ABOS Part I & OITE Orthopaedic Trauma & Lower Extremity Review Questions | Part 21571
Key Takeaway
The page offers advanced multiple-choice questions for ABOS Part I and AAOS OITE exams. It covers high-yield clinical cases in orthopaedic trauma, including complex foot & ankle injuries like subtalar dislocations and severe lower extremity trauma such as Gustilo-Anderson Type IIIC open tibia fractures, focusing on diagnosis, emergent management, and limb salvage strategies.
ABOS Part I & OITE Orthopaedic Trauma & Lower Extremity Review Questions | Part 21571
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old male presents to the Emergency Department following a high-energy motor vehicle accident. He reports immediate pain and deformity in his left foot after an axial load through a plantarflexed foot with a severe inversion component. Clinical examination reveals an 'acquired clubfoot' deformity with significant varus angulation of the hindfoot, supination, plantarflexion, and a prominently palpable talar head dorsolaterally. The skin overlying the talar head is stretched and blanched. Based on this presentation, what is the most likely diagnosis?
Explanation
Correct Answer: C
The patient's presentation is classic for a medial subtalar dislocation. The mechanism of injury (axial load through a plantarflexed foot with severe inversion) directly correlates with the pathomechanics of this injury. Clinically, the 'acquired clubfoot' deformity, significant varus angulation of the hindfoot, supination, plantarflexion, and the prominent dorsolateral talar head are pathognomonic findings for a medial subtalar dislocation. The skin tension over the talar head is a critical sign of impending soft tissue compromise. Lateral subtalar dislocations present with the foot in valgus and pronation, and the talar head prominent medially. Talar neck fractures involve a fracture line through the talar neck, often with variable hindfoot deformity. Chopart joint dislocations involve disarticulation at the talonavicular and calcaneocuboid joints, with an intact subtalar joint. Pantalar dislocations involve simultaneous dislocation of the tibiotalar, subtalar, and talonavicular joints, which is a much more severe and unstable injury.
Question 2
Following the initial clinical assessment, emergent plain radiographs of the left foot and ankle were obtained. The lateral view is provided below. Based on the provided image and the case description, which of the following radiographic findings is most characteristic of this patient's injury?
Explanation
Correct Answer: C
The provided image and case description confirm a medial subtalar dislocation. In this injury, the talus remains perfectly congruent with the distal tibia within the ankle mortise, ruling out option A. The anteroposterior view (described in the text, though not shown) would confirm the navicular resting medial to the talar head, not laterally, ruling out option B. The text explicitly states that 'The calcaneus was displaced medially and anteriorly relative to the talus,' which is a hallmark of a medial subtalar dislocation. The ankle views demonstrated no concomitant tibiotalar subluxation, widening of the syndesmosis (ruling out D), or obvious malleolar fractures (ruling out E). The image clearly shows the talus articulating with the tibia, but disarticulated from the calcaneus and navicular, with the foot (including calcaneus and navicular) displaced relative to the talus.
Question 3
The patient's clinical examination reveals a marked deformity with the skin overlying the dorsolateral talar head appearing stretched and displaying focal pallor, indicating early signs of impending necrosis. Despite strong dorsalis pedis and posterior tibial pulses, the soft tissue envelope integrity is severely compromised. What is the most urgent management priority for this patient?
Explanation
Correct Answer: C
The most urgent management priority for a subtalar dislocation with compromised skin integrity is emergent closed reduction. The case explicitly states, 'The prominent talar head places the overlying skin at imminent risk of pressure necrosis. Therefore, emergent closed reduction is the absolute first step in the surgical decision-making algorithm. Delaying reduction to obtain advanced imaging or waiting for optimal operating room availability is contraindicated if the skin is blanching or tented.' While a CT scan is mandatory post-reduction, it should not delay the immediate reduction. Antibiotics are not indicated for a closed injury unless there is an open wound. Open reduction is reserved for irreducible dislocations after failed closed attempts. Prophylactic fasciotomy is not indicated in the absence of compartment syndrome, and vascular status is currently excellent.
Question 4
During an attempt at closed reduction for this patient's medial subtalar dislocation in the emergency department, the orthopedic resident is struggling to achieve reduction despite adequate sedation and longitudinal traction. Which specific maneuver is highlighted in the case as critical for successful reduction by addressing a common impediment?
Explanation
Correct Answer: C
The case explicitly states under 'Clinical Pearls and Pitfalls': 'Pearl Knee Flexion is Mandatory: The most common reason for a failed closed reduction in the emergency department is inadequate relaxation of the gastrocnemius-soleus complex. Always flex the knee to 90 degrees during the reduction maneuver to eliminate this massive deforming force.' This relaxation is crucial for allowing the calcaneus to be manipulated effectively. Options A and B describe incorrect or incomplete steps. Option A would increase gastrocnemius tension. Option B describes part of the reduction but not the initial disengagement. Option D is not a primary maneuver for muscle relaxation. Option E is unsafe and not the specific maneuver highlighted for muscle relaxation in this context.
Question 5
Following successful closed reduction of the patient's medial subtalar dislocation, the foot is stable on clinical assessment. What is the most important next diagnostic step, and what is its primary purpose?
Explanation
Correct Answer: C
The case clearly states, 'While plain radiographs are sufficient for diagnosing the dislocation and guiding the immediate closed reduction, computed tomography is an absolute requirement following the reduction of any subtalar dislocation.' It further emphasizes, 'A post-reduction non-contrast CT scan of the foot and ankle with fine axial, coronal, and sagittal reformats is mandatory. The primary indications for this CT scan include evaluating for osteochondral shear fractures of the talar dome, talar head, or navicular,' and other periarticular fractures. Plain radiographs (Option B) are typically obtained immediately post-reduction but are insufficient for detecting occult fractures. MRI (Option A) is rarely indicated acutely and is more for subacute/chronic issues like AVN. Arteriography (Option D) and EMG (Option E) are not routinely indicated unless specific vascular or neurological deficits persist after reduction.
Question 6
Despite two well-executed attempts at closed reduction under adequate sedation, the patient's medial subtalar dislocation remains irreducible. The decision is made to proceed with emergent open reduction. For an irreducible medial subtalar dislocation, which of the following soft tissue structures is most commonly implicated as an interpositional block to reduction?
Explanation
Correct Answer: C
The case explicitly details the indications for operative intervention: 'In medial dislocations, the most common blocks to closed reduction include the buttonholing of the talar head through the extensor digitorum brevis muscle belly, the extensor retinaculum, or the talonavicular joint capsule.' The other options (posterior tibial tendon, flexor hallucis longus tendon, deltoid ligament, peroneus brevis tendon) are less common or not typically involved in blocking reduction of a medial subtalar dislocation. The EDB muscle belly, located dorsolaterally, is directly in the path of the prominent talar head during a medial dislocation.
Question 7
The patient undergoes successful open reduction and stabilization of his medial subtalar dislocation. During the post-operative rehabilitation phase, the patient asks about potential long-term complications. Based on the case information, which of the following is the most common long-term complication associated with high-energy subtalar dislocations, even after successful reduction?
Explanation
Correct Answer: C
The case highlights under 'Pitfall Underestimating Long Term Complications': 'Furthermore, post-traumatic subtalar arthritis occurs in up to 50 percent of high-energy cases, regardless of the quality of reduction, due to the initial chondral insult.' While avascular necrosis (Option A) is a concern, its rate is significantly lower in isolated subtalar dislocations compared to talar neck fractures. Chronic ankle instability (Option B) and recurrent dislocation (Option D) are less common if the reduction is stable and appropriate rehabilitation is followed. Tarsal tunnel syndrome (Option E) is a rare complication and not the most common long-term issue.
Question 8
A different patient presents with a severe midfoot deformity after a high-energy twisting injury. Radiographs show complete disarticulation at the talonavicular and calcaneocuboid joints, but the subtalar joint remains intact. Based on the provided differential diagnosis table, what is the most likely injury?
Explanation
Correct Answer: D
The differential diagnosis table explicitly defines 'Chopart Joint Dislocation' as having 'Disarticulation at talonavicular and calcaneocuboid joints, subtalar joint intact.' This perfectly matches the clinical scenario described in the question. Medial and Lateral Subtalar Dislocations involve disarticulation of the talonavicular and talocalcaneal joints. Talar Neck Fractures involve a fracture line through the talar neck. Pantalar Dislocation involves dislocation of the tibiotalar, subtalar, and talonavicular joints simultaneously. Therefore, Chopart Joint Dislocation is the correct answer.
Question 9
Regarding the classification and epidemiology of subtalar dislocations, which of the following statements is most accurate?
Explanation
Correct Answer: D
The case states: 'Medial Dislocations: Account for approximately 80 to 85 percent of all subtalar dislocations. They are typically lower energy than lateral dislocations and have a higher success rate for closed reduction.' This directly supports option D and refutes options A and B. Lateral dislocations account for 15 to 20 percent of cases and are often higher-energy with a higher rate of irreducibility. Anterior and posterior dislocations are 'exceedingly rare, representing less than 1 percent of cases,' refuting option C. Finally, the 'Clinical Pearls and Pitfalls' section notes: 'Pearl Understanding the Nomenclature: Subtalar dislocations are named by the direction the foot travels, not the talus,' refuting option E.
Question 10
During the review of the mandatory post-reduction CT scan for this patient, the orthopedic surgeon is particularly vigilant for specific occult fractures. Which of the following fractures, often missed on plain radiographs and associated with rapid subtalar arthrosis if displaced, is a critical finding to identify?
Explanation
Correct Answer: C
The case specifically highlights this under 'Clinical Pearls and Pitfalls': 'Pitfall Missing the Snowboarders Fracture: The lateral process of the talus is highly susceptible to fracture during the inversion/dorsiflexion moments of peritalar trauma. Missing a displaced lateral process fracture will lead to rapid subtalar arthrosis and chronic lateral-sided foot pain.' While other fractures like sustentaculum tali (Option A) or navicular body (Option E) can occur, the lateral process of the talus fracture is specifically emphasized as a 'snowboarder's fracture' with significant long-term implications if missed. Posterior malleolus (Option B) and medial cuneiform (Option D) fractures are less commonly associated with isolated subtalar dislocations.
Question 11
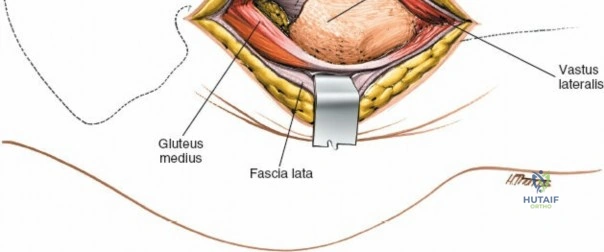
A 35-year-old male presents to the emergency department following a high-speed motorcycle collision, sustaining the injury to his left lower extremity as depicted in the clinical image. Initial assessment reveals a Gustilo-Anderson Type IIIC open tibia and fibula fracture with absent distal pulses and profound neurological deficit. The patient is hemodynamically stable. Which of the following is the MOST appropriate immediate next step after initial resuscitation and application of a tourniquet?

Explanation
Correct Answer: C
The patient presents with a Gustilo-Anderson Type IIIC open fracture, characterized by an open fracture with associated arterial injury requiring repair. This is a surgical emergency. The immediate priorities after initial resuscitation and hemorrhage control (tourniquet application) are to prevent infection and restore vascularity. Broad-spectrum intravenous antibiotics and tetanus prophylaxis are critical to minimize the risk of infection in open fractures, especially Gustilo Type III. Prompt transfer to the operating room for thorough debridement of contaminated and non-viable tissue, along with vascular assessment and repair, is paramount to limb salvage. The 'golden hour' principle for revascularization is crucial to minimize warm ischemia time and improve outcomes.
Option A is incorrect: Immediate definitive internal fixation with an intramedullary nail is contraindicated in a highly contaminated, unstable open fracture with extensive soft tissue damage and vascular compromise. Damage control orthopedics (DCO) with external fixation is the preferred initial skeletal stabilization method, allowing for serial debridements and soft tissue management.
Option B is incorrect: While a comprehensive trauma survey (ATLS protocol) is essential, the case states that a detailed trauma survey revealed no other life-threatening injuries, and the patient's vital signs were stable. The profound neurovascular compromise of the limb makes it the most time-sensitive, limb-threatening injury. Delaying limb management for extensive imaging of other body regions, especially when the patient is stable and other life-threatening injuries have been ruled out, is inappropriate and risks limb loss.
Option D is incorrect: Delaying surgery for an open fracture, particularly one with vascular compromise, significantly increases the risk of infection, limb loss, and poor functional outcomes. The wound must be debrided and vascularity restored emergently.
Option E is incorrect: While a plastic surgeon will be involved for definitive soft tissue coverage, this is typically performed after initial debridement, vascular repair, and skeletal stabilization. Immediate free flap coverage before these critical initial steps is not the correct sequence of management.
Question 12
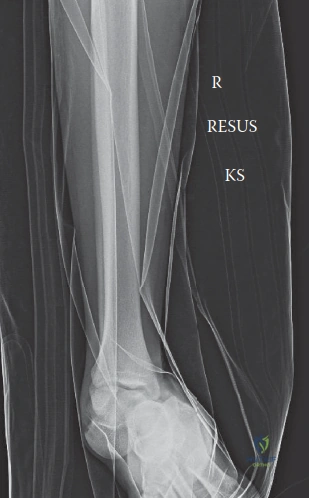
The patient's initial radiographs are shown. Based on these images and the clinical presentation, which of the following best describes the skeletal injury and its implications for initial management?

Explanation
Correct Answer: B
The radiographs clearly show a highly comminuted, segmental fracture of the mid-distal tibial shaft, extending into the metaphysis, with significant shortening and displacement. There is also a comminuted fibula fracture at a similar level. The presence of multiple fragments, bone loss, and the open nature of the injury (Gustilo IIIC) with gross contamination and neurovascular compromise makes immediate definitive internal fixation (like intramedullary nailing or plating) inappropriate. Damage control external fixation is the standard initial approach for such severe injuries, providing provisional stability, allowing for serial debridements, vascular repair, and soft tissue management without introducing further hardware into a contaminated field.
Option A is incorrect: The radiographs do not show a simple transverse fracture; it is highly comminuted and segmental. Immediate intramedullary nailing is contraindicated due to the open nature, contamination, and extensive soft tissue and vascular injury.
Option C is incorrect: While the fracture extends into the metaphysis, it is primarily a diaphyseal/metaphyseal junction fracture, not a true pilon (intra-articular distal tibia) fracture. Even if it were a pilon, immediate ORIF would be contraindicated in this setting due to the severe soft tissue injury and contamination.
Option D is incorrect: The fibula fracture is associated with a severe tibial fracture and significant soft tissue injury. It is not an isolated injury, and the primary concern is the tibia and its associated neurovascular compromise.
Option E is incorrect: The patient is 35 years old, well past skeletal maturity. Salter-Harris classifications apply to physeal (growth plate) injuries in skeletally immature patients.
Question 13
Following initial debridement in the operating room, an intraoperative angiogram is performed, confirming the findings of the pre-operative CTA. The image provided shows the CTA findings. Which of the following statements regarding the vascular injury and its management is most accurate?

Explanation
Correct Answer: C
The CTA findings, as described in the case, confirmed complete transection of the posterior tibial artery approximately 5 cm distal to the popliteal trifurcation. The anterior tibial artery and peroneal artery demonstrated flow, but with signs of intimal injury and reduced caliber distally. For a transected artery, an autologous vein graft (typically reverse saphenous vein from the contralateral leg) is the gold standard for interposition grafting to restore arterial continuity, especially for defects that cannot be repaired primarily. This was the approach taken in the case.
Option A is incorrect: The CTA showed that the anterior tibial artery and peroneal artery demonstrated flow, albeit with signs of intimal injury. Only the posterior tibial artery was completely transected. Therefore, not all three major tibial arteries were occluded, and limb salvage was attempted.
Option B is incorrect: The posterior tibial artery is a major vessel supplying the foot. Its repair is critical for limb salvage, especially in the context of a Gustilo IIIC injury where other vessels may also be compromised. Ligation would significantly increase the risk of limb ischemia and amputation.
Option D is incorrect: The case explicitly states that the posterior tibial artery was completely transected, while the anterior tibial artery showed flow but with signs of intimal injury. Therefore, the posterior tibial artery repair was the primary focus for revascularization.
Option E is incorrect: While the peroneal artery contributes to collateral flow, it is not typically the primary vessel for revascularization in the context of a major tibial artery transection. The posterior tibial artery is a major conduit, and its repair is crucial for distal perfusion.
Question 14
Following vascular reconstruction, the orthopedic trauma team applies an external fixator as shown in the image. What is the primary rationale for choosing this method of skeletal stabilization in this specific case?

Explanation
Correct Answer: C
In a Gustilo-Anderson Type IIIC open fracture with extensive soft tissue injury, contamination, and vascular repair, damage control external fixation is the preferred initial method of skeletal stabilization. Its primary advantages are that it provides provisional stability, allows for easy access to the wound for serial debridements and soft tissue management (e.g., VAC changes, free flap coverage), and avoids placing internal hardware (plates, nails) into a highly contaminated environment, which would significantly increase the risk of deep infection and osteomyelitis.
Option A is incorrect: External fixators provide provisional stability but are not typically used for immediate full weight-bearing, especially in comminuted fractures. Definitive fixation and weight-bearing progression occur much later.
Option B is incorrect: External fixators are excellent for maintaining length and alignment but achieving perfect anatomical reduction in highly comminuted fractures can be challenging and is often not the primary goal of initial DCO. The priority is stability and soft tissue management.
Option D is incorrect: While some micromotion can promote healing, the primary rationale for external fixation in this acute setting is damage control and soft tissue management, not primarily to promote rapid healing through micromotion. Overly flexible frames can lead to non-union.
Option E is incorrect: The cost and surgical skill required are not the primary drivers for choosing external fixation in this critical scenario. Its clinical advantages in managing complex open fractures are paramount.
Question 15
Mr. J.S. undergoes serial debridements and successful vascular reconstruction. Five days post-injury, a clean, granulating wound bed is achieved over the extensive anteromedial defect. Given the exposed bone and large soft tissue defect, what is the most appropriate next step for definitive soft tissue coverage?
Explanation
Correct Answer: D
The case describes an extensive, irregular open wound (15 x 8 cm) with exposed, comminuted distal tibial shaft and metaphyseal fragments. When there is exposed bone, tendon, or hardware, and the defect is too large for primary closure or local flaps, a free tissue transfer (free flap) is the gold standard for definitive soft tissue coverage. A free flap, such as a latissimus dorsi flap, brings its own blood supply, providing well-vascularized tissue to cover the defect, promote healing, and protect the underlying structures.
Option A is incorrect: Primary closure is not possible for such a large defect with significant soft tissue loss and exposed bone. Attempting primary closure would lead to excessive tension, wound dehiscence, and potential flap necrosis.
Option B is incorrect: A split-thickness skin graft requires a well-vascularized, granulating wound bed for successful take. It cannot be applied directly over exposed bone, as bone lacks the necessary blood supply for graft survival.
Option C is incorrect: While VAC therapy helps prepare the wound bed, a defect of this size with exposed bone will not be amenable to delayed primary closure. The tissue loss is too extensive.
Option E is incorrect: Local rotational flaps are typically used for smaller defects or defects where adjacent healthy tissue is available. For a large anteromedial tibial defect with significant soft tissue avulsion, a local flap from the same leg is often insufficient or would compromise already traumatized tissue. A flap from the contralateral leg is not a 'local' flap and would be a complex procedure with significant donor site morbidity for a local flap.
Question 16
Mr. J.S. sustained a complete transection of the posterior tibial artery and a partial transection of the tibial nerve. The vascular injury was repaired during the initial surgery. Regarding the management of the tibial nerve injury, what is the most appropriate approach?
Explanation
Correct Answer: C
In the context of a highly contaminated Gustilo-Anderson Type IIIC open fracture with extensive soft tissue damage, immediate primary repair of a transected nerve is generally not recommended. The priority during the initial surgery is debridement, vascular repair, and skeletal stabilization. Nerve repair is typically delayed until the wound bed is clean, stable, and definitive soft tissue coverage has been achieved, minimizing the risk of infection and ensuring a healthy environment for nerve healing. This allows for a more controlled and precise microsurgical repair, often requiring nerve grafting due to tissue loss.
Option A is incorrect: Immediate primary repair is contraindicated due to contamination and the need for serial debridements, which could disrupt the repair. It is a 'clean' procedure that should be performed in a 'clean' environment.
Option B is incorrect: While functional recovery can be challenging, especially with a complete transection, attempting nerve repair or grafting is indicated in a young, otherwise healthy patient to maximize the potential for functional recovery and sensation, which can significantly improve the quality of life and prevent a non-functional limb.
Option D is incorrect: A complete transection of a major nerve like the tibial nerve will not spontaneously recover. Surgical intervention (repair or grafting) is necessary to bridge the gap and allow for axonal regeneration.
Option E is incorrect: While a complete tibial nerve injury is severe, it does not automatically necessitate amputation, especially if vascularity is restored and the patient is young and motivated. Functional outcomes can still be achieved with nerve grafting and extensive rehabilitation, making the limb more functional than a prosthesis for some activities.
Question 17
The Mangled Extremity Severity Score (MESS) was calculated for Mr. J.S. as 6. Which of the following statements accurately reflects the interpretation and utility of the MESS score in this patient's case?
Explanation
Correct Answer: C
The MESS score is a prognostic tool used to quantify the severity of a mangled extremity and predict the likelihood of amputation. A score of ≥ 7 is often cited as a strong predictor for amputation. Mr. J.S.'s score of 6 is high, indicating a severe injury and a guarded prognosis, but it is just below the conventional threshold. Importantly, the case highlights that the MESS score serves as a powerful prognostic indicator but is not the sole determinant for the final decision. Patient factors (young age, healthy), reconstructible vascular injury, and the availability of a multidisciplinary team argued strongly for an attempt at limb salvage.
Option A is incorrect: A MESS score of 6, while high, is below the conventional threshold of 7 and does not definitively mandate primary amputation. Clinical judgment, patient factors, and surgical resources play a significant role.
Option B is incorrect: The MESS score is a guide, not a rigid rule. It helps quantify severity but does not dictate the decision. Many factors beyond the score influence the final decision, as detailed in the case's 'Salvage vs. Amputation Decision Factors'.
Option D is incorrect: The MESS score includes components for skeletal/soft-tissue injury, limb ischemia (vascular status), shock, and age. Therefore, it explicitly accounts for vascular status.
Option E is incorrect: While a low MESS score generally indicates a better prognosis, it does not guarantee a successful limb salvage or excellent functional outcome. Complications can still arise, and functional recovery depends on many variables.
Question 18
During the post-operative course, Mr. J.S. is at risk for several complications. Which of the following is a critical pitfall to avoid in the immediate post-revascularization period for this patient?
Explanation
Correct Answer: B
The case explicitly lists 'Inadequate Debridement' as the 'most common cause of persistent infection (osteomyelitis) and salvage failure.' Leaving devitalized tissue is a setup for disaster. This is a critical pitfall to avoid in the management of severe open fractures.
Option A is incorrect: Early mobilization and weight-bearing are pitfalls to avoid, but not specifically in the immediate post-revascularization period. The immediate concern post-revascularization is reperfusion injury and compartment syndrome, and early weight-bearing would be contraindicated due to the unstable fracture and soft tissue reconstruction.
Option C is incorrect: Delayed nerve grafting is a 'pearl' or appropriate management strategy, not a pitfall. It is done after the wound is clean and stable.
Option D is incorrect: Aggressive nutritional support is a 'pearl' and crucial for healing in these catabolic patients, not a pitfall.
Option E is incorrect: Meticulous pin site care is a 'pearl' and essential to prevent pin tract infections, not a pitfall.
Question 19
Several weeks after the initial injury, with successful free flap coverage and a stable soft tissue envelope, the orthopedic team plans for definitive skeletal fixation. Given the extensive comminution and segmental bone loss noted on initial X-rays, what is the most appropriate long-term strategy for managing the tibial bone defect?
Explanation
Correct Answer: C
The case describes significant comminution and segmental bone loss. After successful soft tissue coverage and a clean wound, the external fixator can be maintained and modified into a limb reconstruction frame (such as an Ilizarov or Taylor Spatial Frame). These frames are ideal for managing bone defects through techniques like bone transport or distraction osteogenesis, which can regenerate bone. Autologous cancellous bone grafting is then planned once the soft tissue envelope is stable and infection risk is minimized.
Option A is incorrect: While intramedullary nailing is a common definitive fixation for tibial shaft fractures, it is less suitable for large segmental bone defects without additional procedures like bone grafting or transport. Immediate full weight-bearing would also be premature.
Option B is incorrect: A standard locking plate might be used for some comminuted fractures, but for significant segmental bone loss, it would require extensive bone grafting and may not provide the necessary stability for bone regeneration or transport. Compression fixation is not appropriate for a bone defect.
Option D is incorrect: Non-operative management with a cast is entirely inappropriate for a comminuted, segmental open fracture with bone loss, which would almost certainly result in non-union or severe malunion.
Option E is incorrect: While the injury is severe, the decision was made for limb salvage. Bone loss of this magnitude, especially in a young patient, is often reconstructible with advanced techniques like bone transport or staged bone grafting, making primary amputation an incorrect choice at this stage.
Question 20
Mr. J.S.'s rehabilitation is expected to be protracted. Which of the following is a realistic expectation for his long-term functional outcome following successful limb salvage for this severe injury?
Explanation
Correct Answer: C
The case explicitly states under 'Expected Outcome' for limb salvage: 'Prolonged rehabilitation, potential for good functional limb, albeit with potential long-term issues (pain, stiffness, residual deficit).' It also notes that 'Full pre-injury function is often elusive in such severe injuries.' This reflects a realistic and balanced prognosis for such a complex limb salvage.
Option A is incorrect: Full return to pre-injury function, especially high-impact sports, within 6 months is highly unrealistic for a Gustilo IIIC open tibia fracture with neurovascular injury and extensive reconstruction. The rehabilitation trajectory is typically 18-24 months or longer.
Option B is incorrect: Limb salvage typically involves a prolonged hospital stay, multiple surgeries, and a much longer rehabilitation period compared to primary amputation, which often allows for a faster return to function with a prosthetic limb.
Option D is incorrect: While nerve grafting aims to improve function, complete absence of pain and neurological deficits is rarely achieved in such severe nerve injuries. Residual deficits and neuropathic pain are common long-term issues.
Option E is incorrect: Given the extensive soft tissue loss, degloving, and free flap coverage, an excellent cosmetic outcome with no visible scarring is highly improbable. Functional limitations are also a realistic expectation.
Question 21
The case emphasizes the importance of a multidisciplinary approach. Which combination of surgical specialties is most crucial for the immediate and staged management of Mr. J.S.'s Gustilo-Anderson Type IIIC open tibia fracture?
Explanation
Correct Answer: B
The case explicitly states that 'Successful salvage requires a coordinated team: trauma surgeons, orthopedic trauma surgeons, vascular surgeons, plastic surgeons, infectious disease specialists, and rehabilitation specialists.' For the immediate and staged surgical management of a Gustilo-Anderson Type IIIC open tibia fracture with neurovascular injury, the core surgical specialties are:
- Orthopedic Trauma: For debridement, skeletal stabilization (external fixation, definitive fixation), and bone defect management.
- Vascular Surgery: For assessment and repair of the arterial injury (e.g., saphenous vein graft).
- Plastic Surgery: For definitive soft tissue coverage (e.g., free flap) and delayed nerve grafting.
These three specialties are indispensable for the complex reconstruction required.
Options A, C, D, and E are incorrect: While other specialties may be involved in polytrauma, the listed combinations are not directly relevant or primary for the surgical management of this specific lower extremity injury.
Question 22
During the initial debridement of Mr. J.S.'s wound, the deep fascia was opened to fully explore all compartments. This step is critical because:
Explanation
Correct Answer: C
Opening the deep fascia (fasciotomy) during debridement of a high-energy open fracture, especially with significant soft tissue trauma and vascular compromise, is critical for two main reasons: 1) to relieve any potential occult compartment syndrome, which can develop rapidly, particularly after revascularization (reperfusion injury), and 2) to allow for thorough assessment of muscle viability within all compartments. Non-viable muscle must be debrided, and a fasciotomy ensures full access and decompression.
Option A is incorrect: While opening the fascia provides better visualization, its primary purpose is not for fracture fragment identification or reduction, but for compartment decompression and muscle assessment.
Option B is incorrect: Opening the fascia does not directly promote faster skin healing; in fact, it often creates a larger defect that requires more complex soft tissue coverage. Skin healing is dependent on a healthy wound bed and viable tissue.
Option D is incorrect: While a VAC device can be applied over an open fasciotomy, opening the fascia is not done specifically to facilitate VAC application. The VAC is applied after the fasciotomy and debridement.
Option E is incorrect: While thorough debridement is standard for all open fractures, routine fasciotomy for all open fractures is not. It is indicated when there is concern for compartment syndrome, significant muscle injury, or high-energy trauma, as in this case.
Question 23
A 30-year-old male sustains a vertically oriented (Pauwels III) femoral neck fracture following a high-energy fall. Which fixation construct provides the greatest biomechanical stability to resist the high shear forces and varus collapse characteristic of this injury?
Explanation
Question 24
A 28-year-old female presents with a severely comminuted closed tibial shaft fracture. She complains of intense pain exacerbated by passive toe extension. Her diastolic blood pressure is 75 mmHg. Intracompartmental pressure monitoring is performed. Which delta pressure threshold most definitively supports the indication for emergent four-compartment fasciotomy?
Explanation
Question 25
In the initial resuscitation of a hemodynamically unstable patient with an anteroposterior compression (APC) pelvic ring injury, a circumferential pelvic binder must be applied. What is the optimal anatomical landmark for the placement of the binder to effectively reduce pelvic volume?
Explanation
Question 26
A 22-year-old athlete sustains a high-energy knee dislocation. Following closed reduction, the foot remains warm and pink, but pedal pulses are faint. The Ankle-Brachial Index (ABI) is measured at 0.85. What is the most appropriate next step in the management of this patient?
Explanation
Question 27
A 34-year-old male is recovering from a Hawkins Type II talar neck fracture treated with open reduction and internal fixation. At 8 weeks post-operation, an anteroposterior radiograph reveals a subchondral radiolucent band in the talar dome. What does this specific radiographic finding indicate?
Explanation
Question 28
A 45-year-old male is scheduled to undergo open reduction and internal fixation for a displaced Sanders Type III calcaneus fracture via an extensile lateral approach. Which of the following is the most common and significant complication uniquely associated with this surgical approach?
Explanation
Question 29
During the intramedullary nailing of a subtrochanteric femur fracture, the proximal segment is frequently noted to be severely displaced into a flexed, abducted, and externally rotated position. Which muscle is primarily responsible for the flexion deformity of the proximal fragment?
Explanation
Question 30
A 40-year-old female sustains a comminuted intra-articular distal femur fracture. CT imaging demonstrates a concurrent coronal plane shear fracture of the lateral femoral condyle (Hoffa fragment). What is the optimal fixation strategy specifically for this condylar fragment?
Explanation
Question 31
A 28-year-old male presents with a displaced fracture of the talar neck with associated subluxation of the subtalar and tibiotalar joints. According to the Hawkins classification, what is the approximate rate of avascular necrosis (AVN) for this specific injury pattern?
Explanation
Question 32
A 30-year-old male sustains a vertically oriented femoral neck fracture (Pauwels type III) after a fall from a height. Which of the following biomechanical constructs provides the most stable fixation for this specific fracture pattern?
Explanation
Question 33
A 45-year-old male arrives in the trauma bay with a pelvic binder in place after an anteroposterior compression (APC-III) injury. He remains hypotensive despite 2 liters of crystalloid and 2 units of packed RBCs. Focused assessment with sonography for trauma (FAST) is negative. What is the most appropriate next step in management?
Explanation
Question 34
A 55-year-old female presents with a medial tibial plateau fracture following a varus-producing force. Radiographs show a depressed, split fragment of the medial plateau. Which of the following complications is most highly associated with this specific injury pattern compared to isolated lateral plateau fractures?
Explanation
Question 35
A 25-year-old male sustains a closed comminuted tibial shaft fracture. He complains of pain out of proportion to the injury. His diastolic blood pressure is 75 mmHg. Intracompartmental pressure monitoring of the anterior compartment reveals a pressure of 48 mmHg. What is his Delta P, and what is the definitive management?
Explanation
Question 36
A 40-year-old male undergoes open reduction and internal fixation of a displaced intra-articular calcaneus fracture via an extensile lateral approach. Which of the following structures is at the highest risk of iatrogenic injury during the full-thickness flap elevation?
Explanation
Question 37
A 22-year-old football player presents with midfoot pain after an axial load on a plantarflexed foot. Weight-bearing radiographs demonstrate a 3 mm diastasis between the base of the first and second metatarsals. What is the most appropriate definitive management?
Explanation
Question 38
A 35-year-old farmer sustains a severe open tibial shaft fracture (Gustilo-Anderson Type IIIA) heavily contaminated with soil and manure. According to evidence-based guidelines, what is the most appropriate initial empiric antibiotic regimen?
Explanation
Question 39
An 82-year-old female presents with a periprosthetic fracture of the distal femur above a posterior-stabilized total knee arthroplasty (TKA). The fracture is a comminuted spiral fracture proximal to the flange (Vancouver/Su Type II). The femoral component is radiographically well-fixed. What is the preferred surgical treatment?
Explanation
Question 40
A 28-year-old male sustains an anterior knee dislocation during a tackle. The knee is reduced in the ER. His distal pulses are palpable, and the Ankle-Brachial Index (ABI) is 0.85. What is the most appropriate next step?
Explanation
Question 41
A 34-year-old motorcyclist sustains a distal femur fracture. CT imaging reveals an intra-articular coronal plane fracture of the lateral femoral condyle. What is the eponymous name for this fracture pattern, and what is the optimal direction for screw fixation?
Explanation
Question 42
A 45-year-old recreational athlete sustains an acute closed Achilles tendon rupture. When comparing operative repair to functional rehabilitation (non-operative management), which of the following statements is most accurate based on current high-level evidence?
Explanation
Question 43
On an AP pelvis radiograph of a patient with an acetabular fracture, the iliopectineal line is disrupted, but the ilioischial line remains intact. Which specific component of the acetabulum is most likely fractured?
Explanation
Question 44
A 26-year-old male sustains a pronation-external rotation (PER) ankle fracture. Intraoperative stress testing reveals syndesmotic widening. When placing a syndesmotic screw, in what position should the ankle be held, and why?
Explanation
Question 45
A 32-year-old male sustains a high-energy motor vehicle collision resulting in a vertically oriented, displaced femoral neck fracture (Pauwels type III). What is the most mechanically sound construct for surgical fixation of this injury?
Explanation
Question 46
A 42-year-old construction worker falls from a height of 15 feet, sustaining a high-energy injury to his left knee. Radiographs and CT scan demonstrate a bicondylar tibial plateau fracture with complete dissociation of the metaphysis from the diaphysis. According to the Schatzker classification system, what type of fracture is this?
Explanation
Question 47
A 24-year-old male presents with a grossly deformed right knee after a football tackle. After emergent closed reduction in the trauma bay, his pedal pulses are palpable, but the Ankle-Brachial Index (ABI) is measured at 0.8. What is the most appropriate next step in management?
Explanation
Question 48
A 45-year-old male is crushed by heavy machinery and arrives hemodynamically unstable with a blood pressure of 75/40 mmHg. An anteroposterior pelvic radiograph reveals an Anteroposterior Compression (APC) Type III pelvic ring injury. A circumferential pelvic sheet or binder should be applied at which of the following anatomic levels to best reduce the pelvic volume?
Explanation
Question 49
A 21-year-old collegiate soccer player injures his midfoot while planting his cleated foot and twisting. Physical examination reveals plantar ecchymosis. Weight-bearing radiographs show 3 mm of widening between the medial cuneiform and the base of the second metatarsal. Which ligament is primarily injured in this scenario?
Explanation
Question 50
A 38-year-old male undergoes open reduction and internal fixation of a displaced intra-articular calcaneus fracture via an extensile lateral approach. Postoperatively, he complains of numbness and tingling along the lateral aspect of his foot. Which nerve was most likely injured or compressed during the surgical exposure?
Explanation
Question 51
A 28-year-old male presents after an aviation accident with a talar neck fracture. Radiographs show a displaced fracture of the talar neck with subluxation of the subtalar joint, while the ankle joint remains congruous. What is the approximate rate of avascular necrosis (AVN) of the talar body associated with this Hawkins classification?
Explanation
Question 52
A 68-year-old female presents with acute thigh pain and inability to bear weight after a simple trip and fall. Radiographs reveal a transverse fracture of the proximal femoral diaphysis with lateral cortical thickening and medial spiking. She has been taking alendronate for 12 years. What is the primary cellular mechanism contributing to this specific fracture pattern?
Explanation
Question 53
A 30-year-old male sustains a subtrochanteric femur fracture. On preoperative radiographs, the proximal fracture fragment is noted to be flexed, abducted, and externally rotated. Which muscle is primarily responsible for the flexion deformity of the proximal fragment?
Explanation
Question 54
To prevent the typical procurvatum (apex anterior) and valgus deformities associated with intramedullary nailing of proximal third tibial shaft fractures, where is the optimal placement for blocking (Poller) screws in the proximal segment relative to the intended nail path?
Explanation
Question 55
A 28-year-old male sustains a Hawkins Type III fracture of the talar neck. Which of the following provides the predominant blood supply to the talar body, placing it at highest risk for avascular necrosis when disrupted?
Explanation
Question 56
In a highly comminuted, displaced intra-articular calcaneus fracture (Sanders Type III), which anatomical fragment consistently remains aligned with the talus and serves as the foundation for surgical reconstruction?
Explanation
Question 57
A 22-year-old collegiate football player sustains a purely ligamentous Lisfranc injury with lateral subluxation of the 2nd and 3rd metatarsals. According to recent literature, what is the most appropriate definitive surgical management to optimize functional outcome and reduce reoperation rates?
Explanation
Question 58
A 35-year-old female presents to the trauma bay with a grossly unstable knee following a severe hyperextension injury. The limb is well-perfused, but an Ankle-Brachial Index (ABI) is measured at 0.8. What is the most appropriate next step in management?
Explanation
Question 59
What is the primary rationale for utilizing a staged protocol (immediate spanning external fixation followed by delayed internal fixation at 10-14 days) in the management of high-energy tibial pilon fractures?
Explanation
Question 60
A 45-year-old patient presents with a displaced coronal plane fracture of the lateral femoral condyle (Hoffa fracture). Which of the following describes the biomechanically optimal fixation strategy for this specific injury?
Explanation
Question 61
A 25-year-old male sustains a displaced, highly vertical (Pauwels Type III) femoral neck fracture. To maximize biomechanical stability and prevent failure secondary to high shear forces, which of the following constructs is most appropriate?
Explanation
Question 62
When stabilizing an intertrochanteric femur fracture utilizing a sliding hip screw, maintaining a Tip-Apex Distance (TAD) of less than 25 mm on combined AP and lateral radiographs primarily minimizes the risk of which complication?
Explanation
Question 63
During a percutaneous repair of an acute Achilles tendon rupture, the surgeon must be particularly cautious to avoid iatrogenic injury to the sural nerve. At what approximate distance proximal to the calcaneal insertion does the sural nerve cross the lateral border of the Achilles tendon?
Explanation
None
