Orthopedic Surgery Board Exam Review: Lower Limb Deformity, Paley's Principles & TKA | Part 22006
Key Takeaway
This module provides 20 advanced multiple-choice questions for the ABOS Part I and AAOS OITE exams. It covers lower limb deformity analysis, Paley's principles, osteotomy planning, and Total Knee Arthroplasty (TKA) alignment. Key topics include biomechanical angles (mLDFA, MPTA, PPTA, LDTA, NSA, mLPFA, ADTA, JLCA), systematic malalignment tests, and surgical pearls for orthopedic surgeons.
Orthopedic Surgery Board Exam Review: Lower Limb Deformity, Paley's Principles & TKA | Part 22006
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 62-year-old male presents with progressive right knee pain, worse with activity. Full-length standing AP radiographs reveal a Mechanical Axis Deviation (MAD) of 15mm medial to the center of the knee joint. The surgeon suspects a varus deformity originating from the proximal tibia. Based on Paley's principles, which of the following angles, if found to be abnormal, would most directly confirm a proximal tibial varus deformity and guide a high tibial osteotomy (HTO)?
Explanation
Correct Answer: C
The correct answer is C, the Medial Proximal Tibial Angle (MPTA). The case describes a patient with medial Mechanical Axis Deviation (MAD) and a suspicion of proximal tibial varus. According to Paley's principles, the MPTA is the cornerstone of tibial alignment in the frontal plane. A normal MPTA ranges from 85° to 90° (average ~87°). An MPTA of less than 85° specifically indicates tibia vara, which is a proximal tibial varus deformity. High Tibial Osteotomies (HTOs) are designed to correct this angle, typically restoring it to a normal or slightly valgus alignment (e.g., 89-90°) to offload the medial compartment.
Option A (mLDFA) is the mechanical Lateral Distal Femoral Angle. While critical for overall limb alignment, it assesses distal femoral alignment (normal 85-90°). An abnormality here would indicate a femoral deformity, not a proximal tibial one.
Option B (LDTA) is the Lateral Distal Tibial Angle. This angle assesses distal tibial alignment in the frontal plane (normal 86-92°). An abnormality here would indicate a deformity at the ankle level, not the proximal tibia.
Option D (PPTA) is the Posterior Proximal Tibial Angle. This angle assesses the sagittal plane alignment (posterior tibial slope) of the proximal tibia (normal 77-84°). While important for knee kinematics, it does not directly quantify frontal plane varus/valgus deformity.
Option E (NSA) is the Neck-Shaft Angle. This angle assesses the frontal plane alignment of the proximal femur (normal 124-136°). It is unrelated to knee or tibial deformities.
Question 2
A 30-year-old competitive runner presents with chronic anterior knee pain and a feeling of instability, particularly during deceleration. MRI reveals a chronic Anterior Cruciate Ligament (ACL) deficiency. Preoperative planning for an ACL reconstruction and potential concomitant osteotomy includes a detailed assessment of sagittal plane alignment. Based on the provided case, which of the following angles is most critical to evaluate for its impact on ACL strain and knee kinematics?
Explanation
Correct Answer: D
The correct answer is D, the Posterior Proximal Tibial Angle (PPTA). The case explicitly states that the posterior tibial slope, which is directly related to the PPTA (normal 77-84°, equating to ~9° posterior slope), is 'absolutely critical for knee kinematics and ligamentous stability.' An increased posterior slope (meaning a decreased PPTA) shifts the resting position of the tibia anteriorly, thereby increasing strain on the Anterior Cruciate Ligament (ACL). Conversely, a decreased slope (increased PPTA) places excessive strain on the Posterior Cruciate Ligament (PCL). Therefore, evaluating the PPTA is paramount in a patient with ACL deficiency, as an abnormal slope could contribute to instability or impact the success of reconstruction.
Option A (mLDFA) is the mechanical Lateral Distal Femoral Angle. This angle assesses frontal plane distal femoral alignment (normal 85-90°) and is not directly related to sagittal plane ACL strain.
Option B (PDFA) is the Posterior Distal Femoral Angle. This angle assesses sagittal plane distal femoral alignment (normal 79-87°). While important for overall knee extension/flexion, it does not directly dictate the tibial slope's impact on ACL strain.
Option C (MPTA) is the Medial Proximal Tibial Angle. This angle assesses frontal plane proximal tibial alignment (normal 85-90°) and is primarily relevant for varus/valgus deformities, not sagittal plane ligamentous stability.
Option E (LDTA) is the Lateral Distal Tibial Angle. This angle assesses frontal plane distal tibial alignment (normal 86-92°) and is relevant for ankle deformities, not knee ligamentous stability.
Question 3
A 10-year-old male presents with a progressive genu valgum deformity. Preoperative radiographs are obtained for planning a distal femoral osteotomy. When drawing the sagittal plane joint orientation line for the distal femur in this pediatric patient, which of the following surgical pearls, as highlighted in the case, is most crucial to consider?
Explanation
Correct Answer: C
The correct answer is C. The case explicitly states under 'Surgical Pearls for Joint Orientation Mapping' that for sagittal plane knee lines, 'The posterior distal femoral line in children is uniquely drawn at the physis, not the articular cartilage, because the cartilaginous anlage is not fully ossified and cannot be reliably seen on plain films.' This is a critical distinction for pediatric patients, as relying on the unossified articular cartilage would lead to inaccurate measurements.
Option A describes the method for drawing the frontal plane distal femoral joint orientation line in adults, not the sagittal plane line, and doesn't account for the physis in children.
Option B describes the mechanical axis of the femur, not a joint orientation line.
Option D describes the hip joint orientation line used to calculate the mLPFA, not the distal femoral sagittal plane line.
Option E describes the frontal plane proximal tibial joint orientation line, not the distal femoral sagittal plane line.
Question 4
A 55-year-old female undergoes a full-length standing AP radiograph of her lower extremities as part of a workup for knee osteoarthritis. The radiograph reveals a Mechanical Axis Deviation (MAD) of 12mm lateral to the center of the knee joint. The surgeon suspects a distal femoral valgus deformity. Which of the following angles, if found to be outside its normal range, would most accurately pinpoint the distal femur as the source of this valgus deformity?
Explanation
Correct Answer: C
The correct answer is C, the mechanical Lateral Distal Femoral Angle (mLDFA). The case describes a patient with lateral MAD, indicating a valgus deformity, and the suspicion is that it originates from the distal femur. The mLDFA is defined as the angle between the mechanical axis of the femur and a line tangential to the most distal points on the convexity of the two femoral condyles. A normal mLDFA ranges from 85° to 90° (average ~88°). An abnormally low mLDFA (less than 85°) indicates distal femoral valgus (knock-knees), which would cause a lateral shift of the mechanical axis. Distal femoral osteotomies (DFOs) are specifically designed to correct the mLDFA.
Option A (MPTA) assesses proximal tibial alignment (normal 85-90°). An abnormality here would indicate tibia vara or valga, not a distal femoral deformity.
Option B (LDTA) assesses distal tibial alignment (normal 86-92°). An abnormality here would indicate an ankle-level deformity, not a distal femoral one.
Option D (PDFA) assesses sagittal plane distal femoral alignment (normal 79-87°). While related to the distal femur, it describes flexion/extension deformities, not frontal plane valgus.
Option E (NSA) assesses proximal femoral alignment (normal 124-136°). It is unrelated to distal femoral or knee deformities.
Question 5
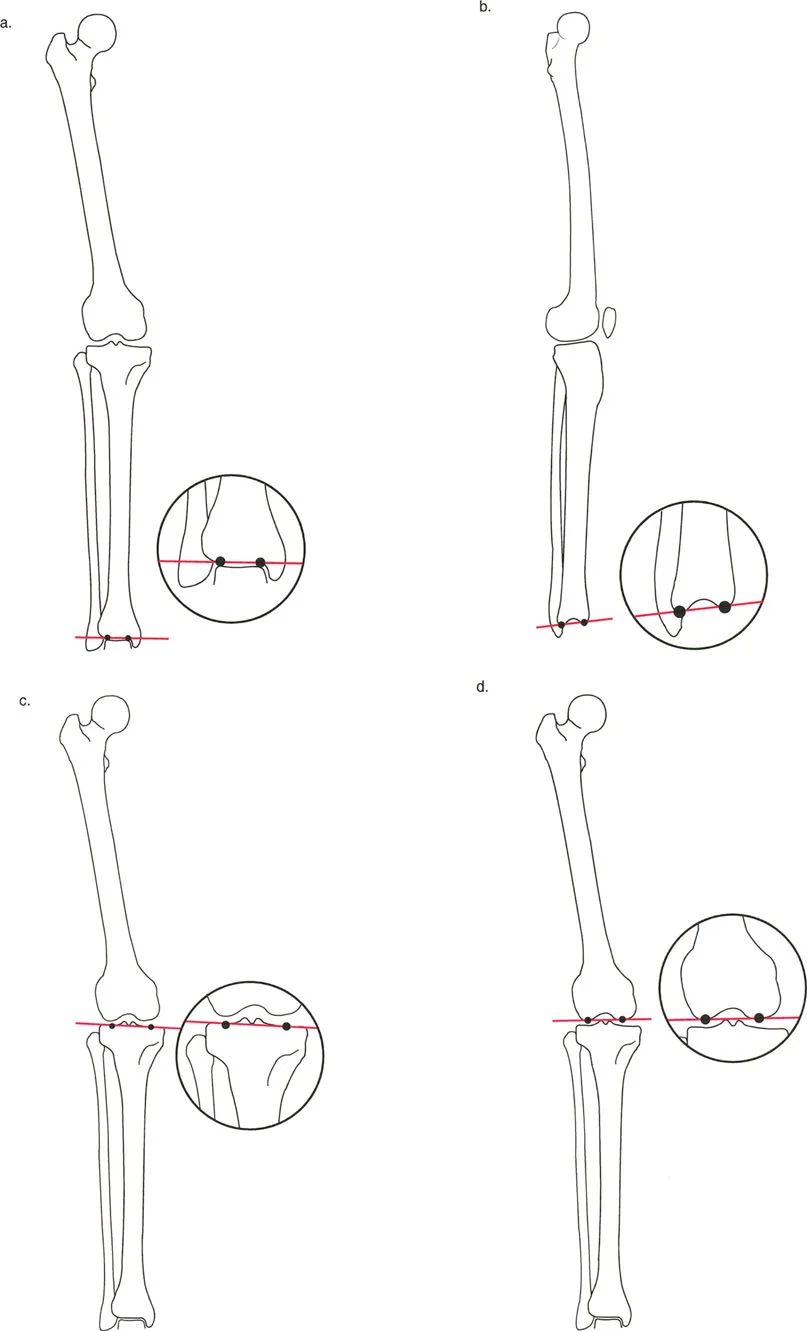
A 40-year-old male presents with chronic ankle pain and progressive varus deformity of the ankle, leading to medial gutter impingement. Preoperative planning for a supramalleolar osteotomy (SMOT) requires precise measurement of the frontal plane ankle orientation. Based on the case, which angle is the primary target for correction in this scenario?
Explanation
Correct Answer: C
The correct answer is C, the Lateral Distal Tibial Angle (LDTA). The case explicitly states that the LDTA is formed when the frontal plane ankle joint orientation line (across the tibial plafond) intersects the mechanical axis of the tibia. A normal LDTA ranges from 86° to 92° (average ~89°). An LDTA less than 86° indicates distal tibial varus, which shifts contact pressures medially and aligns with the patient's presentation of ankle varus deformity and medial gutter impingement. The text further emphasizes that 'Correcting the LDTA is a primary goal in supramalleolar osteotomies (SMOT).'
Option A (MPTA) assesses proximal tibial alignment (normal 85-90°) and is relevant for knee deformities, not ankle varus.
Option B (mLDFA) assesses distal femoral alignment (normal 85-90°) and is relevant for knee deformities, not ankle varus.
Option D (ADTA) is the Anterior Distal Tibial Angle. This angle assesses sagittal plane ankle orientation (normal 78-82°) and is relevant for procurvatum/recurvatum deformities, not frontal plane varus.
Option E (PPTA) assesses sagittal plane proximal tibial alignment (normal 77-84°) and is relevant for knee kinematics and ligamentous stability, not frontal plane ankle varus.
Question 6
A 28-year-old female presents with a Trendelenburg gait and chronic hip pain. Radiographs reveal a femoral neck-shaft angle of 115°. Based on Paley's principles, what is the most likely diagnosis and its direct biomechanical consequence?
Explanation
Correct Answer: D
The correct answer is D. The normal Neck-Shaft Angle (NSA) ranges from 124° to 136° (average ~130°). An NSA of 115° is significantly less than the normal range. The case defines an NSA less than 120° as coxa vara. The clinical implication of coxa vara is that it 'shortens the limb and can lead to a Trendelenburg gait due to abductor weakness' because the abductor muscles lose their mechanical advantage (moment arm) due to the altered femoral neck geometry.
Option A is incorrect because coxa valga is an NSA greater than 135°, and while it affects the abductor moment arm, it typically increases it, not decreases it in the context of a Trendelenburg gait.
Option B is incorrect because coxa vara leads to a decreased abductor moment arm, resulting in weakness, not an increased one.
Option C is incorrect because coxa valga (NSA > 135°) would lead to a relatively longer limb, and the patient has coxa vara.
Option E is incorrect because an NSA of 115° is clearly outside the normal range (124-136°), indicating a significant deformity.
Question 7
A surgeon is planning a complex osteotomy for a multi-planar lower limb deformity using a hexapod circular external fixator. The patient has a combined distal femoral and proximal tibial deformity. To ensure accurate correction and prevent inducing secondary deformities, which of the following principles, as described in the case, is paramount when placing the hinge pins for the osteotomy?
Explanation
Correct Answer: C
The correct answer is C. Under the 'Surgical Pearls for Joint Orientation Mapping' section, the case explicitly states: 'When performing an opening or closing wedge osteotomy, the hinge pin must be perfectly parallel to the joint orientation line to prevent inducing an unwanted secondary deformity in the orthogonal plane.' This principle ensures that the correction occurs purely in the intended plane (e.g., frontal plane for varus/valgus) without inadvertently creating a deformity in the sagittal plane (e.g., flexion/extension).
Option A is incorrect. While the mechanical axis is crucial for overall alignment, hinge pins are oriented relative to the joint line to control the plane of correction, not necessarily perpendicular to the mechanical axis of the entire limb.
Option B is incorrect. Hinge pins are oriented relative to the joint line, not necessarily parallel to the anatomic axis of the bone, especially if the anatomic axis itself is deformed or if the osteotomy is near a joint.
Option D is incorrect. While the CORA is the apex of the deformity and the ideal location for an osteotomy, the hinge pins' orientation (parallel to the joint line) is a separate, critical principle for preventing secondary deformities, regardless of whether the osteotomy is precisely at the CORA or away from it (using Paley's rules).
Option E describes the goal of traditional Mechanical Alignment in TKA, not a general principle for hinge pin placement in osteotomies. Furthermore, achieving 90-degree angles for mLDFA and MPTA might not be the goal for all osteotomies, especially if aiming for kinematic alignment or specific overcorrection.
Question 8
A 70-year-old patient is undergoing Total Knee Arthroplasty (TKA). The surgeon is debating between a traditional Mechanical Alignment (MA) approach and a Kinematic Alignment (KA) approach. Based on the case, what is the fundamental difference in how these two philosophies utilize joint orientation lines?
Explanation
Correct Answer: B
The correct answer is B. The case clearly differentiates Mechanical Alignment (MA) and Kinematic Alignment (KA) in TKA. It states: 'Mechanical Alignment: Traditional TKA aims to cut the distal femur and proximal tibia perpendicular to their mechanical axes. This forces the mLDFA and MPTA to be exactly 90°.' In contrast, 'Kinematic Alignment: Modern KA techniques aim to restore the patient's pre-arthritic joint orientation lines. The surgeon intentionally cuts the tibia at an MPTA of 87° and the femur at an mLDFA of 87° to match the native anatomy...'
Option A incorrectly swaps the definitions. MA aims for a neutral MAD (by making mLDFA and MPTA 90°), while KA aims to restore native joint lines.
Option C is incorrect. NSA and LDTA are not the primary distinguishing factors between MA and KA; the focus is on the knee's frontal plane angles (mLDFA, MPTA).
Option D is incorrect. Both MA and KA consider both frontal and sagittal planes, but the fundamental difference lies in their approach to frontal plane joint orientation (perpendicular to mechanical axis vs. native joint line).
Option E is incorrect. While 87° and 88° are average normal values, MA specifically aims for 90° for both mLDFA and MPTA, which often alters the native joint line. KA aims to restore the individual patient's pre-arthritic angles, which might be around these averages but are not rigidly set to them for all patients.
Question 9
A 35-year-old male presents with chronic posterior ankle pain and limited plantarflexion. Radiographic evaluation reveals an Anterior Distal Tibial Angle (ADTA) of 70°. Based on the case, what is the most likely sagittal plane deformity and its clinical implication?
Explanation
Correct Answer: D
The correct answer is D. The case states that the normal ADTA (Anterior Distal Tibial Angle) ranges from 78° to 82° (average ~80°). An ADTA of 70° is significantly decreased from the normal range. The clinical implication section for ADTA explicitly states: 'If the ADTA is decreased (e.g., <75°), the joint is in recurvatum, leading to posterior impingement and loss of plantarflexion.' This perfectly matches the patient's symptoms of chronic posterior ankle pain and limited plantarflexion.
Option A describes a frontal plane deformity (distal tibial varus) associated with an abnormal Lateral Distal Tibial Angle (LDTA), not ADTA.
Option B describes a frontal plane deformity (distal tibial valgus) also associated with an abnormal LDTA, not ADTA.
Option C describes ankle procurvatum, which occurs when the ADTA is increased (e.g., >85°), leading to anterior impingement and loss of dorsiflexion. This is the opposite of the patient's ADTA and symptoms.
Option E is incorrect because an ADTA of 70° is clearly outside the normal range, indicating a significant deformity.
Question 10
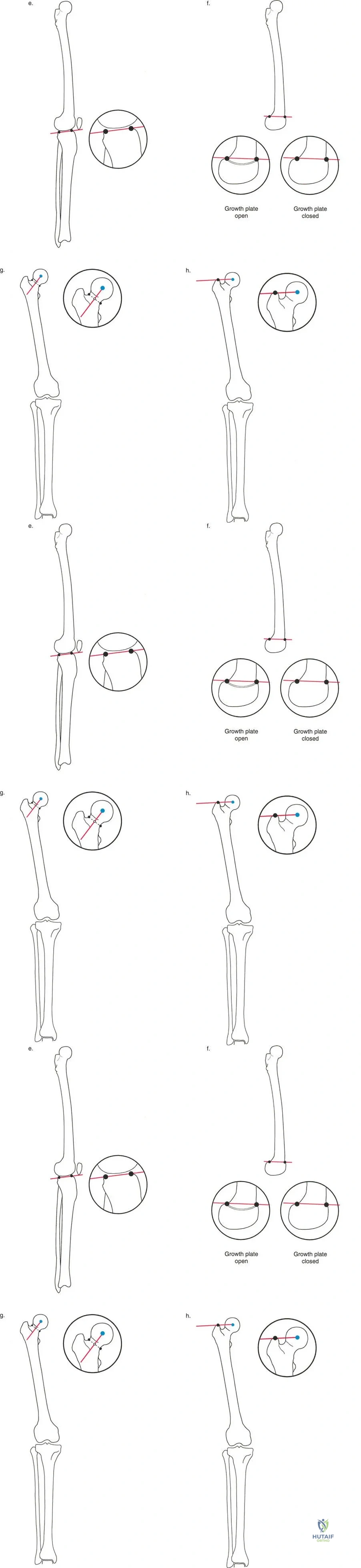
A 50-year-old patient with a history of hip trauma presents with a Trendelenburg gait and reports difficulty with abductor strength. Radiographs show a high-riding greater trochanter relative to the femoral head. Which of the following angles, as defined by Paley's principles, would be most directly affected by this anatomical finding and explain the patient's abductor weakness?
Explanation
Correct Answer: B
The correct answer is B, the mechanical Lateral Proximal Femoral Angle (mLPFA). The case defines the mLPFA as the angle formed when a line from the proximal tip of the greater trochanter to the center of the femoral head intersects the mechanical axis of the femur. A normal mLPFA ranges from 85° to 95° (average ~90°). The clinical implication section for mLPFA explicitly states: 'The mLPFA is a brilliant measure of the articulotrochanteric distance (ATD). If the tip of the greater trochanter rides too high (e.g., due to a collapsed femoral neck or coxa vara), the mLPFA decreases. A high-riding trochanter creates functional abductor weakness because the gluteus medius loses its tension and resting length.' This directly explains the patient's high-riding trochanter and abductor weakness.
Option A (NSA) is the Neck-Shaft Angle. While coxa vara (a low NSA) can lead to a high-riding trochanter, the mLPFA is the direct measure of the articulotrochanteric distance and its impact on abductor mechanics, as described in the text.
Option C (mLDFA) assesses distal femoral frontal plane alignment and is unrelated to hip abductor mechanics.
Option D (MPTA) assesses proximal tibial frontal plane alignment and is unrelated to hip abductor mechanics.
Option E (PDFA) assesses distal femoral sagittal plane alignment and is unrelated to hip abductor mechanics.
Question 11
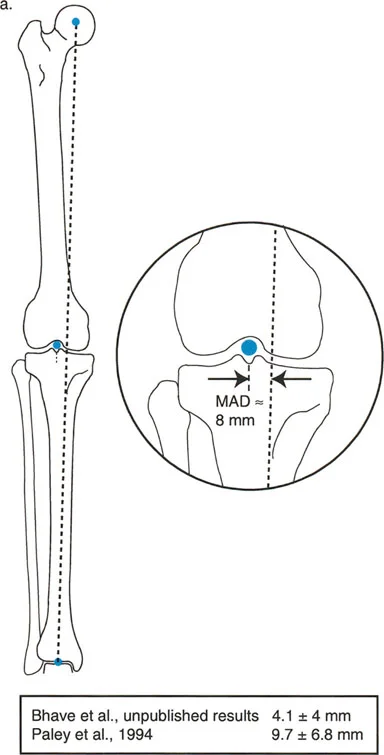
A 62-year-old male presents with progressive right knee pain, worse with ambulation. A long-standing, weight-bearing anteroposterior radiograph of the entire lower extremity is obtained, as shown in the diagram below, demonstrating the mechanical axis of the lower limb. The orthopedic surgeon measures the perpendicular distance from the mechanical axis to the center of the knee joint.
Based on Paley's principles, what is the normal range for this measurement, and what does an excessive medial deviation indicate?
Explanation
Correct Answer: C
The question describes the Mechanical Axis Deviation (MAD), which is the perpendicular distance from the mechanical axis of the entire lower limb to the center of the knee joint. According to the case, the normal MAD is approximately 8 mm (± 7 mm) medial to the center of the knee. An excessive medial deviation (i.e., the mechanical axis passing significantly medial to the knee center) indicates a varus alignment, which predisposes to medial compartment osteoarthritis. Conversely, a mechanical axis passing lateral to the knee center indicates a valgus alignment.
Option A is incorrect because the normal MAD is medial, not lateral, and 0 mm is not the typical normal value.
Option B is incorrect because the normal MAD is medial, not lateral.
Option D is incorrect because the normal MAD is approximately 8 mm medial, not 0 mm, and an excessive medial deviation indicates varus, not valgus.
Option E is incorrect because 15 mm is outside the normal range, and an excessive medial deviation indicates varus, not valgus.
Question 12
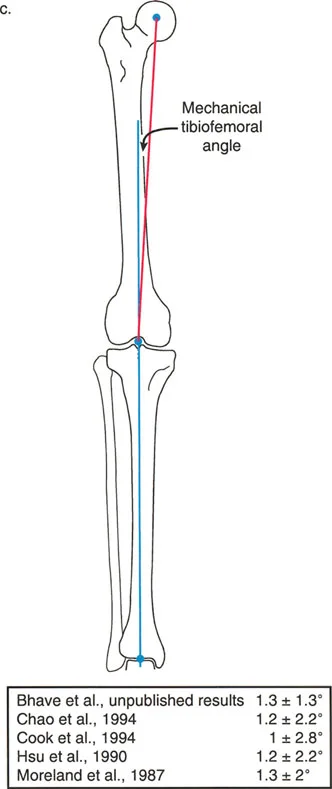
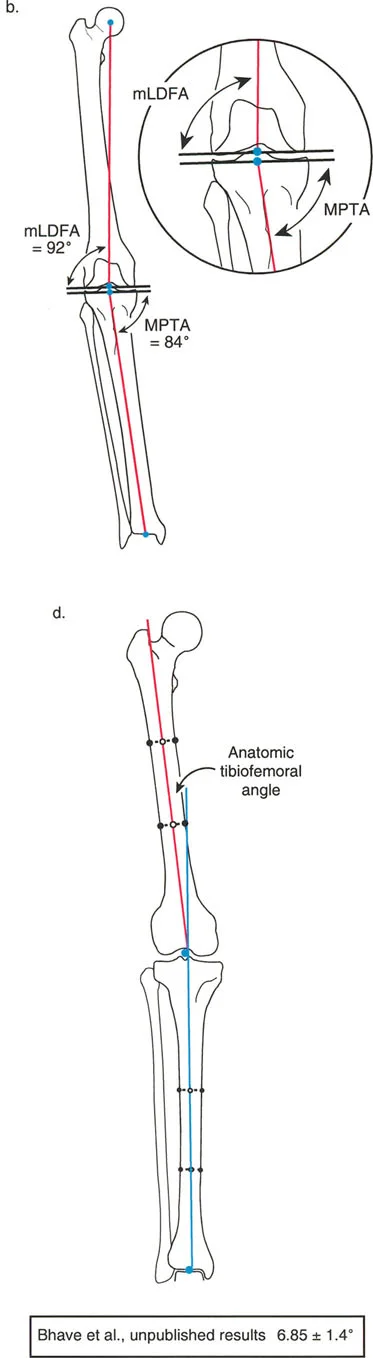
A resident is reviewing a long-standing radiograph of a patient with a distal femoral deformity, attempting to apply Paley's standardized nomenclature. They have drawn the mechanical axis of the femur and the knee joint line, creating two supplementary angles at their intersection, as depicted in the diagram below. The resident measures the medial angle as 92° and the lateral angle as 88°.
According to Paley's 'Less Than 90 Degrees' rule, which angle should be formally named and referenced for the distal femur, and what is its normal value?
Explanation
Correct Answer: B
Paley's 'Less Than 90 Degrees' rule states that when an axis line intersects a joint line, the angle that is normally less than 90° is chosen for formal naming and reference. For the distal femur, the intersection of the mechanical axis and the knee joint line creates the mMDFA (mechanical Medial Distal Femoral Angle) and the mLDFA (mechanical Lateral Distal Femoral Angle). The normal mLDFA is 88°, while the normal mMDFA is 92°. Therefore, the mLDFA is the standard reference angle.
Option A is incorrect because while mMDFA is 92°, it is not the angle chosen by the 'less than 90 degrees' rule.
Option C refers to the anatomic axis (aLDFA), which is 81°, but the question specifically refers to the mechanical axis intersection described by the resident's measurements (88° and 92°).
Option D is incorrect because mMDFA is normally 92°, not 88°.
Option E is incorrect because aMDFA is not the standard reference, and the value is incorrect for the anatomic axis.
Question 13
A 35-year-old female presents with a progressive varus deformity of her left knee. A full-length standing radiograph is obtained, and the orthopedic surgeon performs a detailed deformity analysis using Paley's principles. The diagram below illustrates the key frontal plane angles.
The surgeon measures the mLDFA as 95° and the MPTA as 80°. Based on these findings, what is the primary contributor to the patient's varus deformity?

Explanation
Correct Answer: B
According to the case, the normal mLDFA (mechanical Lateral Distal Femoral Angle) is 88° (range: 85–90°). An mLDFA > 90° indicates femoral varus. The patient's mLDFA of 95° clearly indicates femoral varus.
The normal MPTA (Medial Proximal Tibial Angle) is 87° (range: 85–90°). An MPTA < 85° indicates tibial varus. The patient's MPTA of 80° clearly indicates tibial varus.
Therefore, both the femur and the tibia are contributing to the patient's overall varus deformity.
Option A is incorrect as both measurements indicate varus, not valgus.
Options C and D are incorrect because both bones are contributing to the varus deformity, not just one in isolation.
Option E is incorrect as both femoral and tibial alignments are abnormal and indicate varus, not valgus.
Question 14
A 50-year-old male is scheduled for a high tibial osteotomy (HTO) to correct a varus deformity. During preoperative planning, the surgeon emphasizes the importance of maintaining normal sagittal plane alignment to avoid altering knee kinematics and cruciate ligament tension. The diagram below shows the relevant sagittal plane angles.
Which of the following sagittal plane angles represents the natural posterior slope of the tibial plateau, and what is its normal value?
Explanation
Correct Answer: C
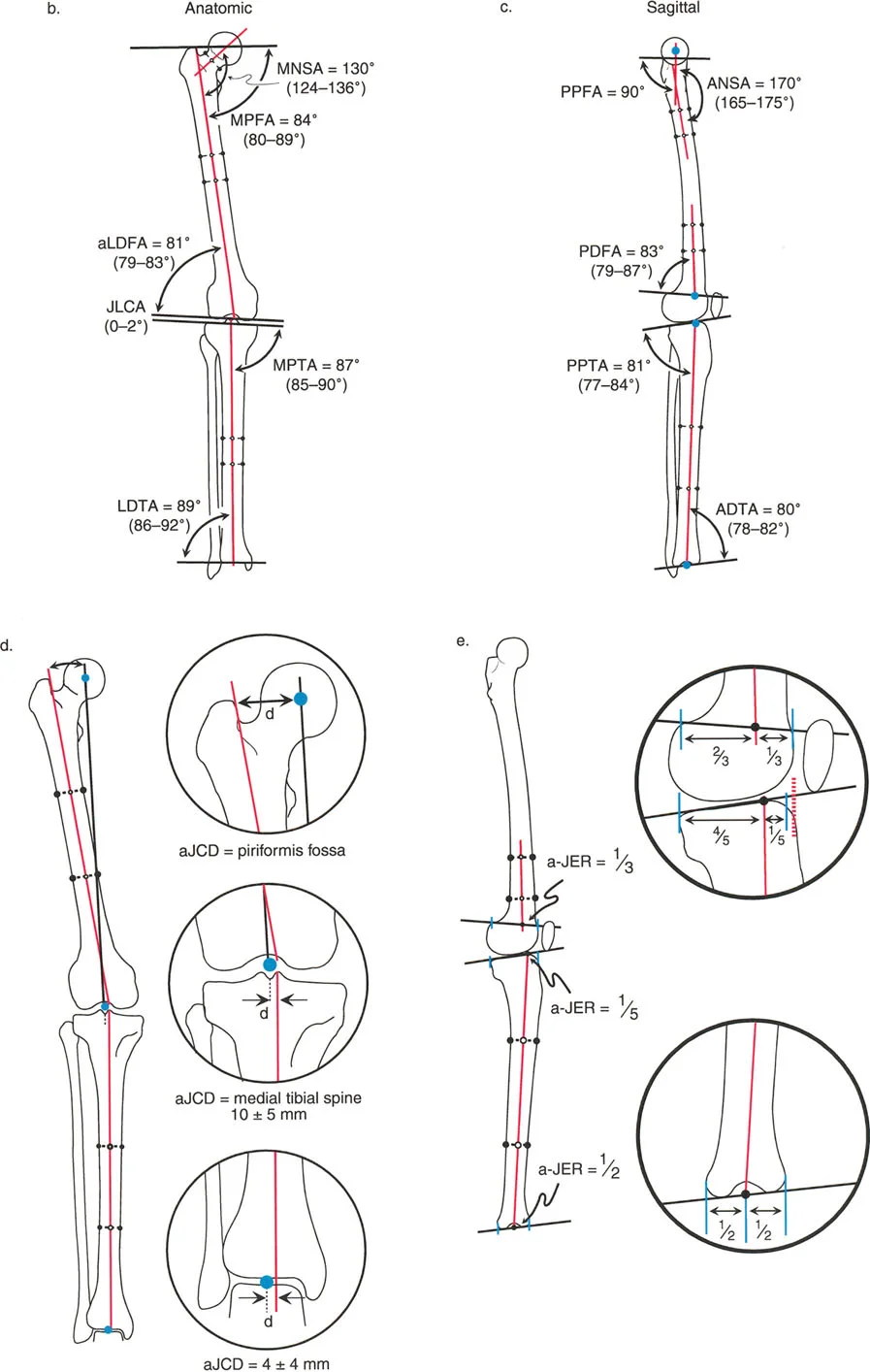
The case explicitly states that the Posterior Proximal Tibial Angle (PPTA) represents the natural posterior slope of the tibial plateau, and its normal value is 81° (range: 77–84°). Maintaining this angle is critical during HTO to avoid altering knee kinematics and cruciate ligament tension.
Option A (PDFA) is the Posterior Distal Femoral Angle, which is normally 83°, but it relates to the distal femur, not the proximal tibia.
Option B (PPFA) is the Posterior Proximal Femoral Angle, normally 90°, related to the proximal femur.
Option D (ADTA) is the Anterior Distal Tibial Angle, normally 80°, related to the distal tibia/ankle joint.
Option E (aJER) is the anatomic axis to joint edge ratio, which describes an intersection point, not an angle, and 1/5 is the ratio for the proximal tibia, but it's not the angle itself.
Question 15
A 40-year-old female presents with a severe valgus deformity of her right knee. A long-standing radiograph reveals an overall mechanical axis deviation lateral to the knee center. The surgeon measures the mLDFA and MPTA, finding both to be within normal limits. However, the medial aspect of the knee joint appears significantly widened on the radiograph, as shown conceptually in the alignment diagram below.
Based on these findings and Paley's principles, what is the most likely primary cause of this patient's valgus malalignment, and what is its normal value?
Explanation
Correct Answer: C
The case states that if a patient has a severe varus or valgus deformity, but the mLDFA and MPTA are normal, the deformity is intra-articular. A widened JLCA (Joint Line Convergence Angle) on the lateral side indicates lateral collateral ligament laxity or severe medial cartilage loss in a varus knee, and conversely, a widened medial JLCA indicates medial collateral ligament laxity or severe lateral cartilage loss in a valgus knee. The normal JLCA is 0–2°, meaning the distal femoral and proximal tibial joint lines should be nearly parallel. In this patient, normal mLDFA and MPTA with a severe valgus deformity and a significantly widened medial aspect of the knee joint strongly suggest an intra-articular deformity, specifically medial collateral ligament laxity, leading to an increased JLCA.
Options A and B are incorrect because the mLDFA and MPTA are stated to be within normal limits, ruling out primary femoral or tibial bony deformities.
Options D and E describe varus deformities, which contradict the patient's presentation of a valgus deformity.
Question 16
A junior resident is presenting a case of a distal femoral deformity and uses the term 'LDFA' without specifying a prefix. The attending surgeon asks for clarification, emphasizing the importance of precise terminology in deformity correction. The diagram below illustrates the concept of joint orientation.
According to Paley's rules for omitting prefixes, why is it crucial to always specify the prefix for the Distal Femoral Angle?
Explanation
Correct Answer: D
The case explicitly states, 'The ONLY time the prefix MUST be used is for the Distal Femoral Angle. Because the anatomic and mechanical axes of the femur diverge by about 7°, the mLDFA (88°) and aLDFA (81°) are vastly different, yet both are less than 90°. You must always specify mLDFA or aLDFA.'
Option A is incorrect; the mechanical and anatomic axes of the femur are NOT collinear; they diverge by about 7°.
Option B is incorrect; the normal values for mLDFA (88°) and aLDFA (81°) are different.
Option C is incorrect; the anatomic axis (aLDFA) is used, for example, during intramedullary nailing or when the full mechanical axis cannot be visualized.
Option E is incorrect; the 'less than 90 degrees' rule applies to the distal femur, but the unique aspect is that both the mechanical and anatomic angles are less than 90°, necessitating the prefix.
Question 17
A 28-year-old male sustains a comminuted mid-shaft femoral fracture. The orthopedic surgeon plans for intramedullary nailing and needs to identify the precise entry point for the nail relative to the proximal femur's anatomic axis. The diagram below shows the frontal plane joint orientation angles, which helps visualize the bone segments.
According to Paley's principles regarding anatomic axis intersection points (aJCD), where does the anatomic axis intersect the proximal femur?
Explanation
Correct Answer: C
The case states under 'Anatomic Axis to Joint Center Distance (aJCD)' that 'The anatomic axis intersects the proximal femur precisely at the piriformis fossa. This is why the piriformis fossa is the traditional starting point for straight antegrade femoral nails.'
Option A is incorrect; the mechanical axis connects to the center of the femoral head, but the anatomic axis intersects at the piriformis fossa.
Option B describes the intersection of the anatomic axis with the distal femur (knee joint line).
Option D describes the intersection of the anatomic axis with the proximal tibia (knee joint).
Option E describes the intersection of the anatomic axis with the distal tibia (ankle joint).
Question 18
A 16-year-old patient presents with a complex multi-planar tibial deformity, including significant procurvatum. During surgical planning, the surgeon needs to understand the sagittal plane relationship between the anatomic axis and the joint lines to accurately place osteotomies and guide wires. The diagram below illustrates the sagittal plane joint orientation angles.
According to Paley's principles regarding the Anatomic Axis to Joint Edge Ratio (aJER) in the sagittal plane, what is the intersection ratio for the proximal tibia and the distal tibia, respectively, measured from the anterior edge?
Explanation
Correct Answer: C
The case details the 'Anatomic Axis to Joint Edge Ratio (aJER)' in the sagittal plane:
- 'Proximal Tibia: The anatomic axis intersects the tibial plateau at an aJER of 1/5 (i.e., very anteriorly).'
- 'Distal Tibia: The anatomic axis intersects the ankle joint exactly in the middle, an aJER of 1/2.'
Therefore, the correct combination is Proximal Tibia: 1/5 and Distal Tibia: 1/2.
Options A, B, D, and E present incorrect combinations or values for the aJER of the proximal and distal tibia.
Question 19
A 70-year-old patient is undergoing a Total Knee Arthroplasty (TKA). The surgeon is using an intramedullary guide for the distal femoral cut. The diagram below shows the frontal plane joint orientation angles, which helps illustrate the relationship between different axes.
Based on Paley's '7-Degree Rule' and its application in TKA, what is the typical angular difference between the mechanical and anatomic axes of the femur, and how is this accounted for when using an intramedullary guide?
Explanation
Correct Answer: B
The case highlights 'The 7-Degree Rule': 'The difference between the mechanical and anatomic axes of the femur is typically 7° (range 5-9°). This is why a standard distal femoral cutting block in Total Knee Arthroplasty (TKA) is usually set to 5° or 7° of valgus—it is converting the anatomic axis (the intramedullary rod) into a mechanical axis cut perpendicular to the load-bearing line.'
Option A is incorrect; there is a significant difference between the two axes.
Option C is incorrect; the correction is typically in valgus, not varus, to achieve a perpendicular cut to the mechanical axis.
Option D is incorrect; the difference is 7°, not 15°.
Option E is incorrect; the difference is 7°, not 2°, and the correction is valgus, not varus.
Question 20
A 55-year-old male presents with a complex multi-planar deformity of his right lower limb following a previous trauma. The orthopedic surgeon initiates a systematic malalignment test to identify the source of the deformity and plan corrective osteotomies. The diagram below illustrates the overall lower limb alignment.
Which of the following sequences correctly represents the systematic malalignment test as described by Paley's principles, and what is the fundamental rule for performing an osteotomy at the CORA?
Explanation
Correct Answer: B
The case outlines the systematic malalignment test as follows:
- Measure the MAD: Is it medial (varus) or lateral (valgus)?
- Measure the mLDFA: Is the femur contributing to the deformity?
- Measure the MPTA: Is the tibia contributing to the deformity?
- Measure the JLCA: Is there ligamentous laxity or cartilage loss contributing to the deformity?
The fundamental rule of osteotomy (Paley's Rule 1) states: 'if an osteotomy is performed at the CORA, and the bone ends are angulated to correct the deformity, the mechanical axis will be perfectly restored without any translation.'
Option A is incorrect because the sequence is wrong, and the rule states 'without translation'.
Option C is incorrect because the sequence is wrong, and the rule states 'without translation'.
Option D is incorrect because the sequence is wrong, and the rule states 'without translation', not 'with rotation'.
Option E is incorrect because the sequence is wrong, and the rule states 'without translation', not 'with rotation'.
Question 21
A 45-year-old male is undergoing deformity correction for a malunited tibial shaft fracture. The surgeon plans an osteotomy at a site proximal to the center of rotation of angulation (CORA) due to poor skin quality over the apex. If the hinge is placed exactly at the CORA, what is the expected geometric outcome of the correction?
Explanation
Question 22
A surgeon is planning a deformity correction for a midshaft tibial varus malunion. If the osteotomy is made 4 cm proximal to the center of rotation of angulation (CORA) but the hinge is placed exactly on the CORA, what is the expected mechanical outcome?
Explanation
Question 23
A 65-year-old female presents for Total Knee Arthroplasty (TKA). She has a mid-diaphyseal femoral malunion with 25 degrees of varus deformity. Which of the following is the most appropriate management to achieve a stable, aligned knee?
Explanation
Question 24
During the preoperative radiographic assessment for a complex varus knee deformity using Paley's malalignment test, the Joint Line Convergence Angle (JLCA) is measured at 6 degrees (open laterally). What does this most likely indicate?
Explanation
Question 25
A 40-year-old male with chronic posterolateral corner (PLC) and PCL deficiency presents with varus malalignment. He is planned for an opening wedge high tibial osteotomy (HTO). How should the sagittal plane be managed during the osteotomy?
Explanation
Question 26
You are performing a corticotomy for tibial lengthening using a circular frame. What is the primary biological rationale for observing a 5 to 7-day latent period prior to initiating distraction?
Explanation
Question 27
During preoperative planning for a TKA in a patient with an accentuated lateral femoral bow, you note an abnormally large anatomic-mechanical angle (AMA) of the femur. How does an increased femoral bow typically alter the standard distal femoral cut if referencing the intramedullary axis?
Explanation
Question 28
A patient requires correction of a distal femoral valgus deformity. The surgeon plans an osteotomy distal to the CORA and places the hinge axis at the osteotomy site rather than the CORA. What is the expected mechanical outcome according to Paley's principles?
Explanation
Question 29
A 65-year-old male undergoes TKA 15 years after a closing wedge high tibial osteotomy. He now has severe patella baja. Which of the following technical modifications is most appropriate to prevent patellar tendon avulsion during surgical exposure?
Explanation
Question 30
When utilizing Paley's malalignment test on full-length weight-bearing radiographs, an abnormality in which of the following standard angles definitively localizes a deformity to the distal femur in the coronal plane?
Explanation
Question 31
In a type II valgus knee (with attenuated medial collateral ligament) undergoing TKA, what is the most appropriate component constraint if a lateral release leaves the knee unbalanced in flexion and extension?
Explanation
Question 32
A patient with osteoarthritis and a 15-degree varus deformity presents for TKA. Preoperative templating reveals an mPTA of 80 degrees and an mLDFA of 88 degrees. To achieve a neutral mechanical axis while restoring parallel joint lines, which technique is most appropriate?
Explanation
Question 33
In evaluating a patient with severe bowing of the tibia, two separate diaphyseal CORAs are identified. Which of the following frame constructs is mechanically optimal for simultaneous correction of both deformities without inducing secondary translation?
Explanation
Question 34
During a TKA, the surgeon inadvertently cuts the proximal tibia with 15 degrees of posterior slope. What is the most likely biomechanical consequence of this error?
Explanation
Question 35
A 16-year-old with a 12-degree distal femoral valgus deformity undergoes a medial closing wedge distal femoral osteotomy (DFO). Where should the anatomical hinge point be located to optimize bone healing and prevent unwanted translation?
Explanation
Question 36
A 45-year-old male presents with a midshaft tibial malunion. Deformity planning identifies the Center of Rotation of Angulation (CORA) at the fracture site. The surgeon plans an osteotomy at the proximal metaphysis to optimize bone healing, but sets the Axis of Correction of Angulation (ACA) at the CORA. According to Paley's principles (Rule 2), what will be the resulting alignment?
Explanation
Question 37
During Total Knee Arthroplasty (TKA) on a patient with a significant diaphyseal anterior bow of the femur, a standard long intramedullary alignment guide is utilized. If the anterior bow is not properly accounted for, what is the most likely consequence for the femoral component alignment?
Explanation
Question 38
A 68-year-old female with severe rheumatoid arthritis presents for TKA. Radiographs demonstrate a 25-degree valgus deformity. On clinical examination, there is a fixed valgus contracture, and the medial collateral ligament (MCL) is completely incompetent and attenuated (Krackow Type II). Which of the following implant choices is most appropriate?
Explanation
Question 39
In the assessment of a lower limb deformity, the Joint Line Congruency Angle (JLCA) is measured. What does an abnormally increased JLCA (>2 degrees) on standing radiographs most commonly indicate?
Explanation
Question 40
A 55-year-old male is undergoing TKA 15 years after a previous opening wedge High Tibial Osteotomy (HTO). Which of the following technical challenges is most specifically anticipated as a direct consequence of the prior opening wedge HTO?
Explanation
Question 41
A 22-year-old female undergoes cosmetic bilateral femoral lengthening using an intramedullary lengthening nail. The lengthening is performed exactly along the anatomical axis of the femur. Without additional surgical modifications, what is the expected effect on the mechanical axis of the lower limb?
Explanation
Question 42
In preparing the distal femur during a TKA for a severe fixed valgus deformity (15 degrees), the surgeon decides to set femoral rotation. If the posterior condylar axis is solely relied upon for referencing, what alignment error is most likely to occur?
Explanation
Question 43
A surgeon is planning a single-level correction for a multi-apical tibial deformity. According to Paley's principles, if a single osteotomy is performed to correct two separate CORAs, what is the unavoidable geometric consequence?
Explanation
Question 44
When evaluating a standing full-length radiograph for lower limb alignment, what is the generally accepted normal value for the mechanical lateral distal femoral angle (mLDFA)?
Explanation
Question 45
A 60-year-old male with end-stage knee osteoarthritis presents with an extra-articular diaphyseal varus deformity of the femur following a prior fracture. The deformity is located 10 cm proximal to the joint line. At what degree of coronal plane angulation is a simultaneous or staged extra-articular corrective osteotomy typically recommended prior to or during TKA?
Explanation
Question 46
A patient presents with a symptomatic knee hyperextension gait following non-operative management of a proximal third tibia fracture. Radiographs reveal a normal mMPTA. Which of the following sagittal plane angles is most likely abnormal, confirming the osseous nature of the recurvatum?
Explanation
Question 47
During a TKA for a severe varus deformity with a tight medial compartment, sequential soft tissue releases are required to balance the knee in extension. What is the standard correct sequence of medial release?
Explanation
Question 48
According to Paley's Rule 3 of deformity correction, if an osteotomy is performed outside the CORA and the ACA is also placed outside the CORA, what is the resulting alignment of the mechanical axes?
Explanation
Question 49
A 16-year-old female undergoes a distal femoral lateral opening wedge osteotomy to correct a symptomatic genu valgum. To ensure stability and prevent unwanted coronal translation during the opening process, where MUST the bone hinge be preserved?
Explanation
Question 50
In a patient with a retained femoral diaphyseal intramedullary nail and severe end-stage osteoarthritis of the knee, TKA is planned. What is the primary advantage of utilizing computer navigation or robotic assistance in this specific scenario?
Explanation
Question 51
A 40-year-old male presents with advanced medial compartment osteoarthritis and a mechanical axis deviation (MAD) of 25mm medial to the knee center. Radiographic analysis shows an mLDFA of 94 degrees and an mMPTA of 87 degrees. What is the primary source of the deformity?
Explanation
Question 52
During TKA utilizing standard extramedullary tibial alignment guides, a patient is noted to have excessive anterior bowing of the tibial shaft. If the surgeon aligns the extramedullary guide parallel to the anterior tibial crest without fluoroscopic verification, what error is most likely to occur in the tibial bone cut?
Explanation
Question 53
A 10-year-old child with severe infantile Blount's disease is being evaluated for a proximal tibial osteotomy. In addition to varus angulation, what other multi-planar deformity components are classically present in the proximal tibia of this patient?
Explanation
Question 54
When planning correction with a Taylor Spatial Frame (TSF) for a complex multi-planar lower limb deformity, the software requires the input of 'mounting parameters'. Which of the following accurately describes what these parameters define?
Explanation
Question 55
A surgeon is evaluating a 55-year-old patient for a TKA. The patient has a severe extra-articular varus deformity of the proximal tibia. According to Wolff and Paley's recommendations for TKA in the setting of extra-articular deformity, an intra-articular compensatory cut becomes absolutely contraindicated (mandating an osteotomy) when the theoretical cut does what?
Explanation
Question 56
A 65-year-old male with knee osteoarthritis and an old midshaft femur fracture malunion is being evaluated for a total knee arthroplasty (TKA). When assessing if his extra-articular diaphyseal femoral varus deformity can be managed strictly with an intra-articular bone resection during TKA, which of the following radiographic findings best confirms that an intra-articular correction is feasible without compromising collateral ligaments?
Explanation
Question 57
According to Paley's rules for deformity correction, if an osteotomy is performed at a level different from the center of rotation of angulation (CORA), but the hinge (axis of correction) is placed exactly at the CORA, what is the expected outcome?
Explanation
Question 58
A 45-year-old female presents with medial compartment osteoarthritis and genu varum. Preoperative long-leg standing radiographs reveal a mechanical axis deviation (MAD) of 25 mm medial to the knee center. Her joint line convergence angle (JLCA) is 2 degrees. The mechanical lateral distal femoral angle (mLDFA) is 87 degrees. What is the most likely mechanical medial proximal tibial angle (mMPTA)?
Explanation
Question 59
A 50-year-old male presents with severe genu valgum. The standing long-leg radiograph shows a lateral mechanical axis deviation. The mLDFA is 82 degrees, mMPTA is 87 degrees, and JLCA is 7 degrees (medial opening). What is the primary contributor to the high JLCA in this clinical scenario?
Explanation
Question 60
During conventional TKA using an intramedullary femoral alignment guide, a patient is noted to have significant excessive anterior bowing of the femoral diaphysis. If the distal femoral cut is made using the standard intramedullary rod without compensation, what sagittal plane error is most likely to occur?
Explanation
Question 61
When evaluating the sagittal plane alignment of the tibia for deformity correction or high tibial osteotomy (HTO), the posterior proximal tibial angle (PPTA) is routinely measured. What is the generally accepted normal value for the anatomic PPTA?
Explanation
Question 62
A 68-year-old female with primary osteoarthritis and a severely lateral bowed femur is undergoing TKA. How should the surgeon alter the entry point for the intramedullary alignment rod to ensure a perpendicular distal femoral cut relative to the mechanical axis?
Explanation
Question 63
A surgeon performs a medial opening wedge high tibial osteotomy (HTO) for a varus knee. If the anterior osteotomy gap is inadvertently opened significantly more than the posteromedial gap, what is the expected change to the proximal tibia?
Explanation
Question 64
A patient presents with a severe post-traumatic multi-apical tibial deformity. According to Paley's Rule 3, if the surgeon chooses to correct this with a single osteotomy and places both the osteotomy and the hinge at a level that does NOT correspond to either CORA, what will be the result if the angular deformity is corrected?
Explanation
Question 65
A 42-year-old male has severe genu varum with a mechanical axis deviation (MAD) of 45 mm medial to the knee. His mLDFA is 95 degrees, mMPTA is 79 degrees, and JLCA is 2 degrees. What is the most appropriate surgical management for this patient to normalize alignment and prevent excessive joint line obliquity?
Explanation
None
