ABOS & OITE Orthopaedic Exam Questions: Biceps, Osteosarcoma, Tarsal Coalitions | Part 21551

Key Takeaway
This orthopaedic board review module offers 30 advanced multiple-choice questions mirroring ABOS Part I and AAOS OITE exams. It covers high-yield topics like distal biceps tendon rupture, osteosarcoma, and tarsal coalitions, detailing diagnosis, surgical techniques, and post-operative rehabilitation. Ideal for comprehensive exam preparation.
ABOS & OITE Orthopaedic Exam Questions: Biceps, Osteosarcoma, Tarsal Coalitions | Part 21551
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 52-year-old male presents to the clinic 3 days after feeling a "pop" in his right elbow while lifting a heavy box. He reports immediate pain, followed by bruising and weakness. On examination, a palpable defect is noted in the distal arm, and he demonstrates weakness with resisted elbow flexion and supination. The image below shows the clinical appearance of his arm.
Explanation
Correct Answer: C
The case explicitly states under 'Pre-Operative Planning & Patient Positioning' that the "Hook Test" is highly sensitive and specific: inability to hook a finger under the intact distal biceps tendon from the lateral side of the cubital fossa is indicative of a complete rupture. While ecchymosis, weakness with resisted elbow flexion, a palpable defect, and the 'Popeye' sign (increased prominence of the biceps muscle belly proximally, as seen in the image) are all important clinical findings suggestive of a distal biceps tendon rupture, the Hook Test provides the most definitive clinical confirmation due to its high sensitivity and specificity.
Question 2
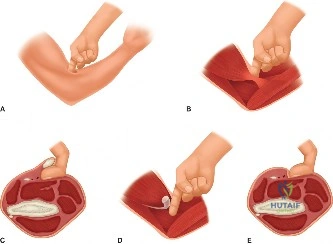
A 48-year-old male undergoes a single-incision anterior repair for an acute distal biceps tendon rupture. During the procedure, the surgeon is meticulously dissecting through the subcutaneous tissue and fascia in the antecubital fossa.

Explanation
Correct Answer: D
The 'Surgical Anatomy & Biomechanics' section highlights key anatomical structures in close proximity and at risk during surgical approaches. It specifically states: "Lateral Antebrachial Cutaneous Nerve (LACN): A terminal branch of the musculocutaneous nerve, the LACN provides sensation to the radial forearm and typically pierces the deep fascia between the biceps and brachialis muscles. It lies superficially and is susceptible to injury during skin incision and subcutaneous dissection." The PIN, Median Nerve, and main trunk of the Radial Nerve are deeper structures, at risk during deeper dissection or tunnel drilling, but not typically during the initial skin incision and subcutaneous tissue dissection. The Ulnar nerve is located medially and posteriorly to the cubital fossa and is not typically at risk with an anterior approach to the distal biceps.
Question 3
During a single-incision anterior repair of a distal biceps tendon rupture, the surgeon has retrieved the retracted tendon and is preparing the radial tuberosity for fixation. The image below depicts a surgical field during such a procedure.
Explanation
Correct Answer: D
The 'Surgical Approach & Technique' section, under 'Protection of the Radial Nerve (PIN)', explicitly states: "With the forearm in full pronation, the posterior interosseous nerve (PIN)... moves away from the surgical field, typically posterior to the radial tuberosity and deep to the supinator muscle. This maneuver increases the distance between the PIN and the radial tuberosity. A deep, blunt Hohmann or cobra retractor is placed beneath the brachioradialis and supinator, hugging the anterior surface of the radius, retracting the muscle belly laterally to expose the radial tuberosity. This retractor acts as a physical barrier, protecting the PIN from drilling and reaming." Maintaining full extension or supination would place the PIN at greater risk. While protecting the brachial artery is important, it is done with careful medial retraction, not specifically for PIN protection. Identifying and dissecting the PIN proximally is not the primary protective maneuver during tuberosity preparation.
Question 4
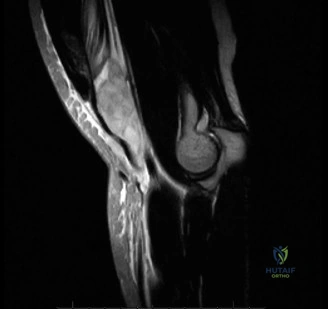
A 68-year-old sedentary male presents with a complete distal biceps tendon rupture sustained 8 weeks prior. He reports mild discomfort but states he can manage most daily activities without significant difficulty, as he primarily uses his left arm for heavier tasks. He has a history of severe coronary artery disease and is on multiple anti-coagulants. MRI confirms a complete rupture with 4 cm of tendon retraction.
Which of the following is the most appropriate initial management strategy for this patient?
Explanation
Correct Answer: C
The 'Indications & Contraindications' section clearly outlines criteria for non-operative management. This patient fits several key indications: "Low-Demand Patients: Sedentary individuals who do not require maximal supination or flexion strength for their daily activities." and "Significant Medical Comorbidities: Patients with severe systemic illnesses that preclude safe surgical intervention (e.g., uncontrolled diabetes, severe cardiovascular or pulmonary disease)." Additionally, his injury is chronic (8 weeks) with significant retraction, making delayed repair more complex and potentially less predictable, especially given his comorbidities. Acute repair is not possible at 8 weeks. Nerve conduction studies are not indicated unless there is a specific neurological deficit.
Question 5
A 42-year-old construction worker undergoes an acute single-incision anterior repair of a distal biceps tendon rupture. Postoperatively, he develops persistent numbness and dysesthesia along the radial aspect of his forearm. Physical examination confirms diminished sensation in this distribution. Motor function is intact.
Which of the following complications is most likely responsible for his symptoms?
Explanation
Correct Answer: C
The 'Complications & Management' section details neurological injuries. It states: "Lateral Antebrachial Cutaneous Nerve (LACN) injury... Management: Usually neuropraxia/neuroma, leading to numbness/dysesthesia in radial forearm." The PIN is a motor nerve, and its injury would primarily cause motor deficits (e.g., wrist or finger extensor weakness), not sensory changes in the radial forearm. Median nerve compression would affect sensation in the thumb, index, middle, and radial half of the ring finger, and potentially motor function of the thenar muscles. A brachial artery pseudoaneurysm would present with pulsatile mass, pain, and potentially ischemia. Heterotopic ossification is the formation of bone in soft tissues and would cause pain and stiffness, not isolated sensory deficits.
Question 6
A 38-year-old athlete undergoes a single-incision distal biceps tendon repair with cortical button fixation. According to the standard post-operative rehabilitation protocol described in the case, what is the most appropriate activity during the initial 2 weeks (Phase I)?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols' section, under 'Phase I Protection & Early Motion', specifies: "Passive Elbow Flexion/Extension: 30-90 degrees for the first 2 weeks, progressing to 15-115 degrees by week 4. Therapist-assisted, non-weight-bearing." It also explicitly states: "Avoid resisted supination" and "No weight bearing through the affected arm. Avoid lifting anything heavier than a cup of coffee." Unrestricted active pronation and supination are also not allowed in Phase I, with supination often restricted to a limited passive range (e.g., 0-30 degrees) to protect the repair.
Question 7
A 55-year-old male sustains a complete distal biceps tendon rupture. He opts for non-operative management due to personal preference and a sedentary lifestyle. Based on the biomechanical principles outlined in the case, what is the most significant functional deficit he is likely to experience?
Explanation
Correct Answer: D
The 'Surgical Anatomy & Biomechanics' section clearly states: "Biomechanically, the distal biceps tendon is the primary supinator of the forearm, contributing approximately 80% of supination power, particularly against resistance." It further notes that "Loss of this insertion leads to substantial functional deficits, especially for activities requiring powerful supination, such as using a screwdriver, turning a doorknob, or lifting heavy objects with the palm up." While it also contributes to elbow flexion (30-40%), the loss of supination strength (often 40-50%) is highlighted as the most significant functional deficit. The biceps is not a primary elbow extensor, pronator, or wrist flexor, nor does it directly contribute significantly to grip strength.
Question 8
A surgeon is discussing options for distal biceps tendon repair with a 40-year-old patient. The patient is concerned about potential complications, particularly heterotopic ossification (HO). Based on the literature review in the case, which statement regarding surgical approaches and HO risk is most accurate?
Explanation
Correct Answer: B
The 'Key Literature & Guidelines Summary' section explicitly addresses this comparison: "Two-Incision Approach (Boyes-O'Brien): Historically popular... However, it is associated with a higher incidence of heterotopic ossification (up to 20%), a major complication limiting range of motion." In contrast, for the single-incision approach, it states: "This approach has gained widespread acceptance due to lower rates of heterotopic ossification and comparable functional outcomes." Therefore, the two-incision approach has a higher incidence of HO. Prophylactic NSAIDs are used for HO prevention regardless of the approach, and HO is a known complication related to soft tissue dissection and hematoma, not primarily the fixation method.
Question 9
A surgeon is performing a distal biceps tendon repair. After retrieving the tendon, they note its unique twisted morphology. Which statement accurately describes the anatomical insertion of the biceps tendon fibers onto the radial tuberosity?
Explanation
Correct Answer: D
The 'Surgical Anatomy & Biomechanics' section describes the unique twist of the distal biceps tendon: "This twist results in the short head fibers inserting more distally and anteriorly on the radial tuberosity, and the long head fibers inserting more proximally and posteriorly." It also clarifies the insertion point: "The distal biceps tendon inserts onto the roughened, ulnar-sided aspect of the radial tuberosity." Therefore, options A, B, C, and E are incorrect based on this detailed anatomical description.
Question 10
A 50-year-old active male presents 6 weeks after sustaining a complete distal biceps tendon rupture. He initially tried conservative management but now desires surgical repair due to persistent weakness impacting his work. MRI shows significant tendon retraction and early muscle atrophy.
What is the most likely implication of this delayed presentation on the surgical repair?
Explanation
Correct Answer: C
The 'Key Literature & Guidelines Summary' section, under 'Timing of Surgery', states: "Acute repair (ideally within 2-3 weeks of injury) is strongly advocated. Delayed repairs (beyond 4-6 weeks) are technically more challenging due to tendon retraction, scarring, and muscle atrophy, often requiring extensive dissection, tendon lengthening procedures (V-Y plasties), or allograft/autograft augmentation." Therefore, a 6-week delayed presentation with significant retraction and atrophy will increase the technical difficulty of the repair and may necessitate additional reconstructive techniques. It does not reduce HO risk, make retrieval easier, increase the likelihood of successful non-operative management for an active patient, or decrease radial nerve injury risk (in fact, extensive dissection in chronic cases can increase nerve risk).
Question 11
A 14-year-old male presents with a 5-month history of progressive left knee and distal thigh pain. Initially, the pain was intermittent and activity-related, but over the preceding eight weeks, it transitioned to constant, severe nocturnal pain that consistently awakened him from sleep and was refractory to over-the-counter medications. Concurrently, a slowly enlarging, firm, non-mobile soft tissue mass was noted on the anterior and lateral aspects of the distal left thigh. Which of the following clinical findings, if present, would be MOST concerning for a malignant etiology in this patient?
Explanation
Correct Answer: C
The case explicitly highlights that the transition of pain from activity-dependent to constant, severe nocturnal pain that awakens the patient from sleep is a critical clinical indicator of an aggressive, space-occupying intramedullary process causing endosteal pressure and periosteal stretching. While the presence of a growing, firm mass is also highly concerning, the evolution of pain to include a severe nocturnal component is a classic red flag for primary malignant bone tumors in the pediatric and adolescent population. Options A and B describe the initial, less concerning symptoms that are often misattributed to benign causes. Option D, the absence of constitutional symptoms, is not a reliable indicator to rule out malignancy, as many sarcomas do not present with systemic symptoms. Option E, mild disuse atrophy, is a secondary effect of pain and functional limitation, not a primary indicator of malignancy itself.
Question 12
During the physical examination of the 14-year-old male with a distal femoral mass, the orthopedic oncologist notes a prominent network of engorged superficial veins overlying the mass, increased local skin temperature, and a positive patellar tap test. Which of these findings, in isolation, is LEAST specific for a high-grade malignant bone tumor?
Explanation
Correct Answer: E
A positive patellar tap test indicates the presence of a knee joint effusion. While a reactive effusion can occur secondary to an adjacent malignant bone tumor (as noted in the case), it is a non-specific finding. Joint effusions can be caused by a wide range of conditions, including trauma, infection, inflammatory arthritis, and other benign processes. In contrast, prominent, engorged superficial veins (neoangiogenesis), increased local skin temperature (increased metabolic activity), a firm and unyielding mass fixed to bone, and ill-defined margins suggesting extraosseous extension are all highly characteristic clinical signs of an aggressive, rapidly growing malignant bone tumor like osteosarcoma.
Question 13
A 14-year-old male presents with progressive left knee pain and a distal femoral mass. Initial plain radiographs of the left distal femur are shown below.
Based on these images and the clinical presentation, which of the following radiographic features is MOST characteristic of the likely diagnosis?

Explanation
Correct Answer: C
The plain radiographs in the case description explicitly detail a 'prominent 'sunburst' or 'hair-on-end' periosteal reaction' and a 'distinct Codman's triangle' along with a mixed lytic and blastic appearance and cortical destruction. These features are classic radiographic hallmarks of osteosarcoma, indicating a rapidly aggressive tumor that is lifting the periosteum and producing new bone in a disorganized fashion. Options A and E describe features more typical of benign or less aggressive lesions (e.g., non-ossifying fibroma, fibrous dysplasia). Option B ('soap bubble' appearance) is characteristic of giant cell tumor or aneurysmal bone cyst. Option D ('onion-skin' periosteal reaction) is a classic feature of Ewing sarcoma, which typically presents with a permeative lytic pattern and is often diaphyseal or metadiaphyseal.
Question 14
Following the concerning plain radiographic findings, a contrast-enhanced MRI of the entire left femur, including the hip and knee joints, was performed. Which of the following critical pieces of information, essential for surgical planning, is BEST provided by the MRI in this case?
Explanation
Correct Answer: D
MRI is considered the gold standard for local staging of primary bone sarcomas. As detailed in the case, it is crucial for accurately defining the intramedullary extent of the tumor (to plan the proximal osteotomy level), assessing the full extent of soft tissue involvement, and critically evaluating the relationship of the tumor to adjacent neurovascular bundles. This information directly dictates the feasibility of limb-salvage surgery and guides the surgical approach to achieve clear margins while preserving vital structures. Option A is achieved by histopathological biopsy. Option B is best characterized by CT scan. Options C and E are assessed by systemic staging studies, specifically chest CT for pulmonary metastases and PET-CT or Technetium 99m bone scan for distant osseous metastases.
Question 15
An image-guided core needle biopsy was performed on the distal femoral mass. The histopathological report subsequently confirmed the diagnosis of High Grade Conventional Osteoblastic Osteosarcoma. Which of the following microscopic findings is the definitive diagnostic feature for this specific tumor?
Explanation
Correct Answer: C
The case explicitly states that the 'defining diagnostic feature was the presence of malignant cells directly producing fine, lace-like, unmineralized osteoid matrix.' This is the pathognomonic feature of osteosarcoma. Option A describes Ewing sarcoma. Option B describes chondrosarcoma. Option D describes Langerhans Cell Histiocytosis (Eosinophilic Granuloma). Option E describes fibrosarcoma or malignant fibrous histiocytoma (now often classified as undifferentiated pleomorphic sarcoma), which are less common in this age group and location for primary bone tumors.
Question 16
Considering the patient's age, clinical presentation, and initial radiographic findings, the orthopedic oncologist included Ewing Sarcoma in the differential diagnosis. Which of the following features would most strongly argue AGAINST a diagnosis of Ewing Sarcoma in this specific patient?
Explanation
Correct Answer: B
The case describes the lesion as 'centered within the distal femoral metaphysis.' While Ewing sarcoma can occur in adolescents and present with a large soft tissue mass, its classic radiographic location is diaphyseal or metadiaphyseal, in contrast to osteosarcoma which is typically metaphyseal. The absence of constitutional symptoms (Option D) also argues against Ewing sarcoma, which often presents with systemic symptoms mimicking infection, but the metaphyseal location (Option B) is a more direct and strong radiographic differentiator from the typical Ewing presentation. Options A, C, and E are all features that can be seen with Ewing sarcoma, thus not arguing against it.
Question 17
Based on the comprehensive staging workup, including histopathology and systemic imaging, the patient's tumor was classified using the Enneking Surgical Staging System. Given the findings described in the case, what was the correct Enneking stage, and what is its primary implication for treatment?
Explanation
Correct Answer: D
The case explicitly states: 'The tumor was classified using the Enneking Surgical Staging System for Musculoskeletal Sarcomas. Grade (G): High grade (G2)... Site (T): Extracompartmental (T2)... Metastasis (M): No regional or distant metastasis identified (M0). Therefore, the patient was staged as Enneking Stage IIB (High grade, extracompartmental, without metastasis). This stage dictates an aggressive, multimodal treatment paradigm.' This stage signifies a high-grade tumor that has extended beyond the bone cortex into surrounding soft tissues but has not metastasized, requiring a comprehensive approach involving both systemic chemotherapy and definitive wide surgical resection to achieve local control and address potential micrometastatic disease.
Question 18
The patient was initiated on a standard multi-agent neoadjuvant chemotherapy regimen (MAP protocol). Which of the following is NOT a primary rationale for administering neoadjuvant chemotherapy in this patient's treatment plan?
Explanation
Correct Answer: D
The definitive diagnosis of osteosarcoma is established through histopathological biopsy before the initiation of neoadjuvant chemotherapy. The case clearly states: 'Following the definitive histopathological diagnosis and completion of the staging workup, the patient's case was presented at the institutional multidisciplinary sarcoma tumor board,' and then 'The patient was initiated on a standard multi-agent neoadjuvant chemotherapy regimen.' The other options (A, B, C, E) are all well-established rationales for neoadjuvant chemotherapy in high-grade osteosarcoma: targeting micrometastases, achieving tumor cytoreduction, evaluating prognostic histologic response, and potentially making limb-salvage surgery easier and safer by shrinking the tumor.
Question 19
Following neoadjuvant chemotherapy, the patient underwent restaging MRI, which demonstrated a reduction in peritumoral edema and no evidence of neurovascular encasement. Given the patient's age, skeletal maturity, and family preference, limb salvage with wide en bloc resection and modular distal femoral replacement was chosen. Which of the following factors was a primary reason *against* recommending a rotationplasty (Van Nes procedure) in this specific patient?
Explanation
Correct Answer: D
The case states that rotationplasty 'was discussed extensively with the patient and family, but they opted for endoprosthetic reconstruction' and that it 'is associated with significant cosmetic and psychological challenges.' This indicates that the patient and family's preference, influenced by the cosmetic and psychological impact, was the primary reason it was not chosen, despite its functional advantages. Option A is incorrect; rotationplasty offers excellent long-term durability, often superior to endoprostheses, especially in young, active patients. Option B is incorrect; the restaging MRI showed no neurovascular encasement, making limb salvage (including rotationplasty) feasible. Option C is incorrect; rotationplasty is an oncologically sound procedure that allows for wide margins. Option E is incorrect; rotationplasty generally has a lower risk of long-term mechanical failure, aseptic loosening, and deep infection compared to massive endoprostheses.
Question 20
During the definitive limb-salvage surgery for the distal femoral osteosarcoma, the surgical team implemented several critical principles. Which of the following intraoperative steps was performed primarily to ensure oncologic safety and guide the extent of resection?
Explanation
Correct Answer: D
Obtaining a sample of the proximal intramedullary canal marrow for immediate intraoperative frozen section analysis is a critical step to ensure oncologic safety. This allows the surgeon to confirm the absence of malignant cells at the planned proximal osteotomy margin, thereby verifying that a wide osseous margin has been achieved. If tumor cells were present, the osteotomy level would need to be extended more proximally. Option A describes a safety measure for hemorrhage control, not directly for oncologic margin assessment. Option B describes the surgical approach, which is important for exposure and excising the biopsy tract, but not directly for guiding the extent of bone resection. Option C describes neurovascular protection, which is crucial for limb preservation but not for defining tumor margins. Option E describes the type of distal resection, which is part of achieving a wide margin, but the frozen section specifically guides the proximal bone cut based on microscopic tumor extent.
Question 21
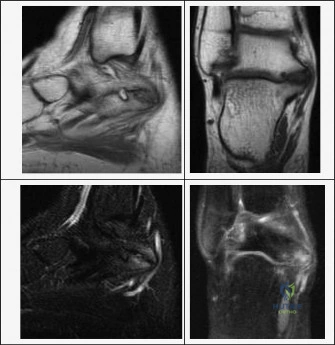
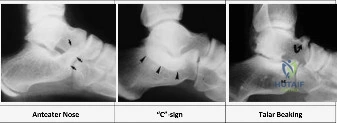
A 14-year-old male presents with a 6-month history of progressive right ankle pain, particularly with activity, and a rigid flatfoot deformity. He reports difficulty walking on uneven surfaces and occasional "giving way" sensations. Physical examination reveals limited subtalar motion and tenderness over the sinus tarsi. Radiographs show a "C-sign." Which of the following is the MOST likely diagnosis and its typical age of symptomatic presentation?
Explanation
Correct Answer: D
The patient's age (14 years), presentation of progressive ankle pain with a rigid flatfoot, limited subtalar motion, and the presence of a "C-sign" on radiographs are all classic indicators of a talocalcaneal (TC) coalition. The case states that TC coalitions most frequently involve the middle facet of the subtalar joint, ossify later, and typically present between the ages of 12 and 16 years. The "C-sign" is a radiographic finding specific to talocalcaneal coalitions, representing continuity of the talar dome and sustentaculum tali. Calcaneonavicular (CN) coalitions typically ossify and become symptomatic earlier, between the ages of 8 and 12 years, and are associated with the "anteater nose sign." While juvenile idiopathic arthritis can cause pediatric subtalar pain, the specific radiographic sign and age of presentation strongly point to a TC coalition.
Question 22
A 10-year-old patient is diagnosed with a tarsal coalition affecting the subtalar joint, leading to restricted hindfoot motion. Based on the normal biomechanics of the subtalar joint as depicted in the provided image and described in the case, which of the following statements accurately describes the coupled motion of the subtalar joint?

Explanation
Correct Answer: C
The case explicitly states that the subtalar joint functions as a single-axis hinge, and its unique orientation dictates that motion occurs as a coupled mechanism: inversion is coupled with plantarflexion and internal rotation of the foot (supination), while eversion is coupled with dorsiflexion and external rotation (pronation). Therefore, option C accurately describes the coupled motion of inversion. Options A, B, and D describe incorrect couplings. Option E is incorrect as subtalar motion involves a complex triplanar motion, not primarily abduction and adduction in a single plane.
Question 23
A 13-year-old female presents with chronic left hindfoot pain and a rigid flatfoot. Initial radiographs show an "anteater nose sign." To definitively characterize the coalition and plan for potential surgical intervention, which imaging modality is considered the gold standard, and what specific information does it provide that is crucial for surgical decision-making?
Explanation
Correct Answer: C
The case identifies Computed Tomography (CT) as the gold standard for mapping the exact three-dimensional anatomy of the coalition. For talocalcaneal (TC) coalitions, coronal CT slices perpendicular to the posterior facet are critical for calculating the percentage of joint surface involved. This information is crucial because a coalition involving more than 50% of the posterior facet surface area is generally considered a contraindication to simple resection, necessitating subtalar arthrodesis instead. While MRI can differentiate between fibrous and cartilaginous coalitions (Option B), and plain radiographs provide initial clues like the "anteater nose sign" (for CN coalitions) or "C-sign" (for TC coalitions) (Option A), CT provides the definitive bony detail and quantitative assessment vital for surgical planning. Bone scans and ultrasound are not the primary modalities for definitive structural characterization of tarsal coalitions.
Question 24
A 15-year-old male has a symptomatic talocalcaneal coalition that has failed 6 months of conservative management. Preoperative CT scans reveal a bony coalition involving 60% of the posterior facet of the subtalar joint, with early degenerative changes noted in the remaining posterior facet. Based on the provided table of indications and contraindications, what is the MOST appropriate surgical recommendation for this patient?
Explanation
Correct Answer: C
The case explicitly states that a talocalcaneal (TC) coalition involving more than 50% of the posterior facet surface area is generally considered a contraindication to simple resection, as the remaining joint will likely be unstable and degenerate rapidly. In such cases, subtalar arthrodesis is indicated. The patient's CT scan shows 60% involvement of the posterior facet, exceeding this critical threshold. Furthermore, early degenerative changes are present, which also favors arthrodesis over resection. Options A and B are incorrect as they describe resection, which is contraindicated here. Option D is incorrect as conservative management has already failed. Option E, triple arthrodesis, would be considered if there were severe arthrosis involving the Chopart joint (talonavicular and calcaneocuboid joints) in addition to the subtalar joint, which is not fully described here, making subtalar arthrodesis the more direct and appropriate choice for isolated severe subtalar pathology.
Question 25
During a calcaneonavicular coalition resection in a 10-year-old patient, the surgeon makes an Ollier-type incision. After elevating the extensor digitorum brevis (EDB) muscle and exposing the coalition, as shown in the image, the resection is performed. Which of the following is a critical step to prevent recurrence and a common error to avoid during this procedure?

Explanation
Correct Answer: A
For calcaneonavicular (CN) coalition resection, the case highlights that the resection must be generous, extending proximally to the normal anterior calcaneal wall, distally to the normal navicular surface, and crucially, medially to the talar head. It explicitly states, "A common error is incomplete medial resection." This incomplete resection is a significant factor in recurrence. Options B, D, and E describe considerations for a medial approach (posterior tibial nerve, FHL interposition, posterior facet protection), which is used for talocalcaneal coalitions, not CN. Option C is incorrect; a generous resection is required, and the 50% rule applies to talocalcaneal coalitions, not CN.
Question 26
A 14-year-old patient undergoes a medial approach for a talocalcaneal coalition resection. After incising the flexor retinaculum, the surgeon identifies and retracts the posterior tibial tendon superiorly and the flexor digitorum longus tendon inferiorly. Which critical structure lies posterior and inferior to the FDL and must be meticulously protected throughout the case?
Explanation
Correct Answer: D
The case describes the detailed surgical approach for a talocalcaneal (TC) coalition, which requires a medial incision. During deep dissection, after identifying and retracting the posterior tibial tendon (PTT) superiorly and the flexor digitorum longus (FDL) tendon inferiorly, the text explicitly states: "The neurovascular bundle (posterior tibial artery and tibial nerve) lies posterior and inferior to the FDL and must be meticulously protected throughout the case." Options A and B (sural nerve, intermediate dorsal cutaneous nerve) are associated with the lateral approach for CN coalitions. Option C (peroneal artery) is not the primary neurovascular structure at risk in this specific medial approach. Option E (flexor hallucis longus tendon) runs directly beneath the sustentaculum tali and is identified, but the neurovascular bundle is the critical structure posterior and inferior to the FDL.
Question 27
A 12-year-old patient undergoes a calcaneonavicular coalition resection via a lateral Ollier approach. Two weeks postoperatively, the patient complains of numbness and burning pain along the lateral aspect of the foot and ankle, extending to the little toe. Based on the provided table of complications, which nerve is MOST likely injured, and what is the primary preventative measure?
Explanation
Correct Answer: B
The patient underwent a calcaneonavicular (CN) coalition resection via a lateral Ollier approach. The symptoms of numbness and burning pain along the lateral aspect of the foot and ankle, extending to the little toe, are characteristic of sural nerve injury. The complications table specifically lists "Sural Nerve Injury" with an incidence of 2%-5% as an etiology of "Retraction injury or direct laceration during the lateral Ollier approach." The primary preventative measure listed is "Careful blunt dissection in the subcutaneous tissues; minimal retraction tension." Options A, D, and E describe other nerves or approaches. Option C, intermediate dorsal cutaneous nerve, is also at risk during a lateral approach but typically affects the dorsum of the foot, not specifically extending to the little toe, and the sural nerve is more commonly implicated in this specific symptom distribution following a lateral hindfoot incision.
Question 28
A 13-year-old patient is 2 weeks post-operative from a successful talocalcaneal coalition resection with fat graft interposition. The wound is healing well, and sutures have been removed. What is the MOST critical next step in the rehabilitation protocol to prevent recurrence and optimize long-term outcomes?
Explanation
Correct Answer: C
The case's Postoperative Rehabilitation Protocols section emphasizes the importance of early motion. In Phase II (Weeks 2-6), it states: "Crucially, active and active-assisted range of motion (ROM) exercises of the subtalar and ankle joints are initiated immediately. The patient is instructed to perform inversion, eversion, dorsiflexion, and plantarflexion exercises multiple times daily. This early mobilization is the most critical non-surgical step in preventing the recurrence of a fibrous or bony coalition." Options A, B, D, and E are either too aggressive, too restrictive, or premature for this stage of rehabilitation.
Question 29
A 16-year-old patient, 18 months status post-talocalcaneal coalition resection, presents with persistent, debilitating hindfoot pain and progressive valgus deformity. A repeat CT scan shows an adequate initial resection but significant degenerative arthrosis of the posterior facet and early arthritic changes in the talonavicular joint. Non-operative measures have failed. What is the MOST appropriate salvage procedure for this patient?
Explanation
Correct Answer: D
The patient presents with persistent, debilitating pain and progressive valgus deformity after a talocalcaneal (TC) coalition resection. The CT scan reveals significant degenerative arthrosis of the posterior facet AND early arthritic changes in the talonavicular joint. The case's "Management of Persistent Pain" section states: "If the resection was adequate, the pain is likely secondary to advanced degenerative arthrosis of the posterior facet or the transverse tarsal joints. In these scenarios, the salvage procedure of choice is a subtalar arthrodesis. If the Chopart joint is also severely arthritic, a triple arthrodesis (subtalar, talonavicular, and calcaneocuboid) may be necessary to provide a stable, plantigrade, and pain-free foot." Since the talonavicular joint (part of the Chopart joint) is involved with early arthritic changes in addition to the posterior facet arthrosis, a triple arthrodesis is the most comprehensive and appropriate salvage procedure to address all affected joints and provide a stable, pain-free hindfoot. Subtalar arthrodesis (Option C) would only address the subtalar joint, leaving the talonavicular arthrosis untreated. Options A, B, and E are not indicated for advanced arthrosis.
Question 30
The understanding and surgical management of tarsal coalitions have been significantly influenced by foundational studies. Which of the following statements accurately attributes a key contribution to the specified researcher or group?
Explanation
Correct Answer: C
The "Summary of Key Literature and Guidelines" section directly attributes the following: Wilde et al. "contributed significantly to the understanding of the middle facet's role in TC coalitions, detailing the medial approach and the importance of preserving the FHL tendon and the neurovascular bundle."
- Option A is incorrect: Mubarak and colleagues established the 50% posterior facet involvement rule for TC coalitions. Cowell's work focused on CN coalitions.
- Option B is incorrect: Cowell's seminal work established the lateral approach and EDB interposition for CN coalitions.
- Option D is incorrect: Modern literature supports the use of interposition grafts (EDB, fat, FHL) to prevent recurrence. Simple resection alone is associated with higher recurrence rates.
- Option E is incorrect: Current guidelines recommend an initial trial of non-operative management for all newly diagnosed, non-arthritic tarsal coalitions.
Question 31
A 14-year-old boy presents with a painful, rigid flatfoot and a history of recurrent ankle sprains. Subtalar motion is markedly limited. A continuous 'C' sign is observed on the lateral foot radiograph. Which of the following is the most accurate anatomical description of the most likely diagnosis?
Explanation
Question 32
A 32-year-old male undergoes a single-incision anterior repair of a distal biceps tendon rupture. Postoperatively, he notes numbness over the radial aspect of his volar forearm. Injury to which of the following structures is the most likely cause?
Explanation
Question 33
A 16-year-old male undergoes neoadjuvant chemotherapy followed by surgical resection for conventional osteosarcoma of the distal femur. Which of the following histological findings in the resected specimen is the most significant predictor of long-term survival?
Explanation
Question 34
Non-operative management of a complete distal biceps tendon rupture typically results in the greatest permanent deficit in which of the following upper extremity functions?
Explanation
Question 35
A 9-year-old boy presents with frequent ankle sprains and a rigid, spastic flatfoot. A 45-degree internal oblique radiograph of the foot reveals an 'anteater nose' sign. If conservative management fails, what is the preferred surgical intervention to prevent recurrence after resection?
Explanation
Question 36
Which of the following genetic syndromes is characterized by a mutation in the RECQL4 helicase gene, presenting with poikiloderma and an increased risk of developing osteosarcoma?
Explanation
Question 37
A 28-year-old weightlifter presents with acute elbow pain and a positive 'hook test.' During surgical repair utilizing a modified two-incision technique, the surgeon must carefully avoid subperiosteal dissection of the ulna to minimize the risk of which complication?
Explanation
Question 38
A low-grade tumor arises from the posterior surface of the distal femur. Radiographs display a densely ossified mass with a broad-based attachment and a radiolucent cleft separating it from the underlying cortex. Which genetic alteration is most characteristic of this lesion?
Explanation
Question 39
In an adolescent patient with a confirmed talocalcaneal coalition, which of the following is considered an absolute contraindication to isolated surgical resection of the coalition?
Explanation
Question 40
During anatomical reattachment of the distal biceps tendon, the surgeon must consider its distinct two-bundle anatomy. Which of the following best describes the anatomical insertion and biomechanical function of the long head of the distal biceps?
Explanation
Question 41
A 15-year-old female presents with severe pain in her proximal tibia. Imaging demonstrates an aggressive, lytic lesion with cortical destruction. Biopsy reveals large, blood-filled cystic spaces lined by anaplastic, pleomorphic cells producing delicate lace-like osteoid. What is the most likely diagnosis?
Explanation
Question 42
A 12-year-old girl is suspected of having a calcaneonavicular coalition. Which specific radiographic view is considered most sensitive and specific for visualizing this pathology?
Explanation
Question 43
When performing a single-incision anterior approach for distal biceps tendon repair, blind placement of deep retractors laterally over the radial neck places which of the following structures at highest risk of iatrogenic injury?
Explanation
Question 44
An 18-year-old male presents with a slow-growing mass on the diaphyseal surface of his proximal tibia. Imaging reveals a broad-based, surface-dwelling lesion with perpendicular periosteal reactions. Biopsy demonstrates an intermediate-grade spindle cell proliferation with a predominantly chondroblastic matrix. What is the diagnosis?
Explanation
Question 45
A 45-year-old male presents 6 weeks after an acute distal biceps rupture. Surgical repair is attempted but the tendon is severely retracted and cannot be directly mobilized to the radial tuberosity. Which of the following is the most commonly utilized autograft option for reconstruction?
Explanation
Question 46
A 45-year-old male presents 3 months after feeling a pop in his anterior elbow. He has not sought prior medical attention. Examination reveals a positive hook test and proximal retraction of the muscle belly. If this patient elects for non-operative management, he will likely experience the greatest functional deficit in which of the following motions?
Explanation
Question 47
Which of the following is considered the most significant independent prognostic factor for long-term survival in a patient with conventional, non-metastatic high-grade intramedullary osteosarcoma?
Explanation
Question 48
A 10-year-old boy presents with a rigid flatfoot and recurrent ankle sprains. Radiographs reveal an 'anteater sign'. What is the most likely diagnosis?
Explanation
Question 49
During a single-incision anterior approach for a distal biceps tendon repair, the surgeon must be careful to protect a sensory nerve that exits the deep fascia just lateral to the biceps tendon. Injury to this nerve leads to numbness in what distribution?
Explanation
Question 50
A 28-year-old female presents with a slowly enlarging mass on the posterior aspect of her distal femur. Imaging shows a densely ossified mass attached to the posterior cortex by a broad base, with a radiolucent cleft separating a portion of the tumor from the underlying bone. Molecular analysis of this lesion is most likely to show amplification of which gene?
Explanation
Question 51
A 14-year-old male complains of medial hindfoot pain and frequent 'sprained ankles.' On examination, he has a rigid pes planovalgus foot with peroneal muscle spasm. A lateral radiograph demonstrates a 'C-sign.' This finding represents an osseous bridge between which two structures?
Explanation
Question 52
Which of the following complications is historically more common with a two-incision approach for distal biceps repair compared to a single-incision anterior approach?
Explanation
Question 53
A 16-year-old male presents with a destructive, lytic lesion in the proximal tibia. MRI reveals multiple fluid-fluid levels within the lesion. Biopsy demonstrates highly pleomorphic, atypical cells directly producing osteoid. What is the most likely diagnosis?
Explanation
Question 54
A 15-year-old patient with a symptomatic talocalcaneal coalition has failed 6 months of non-operative management. CT scan reveals that the coalition involves 60% of the posterior facet. What is the most appropriate surgical management?
Explanation
Question 55
When restoring the anatomical footprint during a distal biceps tendon repair, the tendon should be reattached to which specific aspect of the radial tuberosity to maximize supination strength?
Explanation
Question 56
A 12-year-old child who was treated for bilateral retinoblastoma as an infant presents with a painful mass in the distal femur. Biopsy confirms osteosarcoma. This patient's condition is most strongly associated with a germline mutation in which chromosome?
Explanation
Question 57
Which muscle is most commonly utilized for interposition grafting after resection of a symptomatic calcaneonavicular coalition to prevent recurrence?
Explanation
Question 58
A 45-year-old weightlifter feels a sharp pop in his elbow. On physical exam, the physician is unable to hook their index finger under the lateral edge of the biceps tendon when the patient's elbow is actively flexed to 90 degrees and supinated. This clinical test evaluates the integrity of what structure?
Explanation
Question 59
Which of the following variants of osteosarcoma is characterized as an intermediate-grade, chondroblastic surface lesion that typically presents on the diaphyseal surface of the tibia or femur?
Explanation
Question 60
A patient is evaluated for an acute complete distal biceps rupture. If the surgeon decides to proceed with an anatomic repair, failure to fully release which of the following structures may limit mobilization of the retracted tendon?
Explanation
Question 61
A 50-year-old male presents with a chronic distal biceps rupture that occurred 3 months ago. Intraoperatively, the tendon is found to be severely retracted and cannot be mobilized to the radial tuberosity even with the elbow flexed. Which of the following is the most appropriate reconstruction option?
Explanation
Question 62
The standard neoadjuvant and adjuvant chemotherapy regimen for high-grade conventional osteosarcoma (MAP protocol) consists of which of the following agents?
Explanation
Question 63
Which radiographic projection is most sensitive for confirming the presence of a calcaneonavicular coalition in a pediatric patient?
Explanation
Question 64
During a two-incision approach for a distal biceps tendon repair, the forearm should be placed in which position while the surgeon spreads through the extensor muscle mass to expose the radial tuberosity, in order to protect the posterior interosseous nerve (PIN)?
Explanation
Question 65
A 16-year-old male is suspected of having a conventional high-grade osteosarcoma of the distal femur based on local plain radiographs and MRI. Staging studies are mandatory before initiating treatment. Which of the following sites is the most common location for initial metastasis in this disease?
Explanation
Question 66
A 45-year-old bodybuilder feels a sudden pop in his antecubital fossa while performing heavy curls. He presents with ecchymosis and a palpable defect. The physician asks the patient to actively supinate the forearm and flex the elbow to 90 degrees, then hooks an index finger under a cord-like structure from the lateral side. The structure is absent. Which of the following tendons is most likely ruptured?
Explanation
Question 67
A 38-year-old male undergoes a single-incision anterior repair of a distal biceps tendon rupture. Postoperatively, he complains of numbness and tingling over the radial aspect of his volar forearm. Which of the following nerves was most likely injured or compressed during the surgical approach?
Explanation
Question 68
A 42-year-old male sustains a posterior interosseous nerve (PIN) injury during a modified 2-incision repair of his distal biceps tendon. Which of the following motor deficits is most expected on his postoperative examination?
Explanation
Question 69
A 14-year-old boy presents with progressive knee pain and swelling. Radiographs show a destructive, mixed lytic and sclerotic lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. A biopsy is performed. Which of the following histologic findings is essential for the diagnosis of conventional osteosarcoma?
Explanation
Question 70
A 16-year-old female is diagnosed with conventional high-grade osteosarcoma of the proximal tibia. Genetic analysis of the tumor reveals a mutation associated with an increased risk of a specific childhood ocular malignancy. Which of the following genes is most likely mutated?
Explanation
Question 71
A 12-year-old boy with conventional osteosarcoma of the distal femur completes a 10-week course of neoadjuvant chemotherapy. He then undergoes wide surgical resection. Which of the following histologic parameters evaluated in the resected specimen is the most important prognostic factor for his long-term survival?
Explanation
Question 72
A 10-year-old boy complains of frequent right ankle sprains and lateral foot pain. On examination, he has a rigid flatfoot with restricted subtalar motion. Radiographs show an elongation of the anterior process of the calcaneus, known as the 'anteater nose' sign. Which of the following is the most likely diagnosis?
Explanation
Question 73
A 14-year-old girl presents with deep medial hindfoot pain and a rigid flatfoot. A CT scan confirms a tarsal coalition. Which of the following anatomic locations is most commonly involved in this specific type of coalition?
Explanation
Question 74
A 28-year-old female presents with a slowly enlarging, painless mass on the posterior aspect of her thigh. Radiographs reveal a dense, heavily ossified mass attached to the posterior cortex of the distal femur with a broad base, but lacking medullary involvement. Which of the following is the most likely genetic amplification associated with this lesion?
Explanation
Question 75
A 13-year-old boy presents with a rigid valgus foot and recurrent ankle sprains. A lateral radiograph of the foot demonstrates a continuous rim of bone outlining the talar dome and extending inferiorly to the sustentaculum tali. This radiographic 'C-sign' is indicative of which of the following conditions?
Explanation
Question 76
During a distal biceps tendon repair, the surgeon must decide where to reattach the tendon on the radial tuberosity to optimize postoperative functional mechanics. Reattachment to which aspect of the tuberosity best restores maximum supination strength?
Explanation
Question 77
A 15-year-old male presents with severe pain in his proximal humerus. Radiographs show an aggressive, expansile, completely lytic lesion. MRI reveals multiple fluid-fluid levels. Biopsy shows blood-filled spaces lined by highly atypical, pleomorphic cells producing small amounts of osteoid. What is the most likely diagnosis?
Explanation
Question 78
A 17-year-old male is undergoing multi-agent neoadjuvant chemotherapy for conventional osteosarcoma. His regimen includes Methotrexate, Doxorubicin, and Cisplatin. Routine monitoring for an irreversible side effect of Doxorubicin requires which of the following surveillance studies?
Explanation
Question 79
A 14-year-old male presents with 'peroneal spastic flatfoot'. Examination reveals restricted subtalar motion and painful eversion. The peroneal muscle spasm is considered to be a secondary reflex mechanism. What is the underlying anatomic abnormality most likely causing this presentation?
Explanation
Question 80
A 10-year-old girl with an symptomatic calcaneonavicular coalition fails nonoperative management. She undergoes a surgical resection of the coalition. To prevent recurrence, which of the following tissues is most commonly interposed into the resection gap?
Explanation
Question 81
A surgeon performs a modified two-incision (Boyd-Anderson) approach for a chronic distal biceps tendon rupture. Dissection is taken through the interosseous membrane to retrieve the retracted tendon. Which of the following complications is uniquely heightened by this specific surgical exposure compared to a single-incision approach?
Explanation
Question 82
A 72-year-old male presents with a rapid increase in deep thigh pain. He has a longstanding history of a benign polyostotic bone disorder. Radiographs show cortical thickening and trabecular coarsening of the femur, with a new, superimposed destructive lytic lesion breaking through the cortex. Biopsy confirms osteosarcoma. Which of the following underlying conditions did this patient most likely have?
Explanation
Question 83
A 13-year-old boy requires surgical intervention for a symptomatic talocalcaneal coalition after failing conservative treatment. Preoperative CT imaging is utilized to evaluate the joint. According to current literature, resection of the coalition is generally indicated if it involves less than what percentage of the posterior facet area?
Explanation
Question 84
A 16-year-old male with a history of high-grade osteosarcoma of the distal femur treated with limb-salvage and chemotherapy presents for his 1-year follow-up. He is asymptomatic, but a routine surveillance scan reveals a new finding. Which of the following organs is the most common site of metastasis for this disease?
Explanation
Question 85
During a clinical evaluation for a suspected distal biceps tendon rupture, the examiner notes considerable bruising but palpates a tendon-like structure in the antecubital fossa that remains taut with passive forearm rotation. However, MRI confirms a complete tear of the distal biceps tendon from the radial tuberosity. Which of the following structures is preventing profound proximal retraction of the muscle belly?
Explanation
Question 86
A 12-year-old boy presents with recurrent ankle sprains and lateral foot pain. On examination, he has a rigid flatfoot with severely restricted subtalar motion and peroneal muscle spasm. A 45-degree internal oblique radiograph of the foot demonstrates an elongated anterior process of the calcaneus.
After a failed trial of short-leg casting, which of the following is the most appropriate next step in management?
Explanation
Question 87
A 15-year-old girl presents with progressively worsening right knee pain. Radiographs reveal a destructive metaphyseal lesion of the distal femur with a sunburst periosteal reaction.
Biopsy confirms high-grade spindle cells producing osteoid. A biallelic germline mutation in which of the following tumor suppressor genes is most directly associated with a familial syndrome causing both this bone tumor and bilateral leukocoria in infancy?
Explanation
Question 88
A 45-year-old male undergoes a single-incision anterior repair of a distal biceps tendon rupture. In the recovery room, he is unable to actively extend his thumb and metacarpophalangeal joints, but has intact sensation in his hand and forearm. Which of the following anatomic structures was most likely compressed by a retractor placed on the lateral side of the radial neck?
Explanation
Question 89
A 14-year-old adolescent presents with medial hindfoot pain and a rigid flatfoot deformity. A lateral radiograph demonstrates a continuous bony bridge between the talus and calcaneus (C-sign).
Which anatomic facet is most commonly involved in this specific type of tarsal coalition?
Explanation
Question 90
An 18-year-old male is undergoing treatment for conventional osteosarcoma of the proximal tibia. He receives a standard regimen of neoadjuvant chemotherapy prior to surgical wide resection. Which of the following histologic findings on the definitive resection specimen is the most important prognostic factor for long-term survival?
Explanation
Question 91
A surgeon plans to use a classic two-incision modified Boyd-Anderson approach for the repair of a chronic distal biceps tendon tear. Compared to the single-incision anterior approach, the two-incision technique carries a uniquely increased risk of which of the following complications?
Explanation
Question 92
A 20-year-old male presents with a purely lytic, destructive lesion in the distal femur. MRI reveals multiple fluid-fluid levels within the lesion.
A core needle biopsy demonstrates blood-filled spaces separated by septations containing highly atypical malignant spindle cells that are producing osteoid. What is the most likely diagnosis?
Explanation
Question 93
In a 14-year-old patient with a symptomatic talocalcaneal coalition that has failed conservative management, which of the following is considered a relative contraindication to coalition resection and instead warrants primary subtalar arthrodesis?
Explanation
Question 94
A 45-year-old laborer elects for nonoperative management of an acute, complete distal biceps tendon rupture. Compared to his uninjured contralateral arm, he is expected to have the greatest percentage of strength deficit in which of the following functional motions?
Explanation
Question 95
A 30-year-old female presents with a painless, slow-growing mass on the posterior aspect of her distal femur. Radiographs show a heavily ossified, lobulated mass arising from the cortex with a radiolucent "string sign" cleft between the tumor and the underlying bone.
Which of the following molecular alterations is most characteristic of this specific bone tumor?
Explanation
None
