ABOS Part I Orthopaedic Surgery Review: Shoulder Instability, Blount Disease & Ankle Injuries | Part 21541

Key Takeaway
This ABOS Part I Orthopaedic Surgery Review module offers 42 advanced multiple-choice questions mirroring ABOS Part I and AAOS OITE exams. It comprehensively covers high-yield topics in shoulder instability (e.g., Kim lesion, posterior dislocation), Blount disease (guided growth, osteotomy), and ankle pathologies (Achilles rupture, malleolar fractures, EDB interposition), including surgical approaches, biomechanics, and rehabilitation protocols for effective exam preparation.
ABOS Part I Orthopaedic Surgery Review: Shoulder Instability, Blount Disease & Ankle Injuries | Part 21541
A 32-year-old male presents to the emergency department after a generalized tonic-clonic seizure. He complains of severe left shoulder pain and inability to move his arm. Physical examination reveals the arm held in internal rotation and adduction, with a flattened anterior deltoid contour. Radiographs are obtained.
Based on the provided image and clinical scenario, which of the following is the MOST likely diagnosis and a common associated bony lesion?

Correct Answer: C
The clinical presentation of an arm held in internal rotation and adduction, especially following a seizure, is highly classic for a posterior glenohumeral dislocation. The provided AP radiograph, while often subtle, shows the 'lightbulb sign' (the humeral head appears symmetrically round due to internal rotation) and an overlap of the humeral head with the glenoid, both indicative of a posterior dislocation. The case content explicitly states that traumatic posterior dislocations are typically caused by axial loading of an adducted, internally rotated, and flexed arm, often seen in convulsive disorders (seizures, electrocution). A reverse Hill-Sachs lesion, an impression fracture on the anteromedial aspect of the humeral head, is a common associated bony lesion that occurs when the posterior glenoid rim impacts the humeral head during a posterior dislocation.
Option A is incorrect because anterior dislocations typically present with the arm in slight abduction and external rotation, and a Hill-Sachs lesion is associated with anterior instability.
Option B is incorrect as luxatio erecta presents with the arm held in extreme abduction, and a greater tuberosity fracture is more common with anterior dislocations.
Option D is incorrect as an AC joint separation involves the distal clavicle and acromion, not the glenohumeral joint, and the clinical presentation is different.
Option E is incorrect as a scapular fracture would have different radiographic findings and clinical presentation, and while a rotator cuff tear can be associated, it's not the primary diagnosis or the most common bony lesion in this specific scenario.
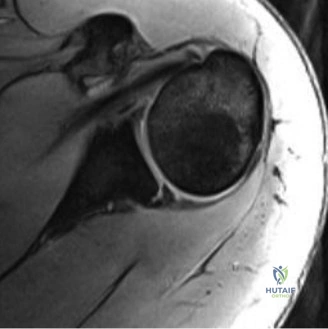
A 28-year-old professional weightlifter presents with chronic, deep-seated posterior shoulder pain and a sensation of 'clunking' during overhead lifts, particularly during bench press. He denies any acute traumatic event but reports a gradual onset of symptoms over 6 months. Physical examination reveals a positive Jerk test and apprehension with combined adduction, internal rotation, and flexion. An MR Arthrography (MRA) is performed.
Based on the clinical presentation and the provided MRA image, which of the following soft tissue lesions is MOST likely present and contributes significantly to his symptoms?

Correct Answer: C
The patient's history of chronic posterior shoulder pain, clunking during overhead activities (especially bench press, which involves adduction and internal rotation), and positive Jerk test are highly suggestive of posterior glenohumeral instability. The MRA image, which is the gold standard for evaluating soft tissue lesions, would be used to identify specific pathology. The case content specifically mentions the 'Kim lesion' as an avulsion of the posterior-inferior labrum from the glenoid rim with an associated partial tear or delamination of the glenoid cartilage, often subtle and potentially missed. This type of lesion is consistent with chronic microtrauma in athletes like weightlifters and contributes to posteroinferior instability.
Option A (Anterior Bankart lesion) is associated with anterior instability and would present with different symptoms and physical exam findings.
Option B (SLAP tear) typically presents with pain during overhead activities, but the primary instability symptoms and positive Jerk test point more specifically to posterior instability.
Option D (Rotator cuff tear of the supraspinatus) would primarily cause pain with abduction and external rotation, and weakness, rather than clunking and apprehension in adduction/internal rotation.
Option E (Subscapularis tendon avulsion) is associated with anterior instability or trauma and would affect internal rotation strength and anterior stability.
A 40-year-old male presents with recurrent posterior shoulder subluxations following a fall onto an outstretched hand (FOOSH) 6 months prior. Conservative management has failed. Pre-operative imaging includes a 3D CT scan, which reveals significant posterior glenoid bone loss. The image below is representative of such a finding.
Given the finding of significant posterior glenoid bone loss, which of the following surgical interventions is MOST appropriate to restore glenoid articular arc and prevent recurrence?

Correct Answer: C
The case content explicitly states that open posterior approaches are indicated for cases with substantial posterior glenoid bone loss (>15-20%). For significant glenoid bone loss, augmentation of the posterior glenoid rim is necessary, typically with an autogenous bone graft (e.g., iliac crest) or allograft, which is shaped and fixed to the posterior glenoid neck to effectively extend the posterior glenoid rim. The 3D CT image is essential for quantifying this bone loss, making an open bone grafting procedure the most appropriate choice to restore the glenoid articular arc and provide a stable platform.
Option A (Arthroscopic posterior labral repair with capsular plication) is generally preferred for isolated soft tissue lesions without significant bone loss. It would be insufficient for substantial bone loss.
Option B (Arthroscopic remplissage procedure) addresses an engaging reverse Hill-Sachs lesion on the humeral head, not glenoid bone loss.
Option D (Arthroscopic biceps tenodesis) is for biceps pathology and does not address glenohumeral instability or bone loss.
Option E (Open anterior Latarjet procedure) is for anterior glenoid bone loss, not posterior, and would be inappropriate in this context.
A 22-year-old college football lineman presents with recurrent posterior shoulder instability. He reports that his shoulder 'pops out' when he is blocking opponents, often with his arm in a position of adduction, internal rotation, and flexion. He has failed a 3-month course of physical therapy focusing on rotator cuff and scapular strengthening. Pre-operative planning is underway for arthroscopic posterior stabilization. During patient positioning, the surgeon opts for the lateral decubitus position.
Which of the following is a critical step in patient positioning for arthroscopic posterior stabilization in the lateral decubitus position to prevent nerve injury?
Correct Answer: C
The case content explicitly states that for arthroscopic posterior stabilization in the lateral decubitus position, 'An axillary roll is placed in the contralateral axilla to protect the brachial plexus and prevent nerve compression.' This is a critical step to prevent iatrogenic injury to the neurovascular structures in the dependent axilla due to prolonged compression.
Option A (Placing the operative arm in maximal external rotation) is incorrect; the arm is typically suspended in abduction and slight forward flexion, and maximal external rotation is avoided, especially in posterior instability cases, as it can stress the anterior capsule.
Option B (Ensuring the head is hyperextended) is incorrect and can lead to cervical spine issues or compromise cerebral perfusion, especially in the beach chair position, but generally not a recommended practice.
Option D (Positioning the patient with the operative shoulder down) is incorrect; in the lateral decubitus position, the operative shoulder is positioned UP to allow access for arthroscopy.
Option E (Applying excessive traction) is incorrect; the case specifies gentle traction (typically 10-15 lbs) to distract the joint. Excessive traction can lead to brachial plexus neuropraxia.
A 35-year-old male undergoes open posterior glenohumeral stabilization for recurrent posterior instability with significant glenoid retroversion. The surgeon plans a posterior deltoid-splitting approach to access the joint. During the approach, careful attention is paid to the internervous plane and nerve protection. The image below depicts a posterior shoulder approach.
Which of the following statements accurately describes the internervous plane utilized in this approach and a critical nerve to protect?
Correct Answer: C
The case content explicitly describes the open posterior approach: 'The approach utilizes the interval between the infraspinatus (innervated by the suprascapular nerve) and the teres minor (innervated by the axillary nerve).' It also highlights that 'Care must be taken to identify and protect the axillary nerve, which typically courses horizontally approximately 5-7 cm distal to the acromial angle' and that 'The split should not extend more than 5 cm distally from the acromion to avoid injury to the axillary nerve.' Therefore, the interval between the infraspinatus and teres minor is the internervous plane, and the axillary nerve is a critical structure to protect.
Option A describes an anterior approach and an incorrect nerve.
Option B describes an incorrect interval and nerve.
Option D describes an incorrect interval and nerve.
Option E describes muscles involved in scapular stabilization, not the direct glenohumeral approach, and an incorrect nerve for this context.
A 19-year-old male presents with a history of recurrent posterior shoulder subluxations during basketball. He reports a feeling of the shoulder 'slipping out' when he reaches across his body or attempts a chest pass. Physical examination reveals a positive Kim test. Which of the following best describes the Kim test and its significance?
Correct Answer: C
The case content provides a precise description of the Kim test: 'With the patient seated, the arm is abducted to 90 degrees. The examiner holds the elbow and lateral aspect of the proximal arm. An axial load and 45-degree elevation are applied, while a posterior and inferior force is applied to the proximal arm. A sudden pain in the posterior shoulder indicates a positive test for posteroinferior labral avulsion.' This test is specifically designed to identify subtle posteroinferior labral pathology, such as a Kim lesion, which is consistent with the patient's symptoms of posterior instability.
Option A describes the anterior apprehension test.
Option B describes the Jerk test, which is also for posterior instability but has a different maneuver.
Option D describes a maneuver for impingement, not instability.
Option E describes the Sulcus sign, which indicates inferior laxity, often seen in multidirectional instability.
A 25-year-old male presents with chronic posterior shoulder pain and a feeling of instability. He is a competitive swimmer and experiences symptoms during freestyle strokes. MRI reveals a posterior labral tear and mild capsular laxity. A CT scan is also performed to rule out bony pathology. The CT scan shows normal glenoid retroversion and no significant glenoid bone loss. Which of the following is the MOST appropriate initial surgical management for this patient?
Correct Answer: C
The case content states that 'Arthroscopic stabilization is generally preferred for isolated posterior labral tears (reverse Bankart lesions) and capsular laxity without significant bone loss.' This patient has a posterior labral tear and mild capsular laxity, with no significant glenoid bone loss or abnormal retroversion, and no mention of an engaging reverse Hill-Sachs lesion. Therefore, arthroscopic posterior labral repair with capsular plication is the most appropriate initial surgical management, aiming to reattach the labrum and tighten the posterior capsule.
Option A (Open posterior glenoid osteotomy) would be indicated for significant glenoid retroversion, which is not present here.
Option B (Open posterior Latarjet procedure) is a complex procedure for significant glenoid bone loss, which is also not present.
Option D (Arthroscopic remplissage procedure) is indicated for an engaging reverse Hill-Sachs lesion, which is not mentioned as present.
Option E (Total shoulder arthroplasty) is a salvage procedure for severe arthritis or irreparable damage, not indicated for this patient's condition.
A 50-year-old sedentary patient undergoes arthroscopic posterior labral repair and capsular plication for recurrent posterior subluxations. Post-operatively, the patient is placed in a sling. The rehabilitation protocol is initiated. Which of the following is a critical restriction during the initial 4-6 weeks of the post-operative rehabilitation protocol?
Correct Answer: C
The case content emphasizes the critical restrictions during Phase 1 (Protection and Early Motion) of post-operative rehabilitation for posterior GH instability. It states: 'Avoid combined adduction, internal rotation, and flexion.' and specifically, 'No internal rotation past neutral for the first 4-6 weeks.' This restriction is crucial to protect the posterior capsulolabral repair from undue stress, as internal rotation combined with adduction and flexion is the position of posterior instability.
Option A (Active external rotation beyond 30 degrees) is generally limited initially, but the primary restriction for posterior repair is internal rotation.
Option B (Passive abduction beyond 120 degrees) is incorrect; PROM for abduction is typically allowed up to 90 degrees, and sometimes higher, but 120 degrees is often achievable passively.
Option D (Passive flexion beyond 150 degrees) is incorrect; PROM for flexion is typically allowed to 90-120 degrees, but 150 degrees is often too aggressive initially.
Option E (Any active elbow, wrist, or hand exercises) is incorrect; the protocol encourages active ROM exercises for the elbow, wrist, and hand to prevent stiffness and maintain circulation.
A 29-year-old professional baseball pitcher presents with persistent posterior shoulder pain and a sense of instability, particularly during the follow-through phase of his pitching motion. He has failed extensive non-operative management. MRI reveals a subtle posterior-inferior labral avulsion with associated partial delamination of the glenoid cartilage, but no discrete labral tear. A 3D CT scan shows no significant glenoid bone loss or engaging reverse Hill-Sachs lesion. Given these findings, which specific soft tissue lesion is MOST likely present and requires careful identification during arthroscopy?
Correct Answer: D
The patient's symptoms of posterior shoulder pain and instability, especially in a high-demand overhead athlete, combined with the MRI findings of a 'subtle posterior-inferior labral avulsion with associated partial delamination of the glenoid cartilage, but no discrete labral tear,' are highly characteristic of a Kim lesion. The case content defines a Kim lesion as 'An avulsion of the posterior-inferior labrum from the glenoid rim with an associated partial tear or delamination of the glenoid cartilage, but without a discrete labral tear. This lesion is often subtle and can be missed.' This description perfectly matches the MRI findings and the clinical scenario.
Option A (Anterior Bankart lesion) is for anterior instability.
Option B (SLAP tear) involves the superior labrum and biceps anchor, not primarily the posterior-inferior aspect.
Option C (Reverse Bankart lesion) is a discrete posterior labral tear, which the description explicitly states is 'without a discrete labral tear' in the Kim lesion definition.
Option E (Posterior superior labral tear) is a different location and typically presents differently.
A 42-year-old male presents with a chronic, unreduced posterior glenohumeral dislocation following a motor vehicle accident 3 months prior. He has significant pain and functional limitation. Pre-operative imaging reveals a large, engaging reverse Hill-Sachs lesion occupying approximately 30% of the humeral head articular surface, in addition to a posterior labral tear. The glenoid morphology is otherwise normal. Which of the following surgical strategies is MOST appropriate to address the engaging reverse Hill-Sachs lesion in this scenario?
Correct Answer: C
The case content specifically addresses the management of engaging reverse Hill-Sachs lesions: 'For engaging reverse Hill-Sachs lesions (often those occupying >25% of the humeral head articular surface), a remplissage procedure (French for 'to fill in') can be performed. This involves tenodesing the infraspinatus tendon and posterior capsule into the humeral head defect using suture anchors. This effectively fills the defect, preventing it from engaging the posterior glenoid rim during internal rotation and adduction.' Given the large, engaging nature of the lesion (30% of the articular surface), a remplissage procedure is the most appropriate strategy to prevent recurrent engagement and instability.
Option A (Arthroscopic posterior labral repair only) would not address the engaging bony defect, leading to high recurrence rates.
Option B (Open posterior glenoid bone block augmentation) is for glenoid bone loss, not for a humeral head defect.
Option D (Debridement of the reverse Hill-Sachs lesion) would remove articular cartilage and potentially worsen the defect, not stabilize it.
Option E (Total shoulder arthroplasty) is an extreme measure for severe arthritis or irreparable damage, not indicated as a primary treatment for an engaging Hill-Sachs lesion in an otherwise normal glenoid.
A 38-year-old male presents with recurrent posterior shoulder instability. He reports that his shoulder dislocates when he falls onto an outstretched hand with his arm in a specific position. Which combination of arm positions places maximal stress on the posterior capsule and labrum, predisposing to posterior glenohumeral instability?
Correct Answer: B
The case content explicitly states the biomechanics of posterior GH instability: 'Posterior GH instability typically occurs when the arm is loaded in positions of adduction, internal rotation, and flexion. This position places maximal stress on the posterior capsule and labrum.' This is a fundamental concept in understanding posterior shoulder instability and is often the mechanism of injury in traumatic cases like falls onto an outstretched hand (FOOSH).
Option A (Abduction, external rotation, and extension) is the classic position of anterior glenohumeral instability.
Option C (Neutral rotation, 90 degrees abduction, and neutral flexion) is a relatively stable position and not typically associated with instability.
Option D (Full extension, neutral rotation, and adduction) does not represent the maximal stress position for posterior instability.
Option E (Hyperabduction and external rotation) is also associated with anterior or inferior instability (luxatio erecta).
A 12-year-old obese African American male presents with progressive right knee varus deformity. He reports no pain but notes difficulty participating in sports due to his bowing. Physical examination reveals a noticeable varus thrust with ambulation. Standing full-length AP radiographs show a right Medial Proximal Tibial Angle (MPTA) of 72 degrees, a Mechanical Axis Deviation (MAD) of 35 mm medial to the center of the knee, and open physes. Left hand and wrist radiograph indicates a skeletal age of 11 years. Which of the following is the most appropriate initial surgical management for this patient?
Correct Answer: D
The patient presents with severe adolescent Blount disease, characterized by an MPTA of 72 degrees and a MAD of 35 mm medial to the center of the knee. According to the case content, lateral hemiepiphysiodesis is indicated for mild to moderate angular deformities, typically with an MPTA between 75-85 degrees and MAD generally less than 20-30 mm. Severe deformities, defined as MAD > 30-40 mm or MPTA < 70 degrees, are a contraindication for hemiepiphysiodesis because the remaining growth potential is unlikely to achieve full correction within a reasonable timeframe, or a rapid, definitive correction is required. In such severe cases, especially in older patients or those with significant deformity, an acute correction osteotomy (proximal tibial varus-producing osteotomy) is the definitive solution. While the patient has open physes, the severity of the deformity outweighs the benefits of guided growth in this scenario. Observation and bracing are typically for milder, non-progressive cases or younger children. Medial hemiepiphysiodesis would worsen the varus. Distal femoral hemiepiphysiodesis would address femoral varus, but the primary pathology here is tibial.
During a lateral proximal tibial hemiepiphysiodesis, a surgeon is performing the dissection to expose the lateral cortex of the proximal tibia. Which neurovascular structure is at highest risk of iatrogenic injury if deep or misguided retractors are used, and where is it typically located relative to the surgical site?
Correct Answer: C
The case explicitly states under the 'Neurovascular Structures' section that the 'Common Peroneal Nerve courses superficially around the fibular neck, approximately 3-5 cm distal to the proximal tibial physis. Extreme care must be taken to avoid injury during lateral dissection and especially with any hardware placed deep and distal.' This makes it the structure at highest risk with deep or misguided retractors in this specific surgical approach. The popliteal artery and vein are located posteriorly, but less directly at risk with a lateral approach to the tibia. The anterior tibial artery passes through the interosseous membrane anteriorly. The saphenous nerve is medial, and the posterior tibial artery is deep in the posterior compartment, making them less vulnerable during a lateral proximal tibial approach.
A 7-year-old patient with progressive infantile Blount disease (Langenskiöld Stage III) undergoes lateral proximal tibial hemiepiphysiodesis. The biomechanical principle primarily responsible for the gradual correction of the varus deformity in this procedure is:
Correct Answer: C
The case clearly outlines the biomechanical basis for hemiepiphysiodesis. It states: 'Hemiepiphysiodesis operates on fundamental biomechanical principles governed by the Hueter-Volkmann law and the concept of guided growth.' The Hueter-Volkmann law states that increased compressive forces across a physis inhibit growth, while decreased compressive forces stimulate growth. In lateral hemiepiphysiodesis, the lateral side of the physis is tethered, which effectively increases compressive forces or restricts growth on that side. This allows the medial physis, which was previously subjected to excessive compressive forces due to varus, to experience relatively decreased compressive forces (or simply grow uninhibitedly), thereby stimulating its growth and correcting the varus deformity. The plate acts as a hinge, not an active compressor of the physis itself, but rather guides differential growth.
A 5-year-old child is being evaluated for progressive infantile Blount disease. Which of the following radiographic views is considered most crucial for a comprehensive assessment of overall lower limb alignment, identification of the deformity's apex, and accurate measurement of the Mechanical Axis Deviation (MAD)?
Correct Answer: C
Under 'Radiographic Evaluation' in the 'Pre-Operative Planning' section, the case states: 'Standing Full-Length AP Radiographs (Mechanical Axis Views): Crucial for comprehensive assessment of overall limb alignment. These films extend from the femoral head to the ankle joint and are used to: Determine the Mechanical Axis Deviation (MAD)... Measure the Medial Distal Femoral Angle (mLDFA)... Measure the Joint Line Convergence Angle (JLCA)... Identify any significant Leg Length Discrepancy (LLD).' While other views provide important information (e.g., knee AP for MPTA, lateral for procurvatum, MRI for physeal integrity), the standing full-length AP radiograph is uniquely essential for assessing the overall mechanical axis and identifying the true extent and location of the deformity in the entire limb.
During lateral proximal tibial hemiepiphysiodesis using an eight-plate, the most critical technical step to ensure effective guided growth and prevent physeal damage is:
Correct Answer: C
The 'Detailed Surgical Approach / Technique' section emphasizes the critical nature of screw insertion. It states: 'The screws should be inserted parallel to the physis and perpendicular to the long axis of the bone segment. This ensures that the growth plate is not compressed or damaged, but rather 'tethered' by the plate.' It further clarifies: 'Crucially, verify that no screw has crossed or damaged the physis. The screw threads should be entirely within either the epiphyseal or metaphyseal bone. The smooth shaft of the screw should pass through the physis, allowing translation.' While bicortical purchase is generally aimed for stability (especially in the metaphysis), unicortical in the epiphysis is often acceptable. The plate should sit flush, but not necessarily be 'tightly compressed' in a way that would impede the hinge effect. Placing the plate too far anteriorly or using an oversized drill bit are not the most critical aspects for guided growth efficacy and physeal protection.
A 9-year-old patient underwent lateral proximal tibial hemiepiphysiodesis for Blount disease 18 months ago. At the most recent follow-up, standing full-length radiographs show a mechanical axis that has shifted significantly lateral to the center of the knee, indicating a genu valgum deformity. The patient's skeletal age is 10 years. What is the most appropriate initial management for this complication?
Correct Answer: A
The case discusses 'Overcorrection (Genu Valgum)' as a common complication. It states: 'Prevention: Close radiographic follow-up every 3-6 months. Hardware removal is typically performed when the limb is slightly overcorrected into valgus (e.g., 5-7 degrees of mechanical valgus) to anticipate potential rebound into varus. Early Detection: Timely removal of the eight-plate.' Since the patient has developed a significant genu valgum deformity, the most appropriate initial management is the immediate removal of the eight-plate to stop the differential growth and prevent further overcorrection. Contralateral hemiepiphysiodesis might be considered if significant valgus persists after hardware removal and there's still growth, but removal is the first step. Osteotomy is a more invasive salvage for severe, fixed valgus. Observation is incorrect as this is an active complication requiring intervention. Re-insertion would worsen the valgus.
Following lateral proximal tibial hemiepiphysiodesis, which aspect of post-operative care is most critical for ensuring a successful outcome and preventing complications like overcorrection or undercorrection?
Correct Answer: C
The 'Monitoring and Correction Phase' section of the 'Post-Operative Rehabilitation Protocols' explicitly states: 'Regular Clinical and Radiographic Follow-up: This is the most critical aspect of the post-operative protocol. Frequency: Typically every 3-6 months until desired correction is achieved. Radiographs: Standing full-length AP radiographs (mechanical axis views) are essential at each visit.' This close monitoring is crucial for determining the precise timing of hardware removal to achieve optimal alignment and prevent overcorrection or undercorrection. The procedure typically allows early weight-bearing. Aggressive or high-impact activities are generally avoided initially. Long-term antibiotics are not indicated for routine hemiepiphysiodesis.
A 6-year-old child presents with progressive bilateral tibia vara. Radiographs reveal a medial physeal beak, epiphyseal-metaphyseal irregularities, and significant physeal widening, consistent with Langenskiöld Stage IV infantile Blount disease. The patient has sufficient remaining growth potential. Based on the case, what is the most appropriate surgical intervention?
Correct Answer: B
The 'Indications for Lateral Hemiepiphysiodesis' section specifically lists: 'Progressive Infantile Blount Disease: Langenskiöld stages II-IV. Age typically between 4 and 8 years (beyond the age of potential spontaneous resolution or bracing efficacy, but before severe physeal damage).' The patient's age (6 years), progressive nature, and Langenskiöld Stage IV classification fall squarely within the indications for lateral proximal tibial hemiepiphysiodesis. Observation with bracing is for Stage I or non-progressive cases. Medial hemiepiphysiodesis would exacerbate the varus. Acute osteotomy is reserved for more severe stages (V-VI) or when guided growth has failed. Permanent physeal arrest is typically for older adolescents nearing skeletal maturity or for LLD management, not primary guided growth for Blount disease.
A 16-year-old male presents with severe, progressive adolescent Blount disease. Radiographic evaluation reveals an MPTA of 65 degrees, a MAD of 45 mm, and nearly closed physes with evidence of a significant medial physeal bar (>50% of the physeal cross-sectional area). Based on these findings, which of the following is the absolute contraindication for lateral proximal tibial hemiepiphysiodesis, and what would be the more appropriate surgical approach?
Correct Answer: C
The 'Contraindications for Lateral Hemiepiphysiodesis' section clearly lists: 'Skeletal Maturity: Closed physes, as there is no remaining growth potential for guided correction. In these cases, acute osteotomy is indicated.' and 'Significant Physeal Bar: A large medial physeal bar (e.g., >50% of physeal cross-sectional area) will mechanically impede medial growth, rendering guided growth ineffective. Physeal bar resection or osteotomy would be more appropriate.' The patient's nearly closed physes and a significant medial physeal bar are absolute contraindications for guided growth. The severe deformity (MPTA 65 degrees, MAD 45 mm) further supports this. Therefore, an acute proximal tibial varus-producing osteotomy is the indicated alternative. Obesity is a risk factor but not an absolute contraindication for surgery. Medial distal femoral hemiepiphysiodesis is for femoral deformity. Bracing is for mild cases. Contralateral hemiepiphysiodesis is not indicated for unilateral disease.
The shift in surgical management of Blount disease from acute osteotomies to guided growth techniques, particularly using eight-plates, is primarily supported by which of the following advantages of guided growth?
Correct Answer: C
The 'Summary of Key Literature / Guidelines' section highlights the advantages of guided growth: 'Advantages highlighted: Minimally invasive, outpatient procedure, allows for gradual and physiological correction, avoids osteotomy-related morbidities, permits early weight-bearing and faster return to activity.' This directly supports option C. Guided growth does not guarantee a faster rate of correction (it depends on growth potential), is less invasive, not more. It is not effective for all stages, especially severe deformities or those with significant physeal bars, and it absolutely requires rigorous post-operative radiographic follow-up to prevent overcorrection or undercorrection.
A 42-year-old male, a self-described "weekend warrior," presents to the emergency department after experiencing a sudden "pop" in his right calf while playing recreational basketball. He reports immediate pain and difficulty pushing off his foot. On examination, a palpable gap is noted in the Achilles tendon, and the Thompson test is positive. Based on the epidemiology and anatomy described in the case, which of the following statements regarding this patient's injury is most accurate?
Correct Answer: C
The case describes the typical patient profile for an acute Achilles tendon rupture as a male, aged 30-50 years, often a "weekend warrior" involved in activities like basketball. The mechanism (sudden "pop," difficulty push-off) and clinical findings (palpable gap, positive Thompson test) are classic for an acute rupture. The text explicitly states, "The vast majority of acute ruptures occur within the mid-substance of the tendon, specifically in a region approximately 2-6 cm proximal to its calcaneal insertion. This region is critically important due to its relatively hypovascular nature, often referred to as the 'watershed zone' or 'critical zone'."
Option A is incorrect because ruptures are most common in the mid-substance, not typically at the musculotendinous junction, and the mechanism involves eccentric load during dorsiflexion with knee extension, not just excessive knee extension. Option B is incorrect as his age and activity level perfectly match the typical patient profile. Option D is incorrect because the watershed zone receives its blood supply predominantly from the paratenon, with fewer direct penetrating vessels, making it hypovascular and prone to reduced healing capacity, not rapid healing from the osseotendinous junction. Option E is incorrect as the symptoms are highly consistent with an acute Achilles tendon rupture.
A 38-year-old professional soccer player sustains an acute Achilles tendon rupture during a match. He undergoes open surgical repair. During the procedure, the surgeon meticulously identifies and protects the sural nerve. Post-operatively, the patient develops numbness and paresthesias along the lateral aspect of his foot. Based on the surgical anatomy described in the case, which statement best explains the course of the sural nerve and its susceptibility to injury?
Correct Answer: D
The case explicitly states, "Of particular surgical relevance is the sural nerve, a sensory nerve arising from the tibial and common peroneal nerves, which courses subcutaneously along the posterior calf, often running close to the lateral border of the Achilles tendon. It is highly susceptible to iatrogenic injury during posterior surgical approaches." This directly explains the patient's symptoms (numbness, paresthesias) and the nerve's anatomical vulnerability.
Option A is incorrect; the sural nerve is sensory, and the triceps surae is innervated by the tibial nerve. Option B is incorrect; the sural nerve courses subcutaneously, not deep to the tendon. Option C is incorrect; the sural nerve arises from the tibial and common peroneal nerves, not the femoral nerve, and typically runs laterally, not medially, to the Achilles tendon. Option E is incorrect; the sural nerve is sensory, and ankle dorsiflexion is primarily by the deep peroneal nerve.
A 55-year-old sedentary individual with a history of type 2 diabetes and peripheral vascular disease presents with a suspected Achilles tendon rupture. He reports no specific traumatic event, but rather a gradual onset of pain and weakness in his calf. Clinical examination reveals a small palpable gap (<1 cm) and a positive Thompson test. Given his comorbidities and the injury characteristics, which management strategy is most appropriate according to the case?
Correct Answer: C
The case outlines specific indications for non-operative management: "Elderly or sedentary individuals," "Significant medical comorbidities: Patients with diabetes, peripheral vascular disease, immunosuppression, or other conditions that increase surgical risks (e.g., wound healing complications, infection, DVT)," and "Small tendon gap (<1 cm) and good apposition." This patient fits all these criteria, making non-operative management with an accelerated functional rehabilitation protocol the most appropriate choice to avoid the high surgical risks associated with his comorbidities.
Option A is incorrect due to the high surgical risks (wound healing, infection) in a patient with diabetes and PVD. Option B, while aiming to reduce wound complications, still carries surgical risks and may not be necessary given the small gap and high comorbidity burden. Option D is incorrect; delayed repair is typically for chronic ruptures, not an initial strategy for acute cases, and would still carry high surgical risks. Option E is an augmentation technique typically reserved for chronic ruptures with significant tissue loss or reruptures, not an initial treatment for an acute rupture with a small gap, especially in a high-risk patient.
A 32-year-old recreational runner presents with a chronic Achilles tendon rupture, 3 months after the initial injury. He initially attempted non-operative management but continued to experience significant weakness and inability to perform a single-leg heel raise. MRI reveals a 3 cm gap with significant retraction and poor tissue quality in the mid-substance. He is now scheduled for operative repair. During pre-operative planning, the surgeon considers augmentation. Which of the following augmentation options is most appropriate for this patient, given the details in the case?
Correct Answer: E
The case states, "For chronic ruptures, large gaps, poor tissue quality in the watershed zone, or reruptures, augmentation may be necessary." It then specifically mentions, "For chronic ruptures with significant retraction or tissue loss, FHL transfer is a robust option. The FHL tendon is harvested from the plantar foot or posteromedial ankle, released distally, rerouted through the calcaneus or through the Achilles tendon, and fixed with interference screws or sutures." Given the 3-month delay, 3 cm gap, and poor tissue quality, FHL transfer is a strong and appropriate augmentation choice.
Option A and D (Gastrocnemius recession/V-Y lengthening) are procedures to gain length in chronic cases with contracture, but they are not augmentation techniques that add new tissue to bridge a gap or reinforce a repair with poor tissue quality. Option B (Plantaris tendon autograft) is mentioned as an augmentation option, but the case implies FHL transfer is a 'robust option' specifically for 'significant retraction or tissue loss' in chronic ruptures, which aligns better with a 3 cm gap and poor tissue quality. Option C (Allograft reconstruction) is mentioned as 'rarely used for acute ruptures, but can be considered for revision surgery or extensive defects,' implying it's less common than autograft options like FHL transfer for this scenario.
A 48-year-old male undergoes open Achilles tendon repair for an acute rupture. Post-operatively, he is placed in a posterior splint with the ankle in 15 degrees of plantarflexion. At 2 weeks, sutures are removed, and he transitions to a CAM boot. According to the described rehabilitation protocols, what is the primary goal and expected progression during the subsequent 4-6 weeks (Phase 2)?
Correct Answer: C
Phase 2 of rehabilitation (Weeks 2/3 - 6/8) is described as "Graduated Protected Motion & Partial Weight-Bearing." The goals are to "Gradually restore range of motion (ROM), initiate controlled weight-bearing, maintain muscle function." The patient is in a CAM boot, with gradual increase from partial weight-bearing (PWB) to full weight-bearing (FWB) over 4-6 weeks, and gradual decrease in plantarflexion angle in the boot to allow incremental dorsiflexion.
Option A is incorrect as Phase 2 involves gradual weight-bearing and motion, not strict NWB and maximal plantarflexion. Option B is incorrect; full weight-bearing without the boot and aggressive dorsiflexion stretching are too aggressive for Phase 2. Option D and E are incorrect; these activities (jogging, sport-specific drills, plyometrics) are reserved for Phase 4 (Months 4-6+).
A 35-year-old patient presents with an acute Achilles tendon rupture. The surgeon plans an open repair. During pre-operative planning, the surgeon reviews the vascular supply to the Achilles tendon, particularly noting the "watershed zone." Which of the following statements accurately describes the vascularity of the Achilles tendon and the significance of the watershed zone?

Correct Answer: C
The case states, "The vascular supply to the Achilles tendon is complex and multifaceted... Critically, a relatively hypovascular zone, the 'watershed zone,' exists approximately 2-6 cm proximal to the calcaneal insertion. This region receives its blood supply predominantly from the paratenon, with fewer direct penetrating vessels compared to the proximal and distal ends." It further notes that the paratenon contains a "rich vascular network" and provides the "primary external blood supply" to the tendon's mid-portion.
Option A is incorrect; while the osseotendinous junction has a supply, the paratenon is primary for the mid-substance. Option B is incorrect; the watershed zone is hypovascular, not richly supplied, and receives less direct supply. Option D is incorrect; the watershed zone, not the musculotendinous junction, is highlighted as the most hypovascular and common rupture site. Option E is incorrect; the text clearly describes a complex, multifaceted supply with a critical hypovascular zone, indicating non-uniformity and implications for healing.
A 68-year-old female with a history of rheumatoid arthritis and long-term corticosteroid use presents with an acute Achilles tendon rupture. She is otherwise healthy and active for her age. The rupture is acute, with a 1.5 cm gap. The surgeon is considering operative versus non-operative management. Based on the case, what is the most significant relative contraindication to surgery in this patient?
Correct Answer: D
The case lists "Relative Contraindications for Surgery" including "Extremely fragile or thin skin (e.g., due to long-term corticosteroid use)." Long-term corticosteroid use significantly compromises skin integrity and wound healing, making it a major concern for surgical complications in this patient.
Option A is incorrect; age is a factor, but not an absolute contraindication, and the case states operative management is 'favored' for young, but non-operative for elderly, implying it's a relative consideration, not an absolute contraindication. Option B is incorrect; acute ruptures can be managed operatively or non-operatively, and the decision is multifactorial. Option C is incorrect; a 1.5 cm gap is considered a 'large tendon gap (>1 cm)' which generally favors operative management. Option E is incorrect; rheumatoid arthritis is mentioned as a systemic condition that may compromise tendon integrity, but it is not listed as an absolute contraindication to surgery, though it would increase surgical risk.
A 40-year-old male undergoes open Achilles tendon repair. The surgeon makes a lateral para-Achilles incision. During closure, the paratenon is carefully repaired. What is the primary rationale for repairing the paratenon, as described in the case?
Correct Answer: B
The case states under 'Closure': "Carefully repair the paratenon with absorbable sutures... This provides an important gliding layer and helps to contain the repair, facilitating revascularization." It also highlights the paratenon's role in providing the primary external blood supply to the tendon's mid-portion, which is crucial for the hypovascular watershed zone.
Option A is incorrect; the sural nerve runs subcutaneously, not within the paratenon. Option C is incorrect; the paratenon is a loose connective tissue sheath, not a primary load-bearing structure for tensile strength. Option D is incorrect; while it helps contain the repair, its primary role is not to prevent scar tissue by isolation. Option E is incorrect; the paratenon is not the primary load-bearing structure; the repaired tendon itself is.
A 50-year-old patient, 5 months post-operative from an open Achilles tendon repair, is struggling with return to sport. He has full range of motion but complains of persistent weakness in push-off and inability to perform a single-leg heel raise more than 5 times. His calf girth is noticeably smaller on the affected side. Based on the potential complications and rehabilitation principles, what is the most likely underlying issue and the recommended next step in his rehabilitation?
Correct Answer: C
The patient's symptoms of persistent weakness in push-off, inability to perform a single-leg heel raise (a key return-to-sport criterion), and reduced calf girth 5 months post-op are classic signs of "Tendon Lengthening/Weakness" as described in the complications section. The management for this is "Often managed conservatively with strengthening exercises. Revision surgery with shortening or augmentation may be considered in severe cases causing significant functional impairment." The rehabilitation section also emphasizes "Eccentric calf strengthening (e.g., calf raises over a step)" as crucial for tendon remodeling and strengthening in later phases.
Option A is incorrect; sural nerve injury typically presents with sensory deficits (numbness, paresthesias), not primary weakness or calf atrophy. Option B is incorrect; while adhesions can cause stiffness, the patient has full ROM, making stiffness less likely the primary issue. Option D is incorrect; while rerupture is a possibility, the description of persistent weakness and inability to perform heel raises, along with calf atrophy, points more towards a lengthened or weak repair rather than an acute rerupture, which would likely present with a sudden event and palpable gap. Option E is incorrect; DVT symptoms are typically swelling, pain, and warmth, not persistent weakness in push-off or calf atrophy.
A 45-year-old male presents with an acute Achilles tendon rupture. He is a highly active individual who desires to return to competitive sports as quickly and safely as possible. He has no significant comorbidities. The rupture gap is 1.2 cm. Based on the summary of key literature and guidelines, which treatment approach is most aligned with his goals and injury characteristics?
Correct Answer: C
The "Current Guidelines and Consensus" section states: "For young, active individuals seeking to return to high-level sports, operative repair combined with early functional rehabilitation is often preferred due to a potentially lower rerupture rate and better strength outcomes." This patient fits this description perfectly (45-year-old, highly active, desires quick return to competitive sports, 1.2 cm gap which is >1cm favoring surgery).
Option A is incorrect; prolonged immobilization is outdated and leads to worse outcomes. Option B is incorrect; while percutaneous repair aims to reduce wound complications, the case highlights that open repair allows for a more robust repair, especially for active individuals, and early functional rehab is key. Option D is incorrect; while modern non-operative protocols have reduced rerupture rates, operative management still generally shows a statistically lower rerupture rate, and the text states operative is 'often preferred' for this demographic. Option E is incorrect; V-Y lengthening is typically for chronic ruptures with significant contracture, not an acute 1.2 cm gap.
The Achilles tendon is composed predominantly of type I collagen fibers, arranged in a highly organized, parallel fashion. The fascicles within the Achilles tendon exhibit a characteristic spiraling course along its length. What is the biomechanical significance of this helical arrangement, as described in the case?
Correct Answer: C
Under 'Tendon Structure and Composition,' the case states: "The fascicles within the Achilles tendon exhibit a characteristic spiraling course along its length, undergoing up to 90 degrees of rotation from proximal to distal. This helical arrangement is thought to distribute stress evenly across the tendon during movement and contribute to its biomechanical efficiency."
Option A is incorrect; while elasticity is important, the primary described function of the spiraling course is stress distribution. Option B is incorrect; the paratenon itself facilitates gliding, not the internal helical arrangement of fascicles. Option D is incorrect; the vascular supply is described as complex and multifaceted, not directly facilitated by the helical arrangement of collagen fibers. Option E is incorrect; the case explicitly states its biomechanical significance.
A 38-year-old male sustains a pronation-external rotation ankle fracture with a displaced lateral malleolus. During open reduction, the surgeon encounters difficulty achieving anatomical reduction despite adequate exposure. The Extensor Digitorum Brevis (EDB) is identified as the interposing structure. Which of the following statements accurately describes the anatomical characteristics of the EDB relevant to its potential for interposition?
Correct Answer: C
The Extensor Digitorum Brevis (EDB) is a small, intrinsic muscle of the foot located on the dorsum. Its medial tendon, often larger and sometimes considered a separate muscle (Extensor Hallucis Brevis), inserts into the dorsal aspect of the proximal phalanx of the great toe. The other three tendons join the lateral three tendons of the Extensor Digitorum Longus (EDL) to insert into the middle and distal phalanges of the 2nd, 3rd, and 4th toes. This specific insertion pattern, particularly of the medial tendon, makes it susceptible to interposition in certain ankle fracture patterns.
Option A is incorrect because the EDB is innervated by the deep peroneal nerve, not the superficial peroneal nerve. Option B is incorrect; its blood supply is from the dorsalis pedis artery (a continuation of the anterior tibial artery), not the posterior tibial artery. Option D is incorrect as the EDB is located on the dorsum of the foot, not in the deep posterior compartment of the leg. Option E is incorrect; the EDB originates from the superolateral surface of the calcaneus, anterior to the calcaneal sulcus, and from the lateral sinus tarsi, not the distal tibia.
A 55-year-old patient presents with a displaced bimalleolar ankle fracture following a high-energy supination-external rotation injury. After initial closed reduction attempts in the emergency department fail to achieve anatomical alignment, the patient is scheduled for ORIF. Intraoperatively, despite a standard lateral approach and direct manipulation of the fibula, the lateral malleolus remains irreducible to the fibular incisura. Based on the provided case, which of the following is the most appropriate next step in management?
Correct Answer: C
The case highlights that a significant challenge arises when anatomical reduction is blocked or incomplete despite appropriate manipulative techniques. Such a scenario mandates careful evaluation for mechanical impediments. The inability to achieve anatomical reduction of the lateral malleolus to the fibular incisura, even with direct manipulation, is a strong indication for soft tissue interposition. The Extensor Digitorum Brevis (EDB) muscle or its tendinous components are specifically mentioned as a less frequently recognized, yet critical, cause of blocked reduction, particularly in specific patterns of lateral malleolar fractures or posteromedial ankle dislocations. Therefore, the most appropriate next step is to visually inspect the fracture site for any interposed soft tissue.
Option A is incorrect because attempting syndesmotic fixation without achieving anatomical reduction of the fibula first will lead to malreduction and poor outcomes. Option B is incorrect as a medial malleolus osteotomy is not indicated for a blocked lateral malleolus reduction. Option D is incorrect; applying increased force against a mechanical block can cause further soft tissue damage and is unlikely to achieve reduction. Option E is incorrect; while a posterior malleolus block can occur, the primary issue described is the irreducibility of the lateral malleolus, which points to a local block on the lateral side, not necessarily a posterior one, unless the posterior malleolus fragment is large and displaced, which is not the primary concern in this specific scenario of lateral malleolus irreducibility.
During open reduction and internal fixation of a displaced lateral malleolus fracture, a surgeon encounters a blocked reduction. Upon inspection, the Extensor Digitorum Brevis (EDB) muscle belly is identified as the interposing structure, as depicted conceptually in the intraoperative field.
What is the most appropriate and least damaging method to manage this EDB interposition to achieve anatomical reduction?
Correct Answer: C
The case explicitly states under 'Management of EDB Interposition' that the correct approach is to 'Gently retract the EDB muscle belly or tendon, usually anteriorly or superiorly, using a small blunt retractor (e.g., Hohmann retractor, Senn retractor, or even a dental pick). Avoid excessive force to prevent muscle damage. Once the EDB is cleared from the fracture site, anatomical reduction should become readily achievable.'
Option A is incorrect because resection of the EDB is unnecessary and would cause permanent damage to the muscle. Option B is incorrect as incising the tendon is an overly aggressive and potentially damaging approach when simple retraction is effective. Option D is incorrect; applying a bone clamp directly to soft tissue like the EDB would cause significant trauma and is not an appropriate surgical technique. Option E is incorrect; a fasciotomy of the anterior compartment is indicated for compartment syndrome, not for clearing an interposing EDB muscle belly from a fracture site.
A 42-year-old patient undergoes ORIF for a displaced bimalleolar ankle fracture. Post-operatively, radiographs reveal persistent widening of the ankle mortise and subtle talar subluxation, despite what was believed to be adequate fixation. The surgeon suspects a missed soft tissue interposition. If the Extensor Digitorum Brevis (EDB) was the missed interposing structure, what is the most likely long-term consequence for this patient?
Correct Answer: C
The case specifically addresses 'Incomplete Reduction' under 'Blocked Reduction and EDB Interposition Complications,' stating: 'If EDB interposition is missed or inadequately addressed, the ankle joint will remain subluxed or malreduced, leading to early onset of post-traumatic arthritis, chronic pain, and functional limitations. This is a critical intraoperative error.'
Option A is a general complication of surgery and immobilization but not the most direct or likely long-term consequence of a missed anatomical malreduction. Option B, CRPS, is a potential complication of any trauma or surgery but is not directly caused by missed EDB interposition. Option D, hardware failure, can occur but is often a consequence of persistent instability or malreduction rather than the primary long-term consequence itself. Option E, superficial peroneal nerve neuropathy, is a risk during the lateral approach but not a direct consequence of missed EDB interposition causing malreduction.
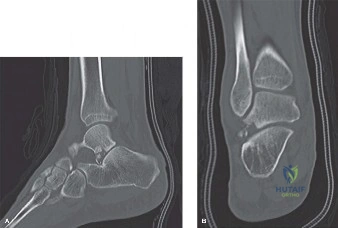
A 60-year-old diabetic patient presents with a complex trimalleolar ankle fracture-dislocation. Initial radiographs show significant comminution and displacement. The surgical team is concerned about potential intra-articular fragments and the precise morphology of the posterior malleolus. Which of the following imaging modalities is most strongly recommended for pre-operative planning in this specific scenario, especially when anticipating potential challenges like blocked reduction?
Correct Answer: C
The case states under 'Pre-Operative Assessment and Imaging' that 'Computed Tomography (CT) Scan is strongly recommended for complex fracture patterns (e.g., trimalleolar, pilon fractures) to delineate articular involvement, fracture comminution, and the presence of osteochondral fragments. It is highly valuable in identifying potential soft tissue interposition pre-operatively, though EDB interposition might not always be clearly evident. It provides a 3D understanding of the deformity and helps plan implant placement.'
Option A, stress radiographs, are primarily used to assess syndesmotic stability, not for detailed fracture morphology or comminution. Option B, MRI, is excellent for soft tissue assessment but is generally not the first-line imaging for acute fracture morphology and is less efficient for bony detail than CT. Option D, contralateral ankle views, are useful for comparison but do not provide the detailed 3D information needed for complex fractures. Option E, bone scintigraphy, is used for metabolic bone activity or occult fractures, not for acute pre-operative planning of complex ankle fractures.
A surgeon is performing an open reduction and internal fixation of a lateral malleolus fracture using a standard longitudinal incision centered over the distal fibula. The image below conceptually illustrates the anatomical region.
During dissection of the skin and subcutaneous tissue, which neurovascular structure is most critical to identify and protect to prevent sensory deficits or painful neuromas?

Correct Answer: E
The case explicitly states under 'Lateral Malleolus Fracture and EDB Interposition' in the 'Dissection' section: 'Carefully incise the skin and subcutaneous tissue. Identify and protect the superficial peroneal nerve (SPN) and its branches, which cross the ankle anteriorly. Aggressive retraction or direct injury to the SPN can lead to sensory deficits or painful neuromas.'
Option A, the posterior tibial nerve, is located in the deep posterior compartment and is not typically at risk during a standard lateral approach. Option B, the saphenous nerve, is located medially and is at risk during a medial malleolus approach. Option C, the sural nerve, is located posterolaterally but is generally posterior to the standard lateral malleolus incision. Option D, the deep peroneal nerve, is in the anterior compartment but is typically deeper and more medial than the superficial peroneal nerve branches that are immediately subcutaneous in the vicinity of a lateral malleolus incision.
Following successful reduction and fixation of the malleolar fractures in a 28-year-old athlete with a pronation-external rotation injury, the surgeon assesses syndesmotic stability. Intraoperative stress tests confirm syndesmotic disruption. The image below shows a common method of syndesmotic fixation.
Which of the following statements regarding syndesmotic fixation is most accurate?
Correct Answer: C
The case states under 'Syndesmotic Fixation' that 'The most common pitfall is over-compression.' Over-compression of the syndesmosis can lead to loss of the normal tibiofibular clear space, altered ankle biomechanics, and potentially pain or early arthritis.
Option A is incorrect; the foot should be placed in neutral dorsiflexion during syndesmotic reduction and fixation to prevent over-compression or malreduction. Option B is incorrect; a quadricortical screw provides increased stiffness compared to a tricortical screw, and neither is designed for dynamic fixation in the way suture button devices are. Option D is incorrect; suture button devices (e.g., TightRope) are increasingly popular and provide dynamic fixation, allowing for micro-motion, and are often used in athletes. Option E is incorrect; syndesmotic screws are typically placed 2-3 cm proximal to the tibial plafond, not 5-6 cm, to ensure adequate purchase while avoiding the articular surface.
A 70-year-old patient with a displaced bimalleolar ankle fracture undergoes ORIF. The primary goal of achieving anatomical reduction and stable internal fixation is to restore the integrity of the ankle mortise. Failure to achieve this anatomical reduction, potentially due to soft tissue interposition like the EDB, directly compromises which of the following biomechanical principles?
Correct Answer: B
The case emphasizes under 'Ankle Stability Biomechanics' that 'Anatomical reduction restores the talar dome's contact with the tibial plafond, ensuring even load distribution and preventing abnormal stresses that can lead to post-traumatic arthrosis. Failure to achieve anatomical reduction, often due to soft tissue interposition like the EDB, directly compromises these biomechanical principles.'
Option A is incorrect; while ankle fractures can affect subtalar motion, the primary biomechanical principle compromised by mortise incongruity is related to the talocrural joint. Option C is incorrect; Achilles tendon tension is not directly related to ankle mortise congruence. Option D is incorrect; blood supply to the talus is critical but not directly compromised by mortise incongruity in this context. Option E is incorrect; early weight-bearing on the calcaneus is a rehabilitation goal, not a biomechanical principle compromised by mortise incongruity.
A 35-year-old male presents with a displaced ankle fracture-dislocation. During closed reduction attempts, the talus remains persistently subluxed despite appropriate manipulative techniques. The orthopedic resident correctly identifies that a mechanical impediment is likely blocking the reduction. Besides the Extensor Digitorum Brevis (EDB), which of the following structures is also a commonly reported cause of blocked ankle fracture reduction?
Correct Answer: C
The case lists several common causes of blocked reduction: 'Common causes of blocked reduction include interposed osteochondral fragments, incarcerated deltoid ligament, tibialis posterior tendon, flexor hallucis longus tendon, or even the posterior talofibular ligament.' It further states, 'Other soft tissue blocks like the tibialis posterior and flexor hallucis longus tendons have been reported, primarily in posteromedial dislocations of the talus.'
Options A, B, D, and E (Plantaris, Peroneus longus, Extensor hallucis longus, and Tibialis anterior tendons) are not explicitly mentioned in the case as commonly reported causes of blocked ankle fracture reduction, although theoretically, any soft tissue could become entrapped in rare circumstances. The Flexor Hallucis Longus (FHL) tendon is specifically highlighted in the provided text.
A 50-year-old patient has undergone ORIF for a stable bimalleolar ankle fracture with syndesmotic repair using a suture button device. The surgeon emphasizes a structured post-operative rehabilitation protocol. In the immediate post-operative period (first 2 weeks), which of the following is the most appropriate weight-bearing and range of motion instruction?
Correct Answer: C
The case outlines the 'Immediate Post-Operative Period' for rehabilitation: 'Weight-Bearing: Non-weight bearing (NWB) on the operative extremity. Crutches, walker, or knee scooter for ambulation.' And for 'Range of Motion (ROM): Active ROM of the toes, knee, and hip of the operative leg to prevent stiffness and promote circulation. Isometric quadriceps and gluteal strengthening exercises.'
Option A and E are incorrect as full weight-bearing is not typically allowed in the immediate post-operative period for ankle fractures requiring ORIF. Option B is incorrect as protected weight-bearing usually begins later (3-4 weeks) for stable fixations, and the initial immobilization is often a splint transitioning to a cast/boot. Option D is incorrect because aggressive active and passive ankle ROM is generally avoided in the immediate post-operative period to protect the healing fracture and soft tissues, especially with syndesmotic repair.
None
