ABOS Part I Orthopaedic Review: TKA Revision & Hallux Valgus Surgical Management | Part 21607

Key Takeaway
This ABOS Part I Orthopaedic Review module provides 20 advanced MCQs for ABOS Part I and AAOS OITE exams. It covers critical topics in Total Knee Arthroplasty (TKA) Revision, such as aseptic loosening and bone loss, and comprehensive Hallux Valgus surgical management, including osteotomies and complication strategies, derived from high-yield clinical cases.
ABOS Part I Orthopaedic Review: TKA Revision & Hallux Valgus Surgical Management | Part 21607
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
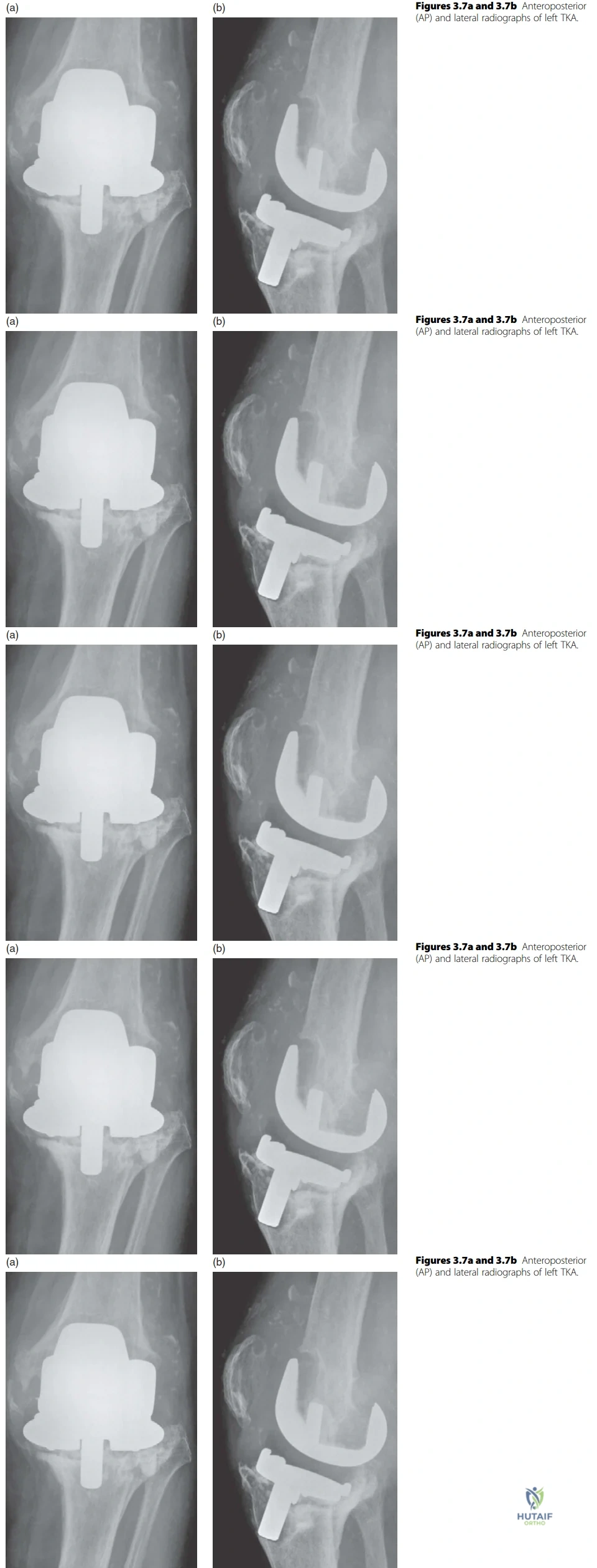
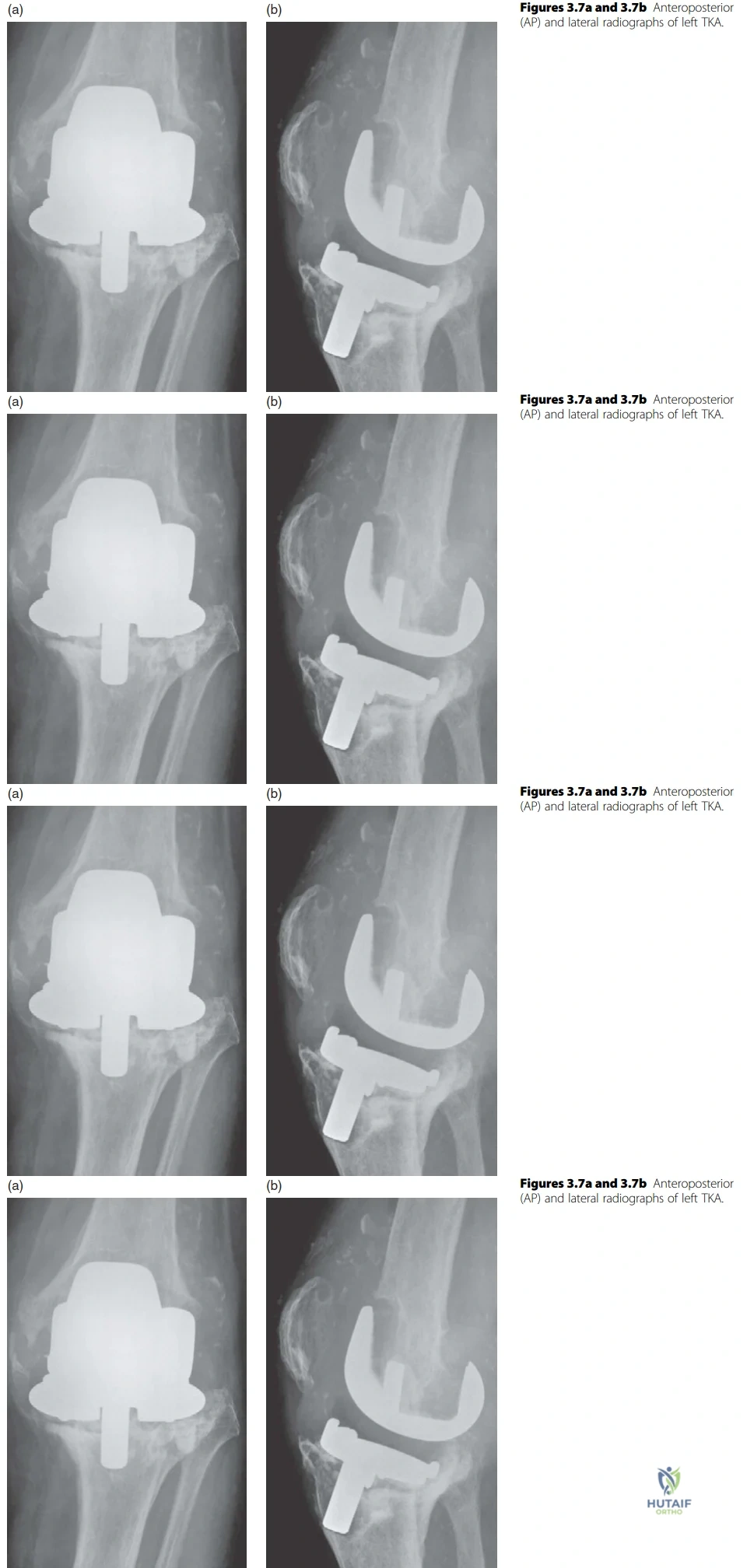
A 65-year-old patient presents with increasing pain and instability in their left knee, 10 years after a primary total knee arthroplasty. The provided radiographs are shown.
Explanation
Correct Answer: C
The radiographs clearly demonstrate widespread lucency around both the femoral and tibial components, indicating loss of fixation. There is significant subsidence of the tibial component and extensive osteolysis, particularly in the proximal tibia and distal femur. These findings are classic for aseptic loosening. While periprosthetic joint infection (PJI) is always in the differential for a painful TKA, the radiographic findings alone are more definitively characteristic of aseptic loosening and associated bone loss. There is no clear evidence of a periprosthetic fracture, and the extent of loosening and osteolysis goes beyond early polyethylene wear or isolated patellar issues.
Question 2
A 72-year-old patient presents with a painful left total knee arthroplasty. Radiographs are provided. The surgeon notes extensive bone loss involving a major portion of both the distal femoral condyles and the proximal tibial plateau, requiring significant augmentation and likely long-stemmed components.
Explanation
Correct Answer: C
The Anderson Orthopaedic Research Institute (AORI) classification for bone loss is crucial in revision TKA planning. Type 1 involves intact metaphyseal bone with minor defects. Type 2 involves damaged metaphyseal bone with loss of cancellous bone, categorized as 2A (one condyle/plateau) or 2B (both condyles/plateaux). Type 3 describes deficient metaphyseal bone where bone loss comprises a major portion of either condyle or plateau, often associated with ligament detachment and requiring long-stemmed implants, bone grafts, or custom prostheses. The case description explicitly states "extensive bone loss involving a major portion of both the distal femoral condyles and the proximal tibial plateau," which directly corresponds to AORI Type 3 for both the femur and tibia. The radiographs support this with widespread osteolysis and significant bone defects.
Question 3
Following the diagnosis of aseptic loosening, the candidate expresses concern about the state of the collateral ligaments, particularly the MCL, and the extensive bone loss. The patient is planned for revision surgery.
Explanation
Correct Answer: C
The case explicitly states, "The collateral ligaments are likely to be dysfunctional and especially the MCL therefore a constrained knee replacement may be required." The constraint ladder for knee implants progresses from PCL retaining (CR) to PCL substituting (PS), then to unlinked constrained condylar (VVC), and finally to linked, constrained condylar (RHK). A VVC implant, such as an LCCK or TC3, is specifically designed to provide anteroposterior and varus-valgus stability, substituting for deficient collateral ligaments. While an RHK (Linked, Constrained Condylar) is used for global instability or severe bone loss/fracture, the primary concern highlighted is dysfunctional collateral ligaments, making VVC the most appropriate initial step up in constraint for this specific issue. CR and PS designs do not adequately address significant collateral ligament insufficiency.
Question 4
The patient, described as "reasonably young," has extensive bone loss around the failed total knee replacement. The surgeon is planning the revision procedure.
Explanation
Correct Answer: C
The case explicitly states, "In this patient who is reasonably young restoration of bone stock is preferable, because of likelihood of further revision surgery." For younger patients with extensive bone loss, preserving and restoring bone stock is paramount to facilitate potential future revisions. This is best achieved through the use of bone grafting (structural or morselized) and/or modular metaphyseal sleeves, which allow for biological ingrowth and reconstruction of the metaphyseal bone. While cement, modular augments, or even hinged prostheses can address defects, they do not primarily restore bone stock. Avoiding complex bone grafting for the sake of surgical time would compromise the long-term outcome and future revision potential in a young patient.
Question 5
The lateral radiograph of the failed total knee replacement clearly demonstrates anterior femoral cortical notching.
Explanation
Correct Answer: C
Anterior femoral cortical notching is a well-recognized complication of total knee arthroplasty, typically resulting from over-resection of the distal femur or improper sizing of the femoral component during the primary surgery. This notching creates a stress riser in the anterior femoral cortex, significantly weakening the bone and increasing the risk of a supracondylar periprosthetic femoral fracture, especially with minor trauma. It is not directly indicative of infection, polyethylene wear, or PCL insufficiency, nor is it a benign finding.
Question 6
The candidate initially suggests that the radiographs are "suggestive of infection until proven otherwise," despite the examiner later confirming aseptic loosening.

Explanation
Correct Answer: A
In the initial workup of a painful total knee arthroplasty, differentiating between aseptic loosening and periprosthetic joint infection (PJI) is critical. Elevated inflammatory markers such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are highly sensitive indicators of PJI. While not definitive on their own, they are the most indicative of infection among the given options. A continuous radiolucent line greater than 2mm and progressive component subsidence are classic radiographic signs of aseptic loosening. Pain with activity that improves with rest is a common symptom of mechanical loosening. Anterior femoral cortical notching is a technical complication related to fracture risk, not directly to infection.
Question 7
The examiner asks about the advantages of PCL substituting (PS) over PCL retaining (CR) designs.
Explanation
Correct Answer: C
The case explicitly lists several advantages of PCL substituting (PS) designs over PCL retaining (CR) designs. These include: conforming surfaces allowing roll-back, no component slide, providing a degree of VVC (varus-valgus constraint), and the cam-post mechanism improving anterior-posterior stability. PS designs also facilitate deformity correction, use more congruent joint surfaces (reducing wear), offer better range of motion, and are often considered technically easier and more reproducible. Options A and B are generally associated with CR designs (PCL preservation potentially leading to less bone resection and more natural kinematics), while options D and E are not recognized advantages of PS designs; in fact, PS designs can sometimes have specific patellofemoral issues related to the box cut, and are generally considered technically simpler than CR in terms of balancing.
Question 8
The patient has extensive bone loss, concerns about collateral ligament integrity, and calcified soft tissues. The surgeon is planning a single-stage revision.
Explanation
Correct Answer: C
The candidate in the case explicitly states, "The soft tissues appear contracted and calcified which may lead to wound complications." This highlights a critical concern for revision surgery, where soft tissue quality is often compromised. Meticulous soft tissue management, including careful dissection, debridement, and thoughtful wound closure techniques, is essential to minimize the risk of wound complications, infection, and skin necrosis. A standard primary TKA system would be inadequate for extensive bone loss and ligamentous instability. A minimally invasive approach is generally not suitable for complex revisions with significant bone loss and soft tissue issues. Avoiding stemmed components would compromise stability and fixation in the presence of extensive bone loss. Relying solely on cement fixation might not be sufficient for severe bone defects, especially in a young patient where bone ingrowth is desired for long-term stability.
Question 9
The radiographs demonstrate calcification of soft tissues, including the popliteal vessels.
Explanation
Correct Answer: C
The presence of soft tissue calcification, particularly involving the popliteal vessels, is a significant finding. The candidate in the case notes that "The soft tissues appear contracted and calcified which may lead to wound complications." Beyond wound complications, calcification of major vessels like the popliteal artery increases the risk of intraoperative vascular injury during dissection, especially in a revision setting with distorted anatomy. It also suggests underlying peripheral vascular disease, which can impair wound healing and increase the risk of other postoperative complications. While heterotopic ossification is a possibility, the immediate and most critical concern for surgical planning relates to vascular integrity and wound healing.
Question 10
The patient is described as "reasonably young" with extensive bone loss, and the examiner emphasizes the importance of long-term planning.
Explanation
Correct Answer: C
The case explicitly states, "In this patient who is reasonably young restoration of bone stock is preferable, because of likelihood of further revision surgery." For younger patients, the expectation of a longer lifespan means a higher probability of requiring additional revision surgeries in the future. Therefore, the primary long-term goal in the current revision is to preserve and, if possible, restore the existing bone stock. This approach ensures that there is adequate bone available for subsequent procedures, making future revisions technically feasible and potentially more successful. While range of motion, cost, and hospital stay are important, they are secondary to the fundamental goal of bone stock management in a young patient with extensive defects. An RHK is not indicated in all cases of extensive bone loss; the choice depends on the specific type of instability and bone defect.
Question 11
A 65-year-old lady presents with bilateral hallux valgus. You obtain weight-bearing radiographs. Based on the provided AP radiograph of the right foot, which of the following findings is most consistent with the described deformity (intermetatarsal angle 15°, hallux valgus angle 35°, and minimal passive correction)?

Explanation
Correct Answer: C
The case describes a significant hallux valgus deformity with an intermetatarsal angle of 15° (normal < 9°) and a hallux valgus angle of 35° (normal < 15°). These severe angular deformities are typically associated with significant lateral subluxation of the sesamoid complex, which is a hallmark of first metatarsal pronation and hallux valgus progression. The AP radiograph (Figure 4.7) would visually confirm this lateral displacement of the sesamoids relative to the first metatarsal head.
Option A (Normal sesamoid position) is incorrect because severe hallux valgus invariably involves sesamoid subluxation.
Option B (Medial sesamoid subluxation) is incorrect; sesamoid subluxation in hallux valgus is typically lateral.
Option D (Widening of the first metatarsophalangeal joint space) is generally not seen in hallux valgus; rather, joint space narrowing might indicate arthritic changes, or the joint space might appear normal or slightly compressed laterally.
Option E (Absence of arthritic changes) is not guaranteed. While the case doesn't explicitly state arthritic changes on the right foot, a long-standing deformity of this magnitude often has some degree of degenerative change, and the question asks for the finding most consistent with the described deformity, which is primarily angular and rotational, leading to sesamoid subluxation.
Question 12
For the 65-year-old lady with an intermetatarsal angle of 15°, a hallux valgus angle of 35°, and minimal passive correction of the hallux on her right foot, assuming a normal first tarsometatarsal joint, what is the most appropriate surgical plan?
Explanation
Correct Answer: C
The case explicitly states that for an intermetatarsal angle of 15° and a hallux valgus angle of 35° with minimal passive correction, the candidate would plan a scarf osteotomy combined with a lateral release and an Akin osteotomy of the proximal phalanx if necessary. This combination addresses the severe intermetatarsal angle, the significant hallux valgus angle, and the lack of passive correction. The Scarf osteotomy is chosen for its versatility and ability to achieve substantial correction without significant shortening, which is crucial for severe deformities.
Option A (Chevron osteotomy) is typically reserved for mild to moderate deformities (IM angle < 13-15°, HV angle < 30-35°) and would likely be inadequate for the described severe deformity.
Option B (Mitchell osteotomy) is also a distal osteotomy and, as mentioned in the case, produces shortening of the first metatarsal, which could lead to transfer metatarsalgia, making it less desirable for severe corrections.
Option D (First metatarsophalangeal joint arthrodesis) is a salvage procedure or indicated for severe arthritis, recurrent deformity, or in specific cases like the patient's left foot with a missing second toe, but not as a primary procedure for a correctable deformity with a normal TMT joint.
Option E (Keller resection arthroplasty) is generally reserved for elderly, low-demand patients with significant MTP joint arthritis and is associated with complications like hallux cock-up deformity and loss of push-off strength, making it less suitable for this active patient with a correctable deformity.
Question 13
Following the decision to perform a Scarf osteotomy for the patient's right foot, the examiner asks why this procedure was chosen over simpler distal osteotomies. Which of the following is the most compelling reason for selecting a Scarf osteotomy in this specific case?
Explanation
Correct Answer: C
The case explicitly states the advantages of a Scarf osteotomy: 'It is a very versatile procedure with stable fixation allowing postoperative mobilization without a cast. It maintains length of the metatarsal but allows translation, angulation and depression of the metatarsal head as necessary. It can also be used to shorten or even lengthen the metatarsal.' The candidate further explains that for the described degree of deformity (IM 15°, HV 35°) and lack of passive correction, a distal osteotomy would provide inadequate correction, and a Mitchell osteotomy specifically produces shortening, which could lead to transfer metatarsalgia. Therefore, the Scarf's versatility in achieving greater correction while maintaining metatarsal length is the key advantage.
Option A (Simpler procedure with faster recovery) is incorrect. Scarf osteotomy is a more complex procedure than distal osteotomies, though it does allow early weightbearing due to stable fixation.
Option B (Primarily addresses metatarsal shortening) is incorrect. Scarf osteotomy maintains metatarsal length and can even lengthen it, which is an advantage over procedures like Mitchell that cause shortening. Shortening is generally undesirable as it can lead to transfer metatarsalgia.
Option D (Less stable fixation) is incorrect. The case states it provides 'stable fixation allowing postoperative mobilization without a cast.'
Option E (Only osteotomy that can be combined with an Akin) is incorrect. An Akin osteotomy is a proximal phalangeal osteotomy and can be combined with various metatarsal osteotomies to address residual hallux valgus interphalangeus.
Question 14
When discussing the proposed Scarf osteotomy with the patient, which of the following complications is specifically mentioned in the case as a potential risk that is difficult to treat?
Explanation
Correct Answer: D
The candidate explicitly states, 'I would mention the possibility of hallux varus as a complication as this is difficult to treat.' This directly answers the question.
Option A (Superficial infection) is mentioned as a risk, but not specifically highlighted as 'difficult to treat' in the same context as hallux varus.
Option B (Recurrence of the deformity) is mentioned as possible, especially in adolescent cases, but not described as 'difficult to treat' in the same way as hallux varus.
Option C (Significant stiffness of the MTP joint) is mentioned as a possibility for a minority of patients, but again, not characterized as 'difficult to treat' in the same manner as hallux varus.
Option E (Intraoperative metatarsal fracture) is mentioned as a possibility, but it's an acute intraoperative event, not a chronic post-operative complication described as 'difficult to treat' in the long term.
Question 15
A few months post-Scarf osteotomy, the patient develops a flexible hallux varus deformity. Which of the following is the most appropriate initial management strategy for this complication, as discussed in the case?
Explanation
Correct Answer: D
The case states, 'A subtle varus may improve as the patient returns to normal foot wear.' This indicates that for a flexible or subtle varus, initial non-operative management with observation and appropriate footwear is the first step. The case then describes soft tissue procedures (EHL slip transfer, abductor hallucis and medial capsular release) for flexible deformity, and arthrodesis for significant stiffness or arthrosis. Since the question specifies a 'flexible' deformity, the initial approach would be the least invasive.
Option A (Immediate revision surgery with MTP joint arthrodesis) is incorrect. Arthrodesis is reserved for significant stiffness or arthrosis, not for a flexible deformity, especially as an initial step.
Option B (Transfer of a slip of the Extensor Hallucis Longus (EHL) tendon) and Option C (Abductor hallucis and medial capsular release) are soft tissue procedures described for flexible deformity, but they would typically follow initial conservative measures if the varus does not resolve with footwear changes.
Option E (Resection of the medial eminence and lateral capsular plication) is a procedure for hallux valgus, not hallux varus. Hallux varus involves the hallux deviating medially, so a lateral capsular plication would worsen it, and medial eminence resection is for the bunion deformity.
Question 16
After successful treatment of the right foot, the patient's left foot, which previously underwent second toe removal and has recurrent hallux valgus symptoms, requires surgical intervention. Considering the oblique view of the left foot and the patient's history, what is the most appropriate surgical recommendation for the left hallux?

Explanation
Correct Answer: C
The case explicitly addresses this scenario: 'So you have successfully treated this lady’s right foot and she is pleased with the result. Would you go ahead and do the same on the left? CANDIDATE: No. The absence of the second toe predisposes to recurrence and I would propose arthrodesis of the hallux MTP joint.' The absence of the second toe significantly alters the biomechanics of the forefoot, increasing the risk of recurrence with traditional hallux valgus correction procedures. Arthrodesis provides a stable, definitive correction in such complex cases.
Option A (Repeat Scarf osteotomy) is incorrect because the case specifically advises against repeating the same procedure due to the altered anatomy and high recurrence risk.
Option B (Chevron osteotomy) is a less powerful osteotomy and would also be prone to recurrence in this setting.
Option D (Proximal phalangeal osteotomy (Akin) alone) only addresses the hallux valgus interphalangeus component and would be insufficient for the overall hallux valgus deformity, especially with the added complexity of a missing second toe.
Option E (Resection arthroplasty) is generally reserved for very low-demand patients or those with severe arthritis and is associated with significant functional limitations and potential for hallux cock-up deformity, making arthrodesis a more reliable option for stability and function in this context.
Question 17
During the physical examination for hallux valgus, the candidate outlines several key assessment points. Which of the following is NOT explicitly mentioned as a component of the physical examination in the case discussion?
Explanation
Correct Answer: D
The candidate's description of the physical examination includes: 'I would examine the gait and the posture of the weighted foot... I would palpate for areas of tenderness, paying particular attention to the hallux MTP joint and lesser metatarsal heads. I would assess the degree of active and passive correction possible and the range of movement of the involved joints and look for gastrocnemius tightness. I would also perform a grind test to assess pain from loading the MTP joint. Neurovascular status must also be assessed.'
While 'gastrocnemius tightness' is mentioned, which involves the ankle, a general 'assessment of ankle range of motion' beyond this specific test is not explicitly listed as a primary component of the hallux valgus examination in the provided text. The 'range of movement of the involved joints' refers specifically to the hallux MTP and first TMT joints.
Options A, B, C, and E are all explicitly mentioned in the candidate's detailed description of the physical examination.
Question 18
The examiner asks about the normal range of key radiographic angles in hallux valgus. Based on the AP radiograph and the case discussion, which statement accurately describes the normal values for the intermetatarsal angle (IMA), hallux valgus angle (HVA), and distal metatarsal articular angle (DMAA)?
Explanation
Correct Answer: B
The case explicitly states the normal ranges for these angles: 'The intermetatarsal angle is normally less than 9. The hallux valgus angle should be less than 15. The distal metatarsal articular angle is normally a maximum of 15 from perpendicular to the axis of the first metatarsal.'
Options A, C, D, and E present incorrect combinations or values for the normal ranges as stated in the case.
Question 19
The candidate emphasizes obtaining a detailed history, including questioning about relevant conditions. Which of the following conditions is NOT specifically mentioned in the case as a relevant condition to inquire about during the history for a patient presenting with hallux valgus?
Explanation
Correct Answer: D
The candidate states: 'I would complete the history, including questioning about relevant conditions such as diabetes, inflammatory arthritis, vascular disease and neuropathy...'
Options A, B, C, and E are all explicitly mentioned in the case as relevant conditions to inquire about during the history.
Option D (Gout) is a common condition that can affect the MTP joint and mimic or exacerbate hallux valgus symptoms, and would typically be part of a comprehensive history. However, it is not explicitly listed in the specific conditions mentioned by the candidate in this teaching case, making it the correct answer to the question 'NOT specifically mentioned'.
Question 20
The candidate describes securing the Scarf osteotomy with two headless compression screws. Which of the following statements accurately describes a key mechanical advantage or characteristic of the Scarf osteotomy, as discussed in the case?
Explanation
Correct Answer: D
The case describes the Scarf osteotomy as 'a very versatile procedure with stable fixation allowing postoperative mobilization without a cast. It maintains length of the metatarsal but allows translation, angulation and depression of the metatarsal head as necessary. It can also be used to shorten or even lengthen the metatarsal.'
Option A (Primarily achieves correction through shortening) is incorrect. The case emphasizes that it 'maintains length' and avoids the shortening seen with procedures like Mitchell osteotomy.
Option B (Simple distal osteotomy, limiting application to mild deformities) is incorrect. The case highlights its versatility and suitability for more severe deformities, contrasting it with distal osteotomies that would be 'inadequate' for the described deformity.
Option C (Provides unstable fixation, necessitating prolonged cast immobilization) is incorrect. The case states it provides 'stable fixation allowing postoperative mobilization without a cast.'
Option E (Its main benefit is the ability to lengthen the first metatarsal without affecting other planes of correction) is partially correct in that it can lengthen, but the primary benefit highlighted is its versatility in allowing translation, angulation, and depression while maintaining length, which is a more comprehensive description of its advantages for correction.
Question 21
In revision total knee arthroplasty, restoring the joint line is critical for proper kinematics. Which of the following landmarks is most accurate for estimating the anatomic joint line?
Explanation
Question 22
A 68-year-old female undergoes revision TKA for aseptic loosening. Intraoperatively, the surgeon notes complete incompetence of the medial collateral ligament (MCL). Which of the following constraint levels is definitively indicated?
Explanation
Question 23
A patient presents with a painful, rigid hallux varus deformity 1 year after a distal chevron osteotomy and lateral soft tissue release for hallux valgus. What is the most likely iatrogenic cause?
Explanation
Question 24
According to the Anderson Orthopaedic Research Institute (AORI) classification, what characterizes a Type III bone defect in revision TKA?
Explanation
Question 25
A 45-year-old female presents with severe hallux valgus, an intermetatarsal angle of 18 degrees, and obvious hypermobility of the first tarsometatarsal (TMT) joint. Which of the following is the most appropriate surgical intervention?
Explanation
Question 26
During a revision TKA, the surgeon notes that the flexion gap is extremely tight, but the extension gap is perfectly balanced. Which of the following is the most appropriate corrective step?
Explanation
Question 27
A patient has a hallux valgus deformity with a distal metatarsal articular angle (DMAA) of 20 degrees. Which of the following procedures is most appropriate to correct this specific angular deformity?
Explanation
Question 28
In revision TKA, long diaphyseal engaging stems are frequently used to achieve stable implant fixation. According to the zonal fixation concept, in which zone do these stems primarily function?
Explanation
Question 29
When performing a distal metatarsal osteotomy for hallux valgus correction, carefully preserving the soft tissue attachments in which specific area minimizes the risk of avascular necrosis of the metatarsal head?
Explanation
Question 30
A patient presents with a chronic patellar tendon rupture 3 years after a primary TKA, demonstrating an active extension lag of 40 degrees. What is currently considered the most reliable surgical reconstruction method?
Explanation
Question 31
A surgeon performs a distal chevron osteotomy for hallux valgus. Intraoperatively, after fully correcting the intermetatarsal angle, the hallux remains in clinical valgus due to an intrinsic deformity within the proximal phalanx. Which procedure should be added?
Explanation
Question 32
When extracting a well-fixed cementless porous-coated femoral component during a revision TKA, which technique is most highly recommended to minimize catastrophic femoral bone loss?
Explanation
Question 33
What is the ideal targeted position for an arthrodesis of the first metatarsophalangeal (MTP) joint to optimize postoperative gait?
Explanation
Question 34
A patient requires a revision TKA with significant uncontained metaphyseal bone defects but an intact diaphysis. The surgeon opts for highly porous tantalum cones. What is the primary biomechanical and biologic advantage of these cones in this setting?
Explanation
Question 35
During a revision total knee arthroplasty, the surgeon inadvertently elevates the joint line by 12 mm while attempting to balance the flexion and extension gaps. Which of the following is the most likely clinical consequence of this technical error?
Explanation
Question 36
A 68-year-old female undergoes a distal chevron osteotomy with a lateral soft tissue release for hallux valgus. Postoperatively, she develops avascular necrosis (AVN) of the first metatarsal head. Which of the following anatomical structures was most likely compromised?
Explanation
Question 37
A 71-year-old patient presents with a painful, loose primary total knee arthroplasty.
Intraoperatively, the surgeon notes AORI Type III bone loss on both the femur and tibia, with complete incompetence of the medial collateral ligament. Which of the following implant constraints is most appropriate?
Explanation
Question 38
A 45-year-old female presents with severe bunion pain. Weight-bearing radiographs reveal a Hallux Valgus Angle (HVA) of 42 degrees, an Intermetatarsal Angle (IMA) of 19 degrees, and clinical evidence of first tarsometatarsal (TMT) joint hypermobility. What is the most appropriate surgical intervention?
Explanation
Question 39
In two-stage revision total knee arthroplasty for periprosthetic joint infection, an articulating spacer is generally preferred over a static spacer. However, which of the following is an absolute indication for using a static spacer instead?
Explanation
Question 40
During a hallux valgus correction, the surgeon aggressively resects the medial eminence of the first metatarsal head, removing bone lateral to the sagittal sulcus. This error most directly predisposes the patient to which of the following postoperative complications?
Explanation
Question 41
A surgeon is balancing the gaps during a revision TKA. With trial components in place, the extension gap is perfectly balanced, but the flexion gap is unacceptably loose. Which of the following is the most appropriate step to achieve a balanced knee?
Explanation
Question 42
A 55-year-old female presents with a symptomatic bunion. Radiographs show an HVA of 14 degrees, an IMA of 8 degrees, and a Distal Metatarsal Articular Angle (DMAA) of 25 degrees. The joint is incongruent. What is the most appropriate surgical correction?
Explanation
Question 43
A 68-year-old male sustains a traumatic avulsion of the patellar tendon from the tibial tubercle 3 years after a primary TKA. Primary repair is attempted but fails. For definitive reconstruction using an allograft extensor mechanism, what postoperative protocol is mandatory for success?
Explanation
Question 44
A 35-year-old patient undergoes a proximal crescentic osteotomy for a severe hallux valgus deformity. Postoperatively, she develops intractable pain under the second metatarsal head. What is the most likely technical error responsible for this complication?
Explanation
Question 45
When utilizing diaphyseal engaging cementless stems in revision total knee arthroplasty, what is the minimum required distance of "scratch fit" (cortical engagement) in the diaphysis to achieve adequate initial stability?
Explanation
Question 46
A patient presents for bunion correction. Radiographs demonstrate an HVA of 20 degrees, an IMA of 8 degrees, and a Hallux Valgus Interphalangeus (HVI) angle of 18 degrees.
Which of the following procedures is most appropriate to address the interphalangeal deformity?
Explanation
Question 47
In the setting of revision TKA for highly porous metal cones versus metaphyseal sleeves, which of the following best describes a biomechanical characteristic of metaphyseal sleeves?
Explanation
Question 48
A 60-year-old female with profound rheumatoid arthritis presents with a severe hallux valgus deformity, complete destruction of the first MTP joint cartilage, and multiple lesser toe deformities. What is the surgical treatment of choice for her first ray?
Explanation
Question 49
During revision TKA, the surgeon encounters an isolated tight extension gap with a well-balanced flexion gap. Assuming the components are currently optimally sized, which of the following is the most appropriate surgical action?
Explanation
Question 50
Which of the following is a known risk associated with a Scarf osteotomy (a diaphyseal Z-step cut) for hallux valgus correction in a patient with osteoporotic bone?
Explanation
Question 51
A patient with a well-fixed, painful TKA is suspected of having a metal hypersensitivity. Patch testing shows a mild reaction to nickel. What is the consensus regarding patch testing prior to revision TKA for suspected metal allergy?
Explanation
Question 52
Which of the following is an absolute contraindication to performing a Keller resection arthroplasty for hallux valgus?
Explanation
Question 53
A 75-year-old male is undergoing a single-stage revision TKA for aseptic loosening. Intraoperatively, there is a massive uncontained medial tibial plateau defect (AORI Type IIb) extending 35 mm distal to the joint line. What is the most appropriate reconstruction method?
Explanation
Question 54
A surgeon performs a modified McBride bunionectomy. During the procedure, the fibular sesamoid is completely excised. What is the most significant biomechanical risk associated with this specific step?
Explanation
Question 55
A 45-year-old female presents with a painful bunion. Radiographs show a hallux valgus angle (HVA) of 45 degrees, an intermetatarsal angle (IMA) of 18 degrees, and hypermobility of the first tarsometatarsal (TMT) joint. What is the most appropriate surgical intervention?
Explanation
Question 56
During a revision total knee arthroplasty, the surgeon notes massive distal femoral bone loss. Elevating the joint line 10 mm proximally will most likely result in which of the following kinematic changes?
Explanation
Question 57
A 55-year-old female presents with a progressively painful, medially deviated great toe 1 year after a modified McBride bunionectomy and distal chevron osteotomy. Clinical exam reveals a flexible first MTP joint. Which of the following is the most appropriate treatment?
Explanation
Question 58
A 70-year-old male requires a revision TKA for aseptic loosening. Preoperative imaging reveals massive osteolysis with deficient metaphyseal bone compromising the collateral ligament attachments on the femur and tibia. Which of the following constraint levels is most appropriate?
Explanation
Question 59
A 32-year-old female undergoes a proximal crescentic osteotomy and distal soft tissue release for hallux valgus. Postoperatively, her HVA is corrected, but she has a prominent medial eminence and the articular surface of the metatarsal head is laterally deviated. Which of the following was likely missed preoperatively?
Explanation
Question 60
In revision total knee arthroplasty, the use of highly porous tantalum metaphyseal cones is best indicated for which AORI (Anderson Orthopaedic Research Institute) bone loss classification?
Explanation
Question 61
During a hallux valgus correction, a surgeon successfully reduces the IMA to 8 degrees and the MTP joint is congruent. However, the patient's great toe remains deviated laterally into valgus due to an interphalangeal angle of 20 degrees. Which of the following is the most appropriate next step?
Explanation
Question 62
When placing diaphyseal engaging stems during a revision total knee arthroplasty, which of the following is an advantage of cemented stems over cementless stems?
Explanation
Question 63
A 60-year-old male presents with dorsal foot pain and limited first MTP joint dorsiflexion. Radiographs reveal dorsal osteophytes with preserved joint space. He is diagnosed with early hallux rigidus. Which surgical procedure is most appropriate?
Explanation
Question 64
A patient undergoes a revision TKA complicated by a complete, intraoperative disruption of the patellar tendon from the tibial tubercle. Primary repair is tenuous. Which of the following reconstruction options provides the best long-term outcome?
Explanation
Question 65
The Scarf osteotomy for hallux valgus correction is relatively contraindicated in patients with which of the following characteristics?
Explanation
Question 66
A 68-year-old female is evaluated for a painful TKA placed 4 years ago. ESR is 45 mm/hr and CRP is 18 mg/L. Aspiration yields a synovial fluid WBC of 3,500 cells/uL with 75% PMNs. Based on the 2018 MSIS criteria, what is the most appropriate next step?
Explanation
Question 67
A patient presents with a recurrent hallux valgus deformity 2 years after a distal chevron osteotomy. The IMA is now 18 degrees and the first MTP joint is subluxated. The medial eminence is flush. What is the most appropriate revision strategy?
Explanation
Question 68
During a difficult revision TKA, the surgeon cannot evert the patella or gain adequate flexion without risking patellar tendon avulsion. Which of the following extensile exposures provides the most direct lateral translation of the extensor mechanism while maintaining blood supply?
Explanation
Question 69
When performing a distal metatarsal osteotomy for hallux valgus, preserving the blood supply to the metatarsal head is paramount to prevent avascular necrosis (AVN). The primary blood supply to the first metatarsal head enters at which location?
Explanation
Question 70
A patient complains of the knee 'giving way' when rising from a chair and descending stairs 2 years after a primary TKA. Examination shows laxity to varus and valgus stress at 90 degrees of flexion, but stability in full extension. Which complication has occurred?
Explanation
Question 71
A 42-year-old female develops avascular necrosis of the first metatarsal head complicated by severe secondary osteoarthritis following a distal chevron osteotomy and lateral release. She complains of unrelenting pain with ambulation. What is the most appropriate definitive management?
Explanation
Question 72
During a revision TKA, the original epicondylar axis is obscured by massive bone loss. Which of the following secondary landmarks is most reliable for establishing proper femoral component rotation?
Explanation
Question 73
To minimize the risk of avascular necrosis during a distal chevron osteotomy, the surgeon should strictly avoid extensive stripping of which capsular structures?
Explanation
Question 74
A 71-year-old female undergoes revision total knee arthroplasty (TKA) for aseptic loosening. Intraoperatively, the medial collateral ligament (MCL) is found to be completely attenuated and incompetent. The knee is globally unstable in both flexion and extension despite the use of a condylar constrained knee (CCK) insert. Which of the following constraint options is the most appropriate next step?
Explanation
Question 75
A 45-year-old female presents with a painful bunion. Clinical examination reveals hypermobility of the first tarsometatarsal (TMT) joint. Weight-bearing radiographs demonstrate an Intermetatarsal Angle (IMA) of 18 degrees and a Hallux Valgus Angle (HVA) of 42 degrees. Which of the following procedures is most appropriate to address this deformity?
Explanation
Question 76
A 68-year-old female presents with a loose TKA. Preoperative planning indicates severe cavitary and segmental bone loss of the proximal tibia with compromised metaphyseal cancellous bone, but an intact diaphyseal isthmus (AORI Type 2B/3).
Which of the following is the most biomechanically sound fixation method for the tibial component?
Explanation
Question 77
A patient develops iatrogenic hallux varus 6 months after a modified McBride bunionectomy. The deformity is symptomatic, but the first metatarsophalangeal (MTP) joint remains fully flexible without arthritic changes. Which of the following is the most appropriate surgical management?
Explanation
Question 78
During a complex revision TKA, the surgeon encounters severe extensor mechanism tightness preventing adequate exposure and eversion of the patella. A tibial tubercle osteotomy (TTO) is chosen. Which of the following is a critical technical aspect of performing this TTO?
Explanation
Question 79
A 32-year-old female presents with mild bunion pain. Radiographs demonstrate an IMA of 11 degrees, an HVA of 22 degrees, but an abnormally increased Distal Metatarsal Articular Angle (DMAA) of 20 degrees. Which of the following osteotomies is most appropriate to specifically correct the DMAA?
Explanation
Question 80
During intraoperative gap balancing in a revision TKA, the surgeon notes that the joint is stable in extension but exhibits symmetric, excessive laxity in flexion.
Which of the following is the most appropriate corrective action?
Explanation
Question 81
To minimize the risk of avascular necrosis (AVN) of the first metatarsal head during a distal chevron osteotomy, the surgeon must be careful to preserve its primary blood supply. Which of the following vascular structures provides the most critical blood supply to the first metatarsal head?
Explanation
Question 82
A surgeon is performing a two-stage exchange arthroplasty for a periprosthetic joint infection. During reimplantation, accurate restoration of the joint line is critical for optimal kinematics. The joint line in a standard TKA is typically referenced to be approximately 2.5 to 3.0 cm distal to which reliable anatomic landmark?
Explanation
Question 83
A 65-year-old female with severe, long-standing rheumatoid arthritis presents with an HVA of 55 degrees, an IMA of 20 degrees, and fixed dorsal subluxations of the 2nd through 5th MTP joints with severe plantar pain. Which of the following surgical procedures is the gold standard for this patient?
Explanation
Question 84
Intraoperative assessment during a revision TKA demonstrates symmetrical tightness in both the flexion and extension gaps. The current polyethylene insert is a standard 10 mm thickness. What is the most appropriate next step to balance the knee?
Explanation
Question 85
A 28-year-old female presents with medial great toe pain. Radiographs reveal a congruent 1st MTP joint, an IMA of 8 degrees, an HVA of 14 degrees, and a Hallux Valgus Interphalangeus (HVI) angle of 22 degrees. What is the most appropriate surgical intervention?
Explanation
Question 86
A 72-year-old male is evaluated for a painful TKA 4 years postoperatively. Synovial fluid aspiration yields a WBC count of 4,500 cells/uL with 85% neutrophils. Fungal and routine cultures are pending. According to the 2018 MSIS/ICM criteria, what additional test would provide the highest specificity for confirming a chronic periprosthetic joint infection (PJI)?
Explanation
Question 87
During a Scarf osteotomy for moderate hallux valgus, the bone cuts are made in a Z-configuration along the diaphysis of the first metatarsal. Which of the following is a well-described, specific biomechanical complication associated with this osteotomy geometry?
Explanation
None
