ABOS Part I Orthopaedic Review: Patellar Instability, Knee OA, & Hallux Rigidus Management | Part 22308

Key Takeaway
The ABOS Part I Orthopaedic Review provides in-depth coverage of patellar instability, including MPFL reconstruction and tibial tubercle osteotomy. It also details knee osteoarthritis management with High Tibial Osteotomy (HTO) and Unicondylar Knee Arthroplasty (UKA). Additionally, it addresses hallux rigidus, outlining surgical interventions like cheilectomy and MTP joint arthrodesis for comprehensive exam preparation.
ABOS Part I Orthopaedic Review: Patellar Instability, Knee OA, & Hallux Rigidus Management | Part 22308
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 16-year-old male presents with recurrent lateral patellar dislocations. Clinical examination reveals a positive J-sign, patellar hypermobility, and a positive apprehension test at 20 degrees of knee flexion. Imaging shows significant trochlear dysplasia, a TT-TG distance of 22 mm, and patella alta. The patient has failed conservative management. Which of the following surgical interventions would be MOST appropriate to address the multiple anatomical risk factors in this patient?
Explanation
Correct Answer: C
This patient presents with a severe form of patellar instability characterized by multiple significant anatomical risk factors: severe trochlear dysplasia, a markedly increased TT-TG distance (normal < 15-20 mm), and patella alta. Isolated MPFL reconstruction would address the medial restraint but not the underlying bony deformities. VMO advancement and lateral retinacular release are typically insufficient for severe bony dysplasia. Tibial tubercle medialization alone would only address the TT-TG and not the trochlear dysplasia or patella alta. Therefore, a comprehensive approach involving trochleoplasty (for the severe dysplasia), MPFL reconstruction (for the medial restraint), and a tibial tubercle osteotomy for both medialization (for TT-TG) and distalization (for patella alta) is indicated for optimal outcomes and recurrence prevention. This combination addresses all major identified risk factors.
Question 2
Regarding the medial patellofemoral ligament (MPFL), which statement is most accurate concerning its anatomy and function?
Explanation
Correct Answer: C
The MPFL is recognized as the primary static restraint to lateral patellar translation, particularly in the initial 20-30 degrees of knee flexion, where the trochlear groove is shallowest. At full knee extension, the joint is less constrained, but the MPFL's role is critical. The femoral attachment is variable but typically found distal and posterior to the adductor tubercle, often blended with the adductor magnus tendon and medial gastrocnemius origin, not consistently on the medial epicondyle. The patellar attachment is usually on the superior medial patella. While avulsions can occur at either end, femoral avulsions are more common in acute dislocations.
Question 3
Which of the following is considered the MOST significant risk factor for recurrent patellar instability?
Explanation
Correct Answer: D
Severe trochlear dysplasia, especially Dejour Types B, C, or D, is consistently identified as the single most significant anatomical risk factor for recurrent patellar instability. The flattened or convex trochlear groove provides inadequate bony constraint against lateral patellar translation. Generalized ligamentous laxity is a risk factor but less potent than severe dysplasia. Dislocation at a younger age (especially under 15) is associated with higher recurrence rates, not older age. A torn MPFL is characteristic of acute dislocation, but its absence doesn't preclude recurrence if other factors exist; its presence increases recurrence risk if left untreated. A Q-angle less than 10 degrees would typically be protective or normal, not a risk factor; an increased Q-angle is a risk factor.
Question 4
During an MPFL reconstruction using a semitendinosus autograft, the most critical step to prevent iatrogenic patellar fracture or over-constraining the patella is:
Explanation
Correct Answer: C
Over-constraining the patella is a known complication of MPFL reconstruction, leading to patellofemoral pain and stiffness. The MPFL is isometric in the initial 0-30 degrees of flexion. Tensioning the graft with the knee in 30 degrees of flexion is crucial. If the graft is tensioned in full extension or hyperflexion, it becomes too tight in mid-flexion, causing increased patellofemoral contact pressures and potentially pain or articular cartilage damage. Fluoroscopy for femoral tunnel placement is essential to avoid violating the physis in skeletally immature patients or drilling too anterior/posterior, but it doesn't directly prevent over-tensioning. Patellar fixation is standard; lateral retinacular release is not routinely performed with MPFL reconstruction unless specific lateral tightness is present.
Question 5
A patient with a history of recurrent patellar instability undergoes an MRI. The report indicates a TTPG (Tibial Tubercle-Trochlear Groove) distance of 20 mm. What is the clinical significance of this finding?
Explanation
Correct Answer: B
A TT-TG distance of 20 mm is considered significantly elevated. Normal values are typically less than 15-20 mm, with values over 20 mm strongly correlating with patellofemoral instability due to a lateralized pull of the patellar tendon and quadriceps mechanism relative to the trochlear groove. It is a key factor indicating bony malalignment. While patella alta can coexist, TT-TG specifically measures the transverse plane relationship, not patellar height. It's a significant risk factor but doesn't necessarily dictate immediate surgery if asymptomatic or if conservative management is successful. Quadriceps imbalance can contribute but isn't directly measured by TT-TG.
Question 6
Which of the following physical examination maneuvers is most specific for diagnosing patellar instability?
Explanation
Correct Answer: C
The patellar apprehension test (or 'Fairbank's test') involves attempting to laterally translate the patella with the knee in varying degrees of flexion while observing for the patient's anxiety, muscle guarding, or resistance, which signifies impending dislocation. This test is highly specific for patellar instability. The other tests are for collateral ligaments (valgus stress), ACL (Lachman), meniscal injury (McMurray), or patellofemoral pain syndrome (patellar grind), not patellar instability directly.
Question 7
A 12-year-old male with open physes experiences his second lateral patellar dislocation. X-rays show no fracture. MRI confirms MPFL rupture and normal trochlear morphology. He has no significant patella alta or increased TT-TG distance. What is the most appropriate surgical approach?
Explanation
Correct Answer: C
For skeletally immature patients with recurrent patellar instability, MPFL reconstruction is the preferred procedure. Given the open physes, techniques that avoid or protect the growth plates are critical, such as an all-epiphyseal (transphyseal without violating growth plates) or transphyseal tunnels placed carefully to minimize growth disturbance. Tibial tubercle osteotomies and trochleoplasty are generally avoided in skeletally immature patients due to the risk of growth arrest, unless there are severe underlying bony deformities that supersede this risk (which are explicitly ruled out in this question). Conservative management has failed after the second dislocation, and lateral release alone is insufficient for MPFL rupture.
Question 8
A 28-year-old female presents with persistent anterior knee pain and crepitus following an MPFL reconstruction performed 1 year ago for recurrent patellar dislocations. She reports no further dislocations but finds stairs and squatting painful. Physical exam shows no apprehension, but diffuse tenderness around the patellofemoral joint. Patellar height is normal. What is the most likely cause of her symptoms?
Explanation
Correct Answer: C
Persistent anterior knee pain, particularly with activities like stairs and squatting, after an MPFL reconstruction that successfully prevented recurrence, strongly suggests patellofemoral overload or over-constraining. This is a common complication if the MPFL graft is tensioned too tightly or fixed in an incorrect position, leading to increased patellofemoral contact pressures. Recurrence is ruled out by the history. Infection would typically present with different symptoms (fever, warmth, redness, systemic signs). Insufficient medialization would lead to continued instability, not just pain without apprehension. Graft rupture would lead to recurrence.
Question 9
Which radiographic measurement is used to assess patellar height?
Explanation
Correct Answer: D
The Insall-Salvati ratio (patellar tendon length to patellar diagonal length on a lateral X-ray) and modified Insall-Salvati ratio are standard measurements for assessing patellar height (patella alta or baja). The Q-angle measures quadriceps alignment, TT-TG measures tibial tubercle lateralization, Dejour classifies trochlear dysplasia, and bisect offset is used for patellar tilt on axial views. Therefore, Insall-Salvati ratio is the correct answer for patellar height.
Question 10
Which of the following is an absolute contraindication to performing a tibial tubercle osteotomy in a patient with patellar instability?
Explanation
Correct Answer: B
An open proximal tibial physis is an absolute contraindication for a standard tibial tubercle osteotomy (e.g., Fulkerson or Elmslie-Trillat) due to the significant risk of growth arrest, angular deformities, or leg length discrepancies. In skeletally immature patients, if a bony procedure is absolutely necessary, techniques that spare the physis (e.g., physis-sparing MPFL reconstruction) or physeal bridging procedures with careful monitoring are considered. Patella alta, severe trochlear dysplasia, and generalized ligamentous laxity are risk factors that may necessitate a tibial tubercle osteotomy, not contraindications. A prior MPFL reconstruction does not contraindicate a subsequent tibial tubercle osteotomy if malalignment persists.
Question 11
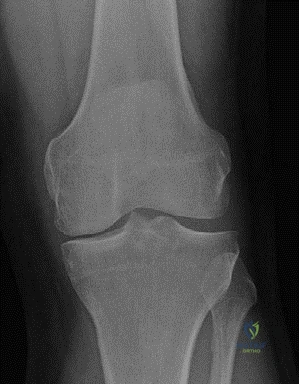
A 42-year-old bricklayer presents with chronic medial knee pain that has failed extensive non-surgical management. He is otherwise fit and well. Physical examination reveals tenderness over the medial joint line, a varus deformity that is correctable, and a full range of motion with stable ligaments. The patient is keen to return to his high-demand job. An AP weightbearing radiograph is shown below.
Based on this presentation and the provided image, which of the following is the most appropriate initial surgical recommendation for this patient?
Explanation
Correct Answer: C
The patient is a 42-year-old bricklayer with medial compartment osteoarthritis, a correctable varus deformity, and a high-demand physical job. High Tibial Osteotomy (HTO) is the most appropriate initial surgical recommendation in this scenario. HTO is indicated for younger, active patients (physiological age < 60 years) with unicompartmental osteoarthritis and a varus deformity, especially those with high physical demands. It aims to shift the mechanical axis laterally, offloading the medial compartment and preserving the native knee joint, which is advantageous for patients engaged in heavy labor.
- A. Total Knee Arthroplasty (TKA) is generally reserved for older patients with more diffuse or severe osteoarthritis, or those with lower activity demands, as it involves replacing the entire joint. A 42-year-old active bricklayer would likely wear out a TKA prematurely.
- B. Medial Unicondylar Knee Arthroplasty (UKA) is an option for unicompartmental OA, but the case explicitly states that UKA is generally not recommended for patients with highly physically demanding jobs due to the risk of accelerated wear. While women may prefer UKA due to better tolerance of angular deformity, and patients with low physical demand may benefit, it is less suitable for this patient's specific occupational demands.
- D. Arthroscopic debridement and microfracture are typically considered for smaller, contained chondral defects, not for moderate medial compartment osteoarthritis with a varus deformity, which implies more widespread cartilage loss and mechanical malalignment. These procedures are unlikely to provide long-term relief for this patient's condition.
- E. Patellofemoral Arthroplasty addresses isolated patellofemoral osteoarthritis. The patient's symptoms and radiographic findings are consistent with medial compartment osteoarthritis, not primarily patellofemoral involvement.
Question 12
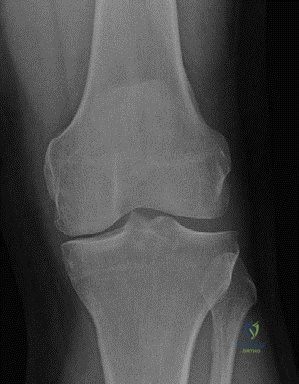
A 48-year-old male patient, similar to the case presented, is being evaluated for surgical management of medial compartment osteoarthritis. He has a varus deformity of 8 degrees, full range of motion, and stable ligaments. However, during the workup, it is discovered that he has a history of rheumatoid arthritis and a large varus thrust with coronal subluxation of 1.5 cm. An AP weightbearing radiograph is shown below.
Considering these additional findings, which of the following is a contraindication for performing a High Tibial Osteotomy (HTO) in this patient?
Explanation
Correct Answer: C
The case explicitly lists inflammatory arthropathy, such as rheumatoid arthritis and psoriatic arthropathy, as main contraindications for HTO. The presence of rheumatoid arthritis significantly increases the risk of poor bone healing, disease progression in other compartments, and overall unpredictable outcomes with osteotomy. Additionally, a large varus thrust with coronal subluxation of > 1 cm is also a contraindication, which this patient also exhibits (1.5 cm).
- A. Physiological age of 48 years is well within the acceptable range (< 60 years) for HTO.
- B. Varus deformity of 8 degrees is within the acceptable range (< 15 degrees) for HTO.
- D. Full range of motion is a favorable condition for HTO, as it indicates good joint mobility and less stiffness.
- E. Stable knee ligaments are a prerequisite for HTO, as ligamentous instability (e.g., incompetent MCL or ACL) is a contraindication.
Question 13
A 55-year-old female patient with medial compartment osteoarthritis and low physical demand is considering surgical options. She has a varus deformity of 7 degrees, no fixed flexion deformity, and good knee flexion. She expresses concern about the cosmetic appearance of angular deformity. Based on the case discussion, which surgical option would be most appropriate for her?
Explanation
Correct Answer: C
The case states that while indications for HTO and UKA are similar, women often prefer UKA because they do not tolerate the angular deformity created by HTO very well. Additionally, patients with low physical demand may benefit from UKA. This patient fits both criteria: she is female, has low physical demand, and is concerned about angular deformity. UKA offers a less invasive option with potentially better cosmetic outcomes and is suitable for her activity level.
- A. High Tibial Osteotomy (HTO), while a viable option for unicompartmental OA, might not be preferred by this patient due to the angular deformity it creates, which women may not tolerate well.
- B. Total Knee Arthroplasty (TKA) is generally considered for more severe, multi-compartmental arthritis or older, less active patients. It is an overtreatment for isolated medial compartment OA in a 55-year-old with low physical demand.
- D. Arthroscopic lavage and debridement are typically palliative and offer limited long-term benefit for established osteoarthritis with structural deformity.
- E. Distal Femoral Osteotomy is indicated for lateral compartment osteoarthritis with valgus deformity, which is not the patient's presentation.
Question 14
A 45-year-old male undergoes a closing wedge High Tibial Osteotomy (HTO) for medial compartment osteoarthritis. Postoperatively, he experiences a complication related to the surgical technique. Which of the following complications is specifically associated with closing wedge HTO, as discussed in the case?
The image shows a post-operative radiograph of a closing wedge HTO.
Explanation
Correct Answer: C
The case specifically mentions that closing wedge osteotomy 'may entail proximal fibular osteotomy or disruption of tibial–fibular joint. It has the risk of peroneal nerve injury'. This is a direct complication associated with the closing wedge technique due to the proximity of the fibula and the common peroneal nerve during the osteotomy and potential fibular shortening or osteotomy.
- A. Late collapse with loss of correction is a disadvantage specifically attributed to opening wedge osteotomy in the case.
- B. Need for bone graft is a disadvantage specifically attributed to opening wedge osteotomy, as the gap created needs to be filled.
- D. Decreased patellar height (patella baja) is associated with opening wedge osteotomy, whereas closing wedge osteotomy is noted to increase patellar height. Historically, patella baja was associated with lateral closing wedge HTO with cast immobilization, but more recent studies show closing wedge increases patellar height.
- E. Increased risk of non-union is not specifically highlighted as a unique complication of closing wedge HTO over opening wedge in the provided text, though it can be a general complication of any osteotomy.
Question 15
A 50-year-old patient undergoes an opening wedge High Tibial Osteotomy (HTO) for medial compartment osteoarthritis. Which of the following is a known disadvantage or potential complication specifically associated with the opening wedge technique, as described in the case?
The image shows a post-operative radiograph of an opening wedge HTO.

Explanation
Correct Answer: D
The case states that the opening wedge osteotomy 'has the disadvantage of having to use bone graft and late collapse with loss of correction'. This directly identifies 'late collapse with loss of correction' as a specific disadvantage of the opening wedge technique.
- A. Loss of bone stock making TKA technically difficult is a disadvantage specifically attributed to closing wedge osteotomy.
- B. Increased patellar height is associated with closing wedge osteotomy, while opening wedge osteotomy is noted to lower patellar height.
- C. Risk of peroneal nerve injury is a specific risk associated with closing wedge osteotomy, particularly with proximal fibular osteotomy or disruption of the tibiofibular joint.
- E. Disruption of the tibiofibular joint is mentioned as a potential consequence of closing wedge osteotomy.
Question 16
A 62-year-old patient with medial compartment osteoarthritis is being considered for surgical intervention. She has a fixed flexion deformity of 20 degrees and a varus deformity of 10 degrees. Her knee flexion is 85 degrees. Based on the prerequisites for HTO discussed in the case, which of her clinical findings would contraindicate a High Tibial Osteotomy?
Explanation
Correct Answer: C
The case lists the prerequisites for HTO, including a fixed flexion deformity of < 15 degrees. This patient has a fixed flexion deformity of 20 degrees, which exceeds this prerequisite and therefore contraindicates HTO.
- A. Varus deformity of 10 degrees is within the acceptable range (< 15 degrees) for HTO.
- B. Physiological age of 62 years is slightly above the stated prerequisite of < 60 years, but 'physiological age' can be subjective. However, the fixed flexion deformity is a more definitive contraindication based on the strict criteria provided. If the patient was physiologically younger than 60 despite chronological age, this might not be an absolute contraindication, but the fixed flexion deformity is.
- D. Knee flexion of 85 degrees is just below the prerequisite of > 90 degrees flexion. While close, it could be a relative contraindication, but the fixed flexion deformity is a more direct and absolute contraindication based on the given thresholds.
- E. Medial compartment osteoarthritis is the indication for HTO, not a contraindication.
Question 17
The case discusses the comparative outcomes of HTO versus UKA, referencing a review by Dettoni et al. (2010). What was the primary conclusion of this review regarding the superiority of one treatment over the other for medial unicompartmental arthrosis of the knee?
Explanation
Correct Answer: C
The case explicitly states, referencing Dettoni et al., that 'They concluded that with the correct indications, both treatments produce durable and predictable outcomes in the treatment of medial unicompartmental arthrosis of the knee. There is no evidence of superior results of one treatment over the other.'
- A. UKA consistently shows significantly better survivorship and functional outcomes. The review reported 'slightly better results for UKA in terms of survivorship and functional outcome,' but immediately qualified this by stating 'the differences are not remarkable' and 'no evidence of superior results of one treatment over the other.'
- B. HTO consistently shows significantly better survivorship and functional outcomes. This is incorrect, as the review suggested slightly better results for UKA, though not remarkably so.
- D. HTO is superior for high-demand patients, while UKA is superior for low-demand patients. While this is the clinical recommendation made by the candidate in the case based on practical considerations (accelerated wear of UKA in high-demand jobs), the Dettoni et al. review's conclusion was specifically about the lack of evidence for superiority in outcomes between the two treatments when indications are correct, not a direct endorsement of one over the other based on activity level in terms of overall outcome superiority.
- E. The review found no reliable data to compare the two treatments effectively. This is incorrect. The review did compare studies but noted that 'the study methods are not homogeneous' and that most papers reported on closing wedge HTOs, which limited strong conclusions, but it still drew a conclusion about the comparable efficacy.
Question 18
A 47-year-old patient, similar to the bricklayer in the case, undergoes a High Tibial Osteotomy (HTO). Several years later, his osteoarthritis has progressed, and he now requires a Total Knee Arthroplasty (TKA). The surgeon notes that the previous HTO has complicated the TKA conversion. Which of the following is a specific implication of a prior opening wedge HTO on patellar height during subsequent TKA?
The image shows a post-operative radiograph of an HTO, which may have implications for patellar height.

Explanation
Correct Answer: B
The case states, 'More recent studies show that closing wedge osteotomy increases patellar height, whereas opening wedge osteotomy lowers patellar height and this can have implications following TKA.' Patella baja (lowered patellar height) can significantly complicate TKA by making patellar tracking more difficult, increasing the risk of patellar impingement, and potentially affecting the choice and placement of prosthetic components.
- A. It typically leads to patella alta, making patellar tracking easier. This is incorrect. Opening wedge HTO lowers patellar height, leading to patella baja. Closing wedge HTO increases patellar height.
- C. It has no significant effect on patellar height, simplifying TKA conversion. This is incorrect, as the case explicitly states it 'can have implications following TKA.'
- D. It causes lateral patellar subluxation, requiring a lateral release. While patellar tracking issues can occur, the primary effect on patellar height is lowering it, not necessarily causing lateral subluxation as a direct consequence of the osteotomy type itself.
- E. It increases the risk of patellar fracture during TKA. While TKA after HTO can have increased risks, the direct implication on patellar height is patella baja, not necessarily an increased fracture risk as the primary concern related to patellar height.
Question 19
A 42-year-old male bricklayer with medial compartment osteoarthritis is undergoing pre-operative planning for a High Tibial Osteotomy (HTO). The initial weightbearing AP radiograph is shown below. Which of the following parameters, if present, would be a contraindication for HTO, as discussed in the case?
The image shows a weightbearing AP radiograph of the left knee.
Explanation
Correct Answer: D
The case lists 'severe OA of medial compartment or lateral compartment/PFJ' as a main contraindication for HTO. If the patient had severe osteoarthritis of the patellofemoral joint, HTO would be contraindicated because it only addresses the tibiofemoral compartments and would not alleviate the patellofemoral pain.
- A. Varus deformity of 12 degrees is within the acceptable range (< 15 degrees) for HTO.
- B. Physiological age of 55 years is within the acceptable range (< 60 years) for HTO.
- C. Fixed flexion deformity of 10 degrees is within the acceptable range (< 15 degrees) for HTO.
- E. Ability to flex the knee to 100 degrees meets the prerequisite of > 90 degrees flexion for HTO.
Question 20
The candidate in the case mentions difficulties with conversion of HTO to TKA. Beyond patellar height changes, what is another significant challenge or disadvantage of a prior closing wedge HTO when converting to a Total Knee Arthroplasty (TKA)?
Explanation
Correct Answer: B
The case states that closing wedge osteotomy 'has the risk of peroneal nerve injury, there is also loss of bone stock making it technically difficult to perform TKA.' This loss of bone stock, particularly from the proximal tibia, can significantly complicate the preparation of the tibial plateau for TKA components, potentially requiring bone grafting or specialized implants.
- A. Increased risk of infection due to retained hardware is a general risk with any retained hardware, but 'loss of bone stock' is a more specific and direct difficulty related to the conversion itself, as highlighted in the text.
- C. Improved bone quality for implant fixation is incorrect; the loss of bone stock generally implies a more challenging bone bed for TKA.
- D. Reduced need for soft tissue balancing is incorrect; prior HTO can alter soft tissue tension and ligamentous balance, often making TKA soft tissue balancing more complex, not less.
- E. Easier restoration of the mechanical axis is incorrect; the altered anatomy and bone loss from HTO can make accurate restoration of the mechanical axis more challenging during TKA.
Question 21
A 55-year-old active male presents with chronic pain and stiffness in his right great toe, particularly during push-off. Physical examination reveals a dorsal exostosis and pain with passive dorsiflexion of the MTP joint, which is limited to 20 degrees. Radiographs show significant dorsal osteophyte formation, joint space narrowing, and subchondral sclerosis affecting approximately 50% of the joint surface. According to the Coughlin and Shurnas classification, what stage of hallux rigidus does this patient most likely have?
Explanation
Correct Answer: C
The Coughlin and Shurnas classification for hallux rigidus is widely used. Stage 1 involves mild flattening of the metatarsal head, minimal osteophytes, and good joint space. Stage 2 presents with moderate osteophytes (dorsal and dorsal-medial), mild-to-moderate joint space narrowing, and flattening of the metatarsal head, with 20-50% cartilage involvement. Stage 3 is characterized by significant osteophytes, moderate-to-severe joint space narrowing, and subchondral sclerosis/cysts, with greater than 50% cartilage involvement and pain at end-range motion. Stage 4 involves ankylosis or severe degenerative changes throughout the entire joint. This patient's presentation of significant dorsal osteophyte formation, joint space narrowing, subchondral sclerosis, and limited dorsiflexion to 20 degrees, affecting approximately 50% of the joint, aligns with Stage 3 hallux rigidus.
Question 22
Which of the following intrinsic foot muscles is primarily responsible for flexion of the great toe MTP joint and contributes significantly to the 'windlass mechanism' that is impaired in hallux rigidus?
Explanation
Correct Answer: B
The flexor hallucis brevis (FHB) is an intrinsic foot muscle with two heads (medial and lateral) that insert into the base of the proximal phalanx, encasing the sesamoids. It is the primary flexor of the great toe MTP joint and plays a critical role in stabilizing the MTP joint during gait, particularly during the push-off phase by facilitating the 'windlass mechanism'. Impairment of this mechanism due to MTP joint stiffness (hallux rigidus) alters normal gait biomechanics. Abductor hallucis abducts and flexes, adductor hallucis adducts and flexes, while lumbricales and flexor digitorum brevis act on lesser toes.
Question 23
A 48-year-old patient with Stage 2 hallux rigidus (Coughlin and Shurnas) continues to experience pain despite activity modification, appropriate footwear, and NSAIDs. Dorsiflexion is limited to 30 degrees, and a prominent dorsal osteophyte is palpable. Which surgical procedure is generally considered the most appropriate initial intervention for this stage, aiming to preserve joint motion?
Explanation
Correct Answer: C
For Stage 2 hallux rigidus, where there is moderate joint space narrowing and moderate osteophyte formation, but still reasonable cartilage (50-75% intact), a dorsal cheilectomy is typically the first-line joint-preserving surgical option. It involves removing the dorsal osteophytes and often a portion of the dorsal metatarsal head to decompress the joint and improve dorsiflexion. Moberg osteotomy is often performed in conjunction with a cheilectomy, or for more advanced cases, to improve dorsiflexion via a plantarflexion osteotomy of the proximal phalanx. Arthrodesis and arthroplasty are generally reserved for more advanced stages (Stage 3 and 4) or failed conservative/joint-sparing procedures. Metatarsal head resection arthroplasty (Keller arthroplasty) is largely historical due to associated complications like transfer metatarsalgia and instability.
Question 24
What is the primary biomechanical advantage of performing a Moberg osteotomy (dorsal closing wedge osteotomy of the proximal phalanx) in conjunction with a cheilectomy for hallux rigidus?
Explanation
Correct Answer: C
A Moberg osteotomy, a dorsal closing wedge osteotomy of the proximal phalanx, effectively plantarflexes the proximal phalanx relative to its articular surface. This maneuver indirectly increases functional dorsiflexion at the MTP joint by changing the resting position of the proximal phalanx, thereby reducing impingement and improving the toe-off phase of gait. It is typically performed in conjunction with a cheilectomy for Stage 2 or early Stage 3 hallux rigidus, or when isolated cheilectomy is insufficient to restore adequate dorsiflexion. It does not primarily offload the metatarsal head, correct hallux valgus (though some subtle correction might occur), or directly enhance intrinsic muscle function.
Question 25
A 60-year-old sedentary patient with Stage 4 hallux rigidus presents with severe, constant pain in the first MTP joint, significantly affecting daily activities. Radiographs show complete obliteration of the joint space and subchondral bone erosions. Considering the patient's age and activity level, which surgical option is generally considered the gold standard for pain relief and functional improvement in this scenario?
Explanation
Correct Answer: C
For Stage 4 hallux rigidus, characterized by severe degenerative changes or ankylosis, joint-preserving procedures like cheilectomy or Moberg osteotomy are inappropriate as they cannot address the diffuse damage. First MTP joint arthrodesis (fusion) is considered the gold standard for severe hallux rigidus, especially in active patients, or when other procedures have failed. It provides reliable pain relief and a stable, pain-free platform for push-off, though it sacrifices MTP joint motion. While interpositional arthroplasty or MTP joint implants might be considered for less active patients or those unwilling to sacrifice motion, arthrodesis typically offers the most predictable and durable pain relief for severe end-stage disease. A sedentary patient might be a candidate for arthroplasty, but for reliable pain relief and functional improvement, especially with complete obliteration, arthrodesis is still considered the gold standard for overall success.
Question 26
What is the most common radiographic finding in early stages of hallux rigidus?
Explanation
Correct Answer: C
In the early stages of hallux rigidus, the most common and often first radiographic sign is the formation of a dorsal osteophyte on the first metatarsal head. This osteophyte impinges on the base of the proximal phalanx during dorsiflexion, leading to restricted motion and pain. Complete ankylosis is a late-stage finding. Subchondral cysts and significant valgus deformity are less specific or later findings. Bone marrow edema is an MRI finding, not typically a primary radiographic finding for early diagnosis.
Question 27
Which of the following is considered a relative contraindication to first MTP joint arthroplasty with an implant for hallux rigidus?
Explanation
Correct Answer: C
Previous infection in the surgical field is a strong contraindication for any joint replacement procedure, including MTP joint arthroplasty with an implant, due to the high risk of recurrent infection and subsequent implant failure. Older, less active patients are often considered good candidates for arthroplasty as motion preservation is prioritized over the robust stability of an arthrodesis. Rheumatoid arthritis can be an indication for arthroplasty, especially with polyarticular involvement. Failed cheilectomy is a common indication for salvage procedures like arthroplasty or arthrodesis. Moderate hallux valgus may need concomitant correction but isn't a direct contraindication to implant arthroplasty itself, though some implants may not be suitable.
Question 28
When performing a cheilectomy for hallux rigidus, what is the recommended amount of bone to resect from the dorsal aspect of the first metatarsal head to achieve adequate decompression and improve dorsiflexion?
Explanation
Correct Answer: B
When performing a dorsal cheilectomy, the goal is to remove the dorsal osteophytes and approximately 10-15% of the dorsal articular cartilage of the metatarsal head. This amount is generally considered sufficient to decompress the joint, improve dorsiflexion, and prevent impingement without excessively shortening the metatarsal or destabilizing the joint. Removing only the visible osteophyte might be insufficient if impingement persists. Resecting 30-40% or the entire dorsal third is excessive and can lead to instability, transfer metatarsalgia, or shortening.
Question 29
A 30-year-old professional athlete develops severe, painful hallux rigidus (Coughlin and Shurnas Stage 3-4). He requires a stable, pain-free foot for continued high-impact activities. Which surgical option would you most strongly recommend for this patient?
Explanation
Correct Answer: C
For a young, active professional athlete with severe hallux rigidus (Stage 3-4), a first MTP joint arthrodesis is the most appropriate and recommended option. While it sacrifices motion, it provides a highly stable, pain-free, and durable platform capable of withstanding high-impact activities required by athletes. Cheilectomy with Moberg is generally for earlier stages (Stage 2-3). Keller arthroplasty (resection of proximal phalanx base) is largely abandoned due to high rates of complications like transfer metatarsalgia and instability. Silicone implants have a high failure rate in active patients and are prone to synovitis and osteolysis. Interpositional arthroplasty may be considered for less active patients but does not provide the same level of stability and predictable outcomes for high-demand individuals.
Question 30
What is the typical alignment of the great toe MTP joint following a successful first MTP joint arthrodesis, for optimal function?
Explanation
Correct Answer: A
The optimal position for first MTP joint arthrodesis is crucial for gait and footwear. While there is some debate, generally, the joint should be fused in 10-15 degrees of dorsiflexion (relative to the weight-bearing surface) and 10-15 degrees of valgus. This position accommodates normal toe-off during gait, allows for comfortable shoe wear, and helps prevent transfer metatarsalgia to the lesser toes. Fusing in too much dorsiflexion can lead to dorsal impingement in shoes, while too much plantarflexion impairs push-off and can cause shoe fitting issues. Excessive valgus or varus can also cause problems. The options often vary, but 10-15 degrees dorsiflexion and valgus is a good range.
Question 31
What is the optimal position for a first metatarsophalangeal (MTP) joint arthrodesis to ensure normal gait and function in a patient with severe hallux rigidus?
Explanation
Question 32
During medial patellofemoral ligament (MPFL) reconstruction, identifying the anatomical femoral attachment is critical to avoid graft anisometry. Where is the normal femoral origin of the MPFL located?
Explanation
Question 33
A 55-year-old male with symptomatic isolated medial compartment knee osteoarthritis desires a unicompartmental knee arthroplasty (UKA). Which of the following is an absolute contraindication for this procedure?
Explanation
Question 34
A 58-year-old female presents with severe pain in her left great toe. Examination reveals pain specifically during the mid-range of passive dorsiflexion and plantarflexion of the 1st MTP joint. Radiographs demonstrate severe joint space narrowing and large dorsal, medial, and lateral osteophytes. According to the Coughlin and Shurnas classification, what is the most appropriate surgical treatment?
Explanation
Question 35
A 21-year-old female presents with recurrent lateral patellar instability. Imaging demonstrates a tibial tubercle-trochlear groove (TT-TG) distance of 24 mm and a Caton-Deschamps index of 1.0. Trochlear depth is normal. What is the most appropriate surgical intervention?
Explanation
Question 36
A 45-year-old active laborer presents with medial knee pain. Radiographs reveal isolated medial compartment osteoarthritis and a mechanical axis that passes through the medial compartment. When planning a valgus-producing high tibial osteotomy (HTO), where should the target mechanical axis ideally pass?
Explanation
Question 37
A patient undergoes a dorsal cheilectomy for Grade 2 hallux rigidus. Postoperatively, she complains of numbness along the dorsomedial aspect of her hallux. Which nerve was most likely injured during the surgical approach?
Explanation
Question 38
The medial patellofemoral ligament (MPFL) provides the primary soft-tissue restraint to lateral patellar translation at which of the following knee flexion angles?
Explanation
Question 39
According to the American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for the non-operative management of knee osteoarthritis, which of the following treatments has a "Strong" recommendation FOR its use?
Explanation
Question 40
In the treatment of hallux rigidus, a Moberg osteotomy is primarily designed to achieve which of the following biomechanical outcomes?
Explanation
Question 41
A lateral radiograph of the knee in a patient with patellar instability demonstrates a "crossing sign" and a "supratrochlear spur", but no "double contour" sign. According to the Dejour classification, what type of trochlear dysplasia does this represent?
Explanation
Question 42
A 70-year-old female with severe rheumatoid arthritis undergoes a primary total knee arthroplasty. Intraoperatively, the posterior cruciate ligament (PCL) is found to be incompetent and severely attenuated. The medial and lateral collateral ligaments are intact. Which of the following implant designs is most appropriate?
Explanation
Question 43
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon must be careful when tensioning the graft. Which of the following describes the optimal position and tensioning technique to avoid iatrogenic complications?
Explanation
Question 44
A 22-year-old female presents with recurrent patellar dislocations. Advanced imaging reveals a tibial tubercle-trochlear groove (TT-TG) distance of 24 mm and a normal Caton-Deschamps index. Which of the following surgical interventions is MOST appropriate?
Explanation
Question 45
According to the American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for the non-operative management of knee osteoarthritis, which of the following treatments is strongly recommended AGAINST?
Explanation
Question 46
A 65-year-old male with end-stage Hallux Rigidus (Coughlin and Shurnas Grade 4) is undergoing a first metatarsophalangeal (MTP) joint arthrodesis. To ensure optimal postoperative gait mechanics, what is the ideal position for the fusion?
Explanation
Question 47
A 45-year-old active male with medial compartment knee osteoarthritis and genu varum undergoes a medial opening wedge high tibial osteotomy (HTO). Which of the following is a common biomechanical consequence if the posterior gap is not appropriately larger than the anterior gap?
Explanation
Question 48
When evaluating a patient with recurrent patellar instability, a lateral radiograph demonstrates the "crossing sign" and a "supratrochlear spur." According to the Dejour classification for trochlear dysplasia, which type does this represent?
Explanation
Question 49
A 55-year-old female presents with medial joint line knee pain. Radiographs demonstrate isolated medial compartment osteoarthritis. Which of the following is an absolute contraindication for a medial unicompartmental knee arthroplasty (UKA)?
Explanation
Question 50
A 48-year-old female with Coughlin and Shurnas Grade 2 hallux rigidus is scheduled for a dorsal cheilectomy. During the procedure, what is the maximum recommended percentage of the dorsal metatarsal head that should be resected to alleviate impingement while preventing joint instability?
Explanation
Question 51
Which of the following orthotic modifications is most appropriate for the non-operative management of symptomatic hallux rigidus?
Explanation
Question 52
Patella alta is a known risk factor for recurrent patellar instability. Which of the following correctly describes the Caton-Deschamps index used to diagnose this condition?
Explanation
Question 53
During a Total Knee Arthroplasty (TKA), the surgeon determines that the knee is tight in full extension but perfectly balanced in 90 degrees of flexion. Which of the following is the most appropriate surgical step to balance the knee?
Explanation
Question 54
A patient complains of a painful "catching" or "popping" sensation at the anterior knee when extending from a flexed position, 1 year after a posterior-stabilized total knee arthroplasty (TKA). What is the underlying pathophysiology of this complication?
Explanation
Question 55
A 35-year-old female presents with severe lateral compartment knee osteoarthritis and a 15-degree valgus deformity due to prior trauma. She desires to return to high-impact activities. Which of the following procedures is most appropriate to unload her lateral compartment?
Explanation
Question 56
In the evaluation of patellar instability, distinguishing between habitual and obligatory dislocations is critical. Which of the following characterizes an obligatory patellar dislocation?
Explanation
Question 57
An orthopaedic surgeon is identifying the femoral footprint of the Medial Patellofemoral Ligament (MPFL) using fluoroscopy (Schöttle's point). Anatomically, where is the MPFL attachment located relative to the local bony landmarks?
Explanation
Question 58
A 60-year-old female with hallux rigidus previously underwent a first MTP joint silastic implant arthroplasty. She now presents with recurrent pain, massive swelling, and radiographic evidence of severe periprosthetic lucencies and bone loss. What is the most likely diagnosis?
Explanation
Question 59
During the physical examination of a patient with anterior knee pain and instability, the examiner observes a positive "J-sign." What is the pathomechanics underlying this clinical finding?
Explanation
Question 60
During a medial patellofemoral ligament (MPFL) reconstruction, identifying the correct femoral attachment is critical to prevent graft anisometry. According to Schöttle's point, where is the anatomic femoral origin of the MPFL located?
Explanation
Question 61
A 55-year-old male presents with dorsal midfoot pain and decreased great toe dorsiflexion. Radiographs reveal dorsal osteophytes with mild-to-moderate joint space narrowing (Coughlin and Shurnas Grade 2). He experiences pain at the extremes of range of motion but denies mid-arc pain. After failing shoe modifications, what is the most appropriate surgical intervention?
Explanation
Question 62
Which of the following patients is the most ideal candidate for a medial opening wedge high tibial osteotomy (HTO)?
Explanation
Question 63
In evaluating a patient with recurrent patellar dislocations, a computed tomography (CT) scan is obtained. At what tibial tubercle-trochlear groove (TT-TG) distance is a tibial tubercle medialization osteotomy generally considered an absolute indication when treating patellar instability?
Explanation
Question 64
A 70-year-old sedentary female undergoes a Keller resection arthroplasty for severe hallux rigidus. Postoperatively, she develops a "cock-up" deformity of the great toe and transfer metatarsalgia. The compromise of which structure during the index procedure most likely caused this complication?
Explanation
Question 65
According to classic Kozinn and Scott criteria, which of the following is considered an absolute contraindication for a medial unicompartmental knee arthroplasty (UKA)?
Explanation
Question 66
A true lateral radiograph of the knee in a patient with patellar instability demonstrates a "crossing sign" and a prominent "supratrochlear spur," but no double contour sign. According to the Dejour classification of trochlear dysplasia, what type does this represent?
Explanation
Question 67
A 60-year-old male with Grade 4 hallux rigidus is undergoing a first metatarsophalangeal (MTP) joint arthrodesis. To optimize postoperative gait, shoe wear, and patient satisfaction, what is the ideal position for the fusion?
Explanation
Question 68
When performing an isolated medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, at what knee flexion angle and tension should the graft be fixed to the femur to prevent medial patellar overload?
Explanation
Question 69
A 22-year-old female presents with recurrent patellar instability. MRI demonstrates a tibial tubercle-trochlear groove (TT-TG) distance of 24 mm and a Caton-Deschamps index of 1.1. No significant trochlear dysplasia is noted. What is the most appropriate surgical intervention?
Explanation
Question 70
A 45-year-old male runner complains of dorsal foot pain during toe-off. Examination reveals pain at the extremes of dorsiflexion of the first MTP joint. Radiographs show a dorsal osteophyte with mild joint space narrowing but preserved plantar joint space (Coughlin and Shurnas Grade 2). Conservative management has failed. Which procedure is most indicated?
Explanation
Question 71
According to the American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for the management of osteoarthritis of the knee, which of the following treatments is strongly NOT recommended?
Explanation
Question 72
A 10-year-old skeletally immature female with open physes requires surgical stabilization for recurrent patellar dislocations. To minimize the risk of iatrogenic growth arrest, the femoral attachment of an MPFL reconstruction should ideally be placed in relation to the distal femoral physis in which location?
Explanation
Question 73
When performing a first metatarsophalangeal (MTP) joint arthrodesis for severe Grade 4 hallux rigidus, what is the optimal position of the proximal phalanx to optimize postoperative gait?
Explanation
Question 74
Which of the following is considered an absolute contraindication for a medial unicompartmental knee arthroplasty (UKA) in a patient with medial compartment knee osteoarthritis?
Explanation
Question 75
During an anatomic medial patellofemoral ligament (MPFL) reconstruction, identifying the correct femoral footprint is critical. Radiographically, Schottle's point represents this attachment. What are the landmarks for Schottle's point on a true lateral radiograph?
Explanation
Question 76
A Moberg osteotomy is occasionally used as an adjunct in the treatment of hallux rigidus. Which of the following best describes the biomechanical effect of this procedure?
Explanation
Question 77
A 42-year-old active laborer presents with medial knee pain. Radiographs demonstrate medial compartment osteoarthritis and a mechanical axis that passes through the medial compartment with 8 degrees of varus. Range of motion is 0-130 degrees. The lateral and patellofemoral compartments are well preserved. What is the most appropriate surgical option?
Explanation
None
