ABOS Part I Orthopaedic & Hand Surgery Exam Prep: Brachial Plexus & Hand Pathology | Part 21558
Key Takeaway
This module offers 31 advanced multiple-choice questions for ABOS Part I Orthopaedic Surgery and AAOS OITE exam preparation. It covers high-yield topics like brachial plexus birth palsy, glomus tumors, osteoid osteomas, digital neuromas, and volar wrist ganglions, providing detailed explanations for comprehensive review and understanding of complex orthopedic and hand surgery concepts.
ABOS Part I Orthopaedic & Hand Surgery Exam Prep: Brachial Plexus & Hand Pathology | Part 21558
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A male newborn, delivered at 40 weeks gestation with shoulder dystocia, presents with his right arm held in an adducted, internally rotated, and pronated position, with absent spontaneous elbow flexion and shoulder abduction. The Moro reflex is absent on the right. This clinical presentation is most consistent with an injury to which of the following brachial plexus components?
Explanation
Correct Answer: C
The clinical presentation described—adducted, internally rotated, and pronated arm (the 'waiter's tip' posture), absent spontaneous elbow flexion, and absent shoulder abduction—is the classic presentation of Erb-Duchenne palsy. This type of brachial plexus birth palsy primarily involves the upper trunk, which is formed by the C5 and C6 nerve roots. These roots are responsible for innervating muscles involved in shoulder abduction (deltoid, supraspinatus), external rotation (infraspinatus, teres minor), and elbow flexion (biceps, brachialis). The absence of the Moro reflex on the affected side further supports a significant motor deficit in these muscle groups. Lower trunk (C8-T1) injuries would typically present with hand weakness and potentially Horner's syndrome. Posterior, medial, and lateral cord injuries are more specific to the divisions of the brachial plexus and would present with more nuanced patterns of weakness, but the overall 'waiter's tip' posture is pathognomonic for upper trunk involvement.
Question 2
A 24-hour-old macrosomic newborn presents with right upper extremity flaccidity and an absent Moro reflex on the affected side, similar to the case described. Initial radiographs of the right shoulder and humerus are normal. Which of the following findings would most strongly suggest a diagnosis of clavicle fracture over brachial plexus birth palsy?
Explanation
Correct Answer: C
The case explicitly states that gentle palpation of the right clavicle, humerus, and shoulder joint revealed no tenderness, crepitus, or focal swelling, effectively ruling out a gross clavicular or humeral fracture. A clavicle fracture is the most common birth injury and often presents with pseudoparalysis (the infant holds the arm still due to pain), focal tenderness, crepitus, or swelling over the clavicle. While the Moro reflex might be guarded due to pain, it is often present. In contrast, brachial plexus birth palsy presents with true paralysis and specific neurological deficits without bony tenderness or crepitus. The other options (intact grasp reflex, 'waiter's tip' posture, absent biceps reflex, normal passive ROM) are all consistent with or characteristic of brachial plexus birth palsy, not a clavicle fracture.
Question 3
The detailed neurological examination of the newborn in the case revealed absent spontaneous movement for shoulder abduction/external rotation and elbow flexion, but present elbow extension and full spontaneous movement of fingers and thumb. Sensory examination showed intact withdrawal reflex in the hand but absent withdrawal in the lateral upper arm. This pattern of motor and sensory deficit is most indicative of involvement of which specific nerve roots?
Explanation
Correct Answer: C
This question directly assesses knowledge of dermatomal and myotomal innervation. The key deficits described are:
- Absent shoulder abduction/external rotation: Primarily C5-C6 (deltoid, supraspinatus, infraspinatus, teres minor).
- Absent elbow flexion: Primarily C5-C6 (biceps, brachialis).
- Present elbow extension: Primarily C7-C8 (triceps), suggesting sparing of these roots.
- Full spontaneous movement of fingers and thumb: Primarily C8-T1, suggesting sparing of these roots.
- Absent withdrawal to noxious stimuli in the lateral upper arm: This corresponds to the C5-C6 dermatome.
- Intact withdrawal reflex in the hand: This corresponds to the C8-T1 dermatome.
Combining these findings, the pattern of weakness and sensory loss is precisely localized to the C5 and C6 nerve roots, characteristic of an Erb-Duchenne palsy.
Question 4
A 3-week-old newborn, presenting with a clinical picture consistent with Erb-Duchenne palsy, undergoes an MRI of the cervical spine and brachial plexus. An image similar to the T2-weighted sagittal view shown below is obtained. The finding of T2 hyperintensity and thickening of the C5 and C6 nerve roots, without clear evidence of pseudomeningoceles, as described in the case, most accurately suggests which type of injury?

Explanation
Correct Answer: C
The case explicitly states the MRI findings: "Sagittal and Axial T2-weighted images demonstrated T2 hyperintensity and thickening of the right C5 and C6 nerve roots in the supraclavicular fossa, consistent with significant stretch injury and edema, likely representing neuromas-in-continuity or ruptures. No clear evidence of pseudomeningoceles in the cervical spinal canal, which reduces the likelihood of complete preganglionic C5/C6 avulsion, but does not definitively rule it out."
- T2 hyperintensity and thickening: These are classic MRI signs of nerve injury, indicating edema, inflammation, and scar tissue formation within the nerve, consistent with a neuroma-in-continuity or a complete rupture.
- Absence of pseudomeningoceles: Pseudomeningoceles (extradural collections of CSF) are highly suggestive of preganglionic root avulsions from the spinal cord. Their absence in this case makes a complete preganglionic avulsion less likely, although it doesn't entirely rule out partial avulsions or avulsions without meningeal tearing.
Therefore, the findings point towards a severe postganglionic injury, such as a rupture or neuroma-in-continuity, rather than a preganglionic avulsion or a mild neurapraxia (which would typically not show such significant T2 changes at 3 weeks).
Question 5
Based on the "Pearls & Pitfalls" section of the case, which of the following is considered the most critical prognostic indicator for spontaneous recovery in a newborn with brachial plexus birth palsy, strongly influencing the decision for surgical intervention?
Explanation
Correct Answer: C
The "Pearls" section of the case explicitly highlights: "'Biceps at 3 Months' Rule: The most important prognostic indicator for spontaneous recovery. Absence of antigravity biceps function by 3 months is a strong indication for surgical consideration. Don't wait beyond 6 months for surgical intervention in severe cases." The ability to actively flex the elbow against gravity (biceps function) is a crucial milestone. If this function does not return by 3 months, it indicates a severe injury (likely axonotmesis or neurotmesis) with a low probability of meaningful spontaneous recovery, thus prompting surgical evaluation and intervention within the critical window (3-9 months).
Question 6
The patient in the case presented with a right upper trunk brachial plexus birth palsy, primarily involving C5 and C6 nerve roots, characterized by weakness in shoulder abduction/external rotation and elbow flexion, with relative sparing of lower root functions. According to the Narakas classification system, this presentation corresponds to which type of injury?
Explanation
Correct Answer: D
The case explicitly states: "Our patient presented as a Narakas Type I injury, primarily affecting C5 and C6 roots." The Narakas classification system categorizes brachial plexus injuries based on the extent of nerve root involvement:
- Type I (Erb-Duchenne): C5-C6 involvement (most common), characterized by shoulder abduction/external rotation and elbow flexion weakness.
- Type II: C5-C7 involvement, similar to Type I with added wrist extension weakness.
- Type III (Total Palsy with Intact Hand): C5-C8 involvement, upper and forearm weakness, hand function generally preserved.
- Type IV (Total Palsy with Hand Involvement): C5-T1 involvement, flail arm, often associated with Horner's syndrome.
The patient's clinical presentation perfectly matches the description of a Narakas Type I injury.
Question 7
During the surgical reconstruction for the patient's Erb-Duchenne palsy, an image similar to the one below might be seen during nerve coaptation. The surgical team performed an Oberlin transfer. What was the primary purpose of this specific nerve transfer?
Explanation
Correct Answer: C
The case details the surgical reconstruction: "To ensure reliable reinnervation of elbow flexion (biceps), a direct nerve transfer was performed. The medial pectoral nerve... was then coapted to the distal stump of the musculocutaneous nerve (or a specific fascicle leading to biceps)... This 'Oberlin transfer' provides a strong, reliable source of axons to the biceps, prioritizing restoration of active elbow flexion, which is critical for hand-to-mouth function."
- The Oberlin transfer typically involves transferring a fascicle of the ulnar nerve (or medial pectoral nerve, as described in this case, which is a common variant) to the motor branch of the musculocutaneous nerve that innervates the biceps.
- Its primary goal is to restore active elbow flexion, a critical function for activities of daily living, particularly hand-to-mouth movements.
- Other transfers, such as the spinal accessory to suprascapular nerve transfer, are used for shoulder abduction and external rotation.
Question 8
Following resection of the neuromatous segments of the C5 and C6 roots, the surgical team in the case performed interpositional nerve grafting. Which of the following nerves was harvested and utilized as a multi-fascicular cable graft for this procedure?
Explanation
Correct Answer: C
The case explicitly states under "Surgical Reconstruction": "The ipsilateral sural nerve was harvested from the calf as a multi-fascicular cable graft, providing sufficient length and caliber." The sural nerve is a commonly used and preferred donor nerve for nerve grafting in brachial plexus injuries due to several advantages:
- It is a sensory nerve, so its harvest results in minimal functional deficit (a small area of numbness on the lateral foot).
- It provides sufficient length and multiple fascicles, making it suitable for bridging gaps in larger nerves.
- Its harvest is relatively straightforward and has low morbidity.
The other nerves listed are either motor nerves (radial, ulnar) whose sacrifice would cause significant functional deficit, or cutaneous nerves that may not provide adequate length or fascicular structure for major nerve grafting.
Question 9
Immediately following the nerve reconstruction surgery for brachial plexus birth palsy, the patient's right arm was placed in an airplane splint. What is the primary purpose of positioning the shoulder abducted to 90 degrees, externally rotated to 30 degrees, and the elbow flexed to 90 degrees?
Explanation
Correct Answer: B
The "Post-Operative Protocol & Rehabilitation" section states: "The patient's right arm was placed in an airplane splint or a long arm cast with the shoulder abducted to 90 degrees, externally rotated to 30 degrees, and the elbow flexed to 90 degrees. This position minimizes tension on the nerve repair sites, particularly the grafted segments and the Oberlin transfer."
- Nerve repairs, especially grafts and transfers, are delicate and susceptible to tension. Maintaining the limb in a position that approximates the origin and insertion points of the repaired nerves reduces stress on the coaptation sites, promoting healing and preventing disruption.
- Early active range of motion is contraindicated immediately post-op. While preventing contractures is a long-term goal, the immediate priority is nerve protection. Glenohumeral dysplasia is a long-term complication, not directly prevented by immediate post-op splinting position. Wound care is important but not the primary reason for this specific positioning.
Question 10
A child who underwent nerve reconstruction for Erb-Duchenne palsy, similar to the case patient, presents at 3 years of age with persistent shoulder internal rotation contracture despite extensive physical therapy. Based on the case's "Post-Operative Protocol & Rehabilitation" section, which of the following secondary procedures would most likely be considered to address this specific deformity?
Explanation
Correct Answer: B
The "Post-Operative Protocol & Rehabilitation" section, under "Management of Secondary Procedures," specifically addresses persistent shoulder internal rotation contractures: "Shoulder internal rotation contractures often develop due to persistent muscle imbalance (stronger internal rotators). If conservative measures fail, secondary procedures like Latissimus Dorsi and Teres Major tendon transfers (for external rotation) or subscapularis release may be considered, typically after 2-3 years of age, or once nerve regeneration plateaus. Humeral derotational osteotomy may be necessary in older children with persistent internal rotation deformity and functional deficits."
- A humeral derotational osteotomy directly corrects the bony rotational deformity of the humerus, which contributes significantly to a fixed internal rotation contracture.
- Latissimus Dorsi and Teres Major tendon transfers are also used to improve external rotation, but are not listed as an option. Subscapularis release is also mentioned.
- Triceps to biceps transfer is for elbow flexion.
- Spinal accessory to suprascapular and medial pectoral to musculocutaneous nerve transfers are primary nerve reconstruction procedures, not secondary procedures for contractures.
- While pectoralis major and minor contribute to internal rotation, the case specifically highlights other procedures for persistent contracture, with humeral derotational osteotomy being a definitive option for bony deformity.
Question 11
A 42-year-old female presents with a 5-year history of intermittent, severe, paroxysmal pain in her right index fingertip, exacerbated by cold exposure. She describes the pain as disproportionate to any visible injury. On examination, there is no obvious swelling or erythema, but she exhibits exquisite, localized tenderness to pinpoint pressure over the subungual region of the index finger. When a digital tourniquet is inflated proximally, the pain temporarily subsides. Given this clinical presentation, which of the following is the most specific diagnostic test for the suspected condition?

Explanation
Correct Answer: D
The patient's presentation—severe, paroxysmal fingertip pain, cold intolerance, and pinpoint tenderness—is classic for a glomus tumor. The case specifically mentions the three mandatory clinical tests for suspected glomus tumors: Love Pin Test, Hildreth Ischemia Test, and Cold Sensitivity Test. Among these, the Hildreth Ischemia Test, which involves the relief of pinpoint pain when a proximal tourniquet is inflated to suprasystolic pressures, is highlighted in the case as being highly specific (approaching 100 percent specificity) for glomus tumors. While the Love Pin Test (pinpoint tenderness) and Cold Sensitivity Test (pain exacerbation with cold) are part of the classic triad and are important diagnostic indicators, the Hildreth test provides the highest specificity for confirming the diagnosis clinically.
High-resolution MRI (Option A) is the gold standard for imaging and confirming the diagnosis, but it is an imaging modality, not a clinical test, and the question asks for the most specific diagnostic test. Electromyography and nerve conduction studies (Option E) would be more relevant for nerve entrapment or neuropathic conditions, which are less likely given the specific clinical triad and positive tourniquet test.
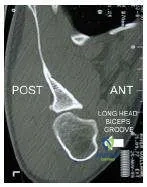
Question 12
A 35-year-old male presents with chronic, insidious nocturnal pain in his long finger, which is partially relieved by over-the-counter NSAIDs. Initial radiographs of the hand were reported as normal. Due to persistent symptoms, a dedicated high-resolution imaging study of the digit is performed. If the suspected diagnosis is an osteoid osteoma of the phalanx, which of the following imaging findings would be most characteristic?

Explanation
Correct Answer: C
The patient's symptoms—insidious, nocturnal pain relieved by NSAIDs—are highly characteristic of an osteoid osteoma. The case states that osteoid osteomas, while less common in the phalanges, can present this way and that their small size and typical lucent nidus can be overlooked on initial radiographs. The pathophysiology involves prostaglandin production by the nidus, causing pain and adjacent bony sclerosis. Therefore, the most characteristic imaging finding for an osteoid osteoma is a lucent nidus with surrounding reactive bony sclerosis (Option C).
Option A describes the typical MRI findings for a glomus tumor. Option B describes a digital neuroma. Option D describes findings associated with CRPS. Option E describes findings that might be seen with a glomus tumor or other soft tissue lesions on ultrasound, but not specifically an osteoid osteoma.
Question 13
A 50-year-old female undergoes surgical excision of a subungual glomus tumor via a transungual approach. During the procedure, the surgeon carefully removes the nail plate and makes an incision in the sterile matrix. Which of the following statements regarding the matrix incision and subsequent repair is most consistent with the principles outlined in the case to prevent postoperative complications?

Explanation
Correct Answer: B
The case provides detailed guidance on the transungual approach for subungual lesions. It explicitly states: "Under loupe magnification, the sterile matrix is inspected... A longitudinal incision is made directly over the mass. Transverse incisions are strictly avoided as they disrupt the longitudinal growth pattern of the nail and significantly increase the risk of postoperative split-nail deformity." It further details: "The sterile matrix is elevated using fine skin hooks. Glomus tumors are typically encapsulated and gelatinous. Using tenotomy scissors or a fine scalpel... the tumor is meticulously shelled out of its bed. Care must be taken to ensure complete excision, as retained microscopic satellites are the primary cause of recurrence." This directly supports Option B.
Option A is incorrect because transverse incisions are strictly avoided due to the risk of nail dystrophy. Option C is incorrect; the case specifies 7-0 or 8-0 absorbable sutures for matrix repair. Option D is incorrect; the native nail plate is preserved and used as a biologic stent. Option E is incorrect; the case states that if a bony crater is present, it is gently curetted.
Question 14
A 60-year-old male presents with chronic, debilitating pain in his small finger following a crush injury 2 years prior. He describes a focal trigger point that, when pressed, sends shooting pain up his arm. Conservative measures, including desensitization therapy and local injections, have failed. Surgical exploration is planned for a suspected digital neuroma. According to the case, which of the following strategies for managing the nerve stump after resection is considered most critical in mitigating postoperative pain?

Explanation
Correct Answer: D
The case discusses the management of painful digital neuromas. It states: "Management of the proximal stump remains controversial and highly variable. Options include: Traction Neurectomy... Intramuscular or Intraosseous Burial... Nerve Capping or Wrapping... Targeted Muscle Reinnervation." However, in the 'Summary of Key Literature and Guidelines' section, it explicitly highlights: "A systematic review by Eberlin et al. highlights that while no single technique for neuroma management (burial, capping, or simple excision) is universally superior, the prevention of mechanical tethering of the nerve stump is the most critical factor in mitigating postoperative pain."
Options A, B, C, and E represent various techniques or approaches, but Option D directly addresses the overarching critical factor identified in the literature review for preventing postoperative pain, which is preventing mechanical tethering. Simple excision (A) without further management often leads to recurrence. Primary repair (B) is generally not feasible for a neuroma stump where the distal segment is lost. Capping (C) is one method to prevent tethering, but D is the more fundamental principle. Neurolysis (E) addresses existing tethering but doesn't inherently prevent future tethering of the resected stump.
Question 15
A 48-year-old female undergoes surgical excision of a subungual glomus tumor. Two months postoperatively, she develops a split-nail deformity and persistent nail plate irregularity. Based on the information provided, which of the following is the most likely iatrogenic cause of this complication?

Explanation
Correct Answer: C
The case explicitly addresses complications, particularly nail dystrophy. Under 'Complications and Management', it states: "Nail Dystrophy (10 to 20 percent) - Etiology: Iatrogenic injury to the germinal matrix; non-anatomic repair of the sterile matrix; transverse matrix incisions." Furthermore, in the 'Detailed Surgical Approach and Technique' section for the transungual approach, it warns: "A longitudinal incision is made directly over the mass. Transverse incisions are strictly avoided as they disrupt the longitudinal growth pattern of the nail and significantly increase the risk of postoperative split-nail deformity." Therefore, a transverse incision in the sterile matrix is the most likely iatrogenic cause of a split-nail deformity.
Option A (incomplete excision) would lead to tumor recurrence, not primarily nail dystrophy. Option B (failure to replace the nail plate) could lead to adherence issues or infection, but not specifically a split-nail deformity. Option D (CRPS) is a systemic pain syndrome, not a direct cause of nail structural deformity. Option E (infection) could cause nail changes but is less specific to a split-nail deformity than a transverse matrix incision.
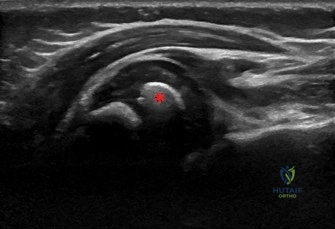
Question 16
A 38-year-old male presents with mysterious fingertip pain. High-resolution MRI of the digit is performed, revealing a well-demarcated mass in the subungual region. The report describes the mass as hypointense on T1-weighted imaging, markedly hyperintense on T2-weighted imaging, and exhibiting avid, homogeneous enhancement following gadolinium administration. Based on these findings, what is the most likely diagnosis?

Explanation
Correct Answer: C
The case specifically details the advanced imaging protocols for glomus tumors. Under 'Pre Operative Planning and Patient Positioning', it states: "For glomus tumors, a dedicated fingertip protocol using a surface coil is required. Glomus tumors typically appear as well-demarcated masses that are hypointense on T1-weighted imaging, markedly hyperintense on T2-weighted imaging, and exhibit avid, homogeneous enhancement following gadolinium administration." The MRI findings described in the question perfectly match the characteristic appearance of a glomus tumor.
Digital neuromas (A) are typically disorganized masses of nerve fibers, often identified by HRUS. Osteoid osteomas (B) are bony lesions with a lucent nidus and sclerosis, best seen on radiographs or CT. Subungual exostoses (D) are bony outgrowths. Epidermoid inclusion cysts (E) would have different signal characteristics on MRI, typically fluid-filled and not showing avid enhancement in the same manner as a highly vascular glomus tumor.
Question 17
A 45-year-old construction worker presents with chronic pain in his dominant thumb pulp, which is exacerbated by pinch and grip activities. He denies any specific injury but notes the pain has been gradually worsening over the past year. Clinical examination reveals a subtle, deep-seated tenderness in the pulp, but no visible mass. Given the high density of sensory receptors and the unique anatomical structure of the digital pulp, why do even microscopic space-occupying lesions in this region often cause disproportionately severe pain?

Explanation
Correct Answer: C
The case specifically addresses the anatomy and biomechanics of the digital pulp. Under 'Digital Pulp and Fibrous Septa', it states: "The volar digital pulp is heavily compartmentalized by dense fibrous septa running from the volar dermis to the periosteum of the distal phalanx. This architectural arrangement stabilizes the skin during pinch and grip but creates closed compartments. Consequently, even microscopic space-occupying lesions... or minor edema can cause exponential increases in compartmental pressure, resulting in disproportionately severe pain." This directly explains why small lesions cause severe pain.
While Pacinian corpuscles (A) contribute to sensation, the primary reason for disproportionate pain from small lesions is the compartmentalization. The rich vascular supply (B) is important but not the direct cause of disproportionate pain from a small mass effect. The nail matrix (D) is dorsal to the pulp and less directly affected by pulp lesions causing pain. While digital nerves are present (E), the key factor highlighted for disproportionate pain from small lesions is the compartmentalization and subsequent pressure increase, rather than just superficial nerve location.
Question 18
A 30-year-old female is diagnosed with a subungual glomus tumor and undergoes surgical excision. Postoperatively, she is instructed on a rehabilitation protocol. Which of the following is a critical component of Phase Two (2-week mark) rehabilitation for this patient?

Explanation
Correct Answer: C
The case outlines the postoperative rehabilitation protocols. Under 'Phase Two Suture Removal and Desensitization', it states: "At the two-week mark, non-absorbable sutures securing the nail plate are removed... Gentle, active range of motion (ROM) of the DIP, PIP, and MCP joints is initiated. A formal desensitization program is critical at this stage, involving tactile stimulation with varying textures, fluidotherapy, and gentle massage to normalize sensory input and prevent hypersensitivity."
Option A (strict immobilization for 6 weeks) is incorrect; early gentle ROM is initiated at 2 weeks. Option B (aggressive strengthening) is typically introduced later, in Phase Three (4-6 weeks). Option D is incorrect; the stenting nail plate is left in situ for 3-6 months, and immediate return to full activities is not advised. Option E (stellate ganglion blocks) is a treatment for CRPS, not a routine part of Phase Two rehabilitation for an uncomplicated glomus tumor excision.
Question 19
A 55-year-old male presents with a chronic paronychia that has been refractory to oral antibiotics and soaks for several weeks. On examination, there is fluctuance and significant tenderness along the lateral nail fold, suggesting a deeper collection. According to the case, what is the operative indication for this patient's condition?

Explanation
Correct Answer: C
The 'Indications and Contraindications' table in the case specifically addresses occult infections. For 'Occult Infection', the operative indications are listed as: "Abscess formation; osteomyelitis of the distal phalanx; failure of targeted antibiotic therapy." The patient's presentation of refractory chronic paronychia with fluctuance and tenderness, indicating a deeper collection, directly aligns with the indication for abscess formation and failure of antibiotic therapy.
Options A and B are listed as non-operative indications for occult infection. Option D is a contraindication for osteoid osteoma surgery, not infection. Option E is a general contraindication for any surgery, but not a specific operative indication for infection.
Question 20
A 40-year-old female presents with a 7-year history of severe, intermittent pain in her ring finger, exacerbated by cold. She reports that the pain is often described as a throbbing or burning sensation. On examination, a small bluish discoloration is noted under the nail plate, and she has exquisite tenderness to pinpoint pressure. The average diagnostic delay for this condition, as described in the case, underscores its 'mysterious' nature. What is the estimated average diagnostic delay for this condition?

Explanation
Correct Answer: D
The patient's symptoms (severe, intermittent pain, cold exacerbation, throbbing/burning, subungual bluish discoloration, pinpoint tenderness) are classic for a glomus tumor. The 'Introduction and Epidemiology' section of the case specifically highlights the diagnostic delay for glomus tumors: "Misdiagnosis or delayed diagnosis is common, with an average diagnostic delay of 5 to 7 years, underscoring their 'mysterious' nature."
Therefore, an average diagnostic delay of 5 to 7 years (Option D) is the correct answer, directly from the provided text.
Question 21
A 33-year-old male is scheduled for surgical excision of a glomus tumor located in the volar pulp of his middle finger. During preoperative planning, the surgeon considers the optimal incision approach. Which of the following incision types is contraindicated for a lesion in the volar pulp, and why?

Explanation
Correct Answer: D
The case details surgical approaches based on lesion location. Under 'Volar Approach for Pulp Lesions', it explicitly states: "For neuromas or glomus tumors located in the volar pulp, a mid-lateral incision or a volar Bruner (zigzag) incision is utilized. Direct longitudinal incisions over the tactile surface of the volar pad are contraindicated due to the risk of painful scar formation in the primary pinch zone."
Options A and B are described as appropriate approaches for volar pulp lesions. Option C (transungual approach) is for subungual lesions, not pulp lesions, making it inappropriate but not 'contraindicated' in the sense of causing harm if used for a pulp lesion (it simply wouldn't expose it). Option E (lateral periungual approach) is for lateral nail unit lesions. The direct longitudinal incision over the tactile surface (D) is specifically highlighted as contraindicated due to the risk of painful scar formation in a critical functional area.
Question 22
A 28-year-old female presents with a 1.5 cm, firm, non-tender mass on the volar-radial aspect of her left wrist, which she noticed 3 months ago. She is a graphic designer and reports no pain or functional limitations, only mild cosmetic concern. Physical examination confirms a mobile, transilluminating mass. An Allen's test is normal. Based on the epidemiology and initial management guidelines presented in the case, what is the most appropriate initial recommendation?
Explanation
Correct Answer: C
The case explicitly states that a significant proportion of ganglions (reported as high as 50% in some series) can undergo spontaneous resolution. Therefore, observation with reassurance is considered a valid and often preferred initial strategy for asymptomatic or minimally symptomatic lesions. The patient in the vignette is asymptomatic with only mild cosmetic concern, making observation the most appropriate first-line recommendation.
Option A is incorrect because immediate surgical excision is typically reserved for symptomatic, functionally limiting, or diagnostically uncertain lesions, not solely for mild cosmetic concern in an otherwise asymptomatic patient.
Option B, aspiration, is a reasonable first-line treatment for symptomatic patients who wish to defer or avoid surgery, but it has a significantly higher recurrence rate (30-70%) compared to surgery. For an asymptomatic patient, it's not the most appropriate initial step.
Option D, MRI, is generally reserved for cases with diagnostic uncertainty, very large/deeply seated ganglions, or suspicion of other tumor types. Given the classic presentation (firm, mobile, transilluminating mass), ultrasound would be the preferred initial imaging if diagnostic confirmation were needed, but observation is still primary for an asymptomatic lesion.
Option E, splinting, is a non-operative measure that can be considered for mild, intermittent pain or as part of an initial conservative trial, but for an asymptomatic mass, observation is simpler and often sufficient.
Question 23
A 35-year-old male presents with a painful volar wrist ganglion located just radial to the FCR tendon. Pre-operative planning is underway for surgical excision. Which of the following anatomical structures is considered the single most critical to identify and meticulously protect during this procedure, and what pre-operative test is mandatory to assess its patency?
Explanation
Correct Answer: C
The case explicitly states, 'The Radial Artery: This represents the single most critical structure to identify and meticulously protect during volar wrist ganglion excision.' It also emphasizes, 'Allen's Test: This is an absolutely mandatory assessment for all volar wrist masses, particularly those located on the radial side. It evaluates the patency of the ulnar artery and the collateral circulation to the hand.' Injury to the radial artery, especially in a hand with dominant radial supply, can lead to severe ischemic consequences.
Option A is incorrect. While the palmar cutaneous branch of the median nerve is the most common nerve injured, it is not considered the 'single most critical structure' in terms of potential for limb-threatening complications. Tinel's test assesses nerve irritation, not arterial patency.
Option B is incorrect. The FCR tendon is a crucial anatomical landmark but not a critical structure in the same sense as the radial artery. Finkelstein's test assesses for De Quervain's tenosynovitis.
Option D is incorrect. The median nerve proper is deep and typically not in direct contiguity with a volar ganglion, though careful dissection is needed. Phalen's test assesses for carpal tunnel syndrome.
Option E is incorrect. The superficial radial nerve branches are less commonly directly involved in volar wrist ganglion excision compared to dorsal approaches. Two-point discrimination assesses sensory function.
Question 24
During surgical excision of a volar wrist ganglion, a surgeon makes the initial skin incision. As the subcutaneous tissue is dissected, a small nerve is encountered superficially, just ulnar to the FCR tendon. The surgeon recognizes this as a structure highly susceptible to iatrogenic injury during this stage of the procedure. Which nerve is most likely being described, and what is its primary clinical significance if injured?
Explanation
Correct Answer: C
The case states, 'Critical First Step: Immediately upon incising the skin and subcutaneous tissue, proactively identify and protect the palmar cutaneous branch of the median nerve. This nerve often courses superficially and can be inadvertently incised or mistaken for fibrous tissue if not specifically anticipated. It typically lies ulnar to the FCR tendon but can have variable courses.' It further notes that injury can lead to 'painful neuroma formation or chronic dysesthesia within its sensory distribution' (radial palm).
Option A is incorrect. The superficial radial nerve is less commonly directly involved in volar wrist ganglion excision, and its sensory distribution is the radial dorsum of the hand and thumb, not the radial palm.
Option B is incorrect. The median nerve proper lies deeper, beneath the flexor retinaculum, and while motor weakness of thenar muscles is a consequence of median nerve injury, it's not the nerve most susceptible to injury during the initial superficial dissection for a volar ganglion.
Option D is incorrect. The ulnar nerve is located on the ulnar side of the wrist and is not typically at risk during a radial volar ganglion excision. Its sensory distribution is the ulnar 1.5 digits.
Option E is incorrect. The radial nerve's motor branch (posterior interosseous nerve) is in the forearm and not typically at risk during a volar wrist ganglion excision. Wrist drop is a consequence of radial nerve palsy, not specific to this procedure.
Question 25
A 42-year-old patient undergoes surgical excision of a recurrent volar wrist ganglion. During the procedure, the surgeon meticulously dissects the ganglion, carefully protecting the radial artery and palmar cutaneous nerve. To minimize the risk of future recurrence, what is the most crucial step the surgeon must perform?
Explanation
Correct Answer: C
The case explicitly states, 'Key to Preventing Recurrence: The definitive step for minimizing recurrence is the complete excision of the stalk along with a small, elliptical cuff of the surrounding joint capsule from which it originates.' It further notes, 'The primary surgical objective is the complete excision of the entire cyst, including its stalk, back to its point of origin from the underlying joint capsule.'
Option A, capsulodesis, is a procedure to stabilize a joint, not directly related to ganglion recurrence prevention.
Option B is incorrect. While the capsular defect is typically left open, this is a consequence of the excision, not the primary action to prevent recurrence. The excision of the stalk and capsule is what prevents recurrence.
Option D, corticosteroid injection, is a non-operative treatment option with high recurrence rates and is not part of the surgical technique to prevent recurrence.
Option E, repairing the FCR tendon sheath, is not mentioned as a step to prevent ganglion recurrence. The FCR tendon is a landmark, and its sheath is not the origin of the ganglion.
Question 26
A 55-year-old male presents with a 3 cm, firm, non-tender mass on the volar aspect of his right wrist. He has a history of osteoarthritis. The mass does not transilluminate. Given the diagnostic uncertainty and the patient's history, which imaging modality is most appropriate to definitively characterize the mass and its relationship to surrounding structures, and why?
Explanation
Correct Answer: D
The case states, 'Magnetic Resonance Imaging (MRI): Generally reserved for cases presenting with diagnostic uncertainty, very large or deeply seated ganglions, or when there is suspicion of intraosseous pathology, complex intra-articular involvement, or alternative soft tissue tumors. MRI offers superior soft tissue contrast, allowing for precise definition of the lesion's extent and its relationship to osseous structures, tendons, nerves, and vessels.' The patient's mass does not transilluminate, which is atypical for a simple ganglion, and his history of osteoarthritis could suggest other pathologies, leading to diagnostic uncertainty.
Option A is incorrect. Plain radiographs are useful to exclude osseous pathology but do not characterize soft tissue masses well.
Option B is incorrect. While high-resolution ultrasound is often the first-line and most valuable imaging modality for confirming the cystic nature and delineating neurovascular relationships, the lack of transillumination and diagnostic uncertainty in this case suggest a need for superior soft tissue contrast to rule out other tumors, making MRI more appropriate.
Option C, CT scan, is excellent for bone detail but less so for soft tissue characterization compared to MRI, especially for differentiating fluid-filled cysts from other soft tissue tumors.
Option E, arteriogram, is invasive and specifically for vascular assessment, not for general mass characterization unless vascular compromise is strongly suspected as the primary pathology.
Question 27
A 30-year-old musician presents with a volar wrist ganglion that causes persistent, debilitating pain during violin practice, significantly impacting her ability to perform. She has undergone two attempts at aspiration with temporary relief, but the ganglion has recurred each time. Physical examination reveals a tender, firm mass. An Allen's test is normal. Based on the case, what is the most appropriate next step in management?
Explanation
Correct Answer: C
The case outlines clear operative indications: 'Persistent or severe pain: When pain is debilitating, unremitting, unresponsive to adequate non-operative measures, or significantly impacts daily activities, occupational function, or sleep quality.' It also lists 'Recurrence after aspiration: Documented recurrence following one or more attempts at non-operative aspiration' as an operative indication. This patient meets both criteria, with debilitating pain impacting her occupation and recurrence after two aspirations.
Option A is incorrect. While aspiration is a non-operative option, the patient has already failed two attempts, making further aspiration less likely to provide definitive relief and delaying definitive treatment.
Option B is incorrect. While psychological support can be part of comprehensive pain management, it is not the primary next step for a surgically amenable lesion causing debilitating pain and functional limitation.
Option D is incorrect. Opioid analgesics are not a definitive treatment for a structural problem like a ganglion and carry risks of dependence. Continued observation is inappropriate given the severity of symptoms and failure of conservative measures.
Option E is incorrect. Prolonged immobilization with a cast is not a standard or effective treatment for symptomatic volar wrist ganglions, especially after failed aspirations, and could lead to stiffness.
Question 28
A 60-year-old patient undergoes surgical excision of a volar wrist ganglion. Six months post-operatively, the patient returns with a palpable, tender mass at the site of the previous surgery, confirmed by ultrasound to be a recurrent ganglion. According to the case, what is the most common reason for ganglion recurrence after surgical excision?
Explanation
Correct Answer: C
The case explicitly states under 'Complications & Management' that for recurrence, it is 'Higher risk if the stalk and a sufficient cuff of adjacent capsule are not fully excised.' In the 'Summary of Key Literature / Guidelines,' it reiterates, 'Incomplete excision of the capsular stalk or failure to remove all accessory loculations is widely considered the predominant cause of recurrence.'
Option A, inadequate post-operative immobilization, is not cited as the most common reason for recurrence. While immobilization is part of post-op care, its primary role is comfort and initial healing, not preventing recurrence from an incompletely excised stalk.
Option B, failure to identify and protect the radial artery, is a severe intraoperative complication but not the cause of ganglion recurrence.
Option D, CRPS, is a rare but severe complication of surgery, not a cause of ganglion recurrence.
Option E, excessive early post-operative wrist mobilization, can contribute to pain or stiffness but is not identified as the primary cause of ganglion recurrence.
Question 29
During a volar wrist ganglion excision, despite meticulous technique, the radial artery is inadvertently lacerated. The pre-operative Allen's test was positive, indicating a dominant radial artery supply to the hand. What is the most appropriate immediate management strategy for this complication?
Explanation
Correct Answer: C
The case states under 'Complications & Management' for Radial Artery Injury: 'Potentially leads to hand ischemia in cases of dominant radial artery supply (identified by a positive Allen's test).' For 'Salvage Strategies / Management,' it advises: 'Immediate Intraoperative: Primary repair if small laceration. Transection/Thrombosis: Microvascular repair or interpositional vein grafting by a surgeon experienced in microsurgery if there is a significant risk of hand ischemia (positive Allen's test).' A positive Allen's test signifies a critical need for repair to prevent ischemia.
Option A is incorrect. Ligation of the radial artery with a positive Allen's test would likely lead to severe hand ischemia and potential tissue loss.
Option B is incorrect. Direct pressure might temporarily control bleeding but does not address the laceration, and observation alone is insufficient given the risk of ischemia with a positive Allen's test.
Option D is incorrect. While post-operative anticoagulation may be necessary after repair, it is not the immediate intraoperative management for an acute laceration.
Option E is incorrect. Delayed repair after packing the wound would increase the risk of ischemia and is not appropriate for an acute arterial injury, especially with a positive Allen's test.
Question 30
A patient has undergone successful open surgical excision of a volar wrist ganglion. The surgeon is planning the post-operative rehabilitation protocol for the immediate period (Day 0-7). Which of the following is a key component of this immediate post-operative phase?
Explanation
Correct Answer: C
The case outlines the 'Immediate Post-Operative Period (Day 0-7)' as follows: 'Elevation: Strict elevation of the hand above heart level... is crucial to minimize post-operative swelling and edema.' And 'Finger ROM: Encourage immediate, gentle active range of motion (AROM) exercises for the fingers and thumb. This helps prevent stiffness in the digits, maintains tendon gliding, and promotes lymphatic drainage.'
Option A, progressive strengthening exercises, is part of the intermediate rehabilitation phase (Weeks 3-6), not the immediate post-operative period.
Option B, suture removal and scar massage, typically occurs in the early rehabilitation phase (Weeks 1-3), after the initial 7-10 days.
Option D, aggressive passive range of motion, is generally avoided in the immediate post-operative period to protect healing tissues and prevent pain. Gentle PROM might be initiated later in the early or intermediate phase, often with a therapist.
Option E, dynamic splinting, is an advanced rehabilitation technique for persistent stiffness and is not part of the immediate post-operative protocol.
Question 31
A 38-year-old patient with a symptomatic volar wrist ganglion inquires about arthroscopic excision, having heard it offers faster recovery and improved cosmesis for wrist ganglions. Based on the summary of key literature and guidelines, what is the most accurate statement regarding arthroscopic excision for *volar* wrist ganglions?
Explanation
Correct Answer: B
The case states under 'Arthroscopic Excision': 'However, for volar wrist ganglions, arthroscopic techniques are significantly more technically challenging. This is primarily due to the anatomically confined operative space, the close proximity of vital neurovascular structures (especially the radial artery), and the inherent difficulty in achieving direct intra-articular visualization and thorough excision of the volar capsule and stalk from within the joint.'
Option A is incorrect. The case explicitly states arthroscopic techniques are more challenging for volar ganglions and are not the preferred method.
Option C is incorrect. While challenging, it is not stated to be absolutely contraindicated, but rather less common and reserved for experienced surgeons.
Option D is incorrect. The literature for arthroscopic excision of volar ganglions is described as 'less robust and mature' compared to dorsal lesions, implying that comparable recurrence rates and faster recovery are not as well-established or universally achieved as with open techniques for volar lesions.
Option E is incorrect. Arthroscopic excision is primarily discussed in the context of soft tissue ganglions (dorsal or volar), not specifically intraosseous ganglions.
Question 32
A 1-month-old infant presents with a flaccid right upper extremity following a complicated macrosomic delivery. Physical examination reveals an ipsilateral ptosis and miosis. Which of the following is the most appropriate management?
Explanation
Question 33
A 25-year-old male sustains a C5-C6 brachial plexus avulsion injury. At 4 months post-injury, he has no spontaneous elbow flexion. An Oberlin nerve transfer is planned. Which of the following best describes this procedure?
Explanation
Question 34
During a fasciectomy for Dupuytren's disease, the surgeon dissects a spiral cord causing a severe PIP joint contracture. What is the typical anatomic relationship of the neurovascular bundle to the spiral cord?
Explanation
Question 35
A 32-year-old rugby player presents with an inability to actively flex the DIP joint of his right ring finger. Radiographs reveal a small bony avulsion fragment volar to the PIP joint. According to the Leddy-Packer classification, what is the appropriate management timeframe?
Explanation
Question 36
A 45-year-old male presents with acute, severe, unremitting right shoulder pain that started one week ago without trauma. The pain is now resolving, but he has noted profound weakness in shoulder abduction and external rotation. MRI of the cervical spine and shoulder are unremarkable. What is the most likely diagnosis?
Explanation
Question 37
A 28-year-old male undergoes exploration of the brachial plexus 4 months after a C5-C6 injury. A neuroma-in-continuity is identified at the upper trunk. Intraoperative nerve action potential (NAP) testing across the neuroma yields a positive response. What is the most appropriate next step?
Explanation
Question 38
A 22-year-old baseball batter reports chronic hypothenar hand pain and new-onset weakness in finger abduction and adduction. Sensory examination over the volar small finger is completely normal. Which of the following is the most likely site of neural compression?
Explanation
Question 39
A patient is asked to make an "OK" sign but instead pinches the pulp of the thumb to the pulp of the index finger. Which of the following muscles is most likely weak or paralyzed?
Explanation
Question 40
A 25-year-old motorcyclist sustains a traumatic brachial plexus injury.
Physical exam reveals intact rhomboid and serratus anterior function, but complete loss of shoulder abduction, elbow flexion, and wrist extension. Horner syndrome is absent. Which roots are most likely involved in this injury?
Explanation
Question 41
A 25-year-old motorcyclist sustains a severe traction injury to his right upper extremity. Examination reveals complete flaccid paralysis of the entire right arm, absent sensation, and right-sided ptosis and miosis. Which of the following nerve roots is most likely avulsed, portending a poor prognosis for spontaneous recovery of distal function?
Explanation
Question 42
A 22-year-old male sustains a C5-C6 root avulsion injury. At 4 months post-injury, he has no active elbow flexion but retains fully intact hand and wrist function. Which of the following is the most appropriate nerve transfer to restore elbow flexion?
Explanation
Question 43
A 45-year-old carpenter presents with aching pain in the volar forearm and numbness in the thumb, index, and middle fingers. Phalen's and Tinel's signs at the wrist are negative. Sensation is decreased over the thenar eminence. Which of the following structures is most likely compressing the affected nerve?
Explanation
Question 44
A 28-year-old rugby player felt a "pop" in his ring finger while grabbing an opponent's jersey. He cannot actively flex the distal interphalangeal (DIP) joint, but proximal interphalangeal (PIP) joint flexion is intact. The affected finger rests in extension compared to the other digits. Which zone of flexor tendon injury does this represent?
Explanation
Question 45
A 55-year-old diabetic female presents with a painful triggering of her right middle finger. She has failed a trial of splinting and one corticosteroid injection given 6 months ago. What is the most appropriate next step in management?
Explanation
Question 46
An infant presents with an absent grasp reflex and a claw hand deformity following a difficult delivery. Shoulder abduction and elbow flexion are fully intact. If a neuroma-in-continuity is identified during surgical exploration, which trunk of the brachial plexus is most likely involved?
Explanation
Question 47
A 32-year-old male presents with severe pain and swelling of his right index finger 2 days after a puncture wound. Examination reveals uniform swelling, a flexed posture, pain on passive extension, and tenderness along the tendon sheath. What is the standard surgical approach for irrigation and debridement?
Explanation
Question 48
A 40-year-old male develops sudden, severe right shoulder pain that wakes him at night. Two weeks later, the pain subsides, but he notices profound weakness in shoulder abduction and external rotation. MRI of the shoulder is unremarkable. EMG shows active denervation in the supraspinatus and infraspinatus without radicular findings. What is the most likely diagnosis?
Explanation
Question 49
A 60-year-old mechanic presents with chronic wrist pain. Radiographs reveal scapholunate interval widening, radioscaphoid arthritis, and capitolunate arthritis. The radiolunate joint is completely spared. What stage of SLAC (Scapholunate Advanced Collapse) wrist does this represent, and what is an appropriate surgical option?
Explanation
Question 50
A 65-year-old female presents with severe pain at the base of her thumb. Radiographs show Eaton-Littler Stage III trapeziometacarpal arthritis with significant subluxation and a 40-degree hyperextension deformity of the metacarpophalangeal (MCP) joint. In addition to a trapeziectomy and LRTI, what additional procedure must be performed?
Explanation
Question 51
A 48-year-old cellist presents with progressive weakness and clumsiness in his left hand. Examination reveals profound atrophy of the first dorsal interosseous muscle, weakness in finger abduction, and a positive Froment's sign. Which nerve and site of compression are most likely responsible?
Explanation
Question 52
A 35-year-old male presents with a persistent left radial nerve palsy 18 months after a humeral shaft fracture. To optimally restore wrist extension without causing excessive radial deviation, which of the following tendon transfers is most commonly performed?
Explanation
Question 53
A 26-year-old elite volleyball player complains of vague posterior shoulder pain and weakness. Examination shows atrophy isolated to the infraspinatus fossa, with normal supraspinatus bulk and strength. An MRI reveals a paralabral cyst. Where is the most likely location of the nerve compression?
Explanation
Question 54
A 25-year-old motorcyclist sustains a severe traction injury to his right brachial plexus. Clinical examination demonstrates a flail, anesthetic right arm, as well as right-sided ptosis, miosis, and anhidrosis. An MRI reveals pseudomeningoceles at the C7, C8, and T1 levels. What is the most likely electrodiagnostic finding 4 weeks post-injury in the affected C8/T1 dermatomes?
Explanation
Question 55
A 30-year-old male presents with a persistent C5-C6 upper trunk brachial plexus injury 6 months after a fall. Examination reveals 0/5 strength in elbow flexion and shoulder abduction, but hand function is fully preserved (5/5). Which of the following nerve transfers is most appropriate to restore elbow flexion in this patient?
Explanation
Question 56
A 42-year-old carpenter sustains a puncture wound to his index finger. Two days later, he presents with the finger held in slight flexion, symmetric fusiform swelling of the digit, tenderness along the entire flexor tendon sheath, and severe pain with passive extension. Which of the following is the most appropriate immediate management?
Explanation
Question 57
A 28-year-old elite volleyball player complains of vague posterior shoulder pain and weakness. Examination reveals isolated atrophy of the infraspinatus muscle with normal bulk and strength of the supraspinatus. Where is the most likely location of the nerve compression?
Explanation
Question 58
A 35-year-old female presents with sudden, excruciating pain in her right shoulder that awakened her from sleep. The severe pain lasts for one week and is followed by profound weakness in shoulder abduction and external rotation, though the pain has now largely resolved. What is the most likely diagnosis?
Explanation
Question 59
A 34-year-old basketball player presents 3 weeks after jamming his ring finger. Examination reveals PIP joint flexion and DIP joint hyperextension.
Which of the following anatomic structures is primarily injured in this deformity?
Explanation
Question 60
A 22-year-old male fell on an outstretched hand 6 months ago but did not seek medical attention. He now presents with dorsal radial wrist pain. Radiographs demonstrate a scaphoid nonunion with a radiocarpal angle of 20 degrees and a scapholunate angle of 85 degrees.
What deformity pattern has developed in this patient's wrist?
Explanation
Question 61
A 45-year-old boxer presents with pain and swelling over the third metacarpophalangeal (MCP) joint after a punch. When he attempts to extend his fingers from a fist, the middle finger lags, and the extensor tendon snaps into the valley between the third and fourth metacarpal heads. Which of the following is the most likely diagnosis?
Explanation
Question 62
A 29-year-old female presents with vague right arm paresthesias, subjective weakness, and coldness in her hand, particularly when reaching overhead. Adson's test is positive, and cervical spine radiographs reveal an accessory cervical rib. Compression of which specific neurovascular structures is most likely responsible for her clinical presentation?
Explanation
None
