Orthopedic Surgery Board Review: ABOS Part I & AAOS OITE MCQ Cases | Part 21553

Key Takeaway
This module offers 30 advanced multiple-choice questions mirroring ABOS Part I and AAOS OITE exams. It covers high-yield orthopedic topics including ACL reconstruction, pediatric fractures, flexor tendon repair, and sports medicine. Ideal for comprehensive board preparation, it provides detailed explanations and rationales for each case.
Orthopedic Surgery Board Review: ABOS Part I & AAOS OITE MCQ Cases | Part 21553
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
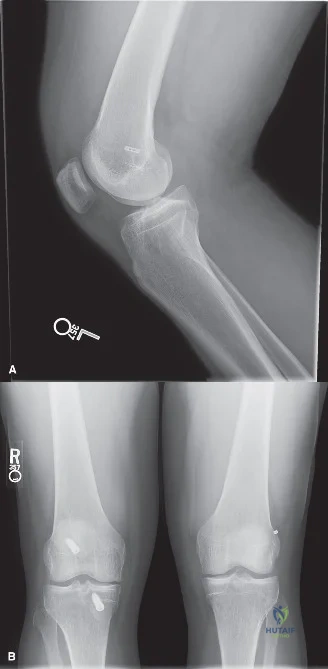
A 24-year-old male ultimate frisbee player presents with a reinjury of his previously reconstructed left knee. He explains that 4 years ago he ruptured his ACL playing basketball and had an allograft repair followed by an uneventful recovery. He returned to sports 8 months after surgery. Radiographs are shown below.
Which factor is most strongly associated with his graft failure?
Explanation
Correct Answer: C
In younger, active individuals, allograft ACL reconstructions have been consistently shown to have a significantly higher failure rate compared to autograft reconstructions. While inadequate fixation and tunnel malposition (femoral or tibial) are common causes of graft failure, the choice of allograft in a young, high-demand athlete is a major contributing factor to reinjury. Meniscal pathology, while impacting long-term knee health, is not directly associated with the primary cause of graft re-tear.
Question 2
A 24-year-old male ultimate frisbee player requires a revision ACL reconstruction. In choosing between a single-stage ACL revision and a two-step, staged ACL revision (removal of hardware with bone grafting, followed by later revision ACL reconstruction), which finding most strongly favors a staged revision?
Explanation
Correct Answer: A
A staged revision is primarily indicated when the existing tunnels from the previous ACL reconstruction are too wide, preventing reliable graft fixation, or if their position significantly compromises the accurate placement of new tunnels for the revision ACL. In such cases, the initial stage involves removing hardware and bone grafting the tunnels to allow for healing and consolidation, followed by the definitive revision reconstruction at a later date. A vertical femoral tunnel can often be addressed in a single stage by creating a new, anatomically correct tunnel. Retained hardware can typically be removed during a single-stage procedure. The type of prior graft (autograft vs. allograft) or the presence of a meniscal tear does not inherently necessitate a staged approach.
Question 3
During a revision ACL reconstruction, the graft impinges in the notch as the knee is extended, making terminal extension 5 degrees short of straight. Which factor is most likely responsible for this limitation in range of motion?
Explanation
Correct Answer: C
Graft impingement in the intercondylar notch, leading to a loss of terminal knee extension, is most commonly caused by an anteriorly placed tibial tunnel. If the tibial tunnel is too anterior, the graft will be taut and impinge against the roof of the intercondylar notch during knee extension. Femoral tunnel position primarily affects rotational stability and anterior translation, not typically terminal extension impingement. A tibial tunnel that is too posterior would lead to graft laxity rather than impingement. The type of graft (autograft or allograft) does not inherently affect the risk of impingement based on tunnel placement.
Question 4
A 56-year-old mason presents with acute swelling of his left knee after prolonged kneeling. He has a firm, non-tender prepatellar bursa without erythema. Which physical finding would be LEAST suggestive of septic bursitis if it were present?
Explanation
Correct Answer: C
Septic bursitis is an infection of the bursa, often presenting with signs of inflammation and systemic symptoms. Findings highly suggestive of septic bursitis include fever (>37.8°C), a significant temperature difference over the bursa compared to surrounding skin (>2.2°C), and overlying skin lesions (e.g., cellulitis, abrasions). Significant local erythema is also a classic sign of infection. Pain with passive range of motion of the knee, however, is more characteristic of an intra-articular process (e.g., arthritis, meniscal tear) rather than an isolated bursitis, whether septic or aseptic. Bursitis pain is typically worse with direct pressure or active motion involving the bursa.
Question 5
A 27-year-old soccer player sustains a PCL injury after falling onto a flexed knee. On examination, there is a slight sag and posterior translation of the tibia less than one centimeter. The initial management of this isolated PCL injury should primarily emphasize:
Explanation
Correct Answer: D
For isolated PCL injuries, especially those with minimal posterior translation, non-operative management is often successful. The primary focus of rehabilitation is quadriceps strengthening. The quadriceps muscle provides an anteriorly directed force on the tibia, which can dynamically stabilize the knee and counteract the posterior laxity caused by the PCL injury. Hamstring strengthening, while important for overall knee health, can exacerbate posterior translation. Strict immobilization can lead to stiffness and atrophy. Open chain exercises may place undue stress on the PCL. Surgical reconstruction is typically reserved for higher-grade PCL injuries or combined ligamentous injuries.
Question 6
A 39-year-old catcher presents with an acutely locked right knee after standing up quickly. Her knee has a limited range of motion, moving from 30 to 45 degrees of knee flexion. Beyond this arc, the endpoint is firm and painful. Anterior-posterior and lateral x-rays reveal an aligned knee without fracture or dislocation. What is the most appropriate next step in her care?
Explanation
Correct Answer: B
An acutely locked knee with a firm endpoint and normal radiographs strongly suggests a mechanical block to motion, most commonly a meniscal tear (e.g., bucket-handle tear) or a loose body. An MRI is the gold standard imaging modality for evaluating the integrity of the menisci, articular cartilage, and identifying loose bodies, providing crucial information for diagnosis and surgical planning. Corticosteroid injections or oral anti-inflammatories will not address a mechanical block. While a long-leg splint might provide comfort, it does not advance the diagnosis or treatment. Attempting a closed reduction without a clear diagnosis from MRI could be inappropriate or ineffective if the block is due to a large meniscal tear or loose body.
Question 7
A 17-year-old female runner presents with increased leg pain and is diagnosed with a stress fracture. Her physician is concerned about the female athlete triad. Which of the following is NOT considered one of the three core components of the female athlete triad?
Explanation
Correct Answer: D
The female athlete triad is a syndrome characterized by three interrelated components: 1) Low energy availability (with or without disordered eating), 2) Menstrual dysfunction (e.g., amenorrhea), and 3) Low bone mineral density (e.g., osteoporosis). Abulia refers to a lack of will or initiative and is a neurological or psychological symptom not directly part of the triad. Low energy availability is now recognized as the underlying cause that links disordered eating to menstrual dysfunction and low bone mineral density.
Question 8
A 17-year-old female runner with a suspected stress fracture has bony edema on MRI, but no clear fracture line on radiographs. Her pain is present with weight bearing. Which of the following stress fracture locations carries the highest risk for fracture propagation and complications?
Explanation
Correct Answer: D
Stress fractures are classified by their risk of progression to complete fracture or nonunion. High-risk locations include the superior femoral neck, anterior tibial diaphysis, navicular, base of the fifth metatarsal, and the neck of the talus. These sites are prone to tensile forces or poor blood supply, making them more susceptible to complications. The calcaneus, medial malleolus, first metatarsal, and inferior femoral neck are generally considered lower to intermediate risk sites.
Question 9
During a preparticipation physical examination for a 12-year-old girl interested in soccer, which of the following historical findings would be considered LEAST worrisome for sports participation?
Explanation
Correct Answer: B
The primary goal of a preparticipation physical examination is to identify life-threatening conditions or conditions that may predispose an athlete to injury or illness during sports. A history of Long QT syndrome, exertional shortness of breath (suggesting asthma or cardiac issues), missed or absent menses (a component of the female athlete triad, indicating potential bone health issues), and prior heat stroke (indicating susceptibility to heat illness) are all significant red flags that require further evaluation before sports participation. A healed long-bone fracture, while important to review for any residual deficits, is generally the least worrisome of the options, assuming it has healed without complications and full function has been restored.
Question 10
A 16-year-old male athlete collapses during a basketball game and is diagnosed with sudden cardiac death. What is the most common underlying cause of sudden cardiac death in young athletes?
Explanation
Correct Answer: D
Hypertrophic cardiomyopathy (HCM) is the most common cause of sudden cardiac death in young athletes. It is an inherited condition characterized by abnormal thickening of the heart muscle, particularly the left ventricle, which can obstruct blood flow and lead to dangerous arrhythmias during physical exertion. While coronary artery abnormalities, Long QT syndrome, Commotio cordis (a blunt chest trauma causing ventricular fibrillation), and Marfan syndrome (which can lead to aortic dissection) are all causes of sudden cardiac death in athletes, HCM accounts for the largest proportion of these tragic events.
Question 11
A 7-year-old girl, weighing 35 kg, presents with a right femoral shaft fracture after playing tackle football. Initial radiographs are shown in and . She is hemodynamically stable with an intact neurovascular examination. Based on her age, weight, and fracture characteristics, what is the most appropriate definitive treatment?

Explanation
Correct Answer: D
The patient is a 7-year-old girl weighing 35 kg with a diaphyseal femur fracture. According to the provided guidelines for femur fracture treatment by age, flexible intramedullary nails are the optimal choice for children aged 6-8 years. While a spica cast is an option for this age group, flexible nailing is generally preferred for its benefits to the patient and family, allowing for earlier mobilization and easier care. Lateral trochanteric intramedullary nails are typically reserved for children 9 years of age or older, those weighing over 49 kg, or those with length-unstable fractures, none of which apply to this patient. External fixation is usually reserved for severely comminuted or open fractures, or in the setting of damage control orthopaedics, which is not indicated here. Traction followed by delayed spica casting is a less preferred option compared to flexible nailing for this age and weight.
Question 12
Following the decision to proceed with flexible intramedullary nailing for the 7-year-old patient, you measure the preoperative x-ray at the femoral isthmus, which is 7.5 mm. To achieve optimal stability, what size nails should be used to obtain approximately 80% canal fill?
Explanation
Correct Answer: B
The goal for flexible intramedullary nail fixation of a femur fracture is to achieve approximately 80% canal fill. The patient's femoral isthmus measures 7.5 mm. To calculate the appropriate nail size, we need to find two nails whose combined diameter is 80% of 7.5 mm. 80% of 7.5 mm is 0.80 * 7.5 mm = 6.0 mm. Therefore, using two 3-mm nails (3 mm + 3 mm = 6 mm) will achieve exactly 80% canal fill. Option A (two 2.5-mm nails = 5 mm) would result in 67% canal fill (5/7.5), which is less than ideal and could lead to fixation failure. Option C (one 3.0-mm and one 3.5-mm nail = 6.5 mm) would result in 87% canal fill (6.5/7.5), which is greater than 80% and increases the risk of complications, as does using nails of different sizes which can contribute to loss of reduction and malalignment. Option D (two 3.5-mm nails = 7 mm) would result in 93% canal fill (7/7.5), which is too high. Option E (one 2.5-mm and one 3.0-mm nail = 5.5 mm) would result in 73% canal fill (5.5/7.5), which is also suboptimal.
Question 13
When discussing the potential complications of flexible intramedullary nailing for a pediatric femoral shaft fracture with the patient's parents, which of the following is the most common complication you should inform them about?
Explanation
Correct Answer: C
The most common complication associated with flexible intramedullary nailing for pediatric femur fractures is pain or irritation at the insertion sites, typically around the knee where the nails exit the bone. This is often due to the ends of the nails irritating the surrounding soft tissues. Studies have shown relatively low rates of infection, significant bleeding, and loss of reduction (especially with length-stable fractures) when proper surgical technique is employed. Delayed union or nonunion is also a rare complication in pediatric femur fractures treated with flexible nails. To minimize the risk of insertion site irritation, it is suggested that the nails be left no more than 25 mm out of the bone.
Question 14
During the preoperative discussion with the family regarding the 7-year-old's femur fracture, they inquire about potential long-term complications, specifically limb length discrepancy. What information should you provide regarding the risk and typical amount of ipsilateral overgrowth that may occur following a femoral shaft fracture in this age group?
Explanation
Correct Answer: C
Children between the ages of 2 and 10 years are at the highest risk for ipsilateral overgrowth following a femoral shaft fracture. While the reported range of overgrowth can be broad (approximately 4 to 25 mm), the average amount of overgrowth observed in this age group is typically around 9 mm. Therefore, stating that there is no risk of overgrowth at this age (Option A) or that it only occurs in children under 2 or over 10 (Option E) is incorrect. Options B and D either underestimate or overestimate the average amount of overgrowth commonly seen in this specific age range.
Question 15
A 14-year-old boy presents with right knee pain after a basketball injury. CT imaging, as shown in , reveals a tibial tubercle fracture. Which of the following conditions is considered a significant risk factor for this type of fracture?

Explanation
Correct Answer: B
Tibial tubercle fractures occur more commonly in adolescents who have a history of Osgood–Schlatter disease. Osgood–Schlatter disease is an overuse injury characterized by repetitive strain across the tibial tubercle apophysis, which can weaken the apophysis and predispose it to avulsion fractures. While a direct causal relationship is not always definitively proven, the association is well-recognized. Patellofemoral syndrome involves anterior knee pain related to overuse but is not a direct risk factor for tibial tubercle avulsion. Sinding-Larsen–Johansson syndrome is similar to Osgood–Schlatter but affects the inferior pole of the patella, not the tibial tubercle. Patellar tendonitis is inflammation of the patellar tendon and is not specifically linked to an increased risk of tibial tubercle fractures. Chondromalacia patellae refers to softening of the articular cartilage of the patella and is unrelated to tibial tubercle fractures.
Question 16
A 14-year-old boy sustains a tibial tubercle fracture. You are concerned about the potential for compartment syndrome. Which compartment is most commonly at risk, and what specific vessel is primarily implicated in this injury?
Explanation
Correct Answer: B
Tibial tubercle fractures, particularly displaced ones, carry a significant risk of developing an isolated anterior compartment syndrome. This is primarily due to injury to the recurrent anterior tibial artery, which is located in close proximity to the tibial tubercle and can be damaged during the fracture event or subsequent swelling. The anterior tibial artery itself is a larger vessel but the recurrent branch is more directly involved in the local vascularity around the tibial tubercle. The medial inferior geniculate artery supplies the knee joint but is not the primary vessel implicated in compartment syndrome with this specific fracture. The lateral compartment and fibular artery are not typically involved in compartment syndrome secondary to a tibial tubercle fracture.
Question 17
The 14-year-old boy has a displaced Type III tibial tubercle fracture, as seen on CT. Given the displacement and the patient's age, what is the most appropriate definitive treatment strategy? An example of fixation is shown in .

Explanation
Correct Answer: D
For a displaced Type III tibial tubercle fracture in an adolescent, an open reduction is necessary to achieve anatomical alignment. Closed reduction with casting or pinning (Options A and B) is insufficient for displaced fractures of this type. While pinning (Option C) can be used, screw fixation is generally preferred over pins or sutures in larger adolescents due to the significant pulling forces exerted by the quadriceps and to provide more stable fixation, allowing for earlier range of motion. Furthermore, Type III fractures are associated with a risk of intra-articular pathology (e.g., meniscal injury, soft tissue incarceration), making an arthrotomy (or arthroscopy) essential to ensure anatomical joint surface reduction and address any associated injuries. Suture fixation (Option E) might be considered in very young adolescents with concerns about growth plate integrity, but screw fixation is superior for stability in older adolescents where the growth plate is already closing.
Question 18
A 13-year-old male presents with acute right ankle pain after a soccer injury. An anteroposterior radiograph of his ankle is shown in . Which of the following answers correctly pairs the eponym commonly used to describe this injury with the affected anatomic structure?

Explanation
Correct Answer: B
The radiograph depicts a Tillaux fracture, which is a transitional ankle fracture in adolescents involving an avulsion of the anterolateral distal tibial epiphysis. This fragment remains attached to the anterior inferior tibiofibular ligament (AITFL), which is one of the primary syndesmotic ligaments of the ankle. Chopart injuries involve the midtarsal joint, not the distal tibia. The Chaput fragment is another eponym for the same fracture piece attached to the AITFL, but it is more commonly used in adult ankle fractures. The anterior talofibular ligament (ATFL) is the most commonly injured ligament in lateral ankle sprains, not typically involved in a Tillaux fracture.
Question 19
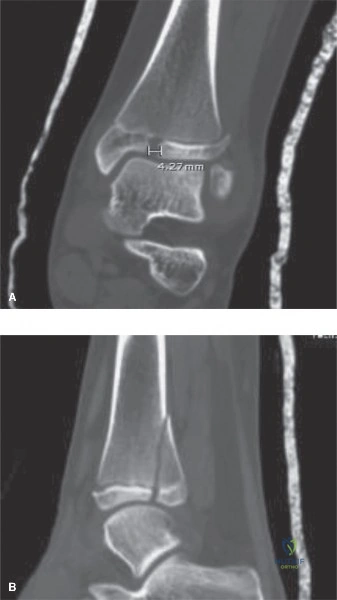
A 13-year-old male presents with a left ankle injury sustained in a soccer match. Radiographs are shown in and . Based on the available imaging, you diagnose this patient with a triplane fracture. Which of the following correctly describes the Salter–Harris classification appearance of a classic triplane fracture on different radiographic views?

Explanation
Correct Answer: B
Classically, a triplane fracture of the distal tibia presents with a characteristic radiographic appearance: it appears as a Salter–Harris II fracture on lateral radiographs (sagittal view) and as a Salter–Harris III fracture (which corresponds to the Tillaux fragment) on coronal imaging (anteroposterior or AP view). This unique combination reflects the fracture's involvement of the physis, epiphysis, and metaphysis in different planes. Therefore, option B accurately describes this classic presentation. Other combinations of Salter-Harris classifications on these views do not represent the typical triplane fracture pattern.
Question 20
Following a closed reduction attempt for the triplane ankle fracture, post-reduction CT images are obtained, as shown in . The images reveal a residual articular gap of >4 mm. Based on this finding, what is the most appropriate next step in management?
Explanation
Correct Answer: D
A residual articular diastasis of greater than 2 mm after reduction of a triplane fracture is generally considered an indication for surgical intervention to minimize the risk of abnormal joint contact forces and subsequent degenerative changes. This patient has a residual articular gap of >4 mm, clearly indicating the need for surgery. While surgical approaches vary, a common and effective method involves reducing the articular surface and fixing it with all-epiphyseal lag screws placed perpendicular to the fracture line in an extraphyseal and extra-articular manner. Given that the patient has a large metaphyseal fragment, additional fixation with lag screws placed across this metaphyseal spike (in addition to epiphyseal screws) would optimize fracture fixation and stability. Therefore, a construct involving lag screws in both the epiphyseal and metaphyseal fragments is the most comprehensive and appropriate surgical approach. Continued immobilization (Option A) is not indicated due to the significant residual displacement. Physeal-spanning compression plates (Option E) are generally not indicated for these fractures due to the risk of physeal arrest.
Question 21
A 32-year-old right-hand dominant male presents with a deep laceration to the volar aspect of his left middle finger, sustained while cutting an avocado. He reports that his finger was tightly flexed around the avocado at the moment of injury. Clinically, he has a complete loss of active PIP and DIP flexion in the affected digit. During surgical planning, the most critical implication of the patient's finger position at the time of injury is:
Explanation
Correct Answer: C
The patient's history of the finger being tightly flexed at the moment of laceration is a critical detail in flexor tendon injuries. When a flexor tendon is lacerated in a flexed position, the distal stump remains near the laceration site. However, once the finger is extended (as it would be during examination or initial wound care), the proximal tendon stump retracts significantly due to the pull of the muscle belly in the forearm. This retraction can be substantial, often pulling the stump proximal to the A1 pulley, into the palm, or even into the distal forearm. Therefore, surgical planning must account for the need for a more extensive proximal exploration, potentially requiring a counter-incision in the palm, to retrieve the retracted proximal tendon stump. This phenomenon is a well-known challenge in Zone II flexor tendon repairs.
Option A is incorrect; while digital nerve injuries are common, the position of the finger at injury primarily affects tendon retraction, not necessarily increasing nerve stretch risk. Option B is incorrect; a flexed position does not inherently lead to a partial laceration; a sharp knife can still cause a complete transection. Option D is incorrect; while some pulleys might be less taut, the primary implication is tendon retraction. Option E is incorrect; the timing of repair (primary vs. delayed) is dictated by the time from injury and wound conditions, not solely by the finger's position at injury, although significant retraction can make primary repair more challenging if delayed too long.
Question 22
Upon arrival at the emergency department, the patient with an acute flexor tendon laceration in Zone II received prophylactic intravenous antibiotics. Given the mechanism of injury (kitchen knife) and the location, which of the following antibiotic choices is most appropriate for initial empiric coverage?
Explanation
Correct Answer: C
For acute penetrating injuries to the hand, particularly those involving flexor tendons, the primary concern for infection is typically skin flora, most commonly Staphylococcus aureus and Streptococcus species. A first-generation cephalosporin, such as Cefazolin, provides excellent coverage against these common gram-positive organisms and is generally well-tolerated. The case specifically mentions the administration of a first-generation cephalosporin, aligning with standard practice for clean-contaminated wounds.
Option A (Vancomycin and Piperacillin-Tazobactam) would be overly broad for an initial empiric choice in this scenario, typically reserved for more severe infections, immunocompromised patients, or those with specific risk factors for MRSA or polymicrobial infections (e.g., human/animal bites, farm injuries). Option B (Ciprofloxacin and Metronidazole) targets gram-negative and anaerobic bacteria, which are not the primary concern for a clean knife injury. Option D (Clindamycin and Gentamicin) is also a broad-spectrum combination, with gentamicin covering gram-negatives and clindamycin covering anaerobes and some gram-positives, but Cefazolin is simpler and usually sufficient. Option E (Doxycycline) is not a first-line empiric choice for acute penetrating hand injuries.
Question 23
A 32-year-old male presents with a deep laceration to the volar aspect of his left middle finger, as shown in the image. Clinical examination reveals a 2.5 cm transverse laceration over the middle phalanx. He is unable to actively flex his PIP and DIP joints, but passive range of motion is full. Sensation is diminished along the radial digital nerve distribution. Based on these findings and the provided image, what is the most likely diagnosis and anatomical zone of injury?

Explanation
Correct Answer: C
The image shows a laceration on the volar aspect of the middle finger. The clinical findings are key: complete inability to actively flex both the PIP (proximal interphalangeal) and DIP (distal interphalangeal) joints. The FDS tendon is primarily responsible for PIP flexion, and the FDP tendon is responsible for DIP flexion. Loss of both indicates a complete transection of both tendons. The laceration location 'over the middle phalanx' places the injury squarely in Flexor Tendon Zone II, which extends from the A1 pulley to the FDS insertion on the middle phalanx. The diminished sensation along the radial digital nerve is a common associated injury but does not change the primary tendon diagnosis.
Option A is incorrect because an FDP avulsion (Jersey finger) typically presents with an inability to flex the DIP joint, but PIP flexion (FDS) would be intact. Zone I is distal to the FDS insertion, involving only the FDP. Option B is incorrect because a partial FDS laceration would likely present with weakness, not complete loss, of PIP flexion, and Zone III is in the palm. Option D is incorrect because an isolated digital nerve laceration would cause sensory deficits but preserve active tendon function. Zone IV is at the wrist. Option E is incorrect because an extensor tendon laceration would affect finger extension, not flexion, and Zone V is at the MCP joint level on the dorsal aspect.
Question 24
During the clinical examination, the patient demonstrated diminished sensation along the radial digital nerve distribution of the left middle finger, with a static two-point discrimination of 8 mm. Sensation along the ulnar digital nerve was intact (4 mm). What is the most appropriate management strategy for this radial digital nerve injury in the acute setting?
Explanation
Correct Answer: B
The case explicitly states that the radial digital nerve was found to be approximately 80% transected during surgical exploration, confirming the clinical suspicion of a severe partial laceration. A two-point discrimination of 8 mm is abnormal and indicates a significant sensory deficit. In the setting of an open wound and a clear clinical deficit, a digital nerve laceration, whether partial or complete, warrants immediate surgical exploration and microsurgical repair. Performing this repair during the same surgical setting as the flexor tendon repair is the standard of care. This allows for primary repair, which generally yields the best outcomes, and avoids the complications of delayed repair such as nerve retraction and scar tissue formation.
Option A is incorrect; while some very minor neuropraxic injuries might recover, a significant laceration (80% transection) will not spontaneously recover adequate function. Option C is incorrect; delayed nerve grafting is reserved for cases where primary repair is not possible due to significant nerve gap or chronic injury. Option D is incorrect; corticosteroids are not indicated for nerve lacerations. Option E is incorrect; NCS/EMG are typically used for chronic nerve compression or entrapment neuropathies, not for acute, open lacerations where the diagnosis is clinically evident and confirmed by exploration.
Question 25
Prior to surgical intervention for the acute flexor tendon laceration, standard posteroanterior (PA), true lateral, and oblique radiographs of the left hand and middle finger were obtained. In this specific clinical scenario, the primary indication for these plain film radiographs is to:
Explanation
Correct Answer: C
The case explicitly states the primary indications for plain film radiography in the setting of a sharp penetrating injury: 1) Exclusion of Foreign Bodies (e.g., metallic shards, glass), and 2) Assessment of Osseous Integrity (e.g., phalangeal fractures, cortical nicking, bony avulsions). While the patient reported a knife injury, it's crucial to rule out other potential foreign bodies or associated bony trauma that might complicate the repair or recovery. The radiographs in this patient demonstrated normal osseous architecture and no foreign bodies.
Option A is incorrect; radiographs are not effective for assessing tendon retraction or gap formation, which are soft tissue structures. Option B is incorrect; radiographs cannot evaluate the integrity of annular pulleys. Option D is incorrect; the anatomical zone of injury is determined clinically by the laceration's location relative to anatomical landmarks and tendon function deficits. Option E is incorrect; while soft tissue swelling can be noted on radiographs, it's not the primary indication, and other imaging modalities or clinical examination are better for quantifying soft tissue changes.
Question 26
A 28-year-old male presents to the emergency department after sustaining a laceration to the volar aspect of his left ring finger. On examination, he is able to actively flex his PIP joint against resistance, but he has a complete inability to actively flex his DIP joint. Radiographs show a small bony fragment avulsed from the volar base of the distal phalanx. Based on the provided case's differential diagnosis, what is the most likely diagnosis?
Explanation
Correct Answer: C
The clinical presentation of intact active PIP flexion but absent active DIP flexion, combined with a bony avulsion fragment from the volar base of the distal phalanx on radiographs, is pathognomonic for a Flexor Digitorum Profundus (FDP) avulsion, commonly known as a Jersey Finger. The FDP tendon inserts onto the volar base of the distal phalanx, and its avulsion results in the loss of DIP flexion. The intact PIP flexion indicates that the FDS tendon, which inserts on the middle phalanx and flexes the PIP joint, is functional.
Option A is incorrect because a complete Zone II FDS and FDP laceration would result in the loss of both PIP and DIP flexion. Option B is incorrect because a partial FDP laceration would typically present with weakened, but not completely absent, DIP flexion. Option D is incorrect because an isolated digital nerve laceration would primarily cause sensory deficits, not a loss of active tendon function. Option E is incorrect because an extrinsic flexor muscle belly injury would likely affect multiple digits or present with more diffuse weakness, and the specific bony avulsion points away from this diagnosis.
Question 27
The surgical team opted for the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique for the flexor tendon repair. Which of the following is the most significant advantage of using WALANT for a Zone II flexor tendon repair, as highlighted in the case?
Explanation
Correct Answer: C
The case explicitly states that the profound advantage of WALANT in Zone II repairs is the ability to communicate with the conscious patient intraoperatively. This allows the surgeon to ask the patient to actively flex and extend the digit after the tendon repair is complete. This provides real-time assessment of the repair construct's strength, direct observation of tendon gliding through the pulleys, and immediate identification and resolution of any triggering or catching before wound closure. This intraoperative validation is a hallmark benefit that significantly contributes to optimizing outcomes and preventing complications like adhesions or impingement.
Option A is incorrect; while WALANT can be efficient, its primary advantage is not necessarily faster anesthetic onset or reduced overall operative time compared to other methods. Option B is incorrect; a Certified Hand Therapist is crucial for postoperative rehabilitation regardless of the anesthesia technique. Option D is incorrect; while epinephrine provides hemostasis, the primary mechanism for infection prevention is sterile technique and prophylactic antibiotics, not the anesthetic itself. Option E is incorrect; while WALANT can be more cost-effective, the most significant clinical advantage highlighted in the case for Zone II repair is the intraoperative assessment.
Question 28
During the repair of the Flexor Digitorum Profundus (FDP) tendon in Zone II, the surgeon utilized a 4-strand modified Kessler core suture technique with 3-0 braided non-absorbable suture, followed by a continuous epitendinous suture with 5-0 monofilament non-absorbable suture. What is the primary biomechanical purpose of adding the epitendinous suture to the core repair?
Explanation
Correct Answer: C
The case clearly outlines the dual functions of the epitendinous suture: 'The epitendinous suture serves two critical functions: it increases the overall tensile strength of the repair by 20-30%, and it neatly tucks in the exposed collagen fibrils at the tendon ends, creating a smooth surface that minimizes gliding resistance and prevents postoperative adhesions.' While the core suture provides the bulk of the initial tensile strength, the epitendinous suture significantly augments it and, crucially, creates a smooth interface that reduces friction and adhesion formation within the tight fibro-osseous sheath of Zone II.
Option A is incorrect; the core suture provides the majority of the tensile strength, not the epitendinous suture. Option B is incorrect; the Quadrigia effect is prevented by ensuring end-to-end repair without excessive shortening, not directly by the epitendinous suture. Option D is incorrect; revascularization occurs through diffusion and the vincula, not primarily through the epitendinous suture. Option E is incorrect; even with a robust repair, early active motion protocols still require protective splinting to prevent rupture during the initial healing phase.
Question 29
Immediately following the flexor tendon repair, a custom thermoplastic dorsal blocking splint was applied. What is the correct positioning of the hand and digits within this splint to relieve tension on the flexor apparatus and facilitate early active motion?
Explanation
Correct Answer: C
The case explicitly details the critical positioning for the dorsal blocking splint: 'Wrist: 20 to 30 degrees of palmar flexion. Metacarpophalangeal (MCP) Joints: 50 to 70 degrees of flexion. Interphalangeal (PIP and DIP) Joints: Full extension (neutral).' This specific position places the flexor tendons in a relaxed state, minimizing tension on the repair site while still allowing for controlled, protected active extension within the splint and passive or place-and-hold flexion exercises as part of an Early Active Motion (EAM) protocol.
Options A, B, D, and E describe incorrect or suboptimal splint positions that would either place excessive tension on the repair, limit necessary motion, or not adequately protect the healing tendons.
Question 30
A patient undergoes a Zone II flexor tendon repair. Six weeks postoperatively, during a hand therapy session, the patient attempts to make a fist. The repaired middle finger achieves full flexion, but the adjacent ring and small fingers are unable to achieve full flexion, appearing to be 'blocked' by the middle finger. What is the most likely cause of this phenomenon?
Explanation
Correct Answer: D
The scenario described, where the repaired middle finger achieves full flexion but the adjacent, uninjured ring and small fingers are unable to achieve full flexion, is the classic presentation of the Quadrigia effect. As explained in the case, 'The Flexor Digitorum Profundus muscle has a common muscle belly in the proximal forearm that gives rise to the tendons of the middle, ring, and small fingers. Because these tendons act in concert, over-advancing the FDP tendon during repair (typically by more than 1 cm) will artificially shorten that specific tendon. When the patient attempts to make a fist, the shortened repaired tendon reaches maximum excursion early, physically blocking the common muscle belly from contracting further. This prevents the adjacent, uninjured fingers from achieving full flexion.'
Option A is incorrect; Lumbrical Plus finger presents as paradoxical PIP extension when attempting to grip, not a blocking of adjacent fingers. Option B is incorrect; tendon adhesions would primarily limit active flexion of the repaired finger, not block adjacent uninjured fingers. Option C is incorrect; a tendon rupture would result in a loss of active flexion in the repaired finger, not a blocking effect on adjacent digits. Option E is incorrect; intrinsic muscle contracture would typically affect MCP flexion and IP extension, not specifically block adjacent FDP function in this manner.
Question 31
A 28-year-old male presents with persistent loss of terminal extension six months after an anterior cruciate ligament (ACL) reconstruction. Lateral radiographs reveal that the entire tibial tunnel is positioned entirely anterior to Blumensaat's line when the knee is in full extension. Which of the following complications is most likely causing his loss of motion?
Explanation
Question 32
A patient complains of severe knee stiffness and an inability to flex the knee past 80 degrees following an ACL reconstruction. Intraoperative notes and postoperative imaging confirm that the femoral tunnel was drilled significantly anterior (high) to the anatomic footprint. What is the kinematic consequence of this technical error?
Explanation
Question 33
The posterior cruciate ligament (PCL) is the primary restraint to posterior tibial translation and is composed of two distinct functional bundles. Which of the following best describes their biomechanical behavior during knee motion?
Explanation
Question 34
A 25-year-old athlete sustains a twisting injury to the knee. On physical examination, the dial test demonstrates a 15-degree increase in external rotation compared to the uninjured contralateral knee at 30 degrees of flexion. At 90 degrees of flexion, the external rotation is symmetric bilaterally. What is the most likely injury pattern?
Explanation
Question 35
Which bundle of the posterior cruciate ligament (PCL) is tightest in deep knee flexion?
Explanation
Question 36
A patient presents with a knee injury. The dial test shows 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side, but symmetric rotation at 90 degrees. What is the most likely diagnosis?
Explanation
Question 37
During which phase of ACL graft incorporation does an autograft typically exhibit its lowest mechanical strength?
Explanation
Question 38
A 45-year-old female sustains a medial meniscus posterior root tear. Biomechanically, the loss of hoop stresses in this condition is most equivalent to which of the following?
Explanation
Question 39
During reconstruction of the medial patellofemoral ligament (MPFL), identifying the anatomic femoral attachment is critical. According to Schöttle, where is this point located radiographically?
Explanation
Question 40
A patient presents with a painful lack of terminal knee extension 4 months following an ACL reconstruction. MRI demonstrates a nodular mass in the anterior intercondylar notch. What is the histologic composition of this mass?
Explanation
Question 41
Which of the following anatomic factors is most strongly associated with an increased risk of non-contact ACL ruptures in female athletes?
Explanation
Question 42
The primary arterial blood supply to the anterior and posterior cruciate ligaments is derived directly from which of the following vessels?
Explanation
Question 43
A patient with a chronic ACL-deficient knee undergoes a high tibial osteotomy (HTO) in preparation for a staged ligament reconstruction. To best protect the future ACL graft, how should the posterior tibial slope be managed during the HTO?
Explanation
Question 44
The classic, most common anatomic location for an osteochondritis dissecans (OCD) lesion of the knee is the:
Explanation
Question 45
During an ACL reconstruction, placing the tibial tunnel too far anteriorly most commonly leads to which of the following complications?
Explanation
Question 46
If the femoral tunnel during an ACL reconstruction is placed too far anteriorly (shallow) in the intercondylar notch, what resulting kinematic mismatch will occur?
Explanation
Question 47
When counseling a 17-year-old competitive soccer player regarding ACL graft choices, what is the most accurate evidence-based information regarding the use of cadaveric allografts in her specific demographic?
Explanation
Question 48
A patient presents with a grossly dislocated knee (Schenck KD-III). Following closed reduction, the Ankle-Brachial Index (ABI) is calculated to be 0.8. What is the most appropriate next step in management?
Explanation
Question 49
A radiograph of an acutely injured knee demonstrates an avulsion fracture of the lateral tibial plateau.
This "Segond fracture" is pathognomonic for a tear of the ACL. Which specific ligamentous structure is directly responsible for this bony avulsion?
Explanation
Question 50
The superficial medial collateral ligament (sMCL) is the primary static restraint to valgus stress. At what degree of knee flexion does it provide the maximum percentage of valgus restraint?
Explanation
Question 51
Regarding the zonal anatomy of articular cartilage, which zone contains the highest concentration of proteoglycans and features collagen fibrils oriented perpendicular to the articular surface?
Explanation
Question 52
During an inside-out repair of the posterior horn of the medial meniscus, which nerve is most at risk of iatrogenic injury when placing the posteromedial incision?
Explanation
Question 53
Current evidence-based consensus guidelines suggest that athletes should delay returning to unrestricted pivoting sports following an ACL reconstruction until their Limb Symmetry Index (LSI) on functional hop testing reaches at least what threshold?
Explanation
Question 54
During primary ACL reconstruction using a bone-patellar tendon-bone autograft, the surgeon inadvertently places the femoral tunnel excessively anterior. Which clinical finding is most likely to result from this technical error?
Explanation
Question 55
A 19-year-old female presents with persistent knee instability 1 year after ACL reconstruction. Exam demonstrates a 1A Lachman but a grade 3 pivot shift.
What is the most likely technical cause for this specific failure pattern?
Explanation
Question 56
When planning a revision ACL reconstruction, which of the following findings is the most universally accepted absolute indication for a two-stage approach with bone grafting prior to revision?
Explanation
Question 57
A 25-year-old male undergoes arthroscopy for an ACL tear. The surgeon suspects a concurrent meniscal ramp lesion. Which of the following describes the most sensitive arthroscopic method to diagnose this specific lesion?
Explanation
Question 58
A 16-year-old female soccer player undergoes primary ACL reconstruction with a hamstring autograft. Which of the following factors represents the most significant independent risk factor for subsequent ACL graft failure in this patient?
Explanation
Question 59
A 30-year-old male sustains a high-energy multiligamentous knee dislocation involving the ACL, PCL, and posterolateral corner (PLC). He presents with a complete foot drop. Which nerve is most likely injured, and what is the typical mechanism?
Explanation
Question 60
During physical examination of a patient with a suspected multiligament knee injury, the Dial test demonstrates 15 degrees of increased external rotation compared to the contralateral side at 30 degrees of knee flexion. However, there is no difference at 90 degrees of flexion. What is the diagnosis?
Explanation
Question 61
A patient presents with anterior knee pain and a sudden loss of terminal extension 4 months following an ACL reconstruction.
MRI reveals a localized soft-tissue nodule situated immediately anterior to the ACL graft in the notch. What is the most appropriate management?
Explanation
Question 62
In anatomic reconstruction of the medial patellofemoral ligament (MPFL), precise placement of the femoral attachment is critical to avoid anisometry. Radiographically (Schöttle's point), where is this isometric point located?
Explanation
Question 63
A 45-year-old male presents with chronic medial knee pain and varus malalignment. Radiographs confirm isolated medial compartment osteoarthritis. He is scheduled for a high tibial osteotomy (HTO). Which of the following conditions represents a relative contraindication to an opening wedge HTO?
Explanation
Question 64
Which specific meniscal injury pattern leads to a loss of hoop stresses that makes the joint biomechanically equivalent to a complete meniscectomy?
Explanation
Question 65
During an all-inside meniscal repair of the posterior horn of the lateral meniscus, the surgeon must exercise extreme caution to avoid injuring a major neurovascular structure located immediately posterior to the joint capsule. Which structure is most at risk?
Explanation
Question 66
A 21-year-old athlete sustains an acute knee dislocation. Following rapid closed reduction in the emergency department, the foot is warm with palpable pulses, but the Ankle-Brachial Index (ABI) is calculated to be 0.8. What is the next most appropriate step?
Explanation
Question 67
What is the primary vascular supply to the anterior cruciate ligament (ACL)?
Explanation
Question 68
A 26-year-old male presents with persistent knee stiffness six months after an anterior cruciate ligament (ACL) reconstruction. Radiographs reveal that the femoral tunnel was placed significantly anterior to the anatomic footprint. Which of the following clinical findings is most likely expected due to this malposition?
Explanation
Question 69
A 30-year-old recreational athlete sustains an acute ACL tear. Magnetic resonance imaging also demonstrates a complete radial tear of the posterior root of the medial meniscus. If left untreated, this meniscal injury leads to which of the following biomechanical alterations?
Explanation
Question 70
A 22-year-old female soccer player undergoes revision ACL reconstruction using a bone-patellar tendon-bone allograft. Which of the following allograft preparation methods is most strongly associated with an increased rate of structural graft failure?
Explanation
Question 71
A 25-year-old skier sustains a twisting injury to his left knee. He reports hearing a 'pop' and experiencing immediate swelling. A radiograph of the knee is obtained.
What is the most likely associated ligamentous injury?
Explanation
Question 72
A 34-year-old man presents with chronic knee instability. On physical examination, the dial test is performed in the prone position. He demonstrates 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is symmetric bilaterally. What is the most likely diagnosis?
Explanation
Question 73
A 19-year-old gymnast experiences a first-time lateral patellar dislocation. An MRI confirms a full-thickness tear of the medial patellofemoral ligament (MPFL). When considering anatomical reconstruction, where is the femoral origin of the MPFL located?
Explanation
Question 74
An 11-year-old male (Tanner stage 1) sustains a midsubstance ACL rupture while playing football. He has significant subjective instability with activities of daily living. Which of the following is the most appropriate surgical management?
Explanation
Question 75
A 28-year-old male is brought to the trauma bay after a motorcycle accident with an anterior knee dislocation (Schenck KD-III). The joint is urgently reduced. Post-reduction, he has palpable dorsalis pedis and posterior tibial pulses. His ankle-brachial index (ABI) is measured at 1.1. What is the most appropriate next step in vascular management?
Explanation
Question 76
A surgeon is performing an isolated single-bundle posterior cruciate ligament (PCL) reconstruction to address chronic posterior knee instability. Which functional bundle is being reconstructed, and in what position of knee flexion is this native bundle under the most tension?
Explanation
Question 77
A 21-year-old collegiate basketball player is undergoing primary ACL reconstruction. The surgeon is deciding between a bone-patellar tendon-bone (BTB) autograft and a quadrupled hamstring autograft. Which of the following post-operative complications is significantly more common with a BTB autograft compared to a hamstring autograft?
Explanation
None
