ABOS Part I & AAOS OITE Orthopedic Review: Lisfranc Injury, Hallux Rigidus, Fibular Deficiency | Part 21550

Key Takeaway
This ABOS Part I & AAOS OITE orthopedic review module provides 33 advanced multiple-choice questions. It covers high-yield clinical cases on Lisfranc injuries, Hallux Rigidus, and Fibular Deficiency. Topics include diagnosis, surgical management, rehabilitation protocols, and common complications, mirroring the format of board examinations for comprehensive preparation.
ABOS Part I & AAOS OITE Orthopedic Review: Lisfranc Injury, Hallux Rigidus, Fibular Deficiency | Part 21550
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
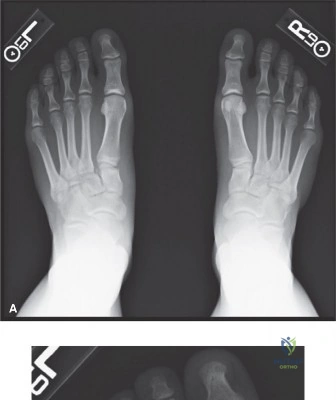
A 32-year-old male presents to the emergency department after a fall from a ladder, landing on his foot. He complains of severe midfoot pain and inability to bear weight. Initial non-weight-bearing radiographs are interpreted as normal. However, due to persistent pain and swelling, a weight-bearing AP radiograph is obtained, as shown below:
Based on the image and the case description, what is the most appropriate next step in management?
Explanation
Correct Answer: C
The provided image, described as a weight-bearing AP radiograph, likely demonstrates subtle widening between the medial cuneiform and the base of the second metatarsal, which is a hallmark of a Lisfranc injury. The case explicitly states that initial non-weight-bearing radiographs were interpreted as normal, highlighting the diagnostic challenge and the importance of weight-bearing views. While the image strongly suggests a Lisfranc injury, a CT scan (Option C) is considered the gold standard for detailed assessment of bony anatomy, fracture patterns, articular involvement, and precise displacement in all three planes. This information is critical for surgical planning. Proceeding directly to ORIF (Option D) without a detailed CT scan would be premature, as the exact extent and pattern of bony injury need to be fully understood. While an MRI (Option E) is useful for purely ligamentous injuries and soft tissue damage, a CT scan is more critical for acute bony dislocations and fracture-dislocations, which are highly suspected here. Discharging the patient (Option A) or initiating non-operative management (Option B) would be inappropriate given the high suspicion for an unstable Lisfranc injury, which typically requires surgical intervention.
Question 2
A 40-year-old male sustains a high-energy twisting injury to his foot. Clinical examination reveals significant midfoot swelling, ecchymosis, and tenderness over the tarsometatarsal joints. Radiographs show a subtle avulsion fracture from the plantar aspect of the second metatarsal base (fleck sign) and a 3mm diastasis between the medial cuneiform and the second metatarsal on a weight-bearing AP view. Which of the following statements regarding the anatomical and biomechanical significance of this injury is most accurate?
Explanation
Correct Answer: C
The case explicitly states that the base of the second metatarsal serves as the keystone of the tarsometatarsal articulation, locking into a recess formed by the medial and intermediate cuneiforms. Its unique anatomical position and strong ligamentous attachments, particularly the interosseous Lisfranc ligament connecting the medial cuneiform to the base of the second metatarsal, render it the linchpin of midfoot stability. An avulsion fracture from the plantar aspect of the second metatarsal base (fleck sign) is pathognomonic for a disruption of this critical interosseous Lisfranc ligament. Option A is incorrect because the dorsal ligaments are weaker and less critical for stability than the interosseous and plantar ligaments. Option B is incorrect; the second metatarsal base is recessed and considered a stable component, not the most mobile. Option D is incorrect; the first and second rays are considered the most stable components due to strong ligamentous attachments. Option E is incorrect; the second metatarsal base, not the cuboid-fourth metatarsal articulation, is described as the keystone.
Question 3
A 28-year-old professional athlete presents with acute midfoot pain after a direct crush injury. Initial radiographs show a fracture of the base of the second metatarsal with 1.5mm widening between the medial cuneiform and the second metatarsal. Stress radiographs under fluoroscopy demonstrate dynamic instability with greater than 3mm diastasis. The patient is otherwise healthy. Which of the following is the most appropriate management strategy?
Explanation
Correct Answer: B
The case outlines clear operative indications for Lisfranc injuries. The patient presents with a fracture of the second metatarsal base and dynamic instability (greater than 3mm diastasis on stress views), both of which are absolute indications for surgical intervention. The overarching goal is anatomical reduction and stable fixation. ORIF with transarticular screw fixation (Option B) is the standard of care for acute, unstable Lisfranc injuries. Non-weight-bearing cast immobilization (Option A) is reserved for truly stable, non-displaced sprains (Grade I), which is not the case here. Primary arthrodesis (Option C) is typically indicated for severe comminuted injuries, chronic unreduced injuries, or in patients with pre-existing midfoot arthritis, not usually for an acute, reducible injury in a young, healthy athlete. External fixation (Option D) is generally reserved for severe open injuries, highly comminuted fractures, or in a 'damage control' scenario for polytrauma patients, which is not described. Discharging the patient (Option E) would lead to chronic instability and poor outcomes.
Question 4
During surgical planning for a Lisfranc injury, the surgeon reviews the patient's CT scan, which confirms a fracture-dislocation involving the second and third tarsometatarsal joints. The surgical approach will involve two dorsal incisions. The dorsal incision for the second/third ray is typically placed between which two structures, and what neurovascular structure is at highest risk?
Explanation
Correct Answer: B
The case details the surgical approach: 'A dorsal incision (Second/Third Ray) is a longitudinal incision over the second TMT joint, often extending to expose the third TMT joint. This incision is placed between the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) tendons, or specifically between the EHL and the tendon to the second toe.' It further states: 'Careful dissection is paramount to avoid neurovascular injury, protecting the dorsalis pedis artery and deep peroneal nerve, which typically lie laterally to the EHL.' Therefore, the deep peroneal nerve is the neurovascular structure at highest risk with this incision. The other options describe incorrect internervous planes or nerves not primarily at risk with this specific dorsal incision.
Question 5
A 55-year-old male undergoes open reduction and internal fixation for a Lisfranc fracture-dislocation. Intraoperatively, after initial debridement, the surgeon begins the reduction sequence. The image below shows an intraoperative fluoroscopic view during the reduction process.
Based on the case description and the image, which of the following best describes the critical next step in achieving anatomical reduction and stability?

Explanation
Correct Answer: C
The case emphasizes the 'Top-Down' approach to reduction, stating: 'Focus on reducing the first and second TMT joints first, as they are the most stable and crucial for midfoot alignment.' It then specifically highlights the second ray reduction as 'the most critical step,' focusing on 'anatomical reduction of the second metatarsal base into its recess within the cuneiforms' and 'restoring the MC-2MT alignment.' The image likely depicts this critical stage of reduction, possibly with provisional K-wire fixation. While the first ray reduction (Option B) is important, the second ray is explicitly called 'the cornerstone' and 'most critical.' Reducing the lateral rays (Option A) comes after the first and second. Indirect reduction (Option D) is an initial step but not the definitive critical step for anatomical reduction. Primary arthrodesis (Option E) is a salvage procedure for specific complex cases, not the primary reduction strategy for an acute, reducible injury.
Question 6
Following successful anatomical reduction of a Lisfranc injury, the surgeon proceeds with definitive internal fixation. The image below shows a post-operative radiograph.
Regarding the critical fixation of the second ray, which of the following statements is most consistent with the recommended technique and subsequent management?

Explanation
Correct Answer: C
The case states: 'A 3.5mm or 4.0mm cortical screw (non-compressive, fully threaded preferred by many to avoid over-compression and potential cartilage damage if left in place) is placed from the dorsal aspect of the medial cuneiform into the base of the second metatarsal. This screw effectively bridges the Lisfranc joint and stabilizes the crucial MC-2MT articulation.' It further specifies: 'Hardware, especially transarticular screws, is typically removed 3-6 months post-operatively to allow for restoration of normal TMT joint motion and prevent hardware-related complications.' Option A is incorrect because hardware is typically removed. Option B is incorrect regarding the timing of removal and the preference for fully threaded screws to avoid over-compression if left in place, though headless screws can be used. Option D is incorrect as K-wire fixation alone is insufficient for definitive stabilization of this critical joint. Option E is incorrect; while dorsal plates are increasingly used, screws remain a gold standard, and plates do not eliminate the need for hardware removal, especially if crossing joints.
Question 7
A 48-year-old construction worker undergoes ORIF for a severe Lisfranc fracture-dislocation. Despite meticulous surgical technique and anatomical reduction, he develops persistent midfoot pain, swelling, and stiffness 18 months post-operatively. Radiographs show degenerative changes across the first, second, and third tarsometatarsal joints. Which of the following is the most common long-term complication of Lisfranc injuries, and what is the most likely salvage procedure for this patient?
Explanation
Correct Answer: D
The case explicitly states that 'Post-Traumatic Arthritis (PTA)' is 'The most common long-term complication, occurring in 20-90% of cases, even after anatomical reduction.' The patient's symptoms of persistent pain, swelling, stiffness, and radiographic evidence of degenerative changes 18 months post-operatively are highly indicative of PTA. For failed conservative management of PTA, the case lists 'arthrodesis (TMT fusion, particularly for the painful first, second, and third rays)' as the primary surgical salvage option. While other complications listed are possible, PTA is the most common long-term issue, and arthrodesis is the appropriate salvage for symptomatic arthritis. Nerve injury (A), hardware failure (B), CRPS (C), and malunion (E) are all potential complications, but the clinical presentation and timeframe strongly point to PTA.
Question 8
A 35-year-old female undergoes ORIF for a Lisfranc injury. Post-operatively, she is placed in a well-padded splint. According to the typical rehabilitation protocol described in the case, which of the following statements accurately reflects the initial phase of her recovery?
Explanation
Correct Answer: D
The case describes Phase 1 of rehabilitation as 'Immobilization and Non-Weight Bearing.' It states: 'Weight Bearing: Strict NWB for the entire period. Crutches or a knee scooter are used.' And 'Immobilization: After wound inspection (1-2 weeks): Non-weight-bearing (NWB) cast or CAM boot.' The duration is typically '6-8 weeks.' For ROM, it states: 'Toe ROM exercises (flexion/extension) may be initiated early if not restricted by pain or swelling. Ankle ROM exercises (dorsiflexion/plantarflexion, inversion/eversion) are encouraged, avoiding any motion that stresses the midfoot.' Therefore, Option D accurately reflects these guidelines. Options A, B, and E are incorrect as they suggest early weight-bearing or midfoot motion, which is contraindicated. Option C is incorrect as hardware removal typically occurs much later (3-6 months).
Question 9
A 60-year-old patient with a history of diabetes and pre-existing midfoot osteoarthritis presents with a severely comminuted Lisfranc fracture-dislocation that is irreducible with closed manipulation. Given the patient's comorbidities and the nature of the injury, the surgeon considers primary arthrodesis. Which of the following statements regarding primary arthrodesis for Lisfranc injuries is most accurate?
Explanation
Correct Answer: C
The case states: 'Primary Arthrodesis: In severe comminuted injuries, chronic unreduced injuries, or in patients with pre-existing midfoot arthritis, primary arthrodesis of the first, second, and third TMT joints may be indicated.' This aligns perfectly with the patient's presentation (severe comminution, irreducible, pre-existing arthritis). Option A is incorrect as it describes indications for non-operative or ORIF in a different patient population. Option B is incorrect because the fourth and fifth TMT joints are often preserved due to their inherent mobility. Option D is incorrect; the literature review states that comparative studies show mixed results, with some suggesting lower reoperation rates but potentially equivalent functional outcomes, not consistently superior outcomes or lower PTA rates. Option E is incorrect; while it aims for stability, it does not necessarily allow for earlier weight-bearing than ORIF, and hardware removal may still be necessary if symptomatic.
Question 10
A 22-year-old collegiate football player sustains a Lisfranc injury. Despite undergoing meticulous anatomical reduction and stable internal fixation, he develops chronic pain and functional limitations. According to the key literature and guidelines, which factor is most strongly correlated with a poor long-term outcome and increased incidence of post-traumatic arthritis in Lisfranc injuries?
Explanation
Correct Answer: C
The 'Summary of Key Literature and Guidelines' section explicitly states: 'Anatomical Reduction is Paramount: The fundamental principle underscored by numerous studies is that anatomical reduction of the TMT joint complex is the strongest predictor of good long-term outcomes and reduced incidence of post-traumatic arthritis. Residual displacement greater than 1-2mm is associated with significantly poorer results.' Options A and B describe standard or recommended surgical/post-operative practices aimed at improving outcomes, not causing poor outcomes. Option D is part of the recommended early rehabilitation protocol. Option E (young age and high activity) might influence the mechanism of injury or the demands placed on the foot, but residual displacement is the direct surgical factor most strongly linked to poor outcomes.
Question 11
A 38-year-old male presents with a Lisfranc injury following a motor vehicle accident. Pre-operative imaging confirms a Type B2 injury according to the Myerson classification, with partial incongruity involving the second and third rays. During the surgical approach, the surgeon identifies the dorsalis pedis artery and deep peroneal nerve. Which of the following statements accurately describes the typical anatomical relationship of these structures relative to the surgical incisions for a Lisfranc repair?
Explanation
Correct Answer: B
The case describes the dorsal incision for the second/third ray as being placed 'between the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) tendons.' It then explicitly states: 'Careful dissection is paramount to avoid neurovascular injury, protecting the dorsalis pedis artery and deep peroneal nerve, which typically lie laterally to the EHL.' This directly supports Option B. Option A is incorrect as these structures are not typically medial to the tibialis anterior in this context. Option C is incorrect; the deep peroneal nerve is typically deeper, not superficial to the retinaculum. Option D is incorrect; the dorsalis pedis artery is vulnerable in dorsal approaches. Option E is incorrect; the medial incision for the first ray is between the tibialis anterior and EHL, not EHL and EDL, and the neurovascular bundle is most prominent more laterally.
Question 12
A 3-year-old male presents with a congenital right lower limb deformity. Clinical examination reveals a significant limb length discrepancy (LLD) of 4 cm, a noticeable ankle valgus, and hypoplasia of the 4th and 5th toes. Radiographs confirm a shortened fibula, but a distinct distal fibular physis is identifiable, and the ankle joint, while in valgus, appears to have some inherent stability. The patient's parents are concerned about the progressive nature of the LLD.
Based on the Paley classification system described in the case, which type of fibular deficiency is most consistent with this patient's presentation?
Explanation
Correct Answer: C
The correct answer is Type 1A. According to Paley's classification, Type 1A fibular deficiency is characterized by a shortened fibula where the distal fibular physis is present and functional. This allows for potential lengthening and is typically associated with moderate LLD and a relatively stable ankle joint, despite the common presence of valgus deformity. The patient's presentation of a 4 cm LLD, ankle valgus, and the presence of a distinct distal fibular physis directly aligns with the criteria for Type 1A.
Type 1B involves a portion of the fibula being present, but the distal physis is absent, leading to progressive LLD and significant ankle instability. Type 2 signifies complete absence of the fibula, resulting in profound LLD and severe ankle instability. Pappas's classification and Achilles-Kuts classification are alternative systems, but Paley's is specifically detailed in the case for its correlation with distal fibular physis presence and ankle stability, making it the most appropriate for this question.
Question 13
A 5-year-old child with fibular deficiency is noted to have a characteristic deformity of the tibia. Clinically, the tibia appears bowed, and radiographs confirm this angulation. The parents are concerned about the progression of this deformity and its potential impact on the skin.
Which of the following best describes the typical tibial deformity seen in fibular deficiency?
Explanation
Correct Answer: B
The correct answer is anterior-medial bowing. The case explicitly states that 'The tibia, in the absence of its fibular buttress, often exhibits anterior-medial bowing.' This deformity can range from subtle curvature to severe angulation, sometimes complicated by skin tethering or impending pseudoarthrosis. This characteristic bowing is a direct consequence of the fibula's absence, which normally provides a lateral buttress and influences tibial growth. The other options describe different types of deformities not specifically highlighted as the typical tibial deformity in fibular deficiency.
Question 14
A 7-year-old male with Paley Type 1B fibular deficiency presents with significant and progressive ankle valgus, making shoe wear difficult and causing a noticeable limp. Radiographs confirm severe talar tilt and a widened ankle mortise. The lateral malleolus is rudimentary and non-functional. The parents are seeking intervention to improve their child's ambulation and stability.
Based on the surgical anatomy and biomechanics described in the case, what is the primary biomechanical reason for the nearly universal ankle valgus deformity in fibular deficiency?
Explanation
Correct Answer: C
The correct answer is absence or hypoplasia of the lateral malleolus. The case clearly states: 'The fibula normally forms the lateral malleolus, providing critical stability to the talus within the mortise. In fibular deficiency... Ankle Valgus: This is nearly universal, ranging from mild to severe, due to the lack of lateral support and often accompanied by talar tilt.' The absence or severe hypoplasia of the fibula directly removes the lateral buttress that stabilizes the talus, leading to its lateral tilt and the resulting valgus deformity. While Achilles contracture contributes to equinus and muscle imbalance can exacerbate the deformity, the fundamental structural cause of valgus is the lack of a competent lateral malleolus. Deltoid ligament hyperplasia is not the primary cause, and peroneal muscle overactivity is contrary to the typical hypoplasia of these muscles.
Question 15
A 5-year-old child with fibular deficiency presents with a rigid foot deformity, characterized by severe equinovalgus and difficulty with ambulation. The child experiences pain with weight-bearing and struggles to find comfortable footwear. Radiographs are obtained to further characterize the foot pathology.
Which of the following foot deformities is a hallmark feature of fibular deficiency and often contributes significantly to rigidity, pain, and progressive deformity, as described in the case?
Explanation
Correct Answer: C
The correct answer is tarsal coalition. The case explicitly lists tarsal coalition as a characteristic foot deformity in fibular deficiency, stating: 'A fibrous, cartilaginous, or bony bridge between two or more tarsal bones, frequently involving the calcaneus and navicular or talus and calcaneus. This can cause rigidity, pain, and contribute to progressive deformity.' This directly matches the clinical presentation of a rigid, painful foot with difficulty in ambulation. While other foot deformities can occur, tarsal coalition is specifically highlighted as a significant contributor to rigidity and pain in the context of fibular deficiency. Metatarsus adductus, hallux valgus, pes cavus, and congenital vertical talus are distinct foot pathologies not universally associated with fibular deficiency in the same hallmark manner.
Question 16
A 7-year-old male with Paley Type 1B fibular deficiency presents with a projected limb length discrepancy (LLD) of 8 cm at skeletal maturity. He exhibits a progressive gait abnormality, and his parents report increasing difficulty with compensatory shoe lifts. Clinical examination also reveals significant anterior-medial bowing of the tibia and progressive ankle valgus. The patient has no significant medical comorbidities.
Based on the indications for intervention described in the case, what is the most appropriate initial management strategy for this patient?
Explanation
Correct Answer: D
The correct answer is gradual limb lengthening and deformity correction with an external fixator. The case outlines operative indications including 'Significant LLD (>3-5 cm or projected significant LLD),' 'Severe Ankle Instability/Deformity,' and 'Progressive Foot Deformity' or 'Tibial Bowing/Pseudoarthrosis Risk.' This patient has a projected LLD of 8 cm, progressive gait abnormality, significant tibial bowing, and progressive ankle valgus, all of which are strong operative indications. Gradual lengthening with an external fixator (e.g., Ilizarov or Taylor Spatial Frame) is the gold standard for correcting significant LLD and multi-planar deformities simultaneously in pediatric patients. Shoe lifts are for mild LLD (<3-5 cm). Contralateral epiphysiodesis is typically considered for less severe LLD or as an adjunct, not as the primary treatment for an 8 cm discrepancy with associated deformities. Primary Syme's amputation is usually reserved for severe Type 2 deficiencies or when limb salvage is deemed unfeasible or less functional. Serial casting might address some soft tissue contractures but cannot correct significant bony LLD or angular deformities.
Question 17
A 2-year-old with severe Paley Type 2 fibular deficiency presents with profound limb length discrepancy, a non-functional foot, and severe ankle instability. The family is counseled on various treatment options, including extensive limb salvage procedures and primary amputation. They are weighing the long-term implications of each approach.
When considering a primary Syme's amputation for this child, which of the following is the MOST compelling advantage compared to extensive limb salvage, as highlighted in the case?
Explanation
Correct Answer: D
The correct answer is preservation of distal tibial growth potential for an end-bearing stump. The case explicitly states the rationale for Syme's amputation: 'Creates an end-bearing stump, preserves growth potential of the distal tibia, and allows for excellent prosthetic fitting. This often results in superior functional outcomes and requires fewer surgeries than complex limb salvage.' While superior functional outcomes and fewer surgeries are also key advantages, the preservation of the distal tibial epiphysis is a unique anatomical benefit that directly contributes to the creation of a robust, end-bearing stump, which is crucial for optimal prosthetic fitting and long-term function. Cosmetic outcome is subjective and often not superior with amputation. Psychological impact is significant with both options and requires support. While external fixation has a high risk of pin site infection, amputation has its own set of infection risks. Complete limb length equality is not guaranteed without further intervention, as the contralateral limb may still grow, requiring future management.
Question 18
A 6-year-old child is undergoing gradual tibial lengthening using an external fixator for fibular deficiency. The surgical team is establishing the post-operative distraction protocol to optimize regenerate bone formation and minimize complications.
According to the principles of distraction osteogenesis described in the case, what is the typical daily distraction rate and latency period for optimal regenerate bone formation?
Explanation
Correct Answer: B
The correct answer is 1 mm/day after a 5-7 day latency period. The case details the distraction protocol: 'Typically, distraction begins 5-7 days post-operatively (latency period) at a rate of 1 mm per day, divided into four equal increments (0.25 mm every 6 hours). This rate aims to optimize regenerate bone formation.' This specific rate and latency period are well-established in distraction osteogenesis to allow for initial callus formation before mechanical stress is applied, promoting robust new bone growth. Deviations from this protocol can lead to complications such as nonunion (too fast) or premature consolidation (too slow).
Question 19
A surgical team is evaluating a 9-year-old for complex limb reconstruction for severe fibular deficiency. The proposed treatment involves multiple staged procedures, including limb lengthening with an external fixator, ankle stabilization, and foot reconstruction. During the counseling session, the family expresses significant doubts about their ability to manage the prolonged rehabilitation, daily pin site care, and frequent clinic visits required over several years. They are also concerned about the child's potential non-compliance with the demanding regimen.
Based on the contraindications for intervention described in the case, the family's expressed concerns represent which of the following in the context of limb reconstruction?
Explanation
Correct Answer: B
The correct answer is a relative contraindication. The case explicitly lists 'Lack of Patient/Family Compliance' as a relative contraindication, stating: 'Successful outcomes from complex limb reconstruction require dedicated adherence to rehabilitation protocols, which can be prolonged and demanding.' While not an absolute contraindication that would completely preclude surgery, a lack of compliance or realistic expectations significantly increases the risk of complications and poor outcomes, making it a serious consideration that must be addressed. It is not a minor risk factor, nor an indication for immediate surgery, nor a reason to delay indefinitely without further discussion; rather, it requires intensive counseling and ensuring commitment before proceeding.
Question 20
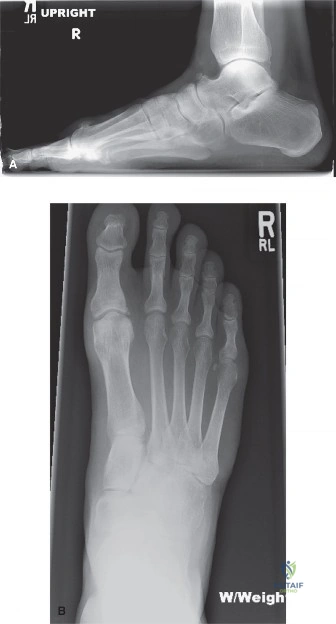
A 1-year-old presents with a short right lower limb and foot deformities. The image below is obtained during the initial evaluation to assess the overall limb. The clinical team suspects fibular deficiency.
Based on the comprehensive assessment principles outlined in the case, what is the MOST critical next step in accurately evaluating this child's limb length discrepancy and overall mechanical alignment?

Explanation
Correct Answer: B
The correct answer is standing full-length AP/Lateral radiographs (LLDograms). The case emphasizes the importance of radiographic imaging, stating: 'Standing Full-Length AP/Lateral Radiographs (LLDograms): Essential for accurate LLD measurement and assessment of overall mechanical alignment of the lower extremity. These are critical for quantifying angular deformities and planning osteotomies.' While MRI is useful for soft tissue and growth plate assessment, and genetic testing may be considered for associated syndromes, LLDograms are the most critical and standard initial imaging modality for precisely quantifying LLD and overall mechanical alignment, which are fundamental for diagnosis and treatment planning in fibular deficiency. Bone biopsy and surgical exploration are invasive procedures not indicated as initial diagnostic steps for LLD and alignment.
Question 21
A 7-year-old child undergoing tibial lengthening for fibular deficiency, as shown in the image below, is in the distraction phase. The patient's parents report a sudden onset of severe pain in the foot, accompanied by swelling and paresthesias in the toes. On examination, the foot is tense, and capillary refill is sluggish.
Based on the potential complications described in the case, what is the MOST immediate and critical concern for this patient?

Explanation
Correct Answer: D
The correct answer is vascular impairment (e.g., compartment syndrome). The symptoms described—sudden onset of severe pain, swelling, paresthesias in the toes, tense foot, and sluggish capillary refill—are classic signs of acute compartment syndrome or other forms of severe vascular compromise. The case lists 'Vascular Impairment: Rare (<1%) but limb-threatening' and specifies 'Immediate release of constricting elements (fasciotomy, removal of tension), surgical exploration, vascular repair/grafting' as management. This is an orthopedic emergency requiring immediate attention to prevent irreversible tissue damage. While pin site infection, premature consolidation, nerve injury, and joint stiffness are all potential complications of limb lengthening, they typically do not present with such acute, limb-threatening symptoms.
Question 22
A 58-year-old male presents with a 2-year history of progressive pain and stiffness in his right great toe, particularly during push-off. He reports difficulty wearing dress shoes and has noticed a compensatory early heel-off during ambulation. Physical examination reveals tenderness and a palpable dorsal prominence at the first MTP joint, with passive dorsiflexion limited to 20 degrees and pain at the end range. Weight-bearing radiographs show moderate dorsal osteophytes, mild joint space narrowing, and subchondral sclerosis. Based on the provided case, which of the following biomechanical factors is most directly implicated in the patient's symptoms and the progression of his hallux rigidus?
Explanation
Correct Answer: C
The case explicitly states that the first MTP joint plays a pivotal role in the propulsion phase of gait and is integral to the 'windlass mechanism.' As the MTP joints dorsiflex during propulsion, the plantar fascia becomes taut, shortening the arch and converting the foot into a rigid lever for propulsion. The patient's symptoms of pain during push-off, difficulty with shoe wear, and compensatory early heel-off, coupled with limited dorsiflexion and dorsal osteophytes, directly point to a mechanical blockade of dorsiflexion. This restriction inhibits the windlass mechanism, leading to a less efficient and more painful gait, which is a core pathobiomechanical aspect of hallux rigidus as described in the case.
A. Hyperpronation of the subtalar joint can alter foot mechanics but is not described as the most direct biomechanical factor for hallux rigidus in the provided text, which emphasizes dorsal impingement and metatarsus primus elevatus.
B. Tibialis posterior dysfunction primarily relates to adult-acquired flatfoot deformity and is not highlighted as a direct cause of hallux rigidus in the case.
D. Intrinsic foot muscle weakness can contribute to various foot deformities but is not presented as the primary biomechanical driver of hallux rigidus symptoms or progression in the context of the windlass mechanism and dorsal impingement.
E. Excessive plantarflexion of the first metatarsal is contrary to the concept of metatarsus primus elevatus, which involves an elevated first metatarsal and increased dorsal compression, a predisposing factor for HR mentioned in the case. Therefore, this option describes an opposite biomechanical scenario.
Question 23
A 35-year-old active runner presents with early-stage hallux rigidus, characterized by intermittent pain and mild dorsal osteophytes on radiographs, consistent with Coughlin and Shurnas Grade 1. He has failed a 3-month trial of NSAIDs and activity modification. During surgical planning for a cheilectomy, the surgeon emphasizes meticulous dissection in the dorsomedial aspect of the first MTP joint. Which neurovascular structure is at highest risk of iatrogenic injury during a standard dorsomedial approach to the first MTP joint?
Explanation
Correct Answer: D
The case explicitly states under 'Neurovascular Structures' within the 'First MTP Joint Anatomy' section that 'The medial dorsal cutaneous nerve (a branch of the superficial fibular nerve) typically courses dorsomedially, posing a risk during dorsal incisions.' Furthermore, in the 'Dorsomedial Approach' section, it reiterates, 'Meticulous dissection is required to identify and protect the branches of the medial dorsal cutaneous nerve, which typically courses dorsomedially over the first MTP joint. Retraction of these nerve branches... is critical to prevent iatrogenic injury, which can lead to post-operative numbness or painful neuroma formation.'
A. The medial plantar nerve provides sensation to the plantar aspect of the great toe and is not typically in the field of a dorsal incision.
B. The deep fibular nerve (deep peroneal nerve) typically innervates the intrinsic muscles of the dorsum of the foot and the first web space, but the medial dorsal cutaneous nerve is the more superficial and directly vulnerable structure in a dorsomedial incision for the first MTP joint.
C. The dorsalis pedis artery and its branches supply the dorsal aspect but are generally deeper and less superficially vulnerable than the medial dorsal cutaneous nerve during the initial skin and subcutaneous dissection for a dorsomedial approach.
E. The flexor hallucis longus (FHL) tendon runs plantarly between the sesamoids and is not at risk during a dorsal approach.
Question 24
A 62-year-old sedentary patient presents with severe, constant pain in her left great toe, significantly limiting her ability to walk even short distances. She has tried various conservative treatments, including orthotics, NSAIDs, and multiple corticosteroid injections over the past year, with only transient relief. Weight-bearing radiographs reveal severe joint space effacement, extensive dorsal and plantar osteophytes, subchondral sclerosis, and cyst formation at the first MTP joint. Based on the Coughlin and Shurnas classification system and the provided case, what is the most appropriate surgical recommendation for this patient?
Explanation
Correct Answer: C
The patient's presentation of severe, constant pain, failure of extensive conservative management, and radiographic findings of 'severe joint space effacement, extensive dorsal and plantar osteophytes, subchondral sclerosis, and cyst formation' are classic indicators of end-stage hallux rigidus, corresponding to Coughlin and Shurnas Grade 4. The case explicitly states under 'Operative Indications' and 'Summary of Key Literature and Guidelines' that 'Arthrodesis (fusion) of the first MTP joint is often considered the gold standard for end-stage hallux rigidus due to its reliable pain relief and high success rates' and 'provides the most reliable and durable pain relief.' Given the patient's sedentary lifestyle, the loss of motion associated with fusion is less of a concern compared to achieving predictable pain relief.
A. Cheilectomy with a Moberg osteotomy is indicated for Grade 1-3 hallux rigidus, primarily for motion preservation in less severe cases, and would be ineffective for end-stage disease.
B. Interposition arthroplasty is indicated for Grade 3-4 HR in older, lower-demand patients who wish to preserve some motion, but the case notes 'results are variable, with concerns regarding graft incorporation, spacer migration, and long-term durability.' Arthrodesis offers more reliable pain relief for end-stage disease.
D. Microfracture is indicated for 'focal cartilage defects... where the surrounding cartilage is relatively healthy' in younger patients, not for diffuse, end-stage arthritis.
E. Hemiarthroplasty is also indicated for Grade 3-4 HR in older, less active individuals seeking motion preservation, but similar to interposition arthroplasty, concerns exist regarding implant loosening, wear of the contralateral cartilage, and less predictable long-term outcomes compared to arthrodesis for severe cases.
Question 25
A 40-year-old female presents with a 6-month history of intermittent pain in her right great toe, exacerbated by high-heeled shoes and prolonged walking. Clinical examination reveals mild dorsal tenderness and a slight restriction in passive dorsiflexion (approximately 45 degrees). Radiographs show minimal dorsal osteophytes with preserved joint space. She is diagnosed with early-stage hallux rigidus (Coughlin and Shurnas Grade 1). According to the case, which of the following non-operative treatment modalities should be the initial recommendation?
Explanation
Correct Answer: C
The case clearly states under 'Non-Operative Indications' that 'Non-operative management is typically the first-line treatment, especially for early stages of hallux rigidus (Coughlin and Shurnas Grade 0, 1, and often Grade 2).' Among the non-operative treatment modalities, 'Footwear Modification: Shoes with a stiff sole, rocker-bottom sole, or wide toe box can reduce motion at the MTP joint and alleviate dorsal impingement' is listed as a primary intervention. This directly addresses the patient's symptoms exacerbated by high-heeled shoes and aims to reduce stress on the affected joint.
A. Corticosteroid injections are mentioned as providing 'temporary pain relief' but are 'not curative' and 'repeated injections are discouraged due to potential cartilage damage.' They are typically considered after initial, less invasive measures.
B. Surgical cheilectomy is an operative indication, considered when conservative measures have failed, not as an initial treatment for early-stage disease.
D. Physical therapy is a modality focused on 'improving range of motion,' but the initial step for early-stage HR often involves reducing aggravating factors through footwear modification before aggressive mobilization, especially if pain is activity-related.
E. Opioid analgesics are not a first-line treatment for chronic musculoskeletal pain like hallux rigidus, especially in early stages, due to their side effect profile and risk of dependence. NSAIDs are mentioned as a more appropriate pharmacological option.
Question 26
A 50-year-old male with Coughlin and Shurnas Grade 2 hallux rigidus undergoes a cheilectomy. During the procedure, after exposing the first MTP joint via a dorsomedial approach, the surgeon identifies significant dorsal osteophytes on both the metatarsal head and the proximal phalanx base. The image below depicts the removal of these osteophytes. What is the primary intraoperative goal of this specific step in the cheilectomy procedure?
Explanation
Correct Answer: B
The case describes cheilectomy as a procedure primarily to 'remove dorsal osteophytes and improve dorsiflexion.' Under 'Cheilectomy Dorsal Decompression - Technique,' it explicitly states: 'Using a small osteotome, rongeur, or a high-speed burr, these osteophytes are systematically resected. The goal is to remove sufficient bone to achieve at least 70-80 degrees of pain-free dorsiflexion intraoperatively.' The image illustrates the removal of these dorsal osteophytes, directly correlating with this primary goal.
A. Shortening the first metatarsal is not the primary goal of a cheilectomy; it might be a secondary effect of some osteotomies (like Watermann) but not the main objective of osteophyte removal.
C. Decompressing the plantar plate complex and releasing the sesamoids is not the primary focus of a dorsal cheilectomy, which targets dorsal impingement.
D. While cheilectomy involves bone resection, its primary goal is not to prepare for arthroplasty unless it's part of a staged procedure or a salvage plan, which is not implied here. Cheilectomy is a motion-preserving procedure on its own.
E. Preventing avascular necrosis (AVN) is not a direct goal of osteophyte removal. AVN is a rare complication, and reducing bone mass in this context is for decompression, not AVN prevention.
Question 27
A 48-year-old patient with Coughlin and Shurnas Grade 2 hallux rigidus undergoes a cheilectomy. Intraoperatively, after adequate dorsal osteophyte resection, the surgeon notes that functional dorsiflexion remains limited, particularly when the hallux is loaded. The patient's pre-operative radiographs also showed a subtle metatarsus primus elevatus. Based on the case, which additional procedure would be most appropriate to functionally increase dorsiflexion by reorienting the proximal phalanx?
Explanation
Correct Answer: C
The case describes the Moberg osteotomy as 'Often combined with cheilectomy for Grade 1-3 hallux rigidus, particularly when functional hallux limitus persists despite adequate cheilectomy or when a metatarsus primus elevatus is present. It functionally increases dorsiflexion of the hallux by reorienting the proximal phalanx.' The patient's scenario of persistent limited dorsiflexion after cheilectomy and pre-existing metatarsus primus elevatus directly aligns with the indications for a Moberg osteotomy.
A. A Watermann osteotomy is a dorsal closing wedge osteotomy of the distal metatarsal that shortens and plantarflexes the metatarsal head. While it can address metatarsus primus elevatus, the question specifically asks for a procedure that reorients the proximal phalanx to increase dorsiflexion, which is the direct effect of a Moberg osteotomy.
B. Interposition arthroplasty is for Grade 3-4 HR and aims to preserve motion by inserting a graft or spacer, not to reorient the phalanx for functional dorsiflexion in a Grade 2 case.
D. Arthrodesis is the gold standard for end-stage (Grade 4) HR and involves fusion, sacrificing motion, which is not the goal for a Grade 2 patient where motion preservation is still desired.
E. Microfracture is for focal cartilage defects in younger patients, not for addressing persistent functional hallux limitus or metatarsus primus elevatus after cheilectomy.
Question 28
A 70-year-old patient with end-stage hallux rigidus (Coughlin and Shurnas Grade 4) undergoes a first MTP joint arthrodesis. During the procedure, after preparing the joint surfaces, the surgeon meticulously positions the joint for fixation. According to the case, what is the ideal position for fusion of the first MTP joint to facilitate comfortable shoe wear and optimize the push-off phase of gait?
Explanation
Correct Answer: C
Under 'Arthrodesis Fusion - Technique,' the case explicitly states: 'The ideal position for fusion is typically 10-20 degrees of dorsiflexion relative to the plantar aspect of the foot (or 5-10 degrees relative to the first metatarsal shaft), 10-15 degrees of valgus, and slight external rotation. This position facilitates comfortable shoe wear and optimizes the push-off phase of gait despite the loss of motion.'
A. 0 degrees dorsiflexion would make push-off difficult and shoe wear uncomfortable.
B. 25-30 degrees dorsiflexion is generally considered excessive and can lead to transfer metatarsalgia or difficulty with shoe wear. 5 degrees varus is also incorrect; valgus is preferred.
D. 5-10 degrees plantarflexion would severely impair push-off and make walking very difficult.
E. While 15-20 degrees dorsiflexion is within the range, 'relative to the first metatarsal shaft' is a different reference point, and 0 degrees valgus and slight internal rotation are not the ideal parameters described in the text.
Question 29
A 55-year-old male undergoes a first MTP joint arthrodesis for severe hallux rigidus. Six months post-operatively, he presents with persistent pain under his second and third metatarsal heads, particularly with ambulation. Radiographs confirm a solid fusion of the first MTP joint in an appropriate position. Based on the case, what is the most likely complication this patient is experiencing, and what is the typical initial management?
Explanation
Correct Answer: C
The patient's symptoms of 'persistent pain under his second and third metatarsal heads' after a solid first MTP joint arthrodesis, even in an appropriate position, are classic for 'Transfer Metatarsalgia.' The case explicitly lists this as a complication: 'Altered weight-bearing mechanics leading to pain under lesser metatarsals (often after cheilectomy due to shortening or arthrodesis).' The recommended management is 'accommodative orthotics, shoe modifications, metatarsal pads. Rarely, lesser metatarsal osteotomies.'
A. Nonunion is ruled out by the statement 'Radiographs confirm a solid fusion.' If it were nonunion, the management would be revision arthrodesis.
B. Malunion is ruled out by 'solid fusion... in an appropriate position.' If it were malunion, a corrective osteotomy might be considered if symptomatic.
D. Hardware irritation typically presents as localized pain over the hardware, not specifically under the lesser metatarsal heads. While hardware removal is a management option, it's not the most likely cause of this specific pain pattern.
E. Avascular necrosis (AVN) is rare and typically affects the metatarsal head, leading to joint collapse and accelerated arthritis, not pain under the lesser metatarsals after a successful fusion.
Question 30
A 42-year-old patient undergoes a cheilectomy and Moberg osteotomy for Coughlin and Shurnas Grade 2 hallux rigidus. Which of the following post-operative rehabilitation instructions is most consistent with the goals of this specific procedure, as outlined in the case?
Explanation
Correct Answer: B
The case, under 'Post-Operative Rehabilitation Protocols - Cheilectomy and Moberg Osteotomy,' states: 'These procedures aim to restore and maintain motion, so early mobilization is typically encouraged.' Specifically, for 'Immediately Post-operative (Day 0 - 2 weeks),' it instructs: 'Range of Motion (ROM): Crucial. Initiate immediate, gentle active and passive ROM exercises for the first MTP joint, focusing on dorsiflexion and plantarflexion. Patients are instructed to perform these exercises frequently throughout the day to prevent stiffness and scar tissue formation.'
A. Strict non-weight-bearing in a cast for 6 weeks is typical for arthrodesis, not for cheilectomy/Moberg osteotomy, which allows for weight-bearing as tolerated in a surgical shoe.
C. No active or passive ROM for 12 weeks is contrary to the goal of motion preservation and would lead to stiffness.
D. Gradual progression to weight-bearing after radiographic confirmation of union at 8 weeks is characteristic of arthrodesis protocols, not cheilectomy/Moberg osteotomy, which allows earlier weight-bearing.
E. Avoidance of MTP joint motion for 4 weeks is incorrect; early motion is emphasized to prevent stiffness.
Question 31
A 68-year-old patient with a history of rheumatoid arthritis and severe, painful hallux rigidus (Coughlin and Shurnas Grade 4) is considering surgical options. She expresses a strong desire to preserve some motion in her great toe, if possible, but her primary goal is reliable pain relief. Based on the provided case, which statement accurately reflects the current understanding of motion-preserving arthroplasty options versus arthrodesis for end-stage hallux rigidus?
Explanation
Correct Answer: C
The case, under 'Summary of Key Literature and Guidelines - Arthrodesis,' explicitly states: 'Fusion of the first MTP joint is widely considered the 'gold standard' for end-stage hallux rigidus (Coughlin and Shurnas Grade 4), providing the most reliable and durable pain relief. Fusion rates typically range from 90% to 98%, with high patient satisfaction despite the sacrifice of motion.' This directly addresses the patient's primary goal of reliable pain relief for end-stage disease.
A. The case states regarding metallic hemiarthroplasty: 'Long-term comparative studies against arthrodesis often show superior pain relief and durability for fusion in severe cases.' This contradicts the option.
B. Regarding interposition arthroplasty, the case notes: 'these procedures generally have less predictable outcomes than fusion, with variable rates of pain relief and maintenance of motion.' This contradicts the option.
D. The case states: 'Silicone implants: Largely abandoned due to concerns regarding particulate synovitis and implant failure.' This contradicts the option.
E. The case states regarding cartilage restoration: 'their application in diffuse, advanced hallux rigidus is limited, and long-term data specific to the first MTP joint is still evolving.' This contradicts the option, especially for an older patient with diffuse, end-stage arthritis.
Question 32
A 30-year-old professional dancer presents with a 5-year history of progressive pain and stiffness in her right great toe, significantly impacting her career. She has failed all conservative measures. Radiographs show moderate dorsal osteophytes, mild joint space narrowing, and a focal osteochondral lesion on the metatarsal head, consistent with Coughlin and Shurnas Grade 2-3. She is highly motivated to preserve motion. Based on the case, which surgical approach, potentially combined with cheilectomy, would be most appropriate for this patient?
Explanation
Correct Answer: D
The patient is a young, active professional dancer with a focal osteochondral lesion and a strong desire to preserve motion. The case, under 'Cartilage Restoration Techniques (Microfracture, OATS, MACI),' states: 'Indication: For younger patients with focal cartilage defects (e.g., osteochondral lesions) associated with early hallux rigidus, where the surrounding cartilage is relatively healthy. Not suitable for diffuse, end-stage arthritis.' Given her age, activity level, and the focal nature of the lesion, a cartilage restoration technique combined with cheilectomy (to address the osteophytes) is the most appropriate motion-preserving option.
A. Arthrodesis sacrifices motion and is the gold standard for end-stage (Grade 4) HR, which would be detrimental to a professional dancer.
B. Hemiarthroplasty is for Grade 3-4 HR, typically in older, less active individuals, and has concerns regarding implant loosening and contralateral cartilage wear, making it less ideal for a young, high-demand patient with a focal defect.
C. Interposition arthroplasty is for Grade 3-4 HR, with variable outcomes and concerns about graft durability, and is not specifically indicated for focal lesions in young patients.
E. Resection arthroplasty (Keller procedure) is not mentioned in the case as a recommended procedure for hallux rigidus. It is an older procedure associated with significant shortening and instability, generally considered a salvage procedure and not suitable for a high-demand patient seeking motion preservation.
Question 33
A 52-year-old male undergoes a first MTP joint arthrodesis for severe hallux rigidus. Post-operatively, he is placed in a non-weight-bearing short leg cast. At his 6-week follow-up, weight-bearing radiographs are obtained to assess for bony union. The radiographs show no clear signs of union, and there is a visible gap at the fusion site. Based on the case, what is the most appropriate next step in management?
Explanation
Correct Answer: C
The patient's presentation of no clear signs of union and a visible gap at the fusion site at 6 weeks indicates a delayed union or potential nonunion. The case, under 'Post-Operative Rehabilitation Protocols - Arthrodesis Fusion - Fusion Confirmation Phase (6 - 12 weeks),' states: 'Once radiographic evidence of early union is confirmed, gradual progression to weight-bearing in a removable CAM boot or stiff-soled shoe is initiated. If union is not evident, NWB may be extended.' Furthermore, under 'Complications & Management - Nonunion (Arthrodesis),' it lists 'Management: revision arthrodesis with bone graft (autograft/allograft), stronger internal fixation, extended immobilization.' Therefore, extending non-weight-bearing is the immediate appropriate step, with revision surgery as a consideration if union remains elusive.
A. Transitioning to weight-bearing without signs of union would jeopardize the fusion and likely lead to nonunion.
B. Initiating aggressive physical therapy to improve range of motion is contraindicated for an arthrodesis, as motion is intentionally sacrificed, and it would disrupt the healing fusion site.
D. Oral corticosteroids are generally not used to promote bone healing and can, in fact, impair it. They are not indicated here.
E. Hardware removal is typically performed after healing is complete if the hardware is symptomatic, not as a primary treatment for nonunion at 6 weeks. Hardware is crucial for stability to achieve union.
Question 34
The Lisfranc ligament is a primary stabilizer of the midfoot. Which of the following accurately describes its anatomic origin and insertion?
Explanation
Question 35
A 38-year-old female sustains a purely ligamentous Lisfranc injury. Studies have shown that primary arthrodesis yields superior functional outcomes for this specific injury pattern compared to open reduction internal fixation (ORIF). Which joints are typically included in this primary arthrodesis?
Explanation
Question 36
A 55-year-old male presents with dorsal pain and stiffness in his right great toe. Radiographs demonstrate dorsal osteophytes and mild joint space narrowing at the first metatarsophalangeal (MTP) joint consistent with Grade 2 hallux rigidus. Which of the following shoe modifications is most appropriate for initial conservative management?
Explanation
Question 37
Fibular deficiency (fibular hemimelia) is the most common congenital long bone deficiency. Which of the following associated tibial deformities is classically seen in these patients?
Explanation
Question 38
During surgical stabilization of a severe Lisfranc fracture-dislocation involving all five tarsometatarsal joints, the surgeon places rigid screw fixation across the 1st, 2nd, and 3rd TMT joints. How should the 4th and 5th TMT joints be optimally managed?
Explanation
Question 39
A 62-year-old female with Grade 4 hallux rigidus undergoes a first metatarsophalangeal joint arthrodesis. To optimize her postoperative gait and prevent adjacent joint arthritis, what is the ideal position for the arthrodesis?
Explanation
Question 40
A 2-year-old child with fibular hemimelia is being evaluated for lower extremity reconstruction versus amputation. Along with the fibular absence and limb length discrepancy, which of the following knee ligament anomalies is most commonly associated with this condition?
Explanation
Question 41
In the open reduction and internal fixation of a classic divergent Lisfranc injury, what is the proper sequence of reduction and fixation?
Explanation
Question 42
A 45-year-old runner with early-stage hallux rigidus fails conservative management and elects to undergo a dorsal cheilectomy. What is the primary biomechanical goal of this procedure?
Explanation
Question 43
In a patient with severe congenital fibular deficiency, which of the following clinical findings strongly favors early Syme amputation over attempts at limb lengthening?
Explanation
Question 44
A 24-year-old athlete sustains a midfoot injury. A weight-bearing AP radiograph shows a small bony fragment in the space between the medial cuneiform and the base of the second metatarsal. This "fleck sign" represents an avulsion of the Lisfranc ligament from which structure?
Explanation
Question 45
A 78-year-old low-demand female undergoes a Keller excision arthroplasty for severe hallux rigidus. Postoperatively, she complains of a new deformity of her great toe and pain under the second metatarsal head. Which of the following is the most likely complication responsible for her symptoms?
Explanation
Question 46
In addition to a missing or hypoplastic fibula, patients with fibular hemimelia frequently have specific anomalies of the foot and ankle. Which of the following is most commonly observed in these patients?
Explanation
Question 47
During physical examination of a patient with a suspected subtle midfoot injury, the presence of plantar ecchymosis is noted. This finding is highly specific for an injury to which of the following?
Explanation
Question 48
The Lisfranc ligament is a primary stabilizer of the midfoot. Which of the following best describes its anatomical origin and insertion?
Explanation
Question 49
A 45-year-old male presents with severe midfoot pain after a misstep off a curb. MRI confirms a complete, purely ligamentous rupture of the Lisfranc complex with associated diastasis on weight-bearing films, but no fractures. Based on recent literature, which of the following treatments provides the lowest rate of hardware failure and subsequent revision surgeries for this specific injury pattern?
Explanation
Question 50
A 2-year-old child presents with a foreshortened leg, absent lateral digits, and an anteromedial bow of the tibia. Which of the following knee anomalies is most universally associated with this patient's underlying diagnosis?
Explanation
Question 51
The Lisfranc ligament is a crucial stabilizing structure of the midfoot. Which of the following accurately describes its anatomic origin and insertion?
Explanation
Question 52
A 24-year-old professional athlete sustains a purely ligamentous Lisfranc injury. Weight-bearing radiographs demonstrate 3 mm of diastasis between the first and second metatarsals. What is the most evidence-based surgical management for this specific injury pattern to minimize the need for future reoperation?
Explanation
Question 53
A 55-year-old female presents with Coughlin and Shurnas Grade 2 hallux rigidus. Conservative management has failed, and a cheilectomy is planned. To prevent postoperative iatrogenic instability or dorsal subluxation of the proximal phalanx, resection of the dorsal first metatarsal head should not exceed what percentage?
Explanation
Question 54
Fibular deficiency (fibular hemimelia) is the most common congenital long bone deficiency. When examining a child with this condition, which of the following knee anomalies is most frequently encountered?
Explanation
Question 55
When evaluating a patient for a suspected subtle Lisfranc injury, specific radiographic landmarks must be scrutinized. On a standard AP weight-bearing radiograph of a normal foot, which of the following alignments must be present?
Explanation
Question 56
A 45-year-old male with mild hallux rigidus presents with pain during the terminal stance phase of gait. He wishes to pursue non-operative management. Which of the following orthotic modifications is most appropriate?
Explanation
Question 57
A 10-month-old infant is diagnosed with severe Achterman and Kalamchi Type II fibular hemimelia. The limb length discrepancy is projected to be 22 cm at skeletal maturity. The foot has three rays and is fixed in severe equinovalgus. What is the most appropriate management?
Explanation
Question 58
A 35-year-old female presents with severe midfoot pain after a fall from a horse. Weight-bearing radiographs and a subsequent MRI reveal a purely ligamentous Lisfranc injury with 4 mm of diastasis between the medial cuneiform and the second metatarsal base, without any associated fractures. Which of the following is the most appropriate definitive management to minimize the risk of hardware failure and long-term reoperation?
Explanation
Question 59
A 58-year-old male runner complains of chronic, progressive right great toe pain. On examination, he has significant pain throughout the mid-range of first metatarsophalangeal (MTP) joint motion. Radiographs reveal severe joint space narrowing, subchondral sclerosis, and large dorsal and lateral osteophytes, consistent with Grade 3 hallux rigidus. He has failed shoe modifications and NSAIDs. What is the gold standard surgical treatment for this patient?
Explanation
Question 60
A newborn infant is evaluated for a right lower extremity deformity. Clinical examination reveals a significantly shortened lower leg and a foot with only three toes. Radiographs confirm complete absence of the right fibula. Which of the following associated lower extremity anomalies is most classically expected in this patient?
Explanation
Question 61
During open reduction of a midfoot fracture-dislocation, the surgeon must carefully identify and clear the interval housing the Lisfranc ligament to achieve an anatomic reduction. The primary stabilizing ligament of this complex originates and inserts on which of the following osseous structures?
Explanation
Question 62
A 45-year-old female undergoes a dorsal cheilectomy for Coughlin and Shurnas Grade 2 hallux rigidus. To relieve impingement and adequately increase first MTP joint dorsiflexion without causing joint instability, what is the maximum recommended percentage of the dorsal articular surface of the first metatarsal head that should be resected?
Explanation
Question 63
A 1-year-old male presents with severe fibular hemimelia (Achterman and Kalamchi Type II). Clinical and radiographic assessments project a leg-length discrepancy of 14 cm at skeletal maturity. The foot is rigidly fixed in extreme equinovalgus, possesses only two toes, and articulates via a ball-and-socket ankle joint. What is the most appropriate definitive management strategy for optimizing the child's long-term mobility?
Explanation
Question 64
A 24-year-old male football player sustains an axial loading injury to a plantarflexed foot. Non-weight-bearing radiographs demonstrate no obvious malalignment, but a distinct "fleck sign" is visualized between the medial cuneiform and the base of the second metatarsal. This radiographic finding specifically represents an avulsion of a structure from which of the following anatomic locations?
Explanation
None
