Orthopaedic Board Review: Forearm & Wrist Fracture MCQs for ABOS Part I & AAOS OITE | Part 21579
Key Takeaway
This module provides 30 advanced multiple-choice questions for ABOS Part I and AAOS OITE exams, focusing on forearm and wrist fractures. It covers Galeazzi and distal radius fractures, surgical management, complications like compartment syndrome and DRUJ instability, and rehabilitation. Ideal for orthopaedic residents and surgeons preparing for board certification.
Orthopaedic Board Review: Forearm & Wrist Fracture MCQs for ABOS Part I & AAOS OITE | Part 21579
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old construction worker sustains a direct blow to his left forearm with obvious deformity and severe pain. On examination, there is a small puncture wound over the ulnar shaft. What is the most critical immediate next step in management after initial ATLS primary survey and limb exposure?

Explanation
Correct Answer: C
While all options are important, immediate assessment of neurovascular status distal to the injury (Option C) is paramount. Any compromise (e.g., absent pulses, severe paresthesias, motor weakness) warrants urgent intervention to prevent limb ischemia and permanent neurological damage. This assessment dictates the immediate urgency of further steps. Identifying the puncture wound implies an open fracture, for which IV antibiotics and tetanus prophylaxis (Option B) are crucial to prevent infection, but limb viability takes precedence. Radiographs (Option A) are necessary to characterize the fracture but follow neurovascular assessment. Immobilization (Option D) provides comfort and prevents further injury but is not the most critical immediate step for limb salvage. Measuring compartment pressures (Option E) is indicated if acute compartment syndrome is suspected, which is a secondary assessment after initial neurovascular evaluation and often triggered by the findings of that initial assessment.
Question 2
A 45-year-old male with a mid-diaphyseal both bones forearm fracture undergoes open reduction and internal fixation (ORIF) with 3.5mm dynamic compression plates. What is the generally accepted minimum number of cortices that should be engaged by screws proximally and distally to achieve adequate stability for these fractures?

Explanation
Correct Answer: C
For adequate stability in plating diaphyseal forearm fractures, the general consensus and biomechanical studies recommend achieving at least 8 cortices (4 screws) proximally and 8 cortices (4 screws) distally. This provides sufficient screw-bone purchase to resist bending, rotational, and axial forces, which are critical for primary bone healing and preventing fixation failure, non-union, or malunion. Fewer than 8 cortices on either side of the fracture can lead to higher rates of fixation failure, screw pullout, and non-union, especially given the high torsional and bending stresses the forearm experiences during daily activities.
Question 3
During surgical exposure for a mid-diaphyseal radial shaft fracture via the Henry (anterior) approach, which neurovascular structure is most directly at risk and requires careful identification and protection?

Explanation
Correct Answer: C
The Henry (anterior) approach for the radial shaft involves dissecting between the brachioradialis and the flexor carpi radialis (or pronator teres, depending on the level). The radial artery and the superficial radial nerve (a sensory branch of the radial nerve) run immediately deep to the brachioradialis muscle. They are thus directly in the surgical field and are at high risk of injury if not carefully identified, mobilized, and retracted, typically ulnarward. The posterior interosseous nerve (PIN) is at risk with dorsal approaches to the radius. The ulnar and median nerves are located more medially in the forearm and are generally not directly in the field of the Henry approach for a mid-diaphyseal radial fracture. The anterior interosseous nerve (AIN) is a deeper structure, lying on the interosseous membrane, and while it can be at risk with very deep or extensive dissection, the radial artery and superficial radial nerve are more superficially and directly vulnerable.
Question 4
Which of the following is considered the most significant factor contributing to rotational malunion after non-operative management of a both bones forearm fracture in an adult?

Explanation
Correct Answer: E
Lack of anatomical reduction (Option E) is the most significant factor for rotational malunion in adult forearm fractures. The forearm's pronation and supination are complex, involving precise interaction between the radius and ulna and the interosseous membrane. Even small degrees of angular or rotational malreduction (typically >10-15 degrees) can significantly impair forearm rotation and lead to substantial functional deficits. While initial displacement (Option B) makes anatomical reduction more challenging, and inadequate immobilization (Option C) can lead to loss of reduction, the final state of malreduction is the direct cause of the malunion. Violation of the interosseous membrane during injury (Option D) is a factor contributing to instability and difficulty achieving reduction, but rotational malunion specifically links to the final achieved alignment, or lack thereof. Age (Option A) impacts remodeling potential, but in adults, remodeling is minimal, making anatomical reduction paramount.
Question 5
A 7-year-old presents with a completely displaced mid-diaphyseal both bones forearm fracture. After an unsuccessful attempt at closed reduction and casting, what is the most appropriate next step in management?

Explanation
Correct Answer: C
For unstable and completely displaced diaphyseal forearm fractures in children where closed reduction fails, flexible intramedullary nailing (FIN) is generally the treatment of choice (Option C). FIN provides stable fixation, allows for early motion, and importantly, preserves the growth plates, which is a major concern in pediatric fractures. Plating (Option B) is generally reserved for older adolescents (near skeletal maturity) or specific complex cases in children due to potential issues with growth plate injury, larger dissection, and the need for hardware removal. Repeating closed reduction (Option A) without a plan for definitive fixation if it fails again is not the most appropriate 'next step' after an initial failure. External fixation (Option D) is typically reserved for open fractures, highly comminuted fractures, or situations with significant soft tissue injury. Observation (Option E) is inappropriate for a completely displaced fracture after failed reduction, as remodeling potential is limited for rotational or significant angular deformities that are not adequately reduced.
Question 6
Which of the following describes the typical displacement of the proximal radial fracture fragment in a mid-diaphyseal radial fracture that is proximal to the insertion of the pronator teres?

Explanation
Correct Answer: C
If the radial shaft fracture is proximal to the insertion of the pronator teres (which inserts at the mid-shaft), the powerful supinator muscles (biceps brachii and supinator) act unopposed on the proximal fragment, leading to a supinated position. The distal fragment, still attached to the pronator teres and pronator quadratus, tends to pronate. This creates a significant rotational malalignment that must be corrected during reduction and fixation to avoid loss of forearm rotation. The proximal fragment is also often radially translated due to muscle pull. Therefore, the proximal fragment is typically supinated and radially translated (Option C).
Question 7
A 35-year-old male sustains an isolated, closed, mid-shaft both bones forearm fracture. He undergoes ORIF with plates and screws. Four hours post-operatively, he complains of severe pain disproportionate to the injury, increasing with passive stretch of fingers, and develops paresthesias in the median nerve distribution. His distal pulses are palpable. What is the most appropriate next step?

Explanation
Correct Answer: D
The patient's symptoms (severe pain disproportionate to injury, pain with passive stretch of the fingers, paresthesias in the median nerve distribution, and palpable pulses) are classic signs of acute compartment syndrome. While removing a tight dressing (Option C) might alleviate external compression in some cases, the most appropriate next step in a suspected acute compartment syndrome, especially post-operatively, is to urgently measure forearm compartment pressures (Option D). This is the definitive diagnostic test. Reassurance (Option A) and increasing analgesia (Option A) are dangerous as they mask symptoms and delay critical intervention. A CT scan (Option B) is not indicated for diagnosing compartment syndrome. Elevation (Option E) can reduce blood flow and worsen ischemia in an already compromised limb with compartment syndrome.
Question 8
Which of the following is a recognized long-term complication unique to both bones forearm fractures, particularly challenging for restoring full function?

Explanation
Correct Answer: D
Heterotopic ossification leading to synostosis (Option D) is a unique and particularly debilitating complication of both bones forearm fractures, especially after open reduction and internal fixation. It involves abnormal bone formation between the radius and ulna, fusing the two bones and severely limiting or completely eliminating pronation and supination. This profoundly impacts the unique rotational function of the forearm. While non-union (Option A), infection (Option B), and refracture (Option E) are general complications of fractures, and post-traumatic arthritis (Option C) can occur, synostosis is specific to the interosseous space of the forearm and directly impairs its most critical function.
Question 9
When assessing acceptable reduction criteria for adult diaphyseal both bones forearm fractures, what is the maximum acceptable rotational malalignment to avoid significant functional impairment?

Explanation
Correct Answer: B
For adult diaphyseal forearm fractures, the widely accepted maximum rotational malalignment to avoid significant functional impairment is generally less than 10 degrees (Option B). While some literature suggests up to 15 degrees may be tolerated in specific circumstances, aiming for less than 10 degrees is crucial to preserve the complex coupled motion of forearm pronation/supination. Rotational malalignment is poorly tolerated functionally because even small degrees can lead to a significant loss of forearm rotation, impacting daily activities. Other acceptable criteria typically include less than 10 degrees of angulation and less than 5mm of shortening.
Question 10
What is the primary biomechanical advantage of fixing both bones in a diaphyseal forearm fracture with separate plates over a single intramedullary nail for both?

Explanation
Correct Answer: C
Plating both bones with separate plates provides superior rotational stability (Option C) compared to attempting to nail both bones. Plates applied to the tension and compression sides of the bone effectively neutralize bending and torsional forces, which are critical in the forearm due to its unique rotational function. Intramedullary nails primarily resist bending and axial forces but provide less rotational stability, especially in the forearm where the two bones must rotate relative to each other. This lack of rotational control with intramedullary nailing in adults can lead to higher rates of rotational malunion. Less surgical exposure (Option A) is generally not true for plating two bones compared to nailing. Risk of infection (Option B) and hardware removal timing (Option D) are not primary biomechanical advantages. Remodeling potential (Option E) is mainly relevant in children and not a biomechanical advantage of fixation type in adults.
Question 11
A 65-year-old female sustains a distal radius fracture with significant comminution, articular involvement spanning both the scaphoid and lunate fossae, and severe metaphyseal comminution, extending into the diaphysis. According to the Fernandez classification, how would this fracture typically be categorized?

Explanation
Correct Answer: E
The Fernandez classification categorizes distal radius fractures based on the mechanism of injury and fracture morphology. Type I is bending (meta-epiphyseal), Type II is shearing (Barton, Hutchinson), Type III is compression (die-punch), Type IV is avulsion (ligament), and Type V is combined or high-energy fractures with extensive comminution and bone loss. Significant comminution, articular involvement of both fossae, and extension into the diaphysis (often implying severe metaphyseal involvement or bone loss) points strongly towards a high-energy injury, characteristic of a Type V Fernandez fracture.
Question 12
Which of the following radiographic findings in a distal radius fracture is LEAST indicative of potential instability requiring surgical intervention following an initially successful closed reduction?

Explanation
Correct Answer: D
Instability criteria often guide the decision for surgical fixation following a distal radius fracture. Common indicators of instability include initial dorsal angulation greater than 20 degrees, radial shortening exceeding 3mm, severe metaphyseal comminution, and particularly, intra-articular step-off or gap greater than 1-2mm. While an ulnar styloid fracture is frequently associated with distal radius fractures and may suggest a TFCC injury, its presence alone is not a direct criterion for radial fracture instability or a primary indication for surgical intervention on the radius, assuming other parameters are acceptable. It might influence DRUJ stability, but not necessarily the stability of the radial reduction itself.
Question 13
During a standard volar approach (Henry approach) to the distal radius for plate fixation, which structure is primarily released or retracted radially to access the volar aspect of the radius?

Explanation
Correct Answer: D
The Henry approach for volar plating of the distal radius involves an incision between the Flexor Carpi Radialis (FCR) and the Radial Artery. The FCR tendon is retracted ulnarly, and the radial artery and brachioradialis are retracted radially. The critical step to expose the volar aspect of the distal radius is the subperiosteal elevation and L-shaped release of the Pronator Quadratus muscle from its radial and distal attachments, which is then reflected ulnarly. The median nerve lies more ulnarly, and the FPL tendon is in the deep flexor compartment and typically not the primary muscle reflected for direct radial access.
Question 14
A 70-year-old patient undergoes open reduction internal fixation with a dorsal plate for a comminuted distal radius fracture. Six months post-operatively, she presents with difficulty extending her thumb IP joint and a positive Finkelstein's test. Assuming the Finkelstein's test is a misdiagnosis or secondary finding, which tendon is most likely to have ruptured?

Explanation
Correct Answer: C
Difficulty extending the thumb IP joint (interphalangeal joint) is the hallmark sign of Extensor Pollicis Longus (EPL) rupture. EPL rupture is a known complication of distal radius fractures, particularly after dorsal plating, due to attrition over rough bone edges, plate prominence, or direct plate impingement. It can also occur post-closed reduction due to attrition over a dorsal bony prominence or as part of a delayed presentation (e.g., following a Colles' fracture). The Finkelstein's test is for De Quervain's tenosynovitis (APL and EPB), which is not directly related to EPL rupture, hence the assumption of it being a secondary finding.
Question 15
When measuring volar tilt on a true lateral radiograph of the wrist, a normal range is considered to be:

Explanation
Correct Answer: C
On a true lateral radiograph of the wrist, the distal articular surface of the radius normally exhibits a volar tilt. The accepted normal range is typically 10 to 15 degrees of volar tilt. A neutral or dorsal tilt is considered abnormal and is a characteristic deformity of a Colles' fracture.
Question 16
Which of the following anatomical structures is considered the primary static stabilizer of the distal radioulnar joint (DRUJ)?

Explanation
Correct Answer: C
The Triangular Fibrocartilage Complex (TFCC) is the primary static stabilizer of the DRUJ. It is a complex structure comprising the articular disc, dorsal and volar radioulnar ligaments, and the meniscal homologue. While the dorsal and volar radioulnar ligaments within the TFCC are key components, the TFCC as a whole unit provides the most significant static stability. The interosseous membrane provides some longitudinal stability to the forearm, and the Pronator Quadratus offers dynamic stability. The ECU tendon sheath is adjacent but not a primary stabilizer.
Question 17
A 40-year-old male presents with persistent wrist pain and decreased range of motion 1 year after non-operative management of a distal radius fracture. Radiographs show a dorsal tilt of 25 degrees, radial shortening of 5mm, and a 3mm intra-articular step-off. According to common malunion criteria, which of these findings is *least* acceptable for good functional outcomes in a younger, active patient?

Explanation
Correct Answer: C
While all listed findings represent aspects of malunion, an intra-articular step-off of 3mm is widely considered the most critical predictor of poor long-term outcomes, particularly post-traumatic arthritis, especially in an active younger patient. Even 1-2mm of intra-articular incongruity is often deemed unacceptable. Dorsal tilt >10-15 degrees and radial shortening >2-3mm are also significant, and ulnar positive variance is directly related to radial shortening. However, articular step-off directly compromises joint congruity and leads to accelerated degenerative changes, making it the least acceptable from a functional prognosis standpoint.
Question 18
A 55-year-old female develops symptoms consistent with Complex Regional Pain Syndrome (CRPS) Type I following a distal radius fracture treated non-operatively. Her symptoms include severe pain out of proportion to injury, allodynia, swelling, and trophic changes. Which of the following is considered the MOST critical early intervention in managing CRPS?

Explanation
Correct Answer: C
Early recognition and aggressive physical and occupational therapy focused on pain-free range of motion, desensitization, and functional use are paramount in managing CRPS. While medications (gabapentin, tricyclic antidepressants) and interventional treatments (sympathetic blocks) have a role, they are often adjuncts. Steroids may be used, but not as the initial most critical step. Spinal cord stimulators are reserved for refractory cases. The key to preventing progression and improving outcomes is early, consistent, and active rehabilitation.
Question 19
A 30-year-old active male sustains a distal radius fracture with a 4mm intra-articular step-off, 5 degrees dorsal tilt, and 1mm radial shortening. Which of these parameters ALONE typically warrants surgical intervention for definitive management?

Explanation
Correct Answer: A
While age and activity level influence treatment decisions, the specific fracture characteristic of a 4mm intra-articular step-off is a very strong, if not absolute, indication for surgical management, regardless of other parameters. Even 1-2mm of articular incongruity is often considered unacceptable, particularly in a younger, active individual, due to the high risk of post-traumatic arthritis. The dorsal tilt and radial shortening mentioned are relatively minor compared to the articular step-off.
Question 20
Following reduction and casting of a distal radius fracture, a patient complains of persistent ulnar-sided wrist pain, particularly with pronation/supination and grasping. Tenderness is noted just distal to the ulnar head. Which of the following tests would be most appropriate to further evaluate for a potential Triangular Fibrocartilage Complex (TFCC) injury?

Explanation
Correct Answer: E
Ulnar-sided wrist pain after a distal radius fracture, especially with DRUJ movements, strongly suggests a TFCC injury. The TFCC compression test (axial load with ulnar deviation and rotation) is a specific provocative test for TFCC tears, eliciting pain and sometimes a click. The Scaphoid Shift (Watson) test assesses scapholunate instability. Finkelstein's test is for De Quervain's tenosynovitis. The Grind test is for carpometacarpal arthritis. The Piano Key test assesses DRUJ stability (dorsal/volar translation of the ulnar head).
Question 21
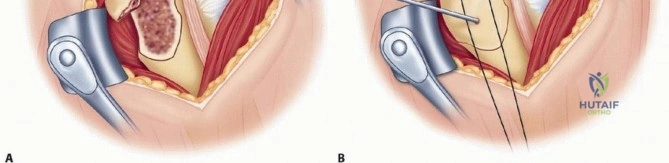
A 42-year-old male presents to the emergency department after falling onto his outstretched left hand with his forearm in pronation. He complains of severe pain and deformity in his distal forearm. Physical examination reveals a shortened, radially deviated forearm with a prominent ulnar head dorsally. Initial radiographs are shown below. Which of the following is the most appropriate initial management step?

Explanation
Correct Answer: B
The patient's presentation (fall on outstretched hand in pronation, shortened/radially deviated forearm, prominent dorsal ulnar head) and the described radiographs are classic for a Galeazzi fracture-dislocation (fracture of the distal third of the radial diaphysis with associated distal radioulnar joint (DRUJ) disruption). In adults, Galeazzi fractures are inherently unstable due to the loss of radial support and muscle forces (brachioradialis, pronator quadratus) acting on the fragments, as well as the associated DRUJ injury. Non-operative management in adults is associated with unacceptably high rates of malunion, nonunion, and persistent DRUJ instability (often 50-100%). Therefore, the definitive management for an adult Galeazzi fracture is immediate open reduction and internal fixation (ORIF) of the radial shaft to restore anatomical length, rotation, and alignment. This is followed by a careful assessment of DRUJ stability, which often reduces indirectly once radial anatomy is restored. If the DRUJ remains unstable, direct stabilization (e.g., temporary K-wire fixation) is performed.
Option A is incorrect because closed reduction and casting are rarely successful in adults due to the inherent instability and high risk of malunion/redislocation. Option C is incorrect as delayed surgical consultation for an adult Galeazzi fracture is inappropriate; definitive fixation is required. Option D is incorrect because pinning the DRUJ without addressing the radial shaft fracture will not provide stability or restore radial length. Option E is incorrect as it prioritizes DRUJ reduction over the primary radial fracture, and attempting to reduce the DRUJ without stabilizing the radius is futile and will not lead to a stable construct.
Question 22
During open reduction and internal fixation (ORIF) of a Galeazzi fracture via a volar (Henry) approach to the distal radius, which of the following anatomical structures is most susceptible to iatrogenic injury?
Explanation
Correct Answer: D
The volar (Henry) approach to the distal radius is commonly used for Galeazzi fractures. During this approach, the interval between the brachioradialis and the flexor carpi radialis is utilized. The anterior interosseous nerve (AIN), a motor branch of the median nerve, is the most vulnerable neurovascular structure. It courses on the interosseous membrane, deep to the flexor digitorum profundus and lateral to the flexor pollicis longus. Injury can occur during aggressive retraction, stripping of the pronator quadratus, or direct trauma during plate application. An AIN injury results in the inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joints of the index and middle fingers (loss of FPL and FDP to index/middle), and loss of pronator quadratus function.
Option A (Ulnar nerve) is located on the ulnar side of the forearm and is not typically at risk with a volar radial approach. Option B (Posterior interosseous nerve) is at risk with a dorsal (Thompson) approach to the radius, not the volar approach. Option C (Superficial radial nerve) is a sensory nerve located more superficially and radially, usually avoided with careful skin incision and dissection. Option E (Radial artery) is located more radially and can be protected with careful dissection, but the AIN is more intimately associated with the deeper dissection plane.
Question 23
Following successful open reduction and internal fixation of the radial shaft in an adult Galeazzi fracture, the surgeon performs an intraoperative assessment of the distal radioulnar joint (DRUJ). Despite anatomical reduction and stable plating of the radius, the DRUJ remains unstable with excessive dorsal translation of the ulna during forearm rotation. What is the most appropriate next step?

Explanation
Correct Answer: C
The primary goal of Galeazzi fracture management is to restore anatomical radial length, rotation, and alignment, which often indirectly reduces and stabilizes the DRUJ. However, if the DRUJ remains unstable after stable radial fixation, direct intervention is necessary. The most appropriate next step is to explore the DRUJ for any incarcerated soft tissues (such as the pronator quadratus muscle, extensor carpi ulnaris (ECU) tendon, or capsule) that might be preventing full reduction. After ensuring no interposition, the DRUJ should be stabilized with temporary K-wires. For dorsal instability, the forearm is typically placed in full supination to tighten the volar radioulnar ligaments, and K-wires are inserted from the dorsal ulna into the radius. These pins are usually left in place for 4-6 weeks to allow capsuloligamentous healing.
Option A is incorrect because persistent DRUJ instability after radial fixation will lead to chronic pain, limited forearm rotation, and poor functional outcomes. Option B (ulnar shortening osteotomy) and Option E (Darrach procedure) are salvage procedures for chronic DRUJ pathology or malunion, not acute management for persistent instability after primary fixation. Option D is incorrect as a second-stage reconstruction is not the initial approach for acute instability; it should be addressed during the primary surgery.
Question 24
A 58-year-old patient presents 6 months after open reduction and internal fixation of a Galeazzi fracture. She complains of chronic pain on the ulnar side of her wrist, especially with pronation and ulnar deviation, and significantly limited forearm rotation. Radiographs show a healed radial shaft fracture but with 8mm of residual radial shortening and a positive ulnar variance. Which of the following is the most likely long-term complication causing her symptoms?

Explanation
Correct Answer: C
Residual radial shortening after a Galeazzi fracture leads to a positive ulnar variance, meaning the ulna is relatively longer than the radius. This altered length relationship is a common and significant complication. It causes the distal ulna to impinge on the lunate and triquetrum, leading to ulnar impaction syndrome. This condition is characterized by chronic ulnar-sided wrist pain, particularly with pronation and ulnar deviation, and can progress to degenerative changes and arthritis of the DRUJ and ulnocarpal joint. The limited forearm rotation is a direct consequence of the altered DRUJ mechanics and potential arthritis.
Option A (Kienbock's disease) is associated with negative ulnar variance, not positive. Option B (Radial nerve palsy) is not a direct long-term consequence of radial shortening malunion. Option D (Flexor tendon rupture) is typically associated with hardware prominence or severe inflammatory conditions, not directly with positive ulnar variance. Option E (Carpal tunnel syndrome) is a median nerve compression neuropathy and, while possible, is not the most direct or common complication of this specific malunion pattern.
Question 25
A 9-year-old child sustains a fall and presents with a fracture of the distal radial diaphysis and associated dorsal dislocation of the distal ulna. Radiographs confirm a Galeazzi-type injury. Compared to the management of an adult with the same injury, what is the most common and often successful initial management approach for this child?

Explanation
Correct Answer: C
The management of Galeazzi-type injuries differs significantly between children and adults. In children, due to their greater remodeling potential, thicker periosteum, and more resilient ligaments, closed reduction of both the radial shaft fracture and the distal radioulnar joint (DRUJ) is often successful. Once reduced, the forearm is typically immobilized in a long arm cast with the forearm in full supination (or neutral position) to help maintain reduction of the DRUJ by tightening the volar radioulnar ligaments. ORIF (Option A) is generally reserved for unstable or irreducible cases in children. External fixation (Option B) is rarely the primary definitive treatment for this injury in children. Ulnar head resection (Option D) is a salvage procedure for chronic DRUJ issues in adults and is never indicated acutely in children. Percutaneous pinning (Option E) might be used in some unstable pediatric cases, but closed reduction and casting is the initial attempt if possible.
Question 26
The interosseous membrane plays a crucial role in forearm stability. In the context of a Galeazzi fracture, which of the following best describes its primary function that is compromised by the injury?

Explanation
Correct Answer: C
The interosseous membrane (IOM) is a strong fibrous sheet connecting the radius and ulna. Its fibers run obliquely from the radius distally and medially to the ulna proximally. This orientation is critical for two main functions: 1) It transmits axial loads from the hand, through the radius, to the ulna, distributing forces across the forearm. 2) More importantly in the context of a Galeazzi fracture, it resists longitudinal displacement and prevents proximal migration of the radius relative to the ulna. When the radial shaft fractures, this load-sharing and stabilizing function is compromised, contributing significantly to the instability of the distal radioulnar joint (DRUJ) and allowing for radial shortening.
Option A is incorrect; wrist extensors primarily attach to the humerus and dorsal forearm bones. Option B is incorrect; fascial septa separate the compartments, not the IOM. Option D is incorrect; neurovascular bundles run in fascial compartments, not within the IOM itself. Option E is incorrect; synovial fluid lubricates joints, not the IOM.
Question 27
A 65-year-old patient presents with chronic, painful distal radioulnar joint (DRUJ) arthritis and severe positive ulnar variance following a malunited Galeazzi fracture treated 2 years prior. She has exhausted non-operative treatments including injections and therapy. Her radial shaft fracture is healed but shortened. Which of the following salvage procedures would be most appropriate to address her DRUJ pathology and improve forearm rotation?

Explanation
Correct Answer: C
For chronic, painful DRUJ arthritis and severe positive ulnar variance resulting from a malunited Galeazzi fracture, salvage procedures are often necessary. The Sauve-Kapandji procedure is a well-established option. It involves arthrodesis (fusion) of the distal radioulnar joint combined with a pseudoarthrosis (creation of a false joint) of the ulna proximal to the fusion. This allows for forearm rotation while maintaining the distal ulna for cosmetic appearance and some stability. Another common salvage procedure is the Darrach procedure (excision of the distal ulna or ulnar head), which also aims to relieve impingement and restore rotation.
Option A (Scaphoidectomy and four-corner fusion) and Option B (Proximal row carpectomy) are procedures for midcarpal or radiocarpal arthritis, not primarily for DRUJ pathology. Option D (Radial shortening osteotomy) would worsen the positive ulnar variance; an ulnar shortening osteotomy might be considered if the radial fracture was anatomically healed and the primary issue was ulnar length, but not for irreducible DRUJ arthritis. Option E (Wrist arthrodesis) fuses the entire wrist, sacrificing all wrist motion, which is a more extensive procedure typically reserved for diffuse pancarpal arthritis or severe instability not amenable to other options, and it doesn't specifically address DRUJ rotation.
Question 28
A 35-year-old male undergoes ORIF of a Galeazzi fracture via a volar (Henry) approach. Postoperatively, he presents with an inability to flex the interphalangeal joint of his thumb and the distal interphalangeal joints of his index and middle fingers. He also has difficulty pronating his forearm against resistance. Sensation is intact. Which of the following nerves was most likely injured during the surgical procedure?

Explanation
Correct Answer: E
The clinical presentation described—inability to flex the interphalangeal joint of the thumb (due to loss of flexor pollicis longus, FPL) and the distal interphalangeal joints of the index and middle fingers (due to loss of the radial half of flexor digitorum profundus, FDP)—along with difficulty pronating the forearm (due to loss of pronator quadratus, PQ), with intact sensation, is pathognomonic for an anterior interosseous nerve (AIN) palsy. The AIN is a purely motor branch of the median nerve. It is the most commonly injured nerve during a volar (Henry) approach to the distal radial shaft, as it lies directly on the interosseous membrane and can be damaged by retraction, direct trauma, or entrapment.
Option A (Ulnar nerve) injury would affect the ulnar two FDPs (ring and small fingers), most intrinsic hand muscles, and sensation to the ulnar side of the hand. Option B (Median nerve main trunk) injury would cause the described motor deficits plus sensory loss in the median nerve distribution. Option C (Superficial radial nerve) is a sensory nerve, so its injury would not cause these motor deficits. Option D (Posterior interosseous nerve) injury would result in a 'wrist drop' and inability to extend the fingers at the MCP joints, as it innervates the wrist and finger extensors.
Question 29
A 28-year-old male presents with a distal radial shaft fracture after a motorcycle accident. Initial AP and lateral radiographs of the forearm are shown. While the radial fracture is evident, the distal radioulnar joint (DRUJ) appears equivocal for dislocation on these standard views. Which additional radiographic finding or view would be most helpful to confirm DRUJ involvement and thus diagnose a Galeazzi fracture?

Explanation
Correct Answer: B
In cases where DRUJ involvement is equivocal on standard AP and lateral radiographs of the injured forearm, obtaining a comparison view of the contralateral, uninjured forearm is extremely helpful. This allows the surgeon to assess the normal anatomical relationship between the distal radius and ulna for that specific patient, including the width of the DRUJ space and the alignment of the ulnar head within the sigmoid notch of the radius. Subtle widening of the DRUJ on the AP view or slight dorsal (or volar) displacement of the ulna on the lateral view, when compared to the uninjured side, can confirm DRUJ disruption. This is a critical step in diagnosing a Galeazzi fracture when the DRUJ dislocation is not grossly obvious.
Option A (Stress view in radial deviation) is more relevant for ulnocarpal instability or TFCC tears, not primary DRUJ dislocation. Option C (Oblique elbow view) is for assessing the elbow joint and radial head, which is relevant for Monteggia or Essex-Lopresti injuries, not Galeazzi. Option D (Carpal tunnel view) is for assessing the carpal tunnel and is not directly useful for DRUJ stability. Option E (Scapholunate interval measurement) is for carpal instability, specifically scapholunate dissociation, and not directly for DRUJ assessment.
Question 30
After successful open reduction and internal fixation of a Galeazzi fracture and temporary K-wire stabilization of a persistently unstable distal radioulnar joint (DRUJ), what is a key principle of early postoperative rehabilitation?

Explanation
Correct Answer: B
When the DRUJ has been stabilized with temporary K-wires following Galeazzi fracture fixation, the primary goal of early postoperative rehabilitation is to protect the healing capsuloligamentous structures of the DRUJ. This necessitates strict immobilization of the forearm, typically in a long arm cast or splint, in the position of DRUJ stability (e.g., supination for dorsal instability). The K-wires are usually maintained for 4-6 weeks to allow sufficient time for soft tissue healing. Premature or aggressive forearm rotation (Option A) would risk disrupting the healing DRUJ ligaments, leading to recurrent instability or pin complications. After K-wire removal and clinical assessment of DRUJ stability, a gradual and protected range of motion program for forearm rotation can be initiated.
Option C is partially correct regarding wrist and elbow motion, but strict immobilization of the forearm is paramount. Option D (aggressive strengthening) is too early and risks disrupting fixation and healing. Option E (early cast removal and full activity) is far too aggressive and would almost certainly lead to failure of DRUJ stabilization and potential radial malunion.
Question 31
A 35-year-old male presents with a distal third radial shaft fracture. During radiographic evaluation, which of the following findings is most reliable for predicting associated distal radioulnar joint (DRUJ) instability?
Explanation
Question 32
A surgeon plans an open reduction and internal fixation of a proximal third radial shaft fracture utilizing the Thompson approach. This surgical exposure develops an internervous plane between which two muscles?
Explanation
Question 33
A 62-year-old female undergoes volar locking plate fixation for a distal radius fracture. At 6 months postoperatively, she returns with sudden inability to flex her thumb interphalangeal joint. The hardware is noted to be prominent at the watershed line. Which structure has most likely ruptured?
Explanation
Question 34
A 55-year-old female treated nonoperatively in a cast for a minimally displaced Colles fracture presents at 6 weeks unable to actively extend her thumb interphalangeal joint. Tenodesis effect is absent for the thumb. What is the most likely etiology of this complication?
Explanation
Question 35
Which of the following patients with a distal radius fracture is the most appropriate candidate for the application of a dorsal spanning (distraction) plate?
Explanation
Question 36
A 6-year-old boy sustains a Bado Type III Monteggia equivalent lesion. Which of the following defines this injury pattern and its most common associated neurological complication?
Explanation
Question 37
A 30-year-old male presents with a Chauffeur's fracture of the radial styloid after a motor vehicle accident. Due to the mechanism of avulsion, this specific fracture pattern is most frequently associated with a tear of which carpal ligament?
Explanation
Question 38
A 42-year-old male sustains an isolated fracture of the ulnar diaphysis (nightstick fracture) from a direct blow. Under what conditions is open reduction and internal fixation generally indicated over nonoperative management?
Explanation
Question 39
A 28-year-old male develops severe pain out of proportion following closed reduction of a both-bone forearm fracture. Passive extension of the digits elicits excruciating pain. Which fascial compartment of the forearm is typically the most severely affected in this condition?
Explanation
Question 40
A 34-year-old male falls on an outstretched hand, sustaining a comminuted radial head fracture and severe wrist pain. Clinical exam reveals distal radioulnar joint (DRUJ) instability. What surgical intervention is absolutely contraindicated in the management of this specific injury pattern?
Explanation
Question 41
A 50-year-old female presents to the emergency department with a severely displaced extension-type distal radius fracture. She complains of acute, dense numbness in her thumb, index, and long fingers. What is the most appropriate initial step in management?
Explanation
Question 42
To appropriately evaluate reduction of a distal radius fracture, the surgeon must understand normal radiographic parameters. Which of the following values most accurately represents the normal native anatomy of the distal radius?
Explanation
Question 43
A 6-year-old boy presents with an anteriorly displaced radial head dislocation and a midshaft ulnar fracture. Following closed reduction of the ulna, the radial head remains irreducible. What is the most likely anatomic structure blocking reduction?
Explanation
Question 44
A 35-year-old man undergoes volar plating of a distal radius fracture. Three months postoperatively, he develops sudden inability to actively flex the interphalangeal joint of his thumb. Which technical error most likely contributed to this complication?
Explanation
Question 45
A 24-year-old falls onto an outstretched hand and sustains a Galeazzi fracture. Following open reduction and internal fixation of the radius, the distal radioulnar joint (DRUJ) remains unstable in supination. What is the most appropriate next step in management?
Explanation
Question 46
A 40-year-old male sustains an Essex-Lopresti injury. He undergoes radial head excision and pinning of the DRUJ. Six months later, he complains of severe ulnar-sided wrist pain. What is the most likely cause of his symptoms?
Explanation
Question 47
When performing the Thompson (dorsal) approach to the proximal radius, the surgeon develops the interval between which two muscles?
Explanation
Question 48
A 30-year-old man presents with a comminuted fracture of the proximal third of the ulna with an associated anterior dislocation of the radial head. Following rigid plate fixation of the ulna, the radial head is stable but the patient exhibits a lack of active thumb and finger extension, while wrist extension remains intact but deviates radially. Which nerve is most likely injured?
Explanation
Question 49
A 55-year-old woman sustains an extra-articular distal radius fracture treated with closed reduction and casting. Four weeks later, she reports a sudden pop and inability to actively extend her thumb interphalangeal joint. What is the most common management for this complication?
Explanation
Question 50
A 28-year-old male sustains a midshaft both-bone forearm fracture. He undergoes ORIF through two separate surgical incisions. Postoperatively, he develops a radio-ulnar synostosis. Which of the following is the most significant risk factor for developing this complication?
Explanation
Question 51
A 45-year-old laborer sustains an isolated fracture of the ulnar shaft (nightstick fracture) from a direct blow. Radiographs show a midshaft transverse fracture with 5 degrees of angulation and 20% displacement. What is the most appropriate initial management?
Explanation
Question 52
During ORIF of a proximal radius fracture utilizing the volar Henry approach, the surgeon must identify and protect the radial artery and the superficial radial nerve. In the proximal third of the forearm, the posterior interosseous nerve (PIN) is protected by keeping the forearm in which position?
Explanation
Question 53
An 18-year-old male sustains a traumatic scaphoid waist fracture. Which of the following best describes the vascular anatomy that puts this fracture at high risk for nonunion and avascular necrosis?
Explanation
Question 54
A 32-year-old male is evaluated in the ER for a highly comminuted distal radius fracture with an associated scaphoid fracture. What is the most common direction of carpal displacement in a classic Barton's fracture?
Explanation
Question 55
A patient is undergoing fixation of a displaced radial styloid fracture (Chauffeur's fracture). Which carpal ligament injury is most frequently associated with this fracture pattern?
Explanation
Question 56
A 25-year-old snowboarder falls and sustains a severely displaced intra-articular distal radius fracture. Which radiographic parameter is most predictive of developing symptomatic post-traumatic radiocarpal osteoarthrosis?
Explanation
Question 57
Following open reduction and internal fixation of a diaphyseal both-bone forearm fracture, anatomic restoration of the normal radial bow is essential. Failure to restore the radial bow most directly limits which motion?
Explanation
Question 58
A 55-year-old female falls on an outstretched hand, sustaining a displaced distal radius fracture. She complains of severe paresthesias in the median nerve distribution. The fracture is closed reduced in the emergency department, but dense numbness persists and her pain acutely worsens over the next hour. What is the most appropriate next step in management?
Explanation
Question 59
A 30-year-old male sustains a Galeazzi fracture. After rigid open reduction and internal fixation of the radius, the distal radioulnar joint (DRUJ) remains unstable in pronation but is stable when the forearm is placed in full supination. What is the most appropriate intraoperative management of the DRUJ?
Explanation
Question 60
A 29-year-old female sustains a high-energy radiocarpal fracture-dislocation. Radiographs demonstrate translation of the entire carpus with a small, displaced volar radial rim (lunate facet) fragment. Which of the following fixation strategies is paramount to prevent late carpal subluxation?
Explanation
Question 61
A 45-year-old male falls from a ladder, sustaining a highly comminuted radial head fracture, proximal radius shaft migration, and acute wrist pain. Radiographs demonstrate distal radioulnar joint (DRUJ) widening. The radial head is deemed unreconstructible. What is the most appropriate surgical management?
Explanation
Question 62
A 60-year-old female undergoes volar locking plate fixation of a distal radius fracture. Six months later, she presents with a sudden inability to actively flex the interphalangeal joint of her thumb. What surgical technical error most likely caused this complication?
Explanation
Question 63
A 25-year-old male sustains an isolated, closed midshaft ulnar fracture (nightstick fracture) from a direct blow. Radiographs show 5 degrees of angulation and 20% displacement. What is the most appropriate initial management?
Explanation
Question 64
When utilizing the dorsal Thompson approach to expose the proximal third of the radius, which nerve is at highest risk of iatrogenic injury, and how is it biomechanically protected during the procedure?
Explanation
Question 65
During open reduction and internal fixation of both bone forearm fractures, anatomic restoration of the radial bow is critical to maximize which of the following functional outcomes?
Explanation
Question 66
A 35-year-old male sustains diaphyseal fractures of the radius and ulna at the same level. To minimize the severe complication of radioulnar synostosis, which surgical principle must be strictly followed?
Explanation
Question 67
A 40-year-old male presents with a volar shear fracture of the distal radius (volar Barton's fracture). The carpus is subluxated volarly with the intra-articular fracture fragment. What is the primary biomechanical function of a volar plate utilized for this specific fracture pattern?
Explanation
Question 68
A 32-year-old male sustains a distal third radial shaft fracture with an associated distal radioulnar joint (DRUJ) dislocation (Galeazzi fracture). Open reduction and internal fixation of the radius is performed. Intraoperatively, the DRUJ is found to be highly unstable in pronation but reduces well in supination. What is the most appropriate next step in management of the DRUJ?
Explanation
Question 69
A 6-year-old child presents with a Bado Type I Monteggia fracture-dislocation. Closed reduction of the ulnar shaft fracture is achieved, but the radial head remains anteriorly dislocated despite appropriate maneuvers. What is the most common anatomic structure blocking radial head reduction in this pediatric scenario?
Explanation
Question 70
A 45-year-old female presents with a volar Barton's fracture of the distal radius and undergoes ORIF with a volar locking plate. Six months postoperatively, she suddenly develops an inability to actively flex the interphalangeal joint of her thumb. Which complication has most likely occurred?
Explanation
Question 71
A 40-year-old male falls from a height, sustaining a comminuted radial head fracture, wrist pain, and positive ulnar variance on wrist radiographs. Diagnosis of an Essex-Lopresti injury is made. What is the most appropriate surgical management for the proximal radioulnar injury?
Explanation
Question 72
During a Thompson (dorsal) approach to the proximal radius for plate fixation of a comminuted fracture, the surgeon develops the interval between the extensor carpi radialis brevis (ECRB) and the extensor digitorum communis (EDC). Which nerve is at greatest risk during this exposure and requires careful protection?
Explanation
Question 73
A 22-year-old male falls on an outstretched hand and sustains a displaced proximal pole scaphoid fracture. Which vascular structure provides the primary blood supply to the proximal pole, explaining the high risk of avascular necrosis in this injury pattern?
Explanation
Question 74
When evaluating a post-reduction radiograph of an adult distal radius fracture, which of the following represents the widely accepted normal radiographic parameters for radial inclination, radial height, and volar tilt, respectively?
Explanation
Question 75
A 35-year-old male sustains an isolated, non-displaced fracture of the distal third of the ulnar shaft (nightstick fracture) after raising his forearm to block a blunt object. What is the most appropriate initial management?
Explanation
Question 76
A 50-year-old smoker underwent ORIF for a midshaft both-bone forearm fracture 8 months ago. Radiographs now demonstrate an atrophic nonunion of the radius with broken hardware, while the ulna has fully healed. What is the most appropriate definitive management?
Explanation
Question 77
During volar locking plate fixation of a distal radius fracture, screws placed into the distal fragments can protrude dorsally if they are too long. Which anatomical landmark serves as a critical pulley for the extensor pollicis longus (EPL) tendon, placing it at high risk of attritional rupture from prominent dorsal hardware?
Explanation
None
