ABOS Part I & OITE Orthopaedic Review: Fibrous Dysplasia, Charcot, Rotator Cuff Tears & Shoulder Arthroplasty | Part 21549
Key Takeaway
These comprehensive orthopaedic board review questions for ABOS Part I and AAOS OITE cover high-yield topics including Fibrous Dysplasia diagnosis and management, Charcot Neuroarthropathy principles and surgical reconstruction, and Rotator Cuff Tear classification, repair techniques, and shoulder arthroplasty. They are designed to mirror exam formats, enhancing your preparation.
ABOS Part I & OITE Orthopaedic Review: Fibrous Dysplasia, Charcot, Rotator Cuff Tears & Shoulder Arthroplasty | Part 21549
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
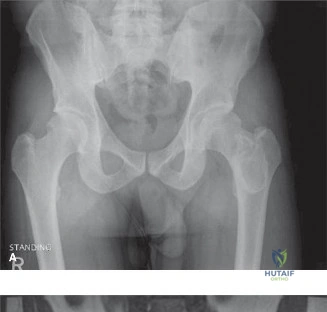
A 25-year-old otherwise healthy male presents to the emergency department with acute onset of severe pain and inability to bear weight in his left thigh following a ground-level fall. He reports a 6-month history of a vague, dull ache in the same area. Initial radiographs of the left femur are shown below.
Based on the clinical presentation and radiographic findings, what is the most likely diagnosis?
Explanation
Correct Answer: C
The clinical presentation of a young adult with a low-energy pathological fracture and a history of prodromal pain, combined with the classic radiographic appearance, strongly points to Fibrous Dysplasia. The initial radiographs (as shown) reveal a displaced, comminuted, transverse fracture of the mid-diaphyseal femur associated with a large, expansile, lytic lesion. Critically, the lesion exhibits the characteristic 'ground-glass' matrix appearance, significant cortical thinning, and endosteal scalloping. This 'ground-glass' appearance is pathognomonic for fibrous dysplasia, reflecting the immature woven bone and fibrous stroma within the lesion. While other lesions can cause pathological fractures, none typically present with this specific radiographic matrix. Osteosarcoma would typically show more aggressive features like periosteal reaction (e.g., sunburst, Codman's triangle), cortical destruction, and osteoid matrix. Enchondroma is usually a benign cartilaginous tumor, often asymptomatic, and would show chondroid matrix calcifications (rings and arcs) rather than ground-glass. Aneurysmal Bone Cyst (ABC) is purely lytic and expansile, often with fluid-fluid levels on MRI, but lacks a specific matrix on plain films. Metastatic carcinoma is less common in a 25-year-old without a known primary and would typically present as a purely lytic or blastic lesion without the ground-glass matrix.
Question 2
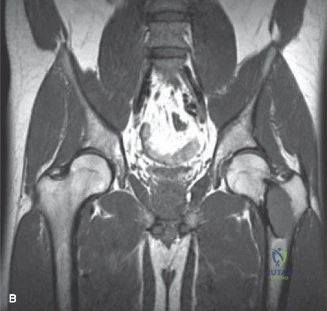
Following initial radiographs, an MRI of the left femur was performed to further characterize the lesion and rule out secondary aneurysmal bone cyst (ABC) or malignant transformation. The MRI findings included heterogeneous low-to-intermediate signal on T1-weighted images, high signal intensity on T2-weighted images, and heterogeneous, predominantly peripheral enhancement post-contrast. Crucially, no definitive fluid-fluid levels were identified. An example MRI image is provided.
Which of the following MRI findings, if present, would have most strongly suggested an alternative diagnosis of an Aneurysmal Bone Cyst (ABC) rather than Fibrous Dysplasia?
Explanation
Correct Answer: C
Aneurysmal Bone Cysts (ABCs) are characterized by blood-filled spaces separated by fibrous septa. On MRI, the classic and most diagnostic feature of an ABC is the presence of prominent fluid-fluid levels, which represent the sedimentation of blood products within these cystic spaces. While fibrous dysplasia can sometimes have cystic degeneration or hemorrhage, leading to areas of high T2 signal and heterogeneous enhancement, it typically lacks definitive fluid-fluid levels unless a secondary ABC has developed within the fibrous dysplastic lesion. The other options (heterogeneous T1 signal, high T2 signal, and heterogeneous enhancement) are non-specific and can be seen in both fibrous dysplasia and ABCs, as well as other bone lesions. The absence of aggressive soft tissue invasion is a feature that helps rule out high-grade malignancy but does not differentiate between fibrous dysplasia and ABC.
Question 3
A 25-year-old male presents with a displaced pathological fracture of the mid-diaphyseal femur through an expansile lytic lesion. The lesion involves more than two-thirds of the cortical diameter, and the patient reported moderate chronic pain prior to the acute fracture. Urgent operative intervention is planned. Applying the Mirels' scoring system to this patient's presentation, which of the following scores and corresponding management recommendations is most appropriate?
Explanation
Correct Answer: C
The Mirels' scoring system is used to assess the risk of impending pathological fracture and guide management. The score is calculated based on four parameters:
- Location: Femur (3 points)
- Pain: Moderate (2 points, for chronic pain leading up to acute fracture)
- Lesion Size: >2/3 cortical diameter (3 points, as the lesion was expansive and involved most of the diaphyseal circumference)
- Nature of Lesion: Lytic (2 points)
Therefore, the total Mirels' score for this patient is 3 + 2 + 3 + 2 = 10 points. A Mirels' score of 9 or greater indicates a very high risk of pathological fracture (or, as in this case, an already present fracture) and mandates urgent operative stabilization. Scores of 7-8 typically recommend prophylactic fixation, while scores of <7 may allow for non-operative management or observation, depending on the specific clinical context. Given the existing displaced fracture, urgent stabilization is unequivocally required.
Question 4
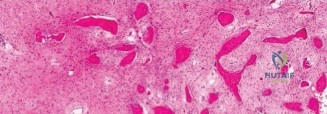
During surgical intervention for the pathological femur fracture, an incisional biopsy was performed by meticulous curettage of the dysplastic tissue. The tissue samples were sent for histopathological examination. Which of the following histopathological findings would definitively confirm the diagnosis of fibrous dysplasia in this patient?
Explanation
Correct Answer: C
The definitive histopathological hallmark of fibrous dysplasia is the presence of irregularly shaped trabeculae of immature woven bone, often described as having a 'Chinese characters' pattern, embedded within a loose, vascular fibrous stroma. Crucially, these woven bone trabeculae lack osteoblastic rimming, which differentiates them from normal or reactive bone formation. Option A describes features of a cartilaginous tumor, such as a chondrosarcoma. Option B describes the characteristic features of an aneurysmal bone cyst (ABC). Option D could describe Ewing sarcoma or lymphoma. Option E describes features often seen in pleomorphic sarcomas or malignant fibrous histiocytoma (now undifferentiated pleomorphic sarcoma). Therefore, option C is the specific and definitive histopathological finding for fibrous dysplasia.
Question 5
Following thorough intralesional curettage of the dysplastic tissue and provisional fracture reduction, the surgeon proceeded to augment the large intramedullary defect and cortical windows. An intraoperative fluoroscopic image after augmentation and intramedullary nail insertion is provided.
What combination of materials was primarily utilized to augment the intramedullary defect and provide structural support in this case, and what is a key benefit of one of these materials?
Explanation
Correct Answer: B
As detailed in the surgical technique, a combination of allograft bone chips and Polymethyl Methacrylate (PMMA) bone cement was utilized to augment the defect. The allograft chips were packed into recesses, and PMMA bone cement was injected. A key benefit of PMMA is that it provides immediate mechanical stability, acting as an internal cast. Its exothermic polymerization reaction is also thought to induce local necrosis in any residual dysplastic cells, potentially reducing recurrence rates. While autograft and DBM (Option A), calcium phosphate cement and BMP (Option C), hydroxyapatite and autograft (Option D), or collagen matrix and PRP (Option E) are all bone graft or augmentation options, they were not the primary materials used in this specific case for immediate structural support in a pathological fracture through fibrous dysplasia, where PMMA's immediate load-bearing capacity is highly advantageous.
Question 6
Post-operatively, the patient was started on a structured, progressive rehabilitation program tailored to the underlying bone pathology and surgical fixation. Given the inherent weakness of the dysplastic bone and the healing fracture, careful consideration was given to weight-bearing progression. What was the initial weight-bearing status permitted for the operative leg in the immediate post-operative period?
Explanation
Correct Answer: C
The case explicitly states that in the immediate post-operative period (Day 0-3), 'Touch-down weight-bearing (TDWB) of 10-15 kg was permitted on the operative leg using crutches or a walker.' Strict adherence to protected weight-bearing was emphasized due to the inherent weakness of the dysplastic bone and the healing fracture. While the intramedullary nail and PMMA provide significant stability, the compromised bone quality and the need for fracture healing necessitate a cautious approach to weight-bearing initially. Full weight-bearing would be too aggressive, and non-weight-bearing might delay rehabilitation unnecessarily given the robust fixation. Partial weight-bearing would typically be a later progression, usually around 4-6 weeks post-operatively.
Question 7
A 45-year-old female presents with a similar expansile lytic lesion in her proximal femur, but her CT scan (similar to the example provided) shows focal cortical breakthrough, significant endosteal erosion exceeding 2/3 of cortical thickness, and characteristic 'rings and arcs' calcification within the lesion. Her biopsy reveals lobules of hyaline cartilage with increased cellularity and nuclear atypia.
Based on these described CT and histopathological findings, which alternative diagnosis should be most strongly considered, and what is its key differentiating feature from fibrous dysplasia?

Explanation
Correct Answer: C
The described CT findings of 'focal cortical breakthrough, significant endosteal erosion exceeding 2/3 of cortical thickness, and characteristic 'rings and arcs' calcification within the lesion' are highly suggestive of a cartilaginous tumor. The 'rings and arcs' pattern is classic for chondroid matrix calcification. When combined with histopathology showing 'lobules of hyaline cartilage with increased cellularity and nuclear atypia,' this definitively points to a Low-Grade Chondrosarcoma (LGCS), also known as an Atypical Cartilaginous Tumor (ACT). Fibrous dysplasia, in contrast, typically shows a 'ground-glass' matrix and woven bone on histology, not chondroid calcification or atypical cartilage. While ABCs have fluid-fluid levels, GCTs are epiphyseal, brown tumors have metabolic derangements, and non-ossifying fibromas have a sclerotic rim, none of these fit the described imaging and pathological features as well as LGCS.
Question 8
A 25-year-old patient with monostotic fibrous dysplasia of the femur undergoes intralesional curettage and intramedullary nailing for a pathological fracture. Two years later, he presents with new onset pain and radiographic evidence of lesion expansion at the previous surgical site. A repeat biopsy confirms recurrent fibrous dysplasia. Which of the following is the most likely reason for this patient's recurrence?
Explanation
Correct Answer: B
One of the key pitfalls in the management of fibrous dysplasia, as highlighted in the case, is incomplete curettage. Fibrous dysplasia lesions, especially aggressive or expansile ones, have a high local recurrence rate if the dysplastic tissue is not thoroughly removed. Simple curettage without aggressive burring or augmentation (e.g., with PMMA) often leaves residual dysplastic cells, leading to recurrence. While malignant transformation (Option A) is a rare but serious complication, it would typically present with more aggressive radiographic changes and a different histopathology (e.g., osteosarcoma). Failure to use an intramedullary nail (Option C) would primarily lead to fixation failure or non-union, not necessarily recurrence of the lesion itself. Development of a secondary ABC (Option D) is possible but less likely to be the primary cause of recurrence if the underlying FD was not adequately addressed. Progression to polyostotic disease (Option E) is a different phenomenon, implying new lesions elsewhere, not recurrence at the original monostotic site.
Question 9
Following successful surgical stabilization and rehabilitation, the patient is discharged with a confirmed diagnosis of monostotic fibrous dysplasia. Given the nature of this condition, what is the most appropriate long-term surveillance strategy for this patient?
Explanation
Correct Answer: B
The case emphasizes that patients with fibrous dysplasia require long-term surveillance due to the potential for disease progression, local recurrence, or, albeit rare (0.4-4%), malignant transformation (most commonly to osteosarcoma). Therefore, annual clinical and radiographic review for several years is advisable. Further imaging (e.g., CT or MRI) should be obtained if any new symptoms (pain, swelling, deformity) or suspicious findings on routine radiographs emerge. Option A is incorrect as surveillance is necessary. Option C (bi-annual MRI for 5 years) is overly aggressive and not standard for routine surveillance of a stable, treated monostotic lesion unless specific concerns arise. Option D (routine blood tests) is generally not indicated unless there are signs of metabolic derangement or suspicion of polyostotic disease with endocrine involvement. Option E (prophylactic radiation therapy) is contraindicated due to the known risk of inducing malignant transformation in fibrous dysplasia.
Question 10
The patient's initial systemic examination and laboratory investigations were unremarkable. Specifically, there was no café-au-lait pigmentation, and serum calcium, phosphate, and alkaline phosphatase levels were within normal ranges. The absence of these findings in this patient helps to rule out which of the following associated syndromes or conditions?
Explanation
Correct Answer: C
McCune-Albright syndrome is a classic triad characterized by polyostotic fibrous dysplasia, café-au-lait skin pigmentation, and various endocrine dysfunctions (e.g., precocious puberty, hyperthyroidism, acromegaly, Cushing's syndrome). The absence of café-au-lait spots and normal endocrine labs (implied by normal calcium, phosphate, and ALP, and specifically mentioned normal PTH in the case) effectively rules out McCune-Albright syndrome in this patient, confirming his monostotic presentation without systemic involvement. Neurofibromatosis Type 1 (Option A) is associated with café-au-lait spots but typically presents with neurofibromas and other skeletal dysplasias, not fibrous dysplasia as its primary bone lesion. Ollier's disease (Option B) and Maffucci syndrome (Option D) are characterized by multiple enchondromas, not fibrous dysplasia. Paget's disease of bone (Option E) is a metabolic bone disease of older adults, characterized by disorganized bone remodeling and typically elevated alkaline phosphatase, which was normal in this patient.
Question 11
A 58-year-old male with a 20-year history of poorly controlled type 2 diabetes mellitus presents to the emergency department with a 3-week history of progressive swelling, erythema, and warmth of his right foot. He denies any specific trauma but reports a dull ache. On examination, his foot appears as shown in the image. He has absent vibratory sensation and diminished protective sensation. His white blood cell count is normal, and ESR/CRP are mildly elevated. The elevation test shows persistent erythema after 10 minutes.

Explanation
Correct Answer: C
The clinical presentation of warmth, erythema, and edema is common to both acute Charcot neuroarthropathy (Eichenholtz Stage 0/I) and osteomyelitis. The elevation test, which shows persistent erythema after 10 minutes, is a useful clinical adjunct that suggests an infectious process rather than acute Charcot, where erythema typically resolves with elevation. Given the suspicion for osteomyelitis, advanced imaging is required for definitive differentiation. Magnetic Resonance Imaging (MRI) with and without contrast is considered the gold standard. Charcot typically demonstrates primary joint-based marrow edema, while osteomyelitis shows contiguous bone marrow edema adjacent to a soft tissue ulceration or sinus tract. Surgical debridement and antibiotics (Options A and B) would be premature without a definitive diagnosis. Waiting for plain radiographic changes (Option D) would delay diagnosis and appropriate treatment, as early Charcot (Stage 0) has normal radiographs and osteomyelitis may not show changes for weeks. Application of a TCC (Option E) is appropriate for acute Charcot but contraindicated if active infection is present, highlighting the critical need for accurate diagnosis.
Question 12
A 62-year-old diabetic patient develops acute Charcot neuroarthropathy. Which of the following molecular pathways is primarily responsible for the aggressive osteolysis seen in the acute phase of this condition?
Explanation
Correct Answer: D
The case explicitly states that modern molecular biology has elucidated the inflammatory cascade driving Charcot neuroarthropathy. The Receptor Activator of Nuclear Factor Kappa-B Ligand (RANKL) and Osteoprotegerin (OPG) pathway plays a central role. Pro-inflammatory cytokines, particularly Interleukin-1 (IL-1) and Tumor Necrosis Factor-alpha (TNF-alpha), upregulate RANKL expression in the setting of acute trauma. In the diabetic, neuropathic patient, this response is exaggerated and uncoupled from normal bone formation, leading to aggressive, unchecked osteoclastic bone resorption. Therefore, exaggerated and uncoupled osteoclastic activity mediated by RANKL is the primary mechanism of osteolysis. Options A, B, C, and E describe processes that are either incorrect or would lead to bone formation/inhibition of resorption, which is contrary to the destructive nature of acute Charcot.
Question 13
A 55-year-old male with long-standing diabetes presents with a progressive foot deformity, now exhibiting a classic rocker bottom appearance as seen in the provided radiograph.

Explanation
Correct Answer: C
The case details the pathomechanics of the rocker bottom deformity, emphasizing that it results from the catastrophic failure of the medial longitudinal arch, heavily driven by biomechanical imbalances. The text specifically highlights an equinus contracture as the most notable factor. Tightness in the gastrocnemius-soleus complex creates a significant plantarflexion force on the calcaneus. During the stance phase of gait, as the tibia advances over the foot, the inability of the ankle to dorsiflex transfers immense bending moments to the midfoot. In the setting of neuropathic osteopenia and ligamentous failure, the midfoot collapses, leading to the characteristic plantar convexity. Options A, B, D, and E do not represent the primary deforming force described for the rocker bottom deformity.
Question 14
A 48-year-old patient with Charcot neuroarthropathy of the midfoot, classified as Eichenholtz Stage III, presents with a chronic plantar ulceration over a prominent talar head that has been recalcitrant to 6 months of aggressive offloading with a CROW boot and wound care. His HbA1c is 7.2%, and his TcPO2 is 55 mmHg. He is compliant with medical management and rehabilitation. Which of the following is the most appropriate next step in management?
Explanation
Correct Answer: C
The patient presents with a severe rocker bottom deformity (implied by prominent talar head) and a chronic plantar ulceration that is recalcitrant to aggressive offloading. The case explicitly lists 'Recurrent plantar ulceration recalcitrant to aggressive offloading and wound care' and 'Chronic osteomyelitis associated with a bony prominence, requiring simultaneous resection and stabilization' as specific indications for operative intervention. The patient is in Eichenholtz Stage III (consolidation), which is generally considered an appropriate stage for surgery when the inflammatory process has subsided. Furthermore, his HbA1c (7.2%) is well-controlled (below the 8.5% contraindication threshold), and his TcPO2 (55 mmHg) indicates adequate vascular inflow for healing (above the 40 mmHg threshold). Given these factors, surgical reconstruction to achieve a plantigrade foot, debride the bony prominence, and stabilize the foot is the most appropriate next step. Continuing conservative management (Option A) has already failed. Initiating antibiotics (Option B) without confirming osteomyelitis or addressing the underlying mechanical issue is insufficient. Amputation (Option D) is a salvage procedure for failed reconstruction or uncontrolled infection, not a primary step here. Achilles tendon lengthening (Option E) is a component of surgical reconstruction but not a standalone solution for a chronic ulcer over a bony prominence.
Question 15
A 60-year-old diabetic patient is being evaluated for surgical reconstruction of a Charcot foot deformity. During preoperative vascular assessment, which of the following findings would be most predictive of successful wound healing post-surgery?
Explanation
Correct Answer: D
The case emphasizes the paramount importance of vascular assessment. It states: 'Non-invasive vascular studies, including Ankle-Brachial Indices (ABIs) and Toe-Brachial Indices (TBIs), should be obtained. In diabetic patients with calcified vessels, ABIs may be falsely elevated; therefore, transcutaneous oxygen measurements (TcPO2) or arterial duplex ultrasonography are often required. A TcPO2 greater than 40 mmHg is generally predictive of successful wound healing.' An ABI of 1.2 (Option A) could be falsely elevated in a diabetic patient due to vessel calcification. A palpable pulse (Option B) does not rule out microvascular disease. A TBI of 0.4 (Option C) is generally considered poor vascularity. Absence of claudication (Option E) is a symptom assessment, not a direct measure of healing potential.
Question 16
During surgical reconstruction of a severe rocker bottom Charcot foot, the surgeon identifies a significant equinus contracture. According to the case description, which of the following is the most critical initial soft tissue procedure to ensure successful deformity correction and prevent hardware failure?
Explanation
Correct Answer: C
The case explicitly states under 'Soft Tissue Balancing and Equinus Correction' that 'Deformity correction must begin with soft tissue balancing, primarily addressing the Achilles tendon. An equinus contracture is universally present and acts as a major deforming force. Attempting to correct a midfoot collapse without lengthening the Achilles tendon will result in excessive tension on the midfoot reconstruction and inevitable hardware failure.' A percutaneous Tendo-Achilles Lengthening (TAL) or an open gastrocnemius recession (Strayer or Baumann procedure) is performed to achieve adequate lengthening, allowing the ankle to dorsiflex to at least 10 degrees beyond neutral. The other options are not described as the most critical initial soft tissue procedure for preventing hardware failure in the context of an equinus contracture in Charcot reconstruction.
Question 17
A 52-year-old patient undergoes surgical reconstruction for a severe Charcot midfoot deformity, as depicted in the post-operative radiograph.

Explanation
Correct Answer: D
The case highlights that 'Standard osteosynthesis techniques frequently fail in Charcot neuroarthropathy due to the profound osteopenia and impaired healing capacity. Consequently, the concept of 'superconstructs,' pioneered by Sammarco, has become the standard of care.' The four primary principles of superconstructs are listed as: 1) Fusion must extend beyond the zone of injury to include normal, healthy bone. 2) Bone resection must be adequate to allow for deformity correction without placing undue tension on the soft tissue envelope. 3) The strongest fixation devices possible must be utilized. 4) Hardware should be applied in a position that maximizes its biomechanical advantage. Therefore, the statement that standard osteosynthesis techniques are preferred is incorrect and directly contradicts the principles of superconstructs.
Question 18
A 65-year-old patient undergoes successful surgical reconstruction of a Charcot midfoot deformity. Six months post-operatively, radiographs show evidence of hardware breakage and a nonunion at the arthrodesis site, but the foot remains plantigrade and the patient is asymptomatic, able to ambulate with a CROW boot without pain or ulceration. What is the most appropriate management strategy?
Explanation
Correct Answer: C
The case discusses complications and management, specifically addressing hardware failure and nonunion. It states: 'Management depends on the clinical presentation. Asymptomatic nonunions with stable hardware and a plantigrade, braceable foot can often be observed.' In this scenario, despite hardware breakage and nonunion, the patient is asymptomatic, the foot is plantigrade, and they are ambulating with a CROW boot without pain or ulceration. This indicates a functionally stable outcome despite radiographic findings. Therefore, continued observation with bracing and close monitoring is the most appropriate management. Revision surgery (Option A) is typically reserved for symptomatic nonunions or those leading to instability or impending skin breakdown. Amputation (Option B) is a last resort for failed salvage. Antibiotics (Option D) are not indicated without signs of infection. External fixation (Option E) would be an option for revision surgery if the foot were unstable or symptomatic, but not for an asymptomatic, stable nonunion.
Question 19
Following a complex Charcot midfoot reconstruction, a patient is placed in a well-padded Jones splint. According to the standard rehabilitation protocols described, what is the typical duration of strict non-weight-bearing (NWB) status before transitioning to a weight-bearing cast or CROW boot, assuming uncomplicated healing?
Explanation
Correct Answer: D
The case details the postoperative rehabilitation protocols, emphasizing the prolonged healing time for neuropathic bone. Under 'Immediate Post Operative Phase,' it states: 'The duration of NWB is highly variable but typically ranges from 12 to 16 weeks, and in complex reconstructions, may extend up to 6 months.' While the patient is transitioned to a fiberglass Total Contact Cast (TCC) or a rigid bivalved cast at two to three weeks postoperatively, this is still within the non-weight-bearing phase. The transition to a weight-bearing cast or CROW boot only occurs once clinical and radiographic evidence of consolidation is confirmed, which typically takes 12-16 weeks of NWB.
Question 20
A 50-year-old patient presents with Charcot neuroarthropathy primarily affecting the subtalar, talonavicular, and calcaneocuboid joints. According to the Brodsky classification system, what type of Charcot involvement does this patient exhibit?
Explanation
Correct Answer: B
The case provides a clear description of the Brodsky classification system for anatomical patterns of Charcot neuroarthropathy. It states: 'The Brodsky classification categorizes these anatomical patterns: Type 1 involves the midtarsal and tarsometatarsal joints; Type 2 involves the subtalar, talonavicular, or calcaneocuboid joints; Type 3A involves the tibiotalar joint; Type 3B involves the calcaneal tuberosity; and Type 4 involves a combination of areas.' Since the patient's primary involvement is in the subtalar, talonavicular, and calcaneocuboid joints, this corresponds to Brodsky Type 2.
Question 21
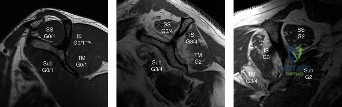
A 70-year-old, right-hand-dominant woman presents with chronic right shoulder pain and weakness, unable to reach overhead. Physical examination reveals significant atrophy of the supraspinatus and infraspinatus, limited active range of motion, and positive drop arm and external rotation lag signs. MRI confirms a massive rotator cuff tear involving the supraspinatus and infraspinatus, with minimal atrophy, minimal fatty infiltration, and retraction to the glenoid. Given these findings, which of the following best describes the initial Goutallier classification of her rotator cuff tear?
Explanation
Correct Answer: C
The patient's MRI shows 'minimal atrophy, minimal fatty infiltration, and retraction to the glenoid' for both the supraspinatus and infraspinatus. According to the Goutallier classification system, which assesses fatty degeneration of the rotator cuff muscles, Stage 0 is normal, Stage 1 is minimal fatty streaks, Stage 2 is a significant amount of fatty streaks but more muscle than fat, Stage 3 is equal amounts of fat and muscle, and Stage 4 is more fat than muscle. The description 'minimal fatty infiltration' aligns most closely with Stage 2, where there are significant fatty streaks but still more muscle than fat. Stage 3 (equal fat and muscle) and Stage 4 (more fat than muscle) would imply more significant fatty infiltration, which is not indicated by 'minimal'. The image (Figure 2-18) visually demonstrates these stages, with Stage 2 showing clear muscle bulk with some interspersed fat, consistent with 'minimal fatty infiltration' compared to the more severe Stage 3 and 4 examples.
Question 22
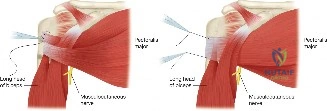
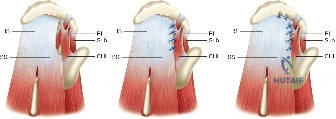
During arthroscopy for a massive, immobile rotator cuff tear, it is confirmed that a small part of the anterior supraspinatus remains attached to the greater tuberosity laterally, and the rotator interval is intact anteriorly. The surgeon plans to mobilize the tear to allow for repair to the greater tuberosity, followed by marginal convergence. Which specific technique is indicated to facilitate the initial mobilization of this tear?

Explanation
Correct Answer: C
The case describes a scenario where a small part of the anterior supraspinatus is still attached to the greater tuberosity laterally and the rotator interval is intact anteriorly. The discussion explicitly states that in an anterior interval slide technique, 'there is some anterior portion of the supraspinatus still attached to the greater tuberosity laterally and rotator interval anteriorly. The greater tuberosity attachment can be incised and the rotator interval attachment can be detached by incising the coracohumeral ligament.' This technique decreases tension and improves lateral mobilization, allowing the supraspinatus to be more easily repaired. The image (Figure 2-16) illustrates this process, showing the incision of the rotator interval and coracohumeral ligament to mobilize the anterior supraspinatus. A posterior interval slide (Option A) is used when the posterior supraspinatus is attached to the infraspinatus. A Krackow stitch (Option B) is a locking stitch for tendinous repairs, not a mobilization technique for rotator cuff tears. Double-bundle reconstruction (Option D) is an ACL reconstruction technique. Subscapularis release (Option E) is not described as a primary mobilization technique for supraspinatus tears in this context.
Question 23
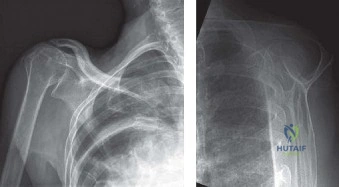
A 75-year-old patient presents with a massive, irreparable rotator cuff tear (Goutallier Stage 3 fatty infiltration of supraspinatus and infraspinatus) and significant glenohumeral arthritis, characterized by superior migration of the humerus, joint destruction, and subchondral osteoporosis. She has failed all conservative management. Which of the following is the most appropriate surgical treatment option?
Explanation
Correct Answer: E
The patient presents with a massive, irreparable rotator cuff tear (Goutallier Stage 3) and significant glenohumeral arthritis, specifically described as cuff-tear arthropathy (superior migration, joint destruction, subchondral osteoporosis). The discussion explicitly states that a reverse total shoulder arthroplasty (RTSA) is the procedure of choice in patients with cuff-tear arthropathy. RTSA eliminates pain from arthritis and restores functional motion by creating an inferior force-couple and a fulcrum, allowing the deltoid to abduct and flex the shoulder without superior migration. The image (Figure 2-17) shows characteristic X-rays of cuff tear arthropathy, which is a key indication for RTSA. Hemiarthroplasty (Option A) reliably relieves pain but does not restore function as well as RTSA. Total shoulder arthroplasty (Option B) is contraindicated in cuff-tear arthropathy due to the risk of glenoid component loosening ('rocking-horse' glenoid). Latissimus dorsi tendon transfer (Option C) is an option for younger, active patients without arthritis. Arthroscopic rotator cuff repair (Option D) is contraindicated given the Goutallier Stage 3 fatty infiltration, which predicts poor outcomes and high failure rates.
Question 24
A 50-year-old, healthy, active patient presents with a massive, irreparable rotator cuff tear involving the supraspinatus and infraspinatus, similar to the initial case, but without any signs of glenohumeral arthritis. He has failed extensive conservative management. Which of the following is the most appropriate surgical treatment option to restore function?
Explanation
Correct Answer: C
For young, active patients (like this 50-year-old) with a massive, irreparable rotator cuff tear involving the supraspinatus and infraspinatus, but without glenohumeral arthritis, a tendon transfer is the most reasonable option to restore function. The discussion specifically highlights the latissimus dorsi tendon transfer as the most popular way to restore the posterior and inferior force-couples and create an external rotation force in such cases. The image (Figure 2-19) illustrates the latissimus dorsi tendon transfer. Arthroscopic rotator cuff repair (Option A) is not indicated for an irreparable tear with significant fatty degeneration. Subscapularis tendon transfer (Option B) would not address the loss of the posterior and inferior force-couple from the torn infraspinatus. Trapezius tendon transfer (Option D) is mentioned as having some interest but is not as popular or well-established for rotator cuff tears as the latissimus dorsi transfer, and often requires allograft. Reverse total shoulder arthroplasty (Option E) is generally reserved for older, less active patients or those with cuff tear arthropathy, as it has limitations in lifting activities and a higher revision risk in younger patients.
Question 25
A patient is diagnosed with a chronic, irreparable tear of the subscapularis tendon after failing conservative treatment. The surgeon plans a tendon transfer to restore internal rotation and humeral head centering. Which of the following tendons is the most reasonable choice for transfer in this scenario?
Explanation
Correct Answer: C
For a chronic, irreparable tear of the subscapularis tendon, the discussion states that using a tendon transfer is the next step. The pectoralis major tendon is highlighted as an effective choice because its force vector is similar to that of the subscapularis, allowing it to restore internal rotation and humeral head centering and compression. The surgery involves detaching the pectoralis major from its humeral insertion and moving it to the lesser tuberosity. The image (Figure 2-20) depicts the pectoralis major tendon transfer. Subscapularis tendon repair (Option A) is impossible by definition if the tear is irreparable. Biceps tenotomy (Option B) might be performed adjunctively but does not restore subscapularis function. Reverse total shoulder arthroplasty (Option D) is typically used for massive, irreparable anterosuperior rotator cuff tears, not isolated subscapularis tears. Supraspinatus tendon transfer (Option E) is not a described procedure for irreparable subscapularis tears.
Question 26
A 68-year-old patient undergoes reverse total shoulder arthroplasty for cuff tear arthropathy. One month post-operatively, the patient develops increasing shoulder pain, warmth, and erythema around the incision site. Initial wound cultures are negative after 48 hours. Based on the typical presentation of delayed shoulder prosthetic infections, what is the most likely causative organism?
Explanation
Correct Answer: C
The patient presents with signs and symptoms of a surgical wound infection one month after reverse total shoulder surgery, and initial cultures are negative. The discussion explicitly states that Propionibacterium acnes (now known as Cutibacterium acnes) is the most common cause of delayed or indolent infections of surgical wounds, and cultures are often negative because it takes a long time (about 14 to 21 days) for it to grow. Staphylococcus aureus (Option A), Streptococcus pyogenes (Option B), and Pseudomonas aeruginosa (Option D) are common causes of acute wound infections, which typically present within a week or two of surgery and are more likely to grow out on standard cultures within 48 hours. Escherichia coli (Option E) is a common cause of urinary tract infections and intra-abdominal infections, but less common for shoulder prosthetic infections, especially with a delayed, culture-negative presentation.
Question 27
A 65-year-old patient with a massive, irreparable rotator cuff tear and significant glenohumeral arthritis is being considered for shoulder arthroplasty. The surgeon explains that a total shoulder arthroplasty (TSA) is contraindicated in this specific condition. What is the primary reason for this contraindication?
Explanation
Correct Answer: D
The discussion clearly states that a total shoulder arthroplasty (TSA) is contraindicated in the case of cuff-tear arthropathy because of glenoid component loosening. It explains that 'if a glenoid component is used in this patient, the superior translation of the humeral head component on the glenoid component could cause it to loosen and rock, producing a 'rocking-horse' glenoid component.' This superior translation is a direct consequence of the massive rotator cuff tear, which leads to an unopposed superior pull of the deltoid. Options A, B, C, and E are not the primary or specific contraindications for TSA in the context of cuff tear arthropathy as described in the text.
Question 28
A 72-year-old patient with a massive, irreparable rotator cuff tear and cuff-tear arthropathy undergoes a reverse total shoulder arthroplasty. Which of the following best describes the biomechanical principle by which this prosthesis restores function?
Explanation
Correct Answer: D
The discussion explains that a reverse total shoulder arthroplasty (RTSA) is a semi-constrained prosthesis that restores function in patients with massive rotator cuff tears by 'constraining a concave humeral cap inferior to a semispherical glenoid component (glenosphere). This creates an inferior force-couple and a fulcrum that replaces the stabilizing function of the infraspinatus maintaining a center of rotation around which the shoulder can move. This allows the deltoid to abduct and flex the shoulder without causing the humerus to migrate superiorly and about the acromion.' This detailed explanation directly supports Option D. Option A is incorrect as RTSA is for irreparable tears. Option B is incorrect as the remaining rotator cuff is insufficient. Option C is incorrect as the deltoid's primary function is abduction, and RTSA enhances this. Option E describes part of the design (semispherical glenoid) but not the full biomechanical principle of how it restores function in the absence of a functional rotator cuff.
Question 29
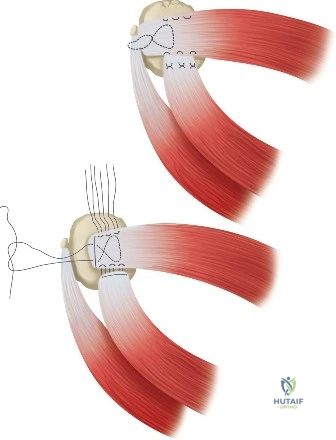
A 60-year-old patient presents with a chronic, U-shaped rotator cuff tear that is retracted to the glenoid. The surgeon determines that the apex of the tear cannot be mobilized to the greater tuberosity. Which repair technique is most appropriate to convert this tear into a reparable configuration?
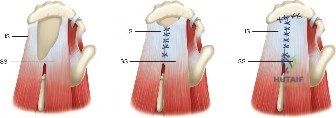
Explanation
Correct Answer: D
The case discussion specifically addresses U-shaped tears, stating that 'U-shaped tears have an apex that extends further medially... and this part cannot be mobilized all the way to the greater tuberosity. Because of this lack of mobility, these tears have to be repaired using marginal convergence, which is essentially zipping up the U from the apex toward the greater tuberosity using side to side sutures to bring together the anterior and posterior leaves of the U-shaped tear. In performing this marginal convergence, you essentially are converting a U-shaped tear into a crescent-shaped tear that can be relatively easily mobilized to the greater tuberosity, allowing it to be repaired.' The image (Figure 2-14) clearly illustrates this process. Anterior (Option A) and posterior (Option B) interval slides are used for massive, immobile tears with specific attachments, not primarily for U-shaped tears that are retracted to the glenoid apex. Crescent repair (Option C) is the final repair type after conversion, not the conversion technique itself. Double-row repair (Option E) is a method of fixation to bone, not a technique to mobilize or convert tear shape.
Question 30
A 55-year-old patient is found to have an L-shaped rotator cuff tear during arthroscopy. The surgeon notes that one leg of the L is a mobile, less retracted crescent-shaped tear, while the other leg is a less mobile, more retracted U-shaped tear. To achieve a successful repair, what is the initial and most critical step for addressing the retracted portion of this L-shaped tear?
Explanation
Correct Answer: C
The discussion describes L-shaped tears as having both a mobile, less retracted crescent-shaped part and a less mobile, more retracted U-shaped part. It explicitly states: 'The retracted U-shaped part, like a normal U-shaped tear, must be repaired using marginal convergence. Then the remaining crescent-shaped part, like a normal crescent-shaped tear, can be mobilized laterally and repaired to bone.' Therefore, the initial and most critical step for addressing the retracted U-shaped portion is marginal convergence. The image (Figure 2-15) illustrates the application of marginal convergence to an L-shaped tear. Direct repair of the crescent-shaped portion (Option A) would be done after the U-shaped portion is addressed. Anterior interval slide (Option B) is for specific massive, immobile tears, not the primary technique for L-shaped tears. A Krackow stitch (Option D) is a type of suture, not a tear-conversion technique. Reverse total shoulder arthroplasty (Option E) is a salvage procedure for irreparable tears, not a repair technique for an L-shaped tear that can be converted.
Question 31
A 14-year-old female presents with multiple bony deformities, unilateral café-au-lait spots with irregular borders, and a history of precocious puberty. A biopsy of a femoral lesion demonstrates woven bone trabeculae in a fibrous stroma without osteoblastic rimming. The pathogenesis of her condition is most directly linked to a mutation affecting which of the following?
Explanation
Question 32
A 45-year-old female with known polyostotic fibrous dysplasia presents with a painless, slow-growing soft tissue mass in her right thigh. Magnetic resonance imaging reveals a well-circumscribed, lobulated intramuscular mass that is T1-hypointense and markedly T2-hyperintense with mild peripheral enhancement. What is the most likely diagnosis associated with this syndrome?
Explanation
Question 33
A 16-year-old male with fibrous dysplasia presents with increasing thigh pain and a progressive varus deformity of the proximal femur, characteristic of a 'Shepherd's crook' deformity. Non-operative management has failed. Which of the following is the most appropriate surgical management?
Explanation
Question 34
Which of the following histological features is considered the classic hallmark of fibrous dysplasia?
Explanation
Question 35
A 55-year-old male with a long-standing history of diabetes mellitus presents with a red, hot, swollen right foot. He denies trauma, fever, or chills. He has palpable pedal pulses and a severe peripheral neuropathy. Radiographs show soft tissue swelling, periarticular debris, and early fragmentation at the tarsometatarsal joints. According to the Eichenholtz classification, what is the most appropriate initial management?
Explanation
Question 36
In the pathogenesis of Charcot neuroarthropathy, the neurovascular theory proposes that autonomic neuropathy directly leads to which of the following physiological changes?
Explanation
Question 37
Differentiating between acute Charcot arthropathy and pedal osteomyelitis in a diabetic patient can be challenging. Which of the following advanced imaging modalities provides the highest specificity for distinguishing osteomyelitis from active Charcot neuroarthropathy?
Explanation
Question 38
According to the Brodsky classification of Charcot joints, which anatomical location represents a Type 1 deformity, being the most common site of involvement?
Explanation
Question 39
A 68-year-old male presents with chronic shoulder pain and weakness. MRI demonstrates a massive, retracted tear of the supraspinatus and infraspinatus tendons. The T1-weighted sagittal oblique images show that there is more fat than muscle tissue within the infraspinatus muscle belly. What Goutallier stage does this represent?
Explanation
Question 40
During dynamic stabilization of the glenohumeral joint, the transverse force couple is essential for maintaining the humeral head centered on the glenoid. Which muscle groups primarily constitute this anterior-posterior transverse force couple?
Explanation
Question 41
A 45-year-old heavy laborer presents with a massive, irreparable posterosuperior rotator cuff tear. He has persistent pain and lack of active external rotation, but his subscapularis is fully intact and he lacks glenohumeral arthritis. Which of the following tendon transfers is most appropriate to restore external rotation and function in this patient?
Explanation
Question 42
In the context of massive, irreparable rotator cuff tears, Superior Capsular Reconstruction (SCR) has emerged as a joint-preserving surgical option. What is the primary biomechanical goal of SCR?
Explanation
Question 43
A 62-year-old female undergoes reverse total shoulder arthroplasty (RSA) for rotator cuff arthropathy. In the original Grammont design, what is the primary biomechanical advantage conferred by the placement and design of the glenosphere?
Explanation
Question 44
A complication unique to reverse total shoulder arthroplasty (RSA) is scapular notching. According to the Sirveaux classification, which of the following intraoperative techniques is most effective in preventing inferior scapular notching?
Explanation
Question 45
A 65-year-old male with primary glenohumeral osteoarthritis is indicated for an anatomic total shoulder arthroplasty. Preoperative CT scan reveals a Walch B2 glenoid morphology. What defines a Walch B2 glenoid?
Explanation
Question 46
Six months after a reverse total shoulder arthroplasty, a 70-year-old female presents with sudden onset lateral shoulder pain and decreased active elevation after lifting a moderately heavy box. Radiographs reveal a stress fracture at the base of the acromion (Levy Type II). What is the primary underlying biomechanical cause of this specific complication?
Explanation
Question 47
A 72-year-old patient with severe glenohumeral osteoarthritis and a massive, retracted rotator cuff tear presents with active forward elevation of 40 degrees and a 'shrug' sign. They have no pain relief after conservative management. In determining the appropriate arthroplasty option, why is an anatomic total shoulder arthroplasty (TSA) contraindicated in this patient?
Explanation
Question 48
In the biological microenvironment of chronic, retracted rotator cuff tears, which specific enzymes are known to be significantly upregulated, leading to collagen degradation and impairment of tendon-to-bone healing post-repair?
Explanation
Question 49
A 50-year-old diabetic male undergoes surgical management for a chronic, draining ulcer over a severe midfoot Charcot deformity. During the procedure, deep bone margins are taken. What histological finding is most indicative of superimposed osteomyelitis rather than the underlying Charcot osteoarthropathy alone?
Explanation
Question 50
When evaluating a patient for a shoulder arthroplasty, assessing the status of the axillary nerve is critical. If a patient requires a reverse shoulder arthroplasty but is found to have profound, irreversible axillary nerve palsy with a completely atrophic deltoid, what is the most appropriate management?
Explanation
Question 51
A 12-year-old girl presents with precocious puberty, cafe-au-lait spots with irregular borders, and a newly discovered lytic lesion in her proximal femur resulting in a 'shepherd's crook' deformity. What is the underlying genetic and pathophysiologic mechanism of this patient's skeletal disease?
Explanation
Question 52
A 55-year-old diabetic male presents with an acutely swollen, red, and warm right foot. He denies trauma. Radiographs reveal periarticular debris, subluxation of the tarsometatarsal joints, and fracture fragmentation. What is the most appropriate initial management?
Explanation
Question 53
In a patient undergoing reverse total shoulder arthroplasty (rTSA) for cuff tear arthropathy, how does the prosthesis alter the biomechanics of the shoulder to restore active elevation?
Explanation
Question 54
A 60-year-old male is evaluated for a massive, retracted rotator cuff tear. An MRI reveals Goutallier Stage 4 fatty infiltration of the infraspinatus. How is Goutallier Stage 4 defined on imaging?
Explanation
Question 55
A 45-year-old female with known polyostotic fibrous dysplasia presents with multiple painless soft tissue masses in her right thigh. Biopsy of one of the masses reveals an intramuscular myxoma. Which of the following syndromes does this patient possess?
Explanation
Question 56
A 40-year-old male with a history of cervical syringomyelia presents with massive swelling, crepitus, and instability of his right shoulder without significant pain. Radiographs demonstrate severe destruction of the humeral head and glenoid with multiple loose bodies. What is the most likely diagnosis?
Explanation
Question 57
A 65-year-old female is undergoing anatomic total shoulder arthroplasty (TSA) for primary osteoarthritis. Preoperative CT planning demonstrates a B2 glenoid. What defines a Walch B2 glenoid deformity?
Explanation
Question 58
During arthroscopic evaluation of a massive rotator cuff tear, the surgeon identifies the 'comma sign'. This anatomical landmark is formed by the avulsion and retraction of which structures?
Explanation
Question 59
A 30-year-old male with fibrous dysplasia of the proximal femur requires surgical stabilization due to progressive pain and impending fracture. Which of the following surgical techniques is most appropriate to maximize long-term construct survival?
Explanation
Question 60
When differentiating between acute Charcot neuroarthropathy of the foot and pedal osteomyelitis, which diagnostic study offers the highest sensitivity and specificity?
Explanation
Question 61
A 45-year-old overhead athlete presents with persistent shoulder pain. MRI reveals a Partial Articular-Sided Tendon Avulsion (PASTA) of the supraspinatus. At what depth of footprint involvement is surgical completion and repair generally indicated?
Explanation
Question 62
Scapular notching is a recognized complication of reverse total shoulder arthroplasty (rTSA). Which technical modification of the glenosphere most effectively reduces the incidence of this complication?
Explanation
Question 63
A 22-year-old male with a symptomatic benign lytic lesion of the diaphyseal humerus undergoes an incisional biopsy. Histology shows irregular trabeculae of woven bone arranged in 'Chinese letter' patterns within a moderately cellular fibrous stroma, completely lacking osteoblastic rimming. What is the diagnosis?
Explanation
Question 64
A 58-year-old diabetic female has been in a total contact cast for 4 months for a Stage I Charcot midfoot deformity. She now presents for follow-up. Clinical exam shows complete resolution of erythema and edema. Radiographs show sclerosis, rounding of bone ends, and solid fusion of major fragments. What is her current Eichenholtz stage?
Explanation
Question 65
A 60-year-old male presents with pseudo-paralysis of his right shoulder and a massive, irreparable posterosuperior rotator cuff tear. Glenohumeral cartilage is intact. He undergoes a superior capsular reconstruction (SCR). Which of the following is an absolute contraindication for an SCR?
Explanation
Question 66
A 68-year-old male is 6 weeks status-post anatomic total shoulder arthroplasty via a deltopectoral approach. He complains of sudden anterior shoulder pain and weakness after reaching out for a door. Exam shows a positive belly-press test and increased passive external rotation compared to his immediate postoperative records. What is the most likely complication?
Explanation
Question 67
A 48-year-old male presents with shoulder pain. MRI shows a full-thickness supraspinatus tear and a cyst at the spinoglenoid notch. Which physical examination finding is most likely to be present?
Explanation
Question 68
A 50-year-old patient with an acute Charcot midfoot flare presents with severe erythema and swelling. The clinician is trying to differentiate between an acute Charcot neuroarthropathy and a severe soft-tissue infection (cellulitis). Which simple clinical test is most useful in this acute setting?
Explanation
Question 69
A 62-year-old male undergoes revision shoulder arthroplasty for unexplained pain and subtle loosening 2 years after his primary surgery. Intraoperative cultures are taken. Fourteen days later, the lab reports growth of Cutibacterium (Propionibacterium) acnes. What are the microbiologic characteristics of this organism?
Explanation
Question 70
A 35-year-old weightlifter presents with acute anterior shoulder pain after a heavy bench press. MRI confirms an isolated full-thickness rupture of the pectoralis major tendon at its insertion. In surgical repair, where should the tendon be anatomically reattached?
Explanation
Question 71
A 12-year-old girl is diagnosed with polyostotic fibrous dysplasia and precocious puberty. What is the underlying molecular pathogenesis of her musculoskeletal condition?
Explanation
Question 72
A 45-year-old female with known polyostotic fibrous dysplasia presents with a painless, slow-growing soft tissue mass in her right thigh. MRI reveals a well-circumscribed intramuscular mass with high T2 signal and low T1 signal. What is the most likely diagnosis of this soft tissue lesion?
Explanation
Question 73
A 55-year-old male with poorly controlled diabetes presents with a red, hot, swollen right foot. Radiographs show periarticular debris, fragmentation, and subluxation at the tarsometatarsal joints. According to the Eichenholtz classification, what stage does this represent and what is the primary initial treatment?
Explanation
Question 74
A 45-year-old manual laborer presents with an irreparable, massive posterosuperior rotator cuff tear. He has intact subscapularis function, a functioning deltoid, and preserved glenohumeral articular cartilage without arthritis. Which of the following is the most appropriate surgical option?
Explanation
Question 75
In reverse total shoulder arthroplasty (RSA), moving the center of rotation medially and distally compared to the native joint achieves which of the following biomechanical advantages?
Explanation
Question 76
A 30-year-old male requires surgical stabilization of a progressive "shepherd's crook" deformity of the proximal femur due to fibrous dysplasia. Which of the following principles is most critical for surgical success?
Explanation
Question 77
A 60-year-old diabetic female presents with a swollen, erythematous midfoot and an overlying plantar ulcer. Radiographs show destruction of the naviculocuneiform joint. Which of the following MRI findings most strongly suggests superimposed osteomyelitis rather than acute Charcot arthropathy alone?
Explanation
Question 78
During an arthroscopic rotator cuff repair, the surgeon evaluates the footprint of the torn tendons. Which of the following accurately describes the anatomic footprint of the infraspinatus tendon on the greater tuberosity?
Explanation
Question 79
A 70-year-old female is 2 years status-post reverse total shoulder arthroplasty for cuff tear arthropathy. Radiographs reveal erosive changes on the inferior scapular neck extending beyond the inferior screw of the baseplate, but not reaching the central peg. According to the Sirveaux classification, what grade of scapular notching is present?
Explanation
Question 80
A 14-year-old male with McCune-Albright syndrome presents with progressive lower extremity bowing and diffuse bone pain. Laboratory evaluation reveals hypophosphatemia, normal serum calcium, and elevated alkaline phosphatase. Which of the following mediators is most likely responsible for his metabolic bone abnormalities?
Explanation
Question 81
A 65-year-old male with a history of midfoot Charcot arthropathy (Eichenholtz Stage 3) presents with a recurrent plantar ulcer beneath a prominent cuboid. The foot is stable, and vascular supply is adequate. Non-operative management with a CROW boot has failed to heal the ulcer over the past 6 months. What is the most appropriate surgical intervention?
Explanation
Question 82
A 28-year-old professional volleyball player complains of vague posterior shoulder pain and weakness with external rotation. Examination reveals isolated atrophy of the infraspinatus fossa. An MRI demonstrates a paralabral cyst. At which of the following anatomical locations is the nerve compression most likely occurring?
Explanation
Question 83
A 62-year-old male presents with advanced osteoarthritis of the right shoulder. CT imaging reveals a biconcave glenoid with 20 degrees of retroversion and posterior subluxation of the humeral head. According to the Walch classification, what type of glenoid morphology is present?
Explanation
Question 84
A 35-year-old overhead athlete undergoes shoulder arthroscopy after failing conservative management for persistent shoulder pain. Diagnostic arthroscopy reveals an articular-sided partial tear of the supraspinatus involving 60% of the tendon thickness. What is the most appropriate management?
Explanation
Question 85
Three years after undergoing an anatomic total shoulder arthroplasty, a 65-year-old male develops progressive shoulder stiffness and pain. Inflammatory markers are normal. Aspiration yields fluid with a normal leukocyte count, but intraoperative tissue cultures eventually grow an organism at 11 days. What is the most likely responsible pathogen?
Explanation
Question 86
A 10-year-old girl is evaluated for precocious puberty and hyperthyroidism. On physical examination, she has large, irregular café-au-lait spots with jagged borders. Radiographs of her right femur reveal an intramedullary, expansile diaphyseal lesion with a "ground-glass" appearance. Which of the following best describes the underlying pathophysiology of her skeletal condition?
Explanation
Question 87
A 55-year-old male with long-standing, poorly controlled diabetes mellitus presents with a red, hot, and swollen right foot. He denies fevers, chills, or any open wounds. Pedal pulses are bounding. Radiographs demonstrate periarticular fragmentation, debris, and subluxation at the tarsometatarsal joints. His WBC count and ESR are within normal limits. What is the most appropriate initial management?
Explanation
Question 88
A 65-year-old man presents with chronic right shoulder pain and weakness. On physical examination, he has full passive range of motion. When his arm is passively abducted to 90 degrees and externally rotated to 90 degrees, the examiner releases the arm and the patient is unable to maintain the externally rotated position, causing the arm to drop into internal rotation. Which of the following muscles is most likely deficient, and what is its primary innervation?
Explanation
Question 89
A 72-year-old female undergoes a reverse total shoulder arthroplasty (rTSA) for severe rotator cuff tear arthropathy. Compared to the native anatomic shoulder, which of the following best describes the biomechanical alteration achieved by the classic Grammont-style reverse shoulder implant?
Explanation
Question 90
A 32-year-old female with known polyostotic fibrous dysplasia presents with worsening right groin pain. Radiographs demonstrate a severe varus deformity of the proximal femur ("Shepherd's crook" deformity) with extensive cortical thinning, but no acute fracture is seen. What is the most appropriate surgical management?
Explanation
Question 91
A 45-year-old man presents with a painless, massively swollen left shoulder. Radiographs show severe destruction of the humeral head, massive joint debris, and dislocation. Neurological examination reveals a loss of pain and temperature sensation in a "cape-like" distribution over his shoulders and upper extremities. What is the most appropriate next diagnostic step to determine the underlying etiology?
Explanation
Question 92
A 55-year-old manual laborer presents with chronic shoulder pain and weakness. MRI reveals a massive, retracted, and fatty-infiltrated tear of the supraspinatus and infraspinatus. His subscapularis is completely intact. Clinically, he has intact active forward elevation but a positive drop sign and severe external rotation lag. There is no evidence of glenohumeral osteoarthritis. Which of the following surgical procedures is most appropriate to restore his external rotation?
Explanation
Question 93
A 75-year-old male is evaluated 3 years after a reverse total shoulder arthroplasty. He is asymptomatic, but a standard AP radiograph shows bone resorption at the inferior scapular neck that extends medially, progressing just past the inferior screw of the glenoid baseplate. According to the Sirveaux classification, what grade of scapular notching does this represent?
Explanation
Question 94
A 22-year-old male undergoes a core needle biopsy of an expansile, radiolucent rib lesion found incidentally. The pathology report describes irregular, C-shaped woven bone trabeculae set within a moderately cellular fibrous stroma. Which of the following additional histologic features is classic for this diagnosis?
Explanation
Question 95
A 48-year-old woman is evaluated for right shoulder pain after a fall. The orthopaedic surgeon asks the patient to place the palm of her right hand on her left shoulder with her elbow pointing forward. The surgeon then attempts to pull the patient's hand off the shoulder while instructing the patient to resist. The patient is unable to keep her hand pressed against the shoulder. This physical examination finding is most indicative of a tear in which of the following structures?
Explanation
None
