ABOS Part I Orthopaedic Exam: Sacral Fractures, Denis, VTE Prophylaxis, THA | Part 21569

Key Takeaway
Orthopaedic sacral fractures are classified by Denis (Type I-III) based on their anatomical location, directly correlating with neurological injury risk. Management ranges from nonsurgical for stable fractures to surgical fixation for unstable patterns. Critical considerations for sacroiliac screw placement include sacral dysmorphism and precise fluoroscopic views to prevent iatrogenic nerve damage.
ABOS Part I Orthopaedic Exam: Sacral Fractures, Denis, VTE Prophylaxis, THA | Part 21569
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
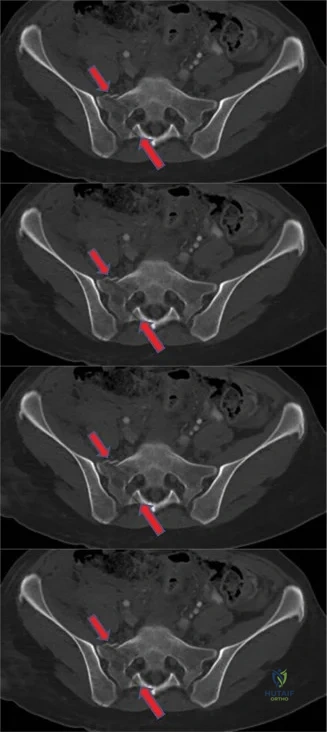
A 24-year-old male presents following a motor vehicle collision with lower back pain. An axial CT scan of his sacrum is shown below. Based on the fracture pattern identified, what is the most likely rate of associated neurological deficit (lower extremity symptoms or bowel/bladder/sexual dysfunction)?
Explanation
Correct Answer: C. Approximately 28%
The image provided is an axial CT scan of the sacrum, which clearly demonstrates a fracture line extending through the right sacral foramen. According to the Denis classification of sacral fractures, a fracture that passes through the sacral foramen is classified as a Denis Type II injury. The case discussion explicitly states that Denis Type II sacral fractures are associated with a 28% rate of neurological injury.
Option A (Less than 5%): This rate is too low. Denis Type I fractures (lateral to the sacral foramen) have a 6% neurological injury rate, which is the lowest among the Denis types.
Option B (Approximately 15%): This rate is not directly associated with any specific Denis type mentioned in the case discussion.
Option D (Approximately 45%): This rate is higher than that for a Denis Type II fracture. Denis Type III fractures (medial to the sacral foramen, involving the central sacral canal) have a 57% neurological injury rate, which is closer to this value but still distinct.
Option E (Greater than 55%): This rate is most consistent with a Denis Type III fracture (57%), which involves the central sacral canal, not the sacral foramen as seen in the image.
Question 2
A 24-year-old male sustains a sacral fracture as depicted in the axial CT scan. Which of the following best describes the Denis classification of this fracture?
Explanation
Correct Answer: B. Denis Type II
The axial CT scan clearly shows a fracture line traversing the sacral foramen on the right side. The Denis classification categorizes sacral fractures based on their relationship to the sacral foramen and central canal:
- Denis Type I: Fractures occurring lateral to the sacral foramen.
- Denis Type II: Fractures passing through the sacral foramen.
- Denis Type III: Fractures involving the central sacral canal, medial to the sacral foramen.
Given the fracture's path through the foramen, it is definitively a Denis Type II fracture.
Option A (Denis Type I): Incorrect, as the fracture is not lateral to the foramen.
Option C (Denis Type III): Incorrect, as the fracture does not involve the central sacral canal medial to the foramen.
Option D (Transverse fracture): Incorrect. Transverse fractures run horizontally across the sacrum and are typically classified by Roy-Camille (e.g., Type I, II, III), not Denis. The image shows a vertical component.
Option E (U-type sacral fracture): Incorrect. A U-type fracture is a highly unstable transverse fracture often associated with spinopelvic dissociation, characterized by bilateral vertical fractures connecting to a transverse component, forming a 'U' or 'H' shape. This is not depicted in the axial image.
Question 3
A 24-year-old male presents with a sacral fracture. Based on the principles discussed in the case, nonsurgical treatment would be considered a reasonable option in all of the following scenarios, EXCEPT which of the following?
Explanation
Correct Answer: C. A neurologically intact patient with a unilateral displaced Denis Type I fracture involving both the ventral and dorsal cortices.
The case discussion states that nonsurgical management is typically reserved for patients with sacral fracture morphology that does not compromise spinopelvic stability. This implies that fractures leading to instability generally require surgical intervention.
- Option A: A nondisplaced transverse fracture below the SI joint (e.g., S4 foramen) is often stable and amenable to conservative treatment, as mentioned in the case discussion.
- Option B: A unilateral nondisplaced Denis Type II fracture involving only the ventral sacral cortex suggests minimal disruption and potential stability, making nonsurgical management a reasonable option, as indicated in the case discussion.
- Option C: A unilateral displaced Denis Type I fracture involving both the ventral and dorsal cortices signifies significant disruption of the sacral ring. Displacement and involvement of both cortices indicate a higher degree of instability, which would typically necessitate surgical stabilization rather than conservative management. This scenario is explicitly listed as an exception to nonsurgical treatment in the case discussion.
- Option D: A neurologically intact elderly patient with bilateral nondisplaced Denis Type II fractures involving only the ventral cortex suggests a relatively stable injury pattern, especially if nondisplaced and only involving one cortex, making conservative treatment a consideration, as mentioned in the case discussion.
- Option E: A minimally displaced Denis Type I fracture without spinopelvic instability is generally considered stable and can often be managed non-surgically. This aligns with the principle of reserving surgery for unstable fractures.
Therefore, a displaced fracture involving both cortices, even if Denis Type I, suggests instability that would typically preclude nonsurgical management.
Question 4
A 24-year-old male with a sacral fracture (as shown in the axial CT) is undergoing percutaneous sacroiliac screw fixation. To minimize the risk of iatrogenic foot drop due to aberrant hardware placement, which intraoperative fluoroscopic view is most critical for assessing the anterior-to-posterior trajectory of the screw?
Explanation
Correct Answer: C. Pelvic inlet view
The case discussion explicitly states that the pelvic inlet view is crucial for visualizing the anterior-to-posterior trajectory of the sacroiliac screw. This view allows the surgeon to monitor the screw's progression and prevent anterior breach, which could injure the lower lumbar nerve roots (specifically L5, which contributes to the peroneal nerve and thus foot dorsiflexion, leading to foot drop) that drape over the ventral surface of the sacral ala.
- Option A (Obturator outlet pelvic view): This view is primarily used to assess the superior-to-inferior trajectory of the screw and ensure it remains within the sacral body, avoiding the greater sciatic notch and sacral foramina. It is less effective for anterior breach.
- Option B (Iliac oblique pelvic view): This view is used to assess the screw's position within the ilium and sacrum in the coronal plane, ensuring it is not too medial or lateral. It does not provide the necessary anterior-to-posterior trajectory assessment.
- Option D (True lateral sacral view): While useful for assessing the overall length and trajectory in the sagittal plane, the inlet view is superior for specifically identifying anterior cortical breach in the axial plane, especially concerning the anterior neurovascular structures.
- Option E (AP pelvic view): The AP view provides a general overview but is insufficient for detailed assessment of screw trajectory in the critical anterior-posterior dimension to prevent anterior breach.
Question 5
A 68-year-old female with osteoporosis presents with a sacral insufficiency fracture. Preoperative planning for potential percutaneous sacroiliac screw fixation includes assessing for sacral dysmorphism. All of the following radiographic findings are indicative of sacral dysmorphism, EXCEPT which of the following?
Explanation
Correct Answer: D. Paradoxical inlet view of the upper sacral segments on the AP or outlet views.
The case discussion explicitly lists several radiographic findings that represent sacral dysmorphism, which are aberrations in sacral osteology that can complicate safe hardware placement. It also identifies one finding that is NOT sacral dysmorphism but rather indicates a different pathology.
- Option A (The sacrum is not recessed within the pelvis on the outlet image): This is listed as a characteristic of sacral dysmorphism.
- Option B (Mammillary processes are seen on the outlet image): This is listed as a characteristic of sacral dysmorphism.
- Option C (A residual disc space between the upper two sacral segments is seen on the outlet image): This is listed as a characteristic of sacral dysmorphism.
- Option D (Paradoxical inlet view of the upper sacral segments on the AP or outlet views): The case discussion states that this finding represents an occult sacral fracture dislocation or a U-type sacral fracture, not sacral dysmorphism. This is a critical distinction for diagnosis and treatment planning.
- Option E ('Tongue-in-groove' SI articulations noted on the CT scan): This is listed as a characteristic of sacral dysmorphism.
Therefore, the paradoxical inlet view indicates a severe traumatic injury pattern (U-type fracture/spinopelvic dissociation) rather than a congenital or developmental variation in sacral anatomy (dysmorphism).
Question 6
A 35-year-old male presents with a sacral fracture that extends medial to the sacral foramen, involving the central sacral canal. According to the Denis classification, what is the expected rate of neurological injury for this fracture pattern?
Explanation
Correct Answer: D. 57%
The question describes a sacral fracture that extends medial to the sacral foramen, involving the central sacral canal. This is the definition of a Denis Type III sacral fracture. The case discussion explicitly states the neurological injury rates for each Denis type:
- Denis Type I (lateral to foramen): 6%
- Denis Type II (through sacral foramen): 28%
- Denis Type III (medial to foramen, involving central canal): 57%
Therefore, a Denis Type III fracture has an associated neurological injury rate of 57%.
Option A (6%): This is the rate for Denis Type I fractures.
Option B (28%): This is the rate for Denis Type II fractures.
Option C (45%): This rate is not directly specified for any Denis type in the provided text.
Option E (75%): This rate is higher than any specified in the provided text for Denis sacral fractures.
Question 7
A 50-year-old male sustains a high-energy pelvic injury, including a sacral fracture. During surgical planning for percutaneous sacroiliac screw fixation, the surgeon is concerned about potential injury to the L5 nerve root. Which of the following anatomical considerations is most relevant to preventing this specific complication?
Explanation
Correct Answer: B. The course of the L5 nerve root draping over the ventral surface of the sacral ala.
The case discussion highlights that the pelvic inlet view helps avoid anterior breach and 'lower lumbar root injury, which drapes over the ventral surface of the sacral ala,' leading to iatrogenic foot drop. Foot drop is typically caused by injury to the peroneal nerve, which receives innervation from the L5 nerve root. Therefore, the L5 nerve root's course over the ventral sacral ala is the most relevant anatomical consideration for preventing iatrogenic foot drop during sacroiliac screw placement.
- Option A (The proximity of the S1 nerve root to the superior aspect of the SI joint): While S1 nerve root injury is a concern with SI screw placement, the question specifically asks about 'foot drop,' which is more directly linked to L5 injury.
- Option C (The location of the superior gluteal artery exiting the greater sciatic notch): Injury to the superior gluteal artery is a known complication of SI screw placement, particularly with posterior breach or screws directed too laterally, but it does not directly cause foot drop.
- Option D (The relationship of the internal iliac artery to the anterior sacrum): The internal iliac artery and its branches are anterior to the sacrum and are at risk with anterior cortical breach, but the L5 nerve root is the primary structure associated with foot drop in this context.
- Option E (The position of the sciatic nerve within the posterior pelvis): The sciatic nerve is a major structure at risk with posterior breach of the sacrum or screws placed too far posteriorly/inferiorly, but the L5 root's vulnerability to anterior breach is specifically linked to the foot drop complication mentioned in the case.
Question 8
A 24-year-old male presents with a sacral fracture, as shown in the axial CT scan. If this patient were to undergo surgical fixation, which of the following fracture characteristics would most strongly indicate the need for surgical stabilization rather than conservative management?
Explanation
Correct Answer: D. A displaced Denis Type I fracture involving both the ventral and dorsal cortices.
The case discussion emphasizes that nonsurgical management is reserved for sacral fracture morphologies that do not compromise spinopelvic stability. Conversely, characteristics that indicate instability would necessitate surgical stabilization.
- Option A (A neurologically intact patient with a nondisplaced transverse fracture at S4): This is explicitly mentioned as a scenario where nonsurgical management is reasonable, indicating stability.
- Option B (A unilateral nondisplaced Denis Type II fracture involving only the ventral cortex): This is also mentioned as a scenario for conservative treatment, implying stability due to lack of displacement and limited cortical involvement.
- Option C (A neurologically intact elderly patient with bilateral nondisplaced Denis Type II fractures involving only the ventral cortex): Similar to option B, nondisplacement and limited cortical involvement suggest stability, making conservative treatment a possibility.
- Option D (A displaced Denis Type I fracture involving both the ventral and dorsal cortices): This scenario is explicitly stated in the case as the exception where nonsurgical treatment is not considered reasonable. Displacement, especially involving both cortices, indicates significant disruption of the sacral ring and compromise of spinopelvic stability, thus requiring surgical intervention.
- Option E (A minimally displaced Denis Type I fracture without spinopelvic instability): Minimally displaced fractures, particularly if stable, are often managed conservatively.
Therefore, a displaced fracture involving both cortices is the strongest indicator for surgical stabilization among the choices provided, as it directly implies instability.
Question 9
A 72-year-old female with severe osteoporosis presents with a sacral insufficiency fracture. During preoperative assessment, a CT scan reveals a 'tongue-in-groove' appearance of the sacroiliac joint. This finding is indicative of which of the following?
Explanation
Correct Answer: C. Sacral dysmorphism, potentially complicating hardware placement.
The case discussion lists '“Tongue-in-groove” SI articulations are noted on the CT scan' as one of the predictable dysplastic patterns that can be easily identified using CT scans and represents sacral dysmorphism. Sacral dysmorphism is a collective term for aberrations in sacral osteology that may preclude safe hardware placement if not recognized preoperatively.
- Option A (Normal age-related degenerative changes of the SI joint): While degenerative changes occur, 'tongue-in-groove' is a specific morphological variation indicative of dysmorphism, not just typical degeneration.
- Option B (An acute traumatic sacroiliac joint dislocation): A dislocation implies a complete loss of articulation, which is different from a 'tongue-in-groove' morphology, although dysmorphism can predispose to instability.
- Option D (A chronic inflammatory arthropathy affecting the SI joint): Inflammatory arthropathies like ankylosing spondylitis cause characteristic erosions, sclerosis, and eventual fusion, which are distinct from a 'tongue-in-groove' appearance.
- Option E (An occult sacral fracture dislocation): While occult fracture dislocations are important to identify, the 'tongue-in-groove' finding itself is a feature of dysmorphism, not a fracture dislocation. A paradoxical inlet view, as mentioned in the case, is indicative of an occult fracture dislocation.
Question 10
A 28-year-old male presents with a high-energy pelvic injury. Radiographs and CT scans confirm a sacral fracture. The surgeon notes that the sacral alar slope appears acute on the lateral view. This finding should alert the surgeon to the possibility of:
Explanation
Correct Answer: C. Sacral dysmorphism, requiring careful preoperative planning for screw placement.
The case discussion lists 'The alar slope is acute on the lateral view' as one of the predictable dysplastic patterns that can be easily identified using plain radiographs and CT scans, falling under the umbrella of sacral dysmorphism. Sacral dysmorphism refers to anatomical variations in the sacrum that can make standard percutaneous sacroiliac screw placement challenging and increase the risk of iatrogenic injury. Recognizing these patterns preoperatively is crucial for safe surgical planning.
- Option A (A stable transverse sacral fracture): An acute alar slope is an anatomical variation, not a direct indicator of fracture stability or type.
- Option B (A Denis Type III sacral fracture with high neurological risk): While Denis Type III fractures have high neurological risk, an acute alar slope is a feature of sacral morphology (dysmorphism), not a specific fracture classification.
- Option D (An isolated sacral avulsion fracture): An avulsion fracture is a specific type of fracture, not related to the general morphology of the sacral alar slope.
- Option E (A chronic stress fracture of the sacrum): A stress fracture is a pathological process, not an anatomical variation like an acute alar slope.
Question 11
A 40-year-old male presents with a complex sacral fracture following a fall from height. The fracture pattern involves bilateral vertical sacral fractures connected by a transverse component, resulting in spinopelvic dissociation. This specific fracture pattern is often associated with which of the following radiographic findings?
Explanation
Correct Answer: D. Paradoxical inlet view of the upper sacral segments on the AP or outlet views.
The question describes a U-type or H-type sacral fracture, which is a severe, unstable injury leading to spinopelvic dissociation. The case discussion explicitly states that a 'Paradoxical inlet view of the upper sacral segments on the AP or outlet views' represents 'occult sacral fracture dislocation or U-type sacral fracture.' This finding is a key radiographic indicator of this highly unstable injury pattern.
- Options A, B, C, and E: These options (mammillary processes, acute alar slope, residual disc space between upper two sacral segments, and 'tongue-in-groove' SI articulations) are all listed in the case discussion as characteristics of sacral dysmorphism. While sacral dysmorphism can complicate surgery and potentially influence fracture patterns, these findings themselves do not represent an acute U-type fracture or spinopelvic dissociation. The paradoxical inlet view is the specific finding linked to this severe injury pattern in the provided text.
Question 12
A 68-year-old male with a history of unprovoked left lower extremity DVT 3 years prior, currently managed with aspirin 81mg daily, is scheduled for an elective right total hip arthroplasty (THA). He has a BMI of 32 kg/m2 and well-controlled hypertension. During preoperative assessment, he expresses concern about VTE recurrence. Based on AAOS guidelines and his risk profile, which of the following statements regarding his VTE risk and prophylaxis is most accurate?

Explanation
Correct Answer: C
The correct answer is C. The case explicitly states that a history of prior DVT or PE is a substantial independent risk factor for recurrent VTE, elevating the relative risk by approximately 2-4 times compared to patients without such history. For such high-risk patients, AAOS guidelines suggest extending pharmacologic prophylaxis up to 35 days postoperatively, and the choice of agent often leans towards more potent options like DOACs or LMWH due to their higher efficacy in preventing recurrent VTE compared to aspirin, especially for initial and extended prophylaxis in this group.
Option A is incorrect because the case states the relative risk increase is 2-4 times, not 1.5 times, and aspirin alone is generally not considered sufficient for primary or secondary prophylaxis in high-risk THA patients with a DVT history, where more potent agents are preferred.
Option B is incorrect because while age and BMI are risk factors, a history of DVT is explicitly highlighted as the 'most significant risk factor requiring augmented or extended prophylaxis' and 'a potent and independent risk factor for recurrent VTE'.
Option D is incorrect because mechanical prophylaxis with IPCs is generally recommended for both limbs postoperatively. While caution is advised for acutely thrombosed limbs, a DVT 3 years prior does not contraindicate IPCs on the unaffected limb intraoperatively and both limbs postoperatively, unless there is active DVT or post-thrombotic syndrome that makes it uncomfortable or ill-fitting. The statement implies a universal contraindication, which is false.
Option E is incorrect because the AAOS does not recommend routine duplex ultrasound screening for asymptomatic DVT following THA. Screening should be reserved for patients with signs or symptoms suggestive of DVT or PE.
Question 13
A 55-year-old female undergoing elective left THA, with a history of right lower extremity DVT 5 years ago, is positioned in the lateral decubitus position. The surgical team is meticulous about padding and alignment. Which of the following intraoperative biomechanical factors is most directly mitigated by careful patient positioning and contributes significantly to VTE risk reduction?

Explanation
Correct Answer: C
The correct answer is C. Careful patient positioning, especially in the lateral decubitus position, is crucial to avoid direct pressure on the dependent leg, which can lead to venous outflow obstruction and significant venous stasis. Prolonged immobility under anesthesia also contributes to stasis. Mitigating these factors directly reduces VTE risk.
Option A is incorrect because systemic hypercoagulability is a physiological response to surgical trauma and is not directly mitigated by patient positioning. It requires pharmacologic intervention.
Option B is incorrect because direct endothelial injury from surgical dissection is related to the surgical technique and tissue handling, not primarily patient positioning.
Option D is incorrect because activation of acute phase reactants is a systemic inflammatory response to surgery, not directly influenced by patient positioning.
Option E is incorrect because reduced fibrinolysis is part of the systemic hypercoagulable state induced by surgery and is not addressed by patient positioning.
Question 14
A 72-year-old male with a history of Factor V Leiden mutation and a prior unprovoked PE 2 years ago, now on chronic apixaban, is scheduled for elective right THA. His creatinine clearance is 45 mL/min. Which of the following is an absolute contraindication to continuing his current pharmacologic VTE prophylaxis strategy perioperatively?

Explanation
Correct Answer: D
The correct answer is D. Severe thrombocytopenia (platelets < 50,000/µL) is listed as an absolute contraindication to pharmacologic prophylaxis due to the unacceptably high risk of bleeding. A platelet count of 40,000/µL falls into this category.
Option A is incorrect because advanced age (>60-70 years) is a risk factor for VTE, not a contraindication to prophylaxis. In fact, it often warrants intensified prophylaxis.
Option B is incorrect because moderate renal impairment (CrCl 45 mL/min) is a relative contraindication or requires dose adjustment for renally cleared anticoagulants like apixaban, but it is not an absolute contraindication to all pharmacologic prophylaxis. Apixaban typically requires dose adjustment for CrCl < 30 mL/min, but 45 mL/min might still allow for a reduced dose or a different agent.
Option C is incorrect because neuraxial anesthesia is a relative contraindication, requiring careful timing considerations for anticoagulant administration to minimize spinal epidural hematoma risk, but it is not an absolute contraindication to pharmacologic prophylaxis itself.
Option E is incorrect because a history of Factor V Leiden mutation is a strong indication for VTE prophylaxis, especially in a patient with a prior PE, not a contraindication.
Question 15
A 62-year-old patient with a history of provoked DVT 4 years ago (due to prolonged immobilization after a tibia fracture) is undergoing elective THA. Preoperative labs are normal, and he is not on chronic anticoagulation. The surgeon plans to use LMWH for VTE prophylaxis. According to AAOS guidelines, what is the recommended minimum duration for pharmacologic prophylaxis in this patient?

Explanation
Correct Answer: B
The correct answer is B. The AAOS strongly recommends continuing pharmacologic prophylaxis for a minimum of 10-14 days postoperatively for most THA patients. For high-risk patients, including those with a history of DVT, the AAOS suggests extending pharmacologic prophylaxis up to 35 days postoperatively. Therefore, 10-14 days is the minimum recommended duration, with a strong consideration for extension up to 35 days given his DVT history.
Option A is incorrect as it is too short. The risk of VTE extends beyond the immediate hospital stay.
Option C is incorrect as 6 weeks is not the standard minimum or suggested extended duration by AAOS; 35 days (approximately 5 weeks) is the suggested extended duration.
Option D is incorrect as this duration is far too short and would not provide adequate protection against VTE.
Option E is incorrect because indefinite prophylaxis is typically reserved for patients with recurrent unprovoked VTE or very high-risk thrombophilias, not a single provoked DVT 4 years ago in the context of THA prophylaxis.
Question 16
A 48-year-old male with a history of unprovoked DVT 1 year prior, currently on warfarin for secondary prevention, is scheduled for elective THA. His target INR is 2.5. The surgical team plans for perioperative bridging. Which of the following is the most appropriate bridging strategy for this patient?

Explanation
Correct Answer: B
The correct answer is B. For patients on chronic warfarin requiring surgery, a typical bridging strategy involves discontinuing warfarin approximately 5 days preoperatively to allow the INR to normalize. LMWH is then initiated (e.g., 3 days preoperatively) and stopped 12-24 hours before surgery (depending on the LMWH dose and patient bleeding risk). Postoperatively, LMWH is resumed once hemostasis is achieved and bleeding risk is acceptable, and warfarin is restarted. LMWH is continued until the INR is therapeutic (typically 2-3 days after warfarin restart).
Option A is incorrect because discontinuing warfarin only 1 day preoperatively is insufficient for INR normalization, and starting LMWH so close to surgery and stopping it 6 hours preoperatively is not a standard, safe bridging protocol.
Option C is incorrect because continuing warfarin perioperatively significantly increases the risk of major bleeding during and after THA, especially with an INR of 2.5.
Option D is incorrect because switching to aspirin is insufficient for a patient on chronic warfarin for secondary prevention of unprovoked DVT, especially given his high VTE risk.
Option E is incorrect because discontinuing warfarin 2 days preoperatively might be too short, and starting DOACs postoperatively without proper bridging (e.g., with LMWH) would leave a significant period of inadequate anticoagulation, especially for a high-risk patient.
Question 17
During an elective THA on a patient with a history of DVT, the surgeon inadvertently causes a small tear in the profunda femoris vein during acetabular preparation. The tear is successfully repaired with fine sutures. What is the most appropriate immediate postoperative VTE prophylaxis adjustment or consideration for this patient?

Explanation
Correct Answer: C
The correct answer is C. Inadvertent venous injury, even if repaired, creates localized endothelial trauma and increases the risk of intraluminal thrombus formation. For a patient already at high risk due to DVT history, this event further elevates localized DVT risk. Therefore, proceeding with robust pharmacologic prophylaxis (LMWH/DOAC for 35 days as per AAOS suggestions for high-risk patients) is appropriate, carefully balancing the bleeding risk from the repair. Additionally, imaging surveillance (e.g., duplex ultrasound) of the affected limb may be warranted to monitor for DVT development at the site of injury.
Option A is incorrect because discontinuing all prophylaxis would leave a high-risk patient unprotected, especially after a direct venous injury. The bleeding risk from a small, successfully repaired tear needs to be weighed against the VTE risk, but usually, prophylaxis is continued.
Option B is incorrect because initiating therapeutic anticoagulation immediately postoperatively is too aggressive and carries a very high risk of bleeding, especially at the surgical site and the venous repair. Prophylactic dosing is the standard.
Option D is incorrect because switching to aspirin from a more potent agent like LMWH would be a downgrade in efficacy, which is inappropriate for a patient with heightened VTE risk due to DVT history and intraoperative venous injury.
Option E is incorrect because a prophylactic IVC filter is not indicated for a successfully repaired venous injury. IVC filters are reserved for patients with acute proximal DVT or PE who have absolute contraindications to anticoagulation or recurrent VTE despite adequate anticoagulation; they are not a primary prophylactic measure.
Question 18
A 65-year-old female with a history of unprovoked DVT 2 years ago, now on apixaban 5mg BID, is scheduled for elective THA. Her preoperative labs are within normal limits, including a platelet count of 250,000/µL and CrCl of 70 mL/min. She is instructed to hold apixaban for 3 days prior to surgery. Postoperatively, on Day 1, she develops sudden onset dyspnea, pleuritic chest pain, and tachycardia. A CT pulmonary angiography (CTPA) confirms a subsegmental pulmonary embolism. Which of the following is the most appropriate immediate management step?

Explanation
Correct Answer: B
The correct answer is B. For a confirmed pulmonary embolism (PE), immediate therapeutic anticoagulation is the cornerstone of management. LMWH or unfractionated heparin is typically initiated promptly, followed by a transition to DOACs or warfarin. This patient is hemodynamically stable (no mention of hypotension or shock), so thrombolysis or embolectomy are not first-line.
Option A is incorrect because aspirin is not therapeutic for an acute PE and would be insufficient.
Option C is incorrect because while a DVT is often the source of a PE, the diagnosis of PE is already confirmed by CTPA. The priority is to treat the PE, not to delay by looking for the source, unless there's a specific clinical reason (e.g., considering IVC filter if anticoagulation is contraindicated).
Option D is incorrect because surgical embolectomy is reserved for massive PE in patients with contraindications to thrombolysis or failed thrombolysis, not for a subsegmental PE in a hemodynamically stable patient.
Option E is incorrect because systemic thrombolysis is indicated for massive PE with hemodynamic instability (hypotension, shock), which is not described in this stable patient with a subsegmental PE.
Question 19
A 70-year-old male with a history of recurrent DVT and known Antithrombin III deficiency is undergoing elective THA. He is receiving LMWH for VTE prophylaxis. On postoperative day 5, his platelet count drops from 220,000/µL preoperatively to 80,000/µL, and he develops new ecchymoses at injection sites. His surgical wound is clean. What is the most likely diagnosis and appropriate initial management?

Explanation
Correct Answer: C
The correct answer is C. The clinical picture of a significant drop in platelet count (from 220,000 to 80,000, a >50% drop) occurring 5 days after starting LMWH, coupled with new thrombotic manifestations (ecchymoses, which can be a sign of paradoxical thrombosis in HIT), is highly suggestive of Heparin-Induced Thrombocytopenia (HIT). HIT is a rare but severe immune-mediated complication of heparin exposure, leading to paradoxical thrombosis. The immediate management is to discontinue all heparin products (including LMWH) and initiate an alternative non-heparin anticoagulant (e.g., argatroban, bivalirudin).
Option A is incorrect because while bleeding is present, the significant drop in platelets points to a systemic issue beyond simple surgical site bleeding. Vitamin K and FFP are not indicated for HIT.
Option B is incorrect because continuing LMWH in suspected HIT is dangerous and can lead to severe thrombotic events. The platelet drop is too significant to simply monitor.
Option D is incorrect because while DIC can cause thrombocytopenia and bleeding, the specific context of heparin exposure and the timing of the platelet drop strongly point to HIT. DIC would typically present with more widespread bleeding and organ dysfunction, and its management differs.
Option E is incorrect because while anemia might be present due to bleeding, it doesn't explain the acute, significant drop in platelet count or the underlying pathology. Transfusing PRBCs addresses a symptom, not the cause.
Question 20
A 58-year-old female with a history of unprovoked DVT 3 years prior, currently not on anticoagulation, is scheduled for elective THA. She has no other significant comorbidities. During preoperative counseling, she expresses a strong preference for aspirin due to a fear of injections and concerns about bleeding with stronger anticoagulants. Based on AAOS guidelines and shared decision-making, which of the following is the most appropriate recommendation?

Explanation
Correct Answer: C
The correct answer is C. The AAOS strongly recommends shared decision-making, which involves discussing individual VTE and bleeding risks, the rationale for specific prophylaxis choices, and potential side effects, allowing patients to make informed choices. While LMWH or DOACs are generally favored for their higher efficacy in high-risk patients with a DVT history, the AAOS guidelines suggest that aspirin may be considered for VTE prophylaxis after THA, particularly when combined with mechanical prophylaxis. For a patient with a strong preference and concerns, a thorough discussion acknowledging aspirin as a potential, albeit less potent, option (especially with extended duration and mechanical adjuncts) aligns with shared decision-making principles, provided the patient fully understands the comparative risks and benefits.
Option A is incorrect because while LMWH/DOACs are preferred, 'insisting' goes against shared decision-making, and aspirin is not absolutely contraindicated by AAOS, though its efficacy in this specific high-risk group is lower.
Option B is incorrect because while respecting preference, prescribing aspirin as sole prophylaxis for only 10-14 days in a high-risk patient with DVT history might be suboptimal. Extended duration and mechanical prophylaxis would still be important considerations.
Option D is incorrect because aspirin is not absolutely contraindicated by AAOS guidelines for THA prophylaxis, though its role in high-risk patients is debated and often considered less efficacious than other agents.
Option E is incorrect because a prophylactic IVC filter is not a primary VTE prophylaxis strategy and is reserved for specific indications (acute VTE with contraindication to anticoagulation or recurrent VTE despite adequate anticoagulation), not to avoid medication risks in a patient without acute VTE.
Question 21
A 60-year-old male with a history of left lower extremity DVT 10 years ago, now fully resolved and not on chronic anticoagulation, is undergoing elective right THA. He is obese (BMI 35 kg/m2). Which of the following non-pharmacologic strategies is most effective and universally recommended by AAOS for VTE prevention in this patient?

Explanation
Correct Answer: B
The correct answer is B. Early and progressive ambulation, starting as soon as medically stable (postoperative day 0 or 1), is a cornerstone of mechanical VTE prophylaxis. It reactivates the calf muscle pump, improves venous return, and is universally recommended by AAOS in conjunction with pharmacologic agents or as a primary mechanical strategy.
Option A is incorrect because while GCS have been used, the AAOS CPGs generally indicate that GCS alone are less effective than other methods and do not typically recommend them as primary VTE prophylaxis for THA. IPCs/SCDs are preferred mechanical methods.
Option C is incorrect because the AAOS does not recommend routine duplex ultrasound screening for asymptomatic DVT following THA. Screening should be reserved for patients with signs or symptoms suggestive of DVT or PE.
Option D is incorrect because an IVC filter is not a primary prophylactic measure and is reserved for specific indications (acute VTE with contraindication to anticoagulation or recurrent VTE despite adequate anticoagulation), not for general VTE prevention in a patient without acute VTE.
Option E is incorrect because avoiding lower extremity exercises would promote venous stasis and increase VTE risk. Ankle pumps, foot circles, and early ambulation are crucial for VTE prevention.
Question 22
A 45-year-old female with a history of unprovoked DVT 6 months prior, currently on rivaroxaban, is scheduled for elective THA. She has no other significant medical history. During the preoperative assessment, the surgeon discusses the optimal VTE prophylaxis strategy. Which of the following AAOS recommendations is most pertinent to her case regarding the choice and duration of pharmacologic prophylaxis?

Explanation
Correct Answer: B
The correct answer is B. The patient has a history of unprovoked DVT, which is a significant risk factor for recurrent VTE. The AAOS guidelines suggest extending pharmacologic prophylaxis up to 35 days postoperatively for high-risk patients. LMWH or DOACs (like rivaroxaban, which she is already on) are generally favored for their efficacy in preventing recurrent VTE in this population.
Option A is incorrect because aspirin is generally considered less efficacious than LMWH or DOACs for high-risk patients with a DVT history, especially for initial and extended prophylaxis. Her DVT being recent further emphasizes the need for potent prophylaxis.
Option C is incorrect because discontinuing prophylaxis immediately post-surgery would leave a high-risk patient vulnerable to VTE, which is contrary to AAOS recommendations for THA.
Option D is incorrect because mechanical prophylaxis is generally used in conjunction with pharmacologic agents, not as the sole method, especially in high-risk patients, unless pharmacologic agents are strictly contraindicated.
Option E is incorrect because while warfarin is effective, it requires regular INR monitoring, making it less convenient than DOACs for many patients, especially for extended prophylaxis. DOACs are also considered preferred agents.
Question 23
A 50-year-old male with a history of severe uncontrolled hypertension (BP 210/115 mmHg) and a prior DVT 2 years ago is scheduled for elective THA. His surgical team is reviewing his VTE prophylaxis plan. Which of the following statements accurately reflects the AAOS guidelines regarding his hypertension and VTE prophylaxis?

Explanation
Correct Answer: B
The correct answer is B. Severe uncontrolled hypertension (e.g., > 200/110 mmHg) is listed as a relative contraindication to pharmacologic prophylaxis. This means it requires careful risk-benefit analysis, shared decision-making, and potentially mechanical-only prophylaxis initially until the blood pressure is better controlled, due to the increased risk of hemorrhagic complications with anticoagulants.
Option A is incorrect because it is a relative, not absolute, contraindication. Mechanical prophylaxis would still be indicated.
Option C is incorrect because while DVT history is a major factor, bleeding risk factors like uncontrolled hypertension must be carefully considered when selecting and initiating pharmacologic prophylaxis.
Option D is incorrect because initiating pharmacologic prophylaxis with severe uncontrolled hypertension significantly increases the risk of major bleeding, including intracranial hemorrhage. Hypertension should ideally be controlled preoperatively.
Option E is incorrect because while aspirin might have a lower bleeding risk profile than some stronger anticoagulants, any pharmacologic agent carries increased risk in the setting of severe uncontrolled hypertension. It is not inherently the 'safest' without addressing the underlying hypertension.
Question 24
A 35-year-old male is involved in a high-speed motor vehicle collision. CT imaging demonstrates a sacral fracture extending medial to the sacral foramina. What is the most likely neurological complication associated with this specific fracture pattern?
Explanation
Question 25
Which of the following best describes the anatomical location and corresponding neurological risk of a Denis Zone I sacral fracture?
Explanation
Question 26
A patient sustains a U-type sacral fracture following a fall from height. Which of the following statements is true regarding this injury pattern?
Explanation
Question 27
According to the American Academy of Orthopaedic Surgeons (AAOS) guidelines, which of the following is an acceptable strategy for venous thromboembolism (VTE) prophylaxis in a standard-risk patient undergoing elective total hip arthroplasty (THA)?
Explanation
Question 28
A 42-year-old male sustains a pelvic ring injury with a sacral fracture passing vertically through the sacral foramina. If the patient develops a neurological deficit, which of the following is the most likely clinical presentation?
Explanation
Question 29
A 29-year-old female presents with severe back pain after a high-energy fall. A CT scan of her pelvis is obtained.
If this imaging demonstrates a fracture extending through the central sacral canal, which classification and treatment principle apply?
Explanation
Question 30
A 33-year-old male undergoes surgical fixation of a complex sacral fracture and associated pelvic ring injury. When is the optimal time to initiate pharmacological VTE prophylaxis postoperatively, assuming no ongoing hemorrhage?
Explanation
Question 31
A 65-year-old male with a history of a provoked deep vein thrombosis (DVT) 5 years ago is scheduled for a total hip arthroplasty (THA). According to major consensus guidelines, what is the most appropriate VTE prophylaxis regimen?
Explanation
Question 32
A 55-year-old female sustains a transverse sacral fracture at the S4 level following a slip and fall. She has normal sphincter tone and no lower extremity neurological deficits. What is the most appropriate initial management?
Explanation
Question 33
A patient with an unstable Denis Zone I sacral fracture with cranial displacement of the alar fragment presents with a new neurological deficit. Which physical examination finding is most consistent with the injured nerve root?
Explanation
Question 34
When performing lumbopelvic fixation for spinopelvic dissociation (U-type sacral fracture), what biomechanical principle is primarily being utilized to restore stability?
Explanation
Question 35
A 72-year-old female with osteoporosis presents with severe lower back and gluteal pain without a specific traumatic event. Plain radiographs of the pelvis and lumbar spine are unremarkable. What is the most sensitive imaging modality to confirm the suspected diagnosis?
Explanation
Question 36
According to the American College of Chest Physicians (ACCP) guidelines, what is the recommended duration of pharmacological VTE prophylaxis following a routine total hip arthroplasty (THA)?
Explanation
Question 37
While VTE rates are similar across total hip arthroplasty (THA) approaches, the direct anterior approach carries a unique risk of injury to which of the following structures?
Explanation
Question 38
A 30-year-old male treated non-operatively for a displaced Denis Zone II sacral fracture develops severe, intractable neurogenic pain in the lower extremity 6 months post-injury. What is the most likely cause?
Explanation
Question 39
A 35-year-old male sustains a severe pelvic crush injury. CT imaging reveals a sacral fracture extending medial to the sacral foramina into the central spinal canal. According to the Denis classification, what is the approximate rate of neurological deficit associated with this specific fracture zone?
Explanation
Question 40
Which of the following best describes the anatomic location and the most common neurological injury associated with a Denis Zone II sacral fracture?
Explanation
Question 41
A 28-year-old female presents with an isolated Denis Zone I sacral fracture after a fall from a height. Despite the fracture being lateral to the foramina, she exhibits weakness in ankle dorsiflexion and great toe extension. What is the most likely cause of her neurological deficit?
Explanation
Question 42
A 40-year-old male is involved in a motorcycle accident and sustains a U-shaped sacral fracture. Clinical examination demonstrates saddle anesthesia and loss of rectal tone. Which of the following is the most appropriate definitive surgical management?
Explanation
Question 43
A 45-year-old male sustains a pelvic ring injury necessitating operative fixation. When evaluating the pelvis for percutaneous iliosacral screw placement, the surgeon notes sacral dysmorphism. Which of the following radiographic features is indicative of a dysmorphic sacrum?
Explanation
Question 44
According to the American Academy of Orthopaedic Surgeons (AAOS) clinical practice guidelines, which of the following is an acceptable and highly recommended venous thromboembolism (VTE) prophylaxis regimen for a standard-risk patient undergoing an elective total hip arthroplasty?
Explanation
Question 45
A 65-year-old female with a known history of Factor V Leiden and a prior unprovoked deep vein thrombosis is scheduled for a total hip arthroplasty. According to current guidelines, what is the most appropriate VTE prophylaxis strategy for this patient postoperatively?
Explanation
Question 46
A patient undergoing total hip arthroplasty is started on Warfarin for VTE prophylaxis due to a documented allergy to low-molecular-weight heparin. Warfarin exerts its anticoagulant effect by inhibiting the gamma-carboxylation of which of the following coagulation factors?
Explanation
Question 47
Rivaroxaban is frequently utilized for chemical VTE prophylaxis following total hip arthroplasty. What is the specific mechanism of action of this medication?
Explanation
Question 48
The Denis classification of sacral fractures categorizes injuries based on their anatomic location. What anatomical landmark is used to separate the sacrum into three distinct zones in this classification system?
Explanation
Question 49
A 34-year-old male sustains a severe pelvic crush injury. Radiographs and a CT scan reveal a sacral fracture extending medial to the sacral neuroforamina, involving the central sacral canal. According to the Denis classification, what is the approximate rate of neurologic deficit associated with this specific zone?
Explanation
Question 50
A 28-year-old female presents after a fall from a height with a Denis Zone I sacral fracture. During physical examination, she demonstrates new-onset weakness in great toe extension and decreased sensation over the dorsal aspect of her foot. Which nerve root is most likely injured?
Explanation
Question 51
A 45-year-old construction worker falls from a roof, landing squarely on his buttocks. Imaging reveals a transverse fracture through the S1-S2 bodies that communicates with bilateral longitudinal fractures through the sacral foramina. What is the most appropriate definitive surgical management for this injury?
Explanation
Question 52
A patient with standard risk factors is scheduled for an elective primary total hip arthroplasty (THA). According to the clinical practice guidelines from the American Academy of Orthopaedic Surgeons (AAOS), which of the following is an acceptable routine pharmacologic agent for the prevention of venous thromboembolism (VTE)?
Explanation
Question 53
A 68-year-old female is preparing for an elective total hip arthroplasty. She has a history of a pulmonary embolism 3 years ago following a general surgical procedure. Which of the following VTE prophylaxis strategies is most appropriate for this high-risk patient?
Explanation
Question 54
A 72-year-old male with a history of atrial fibrillation is chronically managed with apixaban. He is scheduled to undergo an elective total hip arthroplasty. Assuming normal renal function, when should his apixaban be discontinued prior to surgery?
Explanation
Question 55
A 65-year-old patient undergoing a total hip arthroplasty receives intravenous tranexamic acid (TXA) at the beginning and end of the procedure. Which of the following statements regarding the relationship between TXA and venous thromboembolism (VTE) in total joint arthroplasty is true?
Explanation
Question 56
During the placement of a percutaneous S1 iliosacral screw for a sacral fracture, the surgeon inadvertently breaches the anterior cortex of the sacral ala. Which anatomic structure is at greatest immediate risk of injury?
Explanation
Question 57
A 55-year-old female with a heavily fused lumbar spine extending to the sacrum (L2-Pelvis) presents for a total hip arthroplasty due to severe osteoarthritis. Due to her lumbopelvic stiffness, she is at a significantly increased risk for which of the following postoperative complications?
Explanation
Question 58
Which of the following radiographic findings is classically associated with sacral dysmorphism, necessitating extreme caution or altered trajectories when placing percutaneous iliosacral screws?
Explanation
Question 59
A 40-year-old trauma patient has a vertically unstable pelvic ring injury with a sacral fracture. Which specific plain radiograph is most critical for assessing the vertical translation of the hemipelvis and evaluating the shape of the sacral foramina?
Explanation
Question 60
A 75-year-old male sustains an intertrochanteric hip fracture requiring urgent surgical intervention. He is on chronic warfarin therapy with an admission INR of 3.8. What is the most appropriate and rapid reversal agent to administer to expedite safe surgery?
Explanation
Question 61
A patient with severe hemophilia A requires an elective total hip arthroplasty. Due to the exceptionally high risk of perioperative bleeding, pharmacologic VTE prophylaxis is contraindicated. What is the standard of care for VTE prophylaxis in this specific scenario?
Explanation
Question 62
A 25-year-old male sustains a sacral fracture following a motor vehicle collision.
Imaging confirms the fracture passes completely through the sacral neuroforamina but does not involve the central canal. Which of the following is the most likely clinical presentation of a neurologic deficit in this patient?
Explanation
Question 63
According to the American College of Chest Physicians (ACCP) guidelines, for a patient undergoing total hip arthroplasty, what is the recommended optimal duration of extended pharmacologic VTE prophylaxis?
Explanation
Question 64
A patient presents with a malunited Denis Zone III sacral fracture that occurred 10 years ago, resulting in significant, fixed pelvic obliquity. He now requires a total hip arthroplasty (THA) for severe secondary osteoarthritis. How does this fixed pelvic deformity most critically impact THA surgical technique?
Explanation
Question 65
A 60-year-old female is 4 days post-op from a total hip arthroplasty. She complains of sudden onset pleuritic chest pain, dyspnea, and tachycardia. Oxygen saturation is 88% on room air. What is the most appropriate initial diagnostic imaging study to evaluate her symptoms?
Explanation
Question 66
A 40-year-old male sustains a severe pelvic fracture with spino-pelvic dissociation. You plan to perform lumbopelvic fixation. Which biomechanical advantage does lumbopelvic fixation provide over standard iliosacral screws in this specific fracture pattern?
Explanation
Question 67
Which radiographic view provides the best assessment of the anterior-posterior translation of the sacrum and is critical for evaluating the AP diameter of the sacral canal in suspected Denis Zone III fractures?
Explanation
Question 68
A 32-year-old male sustains a severe crush injury to the pelvis. CT scan demonstrates a sacral fracture involving the central spinal canal. According to the Denis classification, what is the most likely neurologic deficit associated with this injury?
Explanation
Question 69
A 45-year-old female presents after a high-speed MVC. Imaging shows a vertical fracture through the sacral ala lateral to the neural foramina. If the patient exhibits a neurologic deficit, which of the following is most likely expected?
Explanation
Question 70
A 28-year-old male sustains a sacral fracture following a fall. Assuming the image depicts a transforaminal fracture, what is the reported incidence of associated neurological injury according to the Denis classification?
Explanation
Question 71
According to recent ACCP and AAOS guidelines, which of the following regimens is deemed acceptable and non-inferior for VTE prophylaxis in a standard-risk patient undergoing an elective primary total hip arthroplasty (THA)?
Explanation
Question 72
A 65-year-old male undergoes a routine, uncomplicated total hip arthroplasty. According to the American College of Chest Physicians (ACCP), what is the recommended minimum duration for pharmacologic venous thromboembolism (VTE) prophylaxis?
Explanation
Question 73
A 35-year-old construction worker falls from a height of 20 feet. Imaging reveals a transverse fracture through the upper sacral segments communicating with bilateral transforaminal vertical fractures. What is the classic radiographic sign seen on an AP pelvis radiograph for this injury?
Explanation
Question 74
During percutaneous placement of an iliosacral screw for a sacral fracture, intraoperative fluoroscopy is utilized. Which fluoroscopic view is most critical for assessing the anteroposterior position of the screw within the sacral body to avoid injury to the iliac vessels?
Explanation
Question 75
When placing an iliosacral screw into the S1 vertebral body, the pelvic outlet view is primarily used to evaluate which of the following?
Explanation
Question 76
A 42-year-old male polytrauma patient sustains an unstable pelvic ring injury including a displaced Zone II sacral fracture. He has no intracranial hemorrhage or solid organ injury. What is the preferred initial pharmacologic VTE prophylaxis in this patient once he is hemodynamically stable?
Explanation
Question 77
Which of the following sacral fracture patterns is the strongest indication for triangular osteosynthesis (lumbopelvic fixation combined with iliosacral screws) rather than isolated iliosacral screw fixation?
Explanation
Question 78
A 28-year-old female slips and falls on her buttocks. Radiographs and CT show an isolated transverse fracture of the sacrum at the level of S4. Neurological examination reveals intact bowel and bladder function. What is the most appropriate management?
Explanation
Question 79
A patient presents with a Denis Zone III sacral fracture and a new-onset loss of anal sphincter tone and saddle anesthesia. Decompression of the sacral nerve roots is being considered. Which of the following is true regarding sacral neurologic deficits in this setting?
Explanation
Question 80
A 40-year-old male sustains a severely displaced sacral fracture and a subarachnoid hemorrhage following a motorcycle collision. Regarding VTE prophylaxis for this patient on hospital day 1, which of the following is the most appropriate management?
Explanation
Question 81
A surgeon is performing an open reduction and sacral laminectomy for a patient with a Denis Zone III sacral fracture and cauda equina syndrome. During the posterior approach, the surgeon must be careful to avoid extensive lateral dissection past the sacral foramina primarily to prevent injury to which structures?
Explanation
Question 82
A 72-year-old female undergoes a primary THA and is discharged on Apixaban for VTE prophylaxis. Two weeks later, she presents with severe hip pain, swelling, and persistent wound drainage. Aseptic loosening is ruled out. What is the most likely complication driving her current presentation?
Explanation
Question 83
Which of the following statements is most accurate regarding Denis Zone I sacral fractures?
Explanation
Question 84
A 25-year-old male with a severe Denis Zone 2 sacral fracture and an anterior-posterior compression (APC) pelvic ring injury presents in hemorrhagic shock. A pelvic binder is applied. What is the primary source of life-threatening bleeding in this specific injury pattern?
Explanation
None
