAST guidelines mentioned in the case?
Explanation
Correct Answer: B
The case states, 'I would give antibiotics as per local microbiology protocols (the BOAST guidelines suggest cefuroxime 1.5 g IV)... Antibiotics would be given at the time of surgery and continued for 72 hours or until wound closure, whichever occurs soonest.' This directly matches option B.
Option A: Oral antibiotics are generally insufficient for open fractures, which require intravenous administration for adequate tissue penetration and systemic effect.
Option C: While vancomycin and gentamicin might be used for specific types of contamination (e.g., farmyard, marine) or in cases of penicillin allergy, cefuroxime is the general recommendation for Grade I/II open fractures as per BOAST guidelines mentioned in the text. The duration of 7 days is also longer than the recommended 72 hours or until wound closure.
Option D: Penicillin G is not the broad-spectrum antibiotic of choice for open fractures; cefuroxime (a second-generation cephalosporin) provides broader coverage against common pathogens in open fractures.
Option E: Antibiotic prophylaxis is crucial for all open fractures, regardless of the timing of debridement, to reduce the risk of infection.
Question 41
A 35-year-old male undergoes surgical debridement and internal fixation for a high-energy open tibial fracture. Twenty-four hours post-operatively, he develops severe, unremitting pain in the affected leg, disproportionate to the injury, and has increasing paresthesias in the foot. Clinical examination reveals a tense and firm anterior compartment. Despite the open nature of the fracture, the orthopedic team suspects acute compartment syndrome. What is the definitive treatment for this condition?
Explanation
Correct Answer: C
The case directly addresses the treatment of compartment syndrome: 'I would perform an emergency two-incision, four-compartment fasciotomy of the lower leg.' This is the definitive surgical treatment for acute compartment syndrome.
Option A: Elevation and observation are contraindicated in suspected compartment syndrome as they delay definitive treatment and can worsen outcomes. Elevation can decrease arterial inflow, further compromising perfusion.
Option B: Mannitol is a diuretic that can reduce generalized edema but is not effective in reversing the high compartmental pressures seen in acute compartment syndrome, which requires surgical decompression.
Option D: Applying a cast would further restrict the limb and exacerbate the compartment syndrome by increasing external pressure, making it highly detrimental.
Option E: While repeat debridement might be necessary for the open fracture wound itself, it does not address the underlying pathology of compartment syndrome, which is increased pressure within the fascial compartments. A fasciotomy is required to relieve this pressure.
Question 42
A 16-year-old male presents with anterior sternoclavicular (SC) joint deformity after a wrestling match. Radiographs demonstrate medial clavicular swelling and apparent anterior subluxation. What is the most common actual pathology in this age group presenting with these findings?
Explanation
Question 43
During open reduction of a traumatic, irreducible posterior sternoclavicular dislocation, the surgeon dissects posterior to the medial clavicle. Which of the following vascular structures is at greatest risk of iatrogenic injury directly posterior to the SC joint?
Explanation
Question 44
A 25-year-old cyclist sustains a midshaft clavicle fracture. Which of the following is considered an absolute indication for operative fixation?
Explanation
Question 45
A 45-year-old man sustains a completely displaced Type II distal clavicle fracture (Neer classification). What is the primary deforming force responsible for the displacement of the proximal fragment?
Explanation
Question 46
A 35-year-old male sustains a high-energy trauma resulting in a 'floating shoulder.' What defines the true anatomic basis of this injury pattern?
Explanation
Question 47
A 22-year-old motorcyclist presents with severe lateral displacement of the scapula on a chest radiograph and massive shoulder swelling (scapulothoracic dissociation). Which vascular structure is most commonly injured in this specific severe trauma pattern?
Explanation
Question 48
A 24-year-old male presents with recurrent anterior shoulder instability. MRI arthrogram reveals an avulsion of the anterior labrum along with the anterior band of the inferior glenohumeral ligament (IGHL) from the glenoid rim. This lesion is formally known as:
Explanation
Question 49
During arthroscopic stabilization for recurrent anterior shoulder instability, the surgeon notes an intact anterior labrum but an avulsion of the inferior glenohumeral ligament from its humeral insertion. What is the appropriate terminology for this lesion?
Explanation
Question 50
In a severe 4-part proximal humerus fracture, what is the primary arterial supply to the humeral head that is typically disrupted, leading to a high risk of avascular necrosis?
Explanation
Question 51
A 28-year-old male falls onto his adducted shoulder, sustaining an acromioclavicular (AC) joint injury. Radiographs show superior displacement of the clavicle by 150% of the acromion width, with severe disruption of the deltotrapezial fascia. Which Rockwood classification type is this?
Explanation
Question 52
A 19-year-old male with a traumatic posterior sternoclavicular dislocation is undergoing closed reduction in the operating room. What is the recommended patient positioning and manipulative maneuver to facilitate this reduction?
Explanation
Question 53
To better visualize the sternoclavicular joint and assess anterior versus posterior displacement in a trauma patient, a 'serendipity view' is ordered. What is the proper X-ray beam angulation for this specialized view?
Explanation
Question 54
A 42-year-old polytrauma patient is diagnosed with a displaced scapular body and neck fracture. Which of the following measurements is considered a strong relative indication for open reduction and internal fixation (ORIF) to restore shoulder biomechanics?
Explanation
Question 55
Which of the following specific combinations of injuries constitutes the classic 'terrible triad of the shoulder'?
Explanation
Question 56
A 30-year-old male presents with a closed spiral fracture of the distal third of the humeral shaft (Holstein-Lewis) and an isolated, dense radial nerve palsy present immediately after the injury. What is the most appropriate initial management?
Explanation
Question 57
A 33-year-old weightlifter feels a 'pop' in his anterior chest wall during a heavy bench press. Exam reveals a loss of the anterior axillary fold and weakness in internal rotation. Which specific portion of the pectoralis major is most commonly ruptured in this scenario?
Explanation
Question 58
Which of the following is considered the most significant radiographic risk factor for the development of a nonunion in a midshaft clavicle fracture treated non-operatively?
Explanation
Question 59
A 45-year-old intravenous drug user presents with swelling, erythema, and severe pain over the sternoclavicular joint. Aspiration yields purulent fluid. What is the most common organism responsible for septic arthritis of the SC joint in this patient population?
Explanation
Question 60
When performing an open distal clavicle excision (Mumford procedure), the surgeon must be careful not to resect too much bone to prevent iatrogenic acromioclavicular instability. What is the maximum amount of distal clavicle that should safely be resected?
Explanation
Question 61
A 24-year-old motorcyclist sustains a severe traction injury to his right shoulder, presenting with a flail, insensate arm. Physical examination reveals right-sided ptosis, miosis, and anhidrosis. This specific constellation of clinical findings indicates an injury at which level?
Explanation
Question 62
What is the primary anatomical restraint to both anterior and posterior translation of the sternoclavicular joint?
Explanation
Question 63
An 18-year-old male sustains a posterior medial clavicle displacement following a rugby tackle. Magnetic resonance imaging reveals that the medial epiphysis remains articulated with the sternum while the metaphysis is displaced posteriorly. In a hemodynamically stable patient with no neurovascular compromise, what is the most appropriate initial management?
Explanation
Question 64
A 'serendipity' radiographic view is requested to evaluate a patient for a suspected sternoclavicular joint dislocation. What is the proper positioning of the X-ray beam to obtain this image?
Explanation
Question 65
A 24-year-old male presents with a confirmed anterior sternoclavicular joint dislocation. The overlying skin is intact. What is the most appropriate definitive management for this injury?
Explanation
Question 66
Which of the following clinical findings is considered an absolute indication for operative fixation of an acute midshaft clavicle fracture?
Explanation
Question 67
In the setting of a traumatic posterior sternoclavicular dislocation, which of the following vascular structures is most commonly at risk for compression or direct injury?
Explanation
Question 68
What is the primary stabilizing function of the costoclavicular (rhomboid) ligament in the shoulder girdle?
Explanation
Question 69
A 45-year-old male sustains a high-energy traction injury to his right arm. Physical examination reveals massive swelling and marked lateral displacement of the scapula. An angiogram demonstrates a right subclavian artery occlusion. What concomitant neurologic injury is most frequently associated with this diagnosis?
Explanation
Question 70
A 30-year-old cyclist falls onto the point of his shoulder and is diagnosed with a Rockwood Type III acromioclavicular (AC) joint separation. Which of the following accurately describes the status of the supporting ligaments in this injury pattern?
Explanation
Question 71
During open reduction and internal fixation of a comminuted midshaft clavicle fracture, the surgeon drills from anterior to posterior to place a lag screw. Which neurovascular structure is most at risk from over-penetration by the drill bit?
Explanation
Question 72
Which of the following patients with a midshaft clavicle fracture possesses the highest risk of nonunion if managed nonoperatively?
Explanation
Question 73
A 28-year-old male is undergoing ligamentous reconstruction for chronic posterior sternoclavicular instability. The surgeon plans a figure-of-8 reconstruction. Between which two osseous structures is the tendon graft typically routed?
Explanation
Question 74
What is the most common indirect mechanism of injury leading to a posterior sternoclavicular joint dislocation?
Explanation
Question 75
A 34-year-old male sustains a Neer Type IIB distal clavicle fracture. Why is operative fixation strongly considered for this specific fracture pattern?
Explanation
Question 76
A 50-year-old female presents with a closed, isolated extra-articular scapular body fracture after a high-speed motor vehicle crash. Which of the following parameters represents a generally accepted indication for operative fixation?
Explanation
Question 77
A 22-year-old patient with an acute posterior sternoclavicular dislocation is undergoing closed reduction under general anesthesia. Traction is applied to the arm in abduction and extension, but the medial clavicle fails to reduce. What is the most appropriate next step in the reduction maneuver?
Explanation
Question 78
When evaluating a standard anteroposterior chest radiograph for a suspected scapulothoracic dissociation, which finding is most diagnostic of this condition?
Explanation
Question 79
Which of the following statements regarding the normal anatomy and development of the sternoclavicular (SC) joint is accurate?
Explanation
Question 80
Which of the following ligaments provides the primary restraint to both anterior and posterior translation of the sternoclavicular (SC) joint?
Explanation
Question 81
A 16-year-old male presents to the emergency department with severe pain and a posterior deformity at the medial aspect of his clavicle after a direct blow during a football game. Imaging suggests a posterior displacement of the medial clavicle. What is the most likely true anatomical nature of this injury?
Explanation
Question 82
When obtaining a "serendipity" radiographic view to evaluate a suspected sternoclavicular joint injury, how should the x-ray beam be directed?
Explanation
Question 83
A 22-year-old male sustains an acute, traumatic anterior sternoclavicular joint dislocation. There is no evidence of neurovascular compromise. What is the most appropriate initial management?
Explanation
Question 84
During the closed reduction of a posterior sternoclavicular joint dislocation in the operating room, which of the following logistical precautions is most critical?
Explanation
Question 85
Which specific vascular structure is located immediately posterior to the sternoclavicular joint and is at greatest risk of injury in a posterior sternoclavicular dislocation?
Explanation
Question 86
A 19-year-old gymnast presents with a long-standing history of spontaneous, painless anterior subluxation of her sternoclavicular joint when she raises her arm overhead. The joint reduces automatically when she lowers her arm. What is the recommended treatment?
Explanation
Question 87
A 45-year-old male presents with severe shoulder pain after a motorcycle accident. Radiographs reveal lateral displacement of the intact scapula relative to the thoracic spine, an intact clavicle, and significant soft tissue swelling. What devastating concomitant injury is highly associated with this pattern?
Explanation
Question 88
Which of the following clinical findings represents the earliest and most reliable sign of compartment syndrome in an alert patient sustaining a tibial plateau fracture?
Explanation
Question 89
When determining the need for fasciotomies in a patient with a closed tibial shaft fracture and suspected compartment syndrome, which pressure threshold is generally accepted as an absolute indication for surgery?
Explanation
Question 90
A 35-year-old trauma patient with an unstable pelvic ring injury requires the application of a pelvic binder to reduce pelvic volume and control hemorrhage. For maximum biomechanical effectiveness, over which anatomical landmark should the binder be centered?
Explanation
Question 91
A 28-year-old male sustains a midshaft clavicle fracture. Which of the following radiographic findings is most strongly associated with a higher risk of nonunion if treated non-operatively?
Explanation
Question 92
Which of the following describes the pathophysiology of a Neer Type II distal clavicle fracture, leading to its high nonunion rate?
Explanation
Question 93
A 25-year-old male sustains a gunshot wound to the thigh. Radiographs confirm a comminuted distal femur fracture with the bullet lodged entirely within the knee joint capsule. What is the most appropriate management regarding the retained bullet?
Explanation
Question 94
A 40-year-old male with multiple long bone fractures becomes acutely confused, hypoxic, and develops a petechial rash over his axilla and chest 48 hours after admission. What is the most likely diagnosis?
Explanation
Question 95
Which of the following injuries is classified as a Gustilo-Anderson Type IIIA open fracture?
Explanation
Question 96
In the setting of a severe "mangled" lower extremity, which of the following is generally considered an absolute indication for primary amputation?
Explanation
Question 97
A patient requires surgical stabilization for a chronic, painful posterior sternoclavicular joint dislocation that cannot be reduced closed. If a figure-of-eight ligament reconstruction is planned using a tendon graft, what structure is most typically used as the graft source?
Explanation
Question 98
A patient with flail chest and multiple displaced rib fractures is being evaluated by the orthopedic trauma service. According to current literature, what is the most widely accepted primary indication for surgical rib fixation (plating)?
Explanation
None
