
Demystify Posterior Approaches to the Hip: Es...
00:00
Start Quiz
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
Sudden cardiac arrest following a blow to the chest in young athletes has been termed "commotio cordis." It is most common in Little League and other youth projectile sports (eg, ice hockey, lacrosse). The cause, although not completely determined, is most likely an arrhythmia related to the impact in a vulnerable time in the cardiac cycle. Resuscitation has proven to be exceedingly difficult, resulting in a high mortality rate. Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
- Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 304.
Question 3High Yield
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include

Explanation
Typically, posterior spinal fusion to the pelvis is recommended for patients with spinal muscular atrophy and advanced scoliosis. Examination for lower extremity muscle contractures is important because the contractures may interfere with good sitting balance. Anterior release and fusion usually are not advised. Diaphragmatic pacing is not indicated because diaphragm function usually is not affected. Patients with spinal muscular atrophy usually are not ambulatory or only marginally ambulatory at the time of scoliosis surgery; therefore, gait analysis usually is not relevant. While a muscle biopsy may have a role in the diagnosis of this disorder, it plays no subsequent role in determining life expectancy or the value of spinal surgery. Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Question 4High Yield
A 65-year-old man has chronic Achilles insertional tendinitis that is refractory to nonsurgical management. A radiograph is shown in Figure 9. Preoperative counseling should include a discussion of the realistic duration of postoperative recovery. You should inform the patient that his expected recovery will last

Explanation
An older patient with calcaneal enthesopathy may take a year or more to recover after tendon debridement and calcaneal ostectomy. Young patients, and those with purely tendon pathology, may recover more quickly. McGarvey WC, Palumbo RC, Baxter DE, et al: Insertional Achilles tendinitis: Surgical treatment through a central tendon splitting approach. Foot Ankle Int 2002;23:19-25.
Question 5High Yield
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
References:
- Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 6High Yield
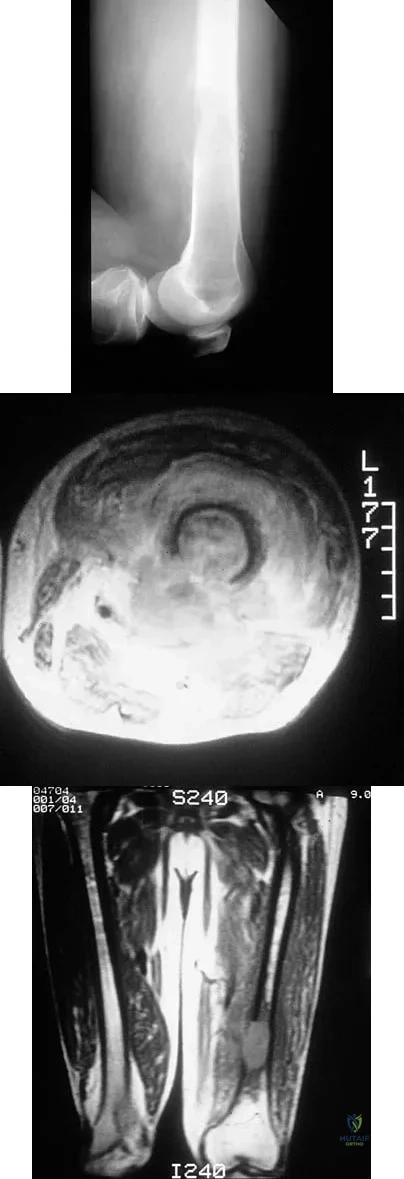
An otherwise healthy 16-year-old dancer reports a 1-month history of leg pain. AP and lateral radiographs of the distal femur are shown in Figures 67a and 67b. What is the next most appropriate step in management?
Explanation
Explanation
67b The radiographs show a very ill-defined, aggressive, moth-eaten bony destruction involving the distal left femoral diaphysis just above the metaphyseal junction. The differential diagnosis includes Ewing's sarcoma, osteosarcoma, lymphoma of bone, eosinophilic granuloma, osteomyelitis, and others. MRI would further define the lesion, and soft-tissue and intramedullary extension. There is aggressive periosteal reaction in the posteromedial aspect of the adjacent lesion with some multilayered components in the distal interface of the periosteum. The lateral radiograph shows cortical penetration and irregular periosteal reaction of the posterior margin, suggesting some posterior soft-tissue extension at this site as well. Gebhardt MC, Ready JE, Mankin HJ: Tumors about the knee in children. Clin Orthop Relat Res 1990;255:86-110.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 7High Yield
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
Explanation
The coronal MRI scan of the wrist shows the scaphoid. There is a subtle fracture line with a step-off at the radial surface consistent with a nonunion. The signal intensity is markedly different between the two fragments of the scaphoid. This strongly suggests osteonecrosis. Preiser's disease is osteonecrosis typically involving most or all of the scaphoid. Kienbock's disease involves the lunate. Intraosseous ganglia are easily diagnosed on MRI but typically have a fluid-filled area surrounded by denser bone in the periphery. Scapholunate dissociation can be seen on MRI as an injury to the scapholunate ligament and widening of the scapholunate interval, neither of which is seen on this image.
References:
- Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 8High Yield
What are the four most common soft-tissue sarcomas to spread via the lymph node system?
Explanation
Explanation
Soft-tissue sarcomas most frequently metastasize to the lung, but certain histologic types have a predilection for the lymph node system as well. Rhabdomyosarcoma, clear cell sarcoma, epithelioid sarcoma, and synovial sarcoma are four of the most common types to spread in this fashion. Careful evaluation and/or sentinel lymph node biopsy plays a role in disease staging and prognosis. Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
References:
- Blazer DG III, Sabel MS, Sondak VK: Is there a role for sentinel lymph node biopsy in the management of sarcoma? Surg Oncol 2003;12:201-206.
Question 9High Yield
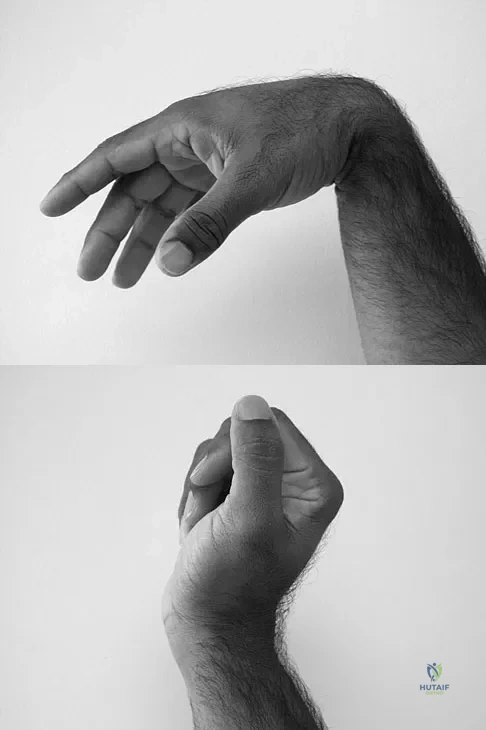
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 10High Yield
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Explanation
Both autograft and allograft have been used for complex acetabular reconstructions. They have been shown to be successful in the short term. However, graft resorption with collapse and subsequent cup loosening have occurred at high rates for both types of grafts, especially if reinforcement rings or cages are not used. Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 11High Yield
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
Explanation
The collagen orientation changes from parallel in the superficial zone to a more random pattern in the middle zone and finally to perpendicular in the calcified zone. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
References:
- Mankin HJ, Mow VC, Buckwalter JA: Articular cartilage structure, composition, and function, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 12High Yield
A patient with no history of patellar instability sustains a traumatic lateral patellar dislocation. What structure most likely has been torn?

Explanation
Any of the above structures may be involved in a lateral patellar dislocation. However, biomechanic studies have found that the medial patellofemoral ligament is the major soft-tissue static restraint of lateral patellar displacement, providing at least 50% of this function. Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65. Conlan T, Garth WP Jr, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 1993;75:682-693.
Question 13High Yield
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression. Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Question 14High Yield
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
Ankle arthrodesis for posttraumatic ankle arthrosis provides reliable pain relief. However, the long-term sequela of joint arthrodesis is the development of arthrosis in the surrounding joints. Over time, following ankle arthrodesis, the ipsilateral hindfoot and midfoot joints show signs of joint space wear, and this may be symptomatic. With a stable ankle arthrodesis, progressive limb-length discrepancy or talar osteonecrosis is not expected. Ankle arthrodesis has not been definitively linked to ipsilateral knee arthritis or contralateral ankle arthritis. Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 15High Yield
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
Explanation
Explanation
12b 12c Injury to the spinal accessory nerve can occur after penetrating trauma to the shoulder. Blunt trauma may also cause loss of trapezius function. Most commonly, surgical dissection in the posterior triangle of the neck, such as lymph node biopsy, may expose the nerve to possible damage. Surgical repair of the nerve may be considered up to 1 year after injury; after this time muscle transfer is usually associated with a better functional outcome. Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
References:
- Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop Relat Res 1999;368:5-16.
Question 16High Yield
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?

Explanation
The patient has sustained a Vancouver B2 periprosthetic femoral fracture (a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthoplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 17High Yield
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
Although obesity can make brace or halo wear difficult, it has not been associated with an increased risk for nonunion. Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 235-238.
Question 18High Yield
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
Explanation
A 32-mm head design results in less linear wear but more volumetric wear particles. Modular components that allow motion between the polyethylene insert and the shell can result in backside wear. The oxidative degradation of gamma-irradiated polyethylene stored in air leads to increased wear. All of these factors lead to a greater particulate load and more osteolysis. Circumferential porous coating blocks ingrowth of particle-laden fluid and decreases osteolysis. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Fisher J, Hailey JL, Chan KL, et al: The effect of aging following irradiation on the wear of UHMWPE. Trans Orthop Res Soc 1995;20:12.
References:
- Archibeck MJ: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Question 19High Yield
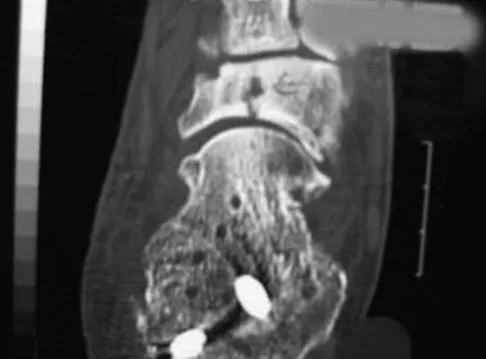
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of

Explanation
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Question 20High Yield
A 9-year-old girl reports the immediate onset of severe groin pain and the inability to walk after tripping on a curb. Examination reveals marked hip pain with passive range of motion. A radiograph is shown in Figure 21. Regardless of treatment, what is the most common complication following this injury?
Explanation
Explanation
The patient has an unstable slipped capital femoral epiphysis (SCFE). According to the classification system based on physeal stability, an unstable SCFE is one in which the patient is unable to walk, even with crutches. Ishemic necrosis, or osteonecrosis, of the femoral head is the most devastating complication of SCFE. One study found a 47% incidence of ischemic necrosis following unstable slips. This complication is most likely the result of vascular injury associated with initial femoral head displacement rather than the result of either tamponade from joint effusion or gentle repositioning prior to stabilization. Chondrolysis is a relatively uncommon complication following treatment of SCFE. This complication has been associated with persistent penetration of the hip joint with screws or pins used to stabilize the femoral head or with spica cast immobilization. There are no reports to suggest that osteochondritis dissecans, nonunion, or coxa magna follows treatment of SCFE. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
References:
- Rhoad RC, Davidson RS, Heyman S, et al: Pretreatment bone scan in SCFE: A predictor of ischemia and avascular necrosis. J Pediatr Orthop 1999;19:164-168.
Question 21High Yield
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal and superior laryngeal nerves are both at risk during the exposure but are not located between the trachea and the esophagus. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 22High Yield
A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy specimen is shown in Figure 10c. Management should consist of
Explanation
Explanation
10b 10c Based on these findings, the patient has an aneurysmal bone cyst. Frequently, fluid-fluid levels can be detected on MRI or CT images. The histologic results show a lesion that consists of cavernous spaces filled with blood. The lining of the cavity contains spindle cells, multinucleated giant cells, and reactive bone. Curettage and bone grafting is the preferred treatment method. Without treatment, these lesions can become quite large and destructive. Radiation therapy is not recommended for resectable lesions. Chemotherapy is not required for these benign lesions. Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
References:
- Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 232.
Question 23High Yield
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?

Explanation
The most common complication associated with tarsometatarsal joint injury is posttraumatic arthritis. In one series, symptomatic arthritis developed in 25% of the patients and half of those went on to fusion. In another series, 26% had painful arthritis. Initial treatment should consist of shoe modification, inserts, and anti-inflammatory drugs. Fusion is reserved for failure of nonsurgical management. Hardware failure may occur, but it is clinically unimportant. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618. Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Question 24High Yield
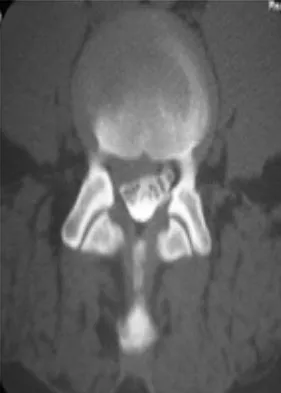
In the spine, osteoblastomas usually originate in the

Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 25High Yield
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 26High Yield
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
Explanation
7b The MRI scan shows a Segond fracture, which is a small avulsion of the lateral joint capsule from the anterolateral aspect of the proximal tibia. It is almost always associated with anterior cruciate ligament rupture and often with a tear of either the medial or lateral meniscus. Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
References:
- Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 27High Yield
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?

Explanation
A Jones fracture occurs at the metaphyseal-diaphyseal junction of the fifth metatarsal. It is often an acute fracture in conjunction with a chronic stress-related injury. It requires either a short leg cast with strict non-weight-bearing or surgical fixation. In the high performance athlete, the need for rapid return to sport activity usually requires surgical intervention, most commonly with an intramedullary screw. Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2, pp 2391-2409.
Question 28High Yield
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of

Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 29High Yield
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of
Explanation
Explanation
4b Humeral arthroplasty provides excellent pain relief and function for stage IV osteonecrosis with humeral collapse. In late disease with glenoid involvement (stage V), total shoulder arthroplasty is preferred. Some authors have reported satisfactory results with core decompression of the humeral head for early stages of osteonecrosis, but results for stage IV osteonecrosis are less satisfactory when compared with those for humeral arthroplasty. Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. LePorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS: Osteonecrosis of the humeral head treated by core decompression. Clin Orthop 1998;355:254-260.
References:
- Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 194-202.
Question 30High Yield
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
Electromyography during walking reveals the tibialis anterior muscle is active during early swing, allowing the foot to clear the ground. All of the other muscles are quiet, as the limb moves forward through space with minimal muscular effort. The other muscles are primarily active during weight acceptance or push-off. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Question 31High Yield
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of

Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 32High Yield
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Explanation
Explanation
Approximately 75% of people have the artery on the left side between T9 and T11. Its relevance to iatrogenic spinal cord problems is still uncertain. Stambaugh J, Simeone F: Vascular complication in spine surgery, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1715.
References:
- Lazorthes G: Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-262.
Question 33High Yield
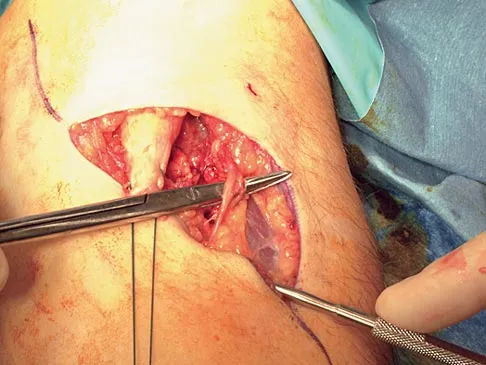
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach. Kelly EW, Morrey BF, O'Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Question 34High Yield
When an adult hip is surgically dislocated for relief of femoro-acetabular impingment, what is the risk of postoperative iatrogenic osteonecrosis?
Explanation
Explanation
In a report of more than 70 hips treated by surgical dislocation, iatrogenic osteonecrosis failed to develop in any of the hips.
References:
- Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U: Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.
Question 35High Yield
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 36High Yield
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Knee pain and swelling in the first week after ACL reconstruction is usually related to a postoperative hemarthrosis. A large hemarthrosis creates capsular distension, which inhibits active quadriceps contraction by a neurologic reflex, the H. reflex. Kennedy and associates reported that an experimentally induced knee effusion at 60 mL was found to result in profound inhibition of reflexly evoked quadriceps contraction. Removal of the hemarthrosis by aspiration will improve strength and often instantaneously restore the ability to contract the quadriceps muscle. A large effusion will also limit knee flexion. EMG and NCVS are not necessary unless there is a high index of suspicion of a femoral neuropathy. Diagnostic ultrasonography is not necessary in this patient but can be useful in the assessment of patellar tendon integrity. MRI is not indicated and would most likely be limited by artifact and postoperative changes. Continuous passive motion is not indicated and would most likely worsen the patient's symptoms. Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Question 37High Yield
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
The median survival of patients after discovery of bone metastasis from primary lung carcinoma is shorter compared with other primary sites.
Question 38High Yield
Which of the following lesions most closely resembles Ewing's sarcoma histologically?
Explanation
Explanation
Ewing's sarcoma is characterized by small round blue cells. Lesions with a similar appearance include lymphoma, primitive neuroectodermal tumor, rhabdomyosarcoma, small cell lung tumor, and metastatic neuroblastoma. Karyotyping, immunohistochemistry, and electron microscopy can help differentiate these lesions.
References:
- Wold LE, McLeod RA, Sim FH, Unni KK: Atlas of Orthop Pathology. Philadelphia, PA, WB Saunders, 1990.
Question 39High Yield
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 40High Yield
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?

Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 41High Yield
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?

Explanation
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Question 42High Yield
A 46-year-old woman who was involved in a motor vehicle accident reports a 4-month history of right-sided lower back pain and pain radiating into the right thigh. The patient underwent an extensive 3-month course of physical therapy and now is dependent on narcotic medication for pain control. Epidural injection therapy has failed to improve her symptoms. Examination is significant for weakness of hip flexion in the seated position and for decreased sensation to light touch in the medial anterior thigh region. Straight leg raise is negative, but the femoral stretch test reproduces anterior thigh pain. A CT myelogram image, at L3-L4, is shown in Figure 3. What is the most appropriate management at this time?
Explanation
The CT scan reveals a right-sided lateral disk protrusion at L3-4 that has been symptomatic for more than 4 months despite appropriate nonsurgical management. Relative surgical indications include persistent radiculopathy despite an adequate trial of nonsurgical management, recurrent episodes of sciatica, persistent motor deficit with tension signs and pain, and pseudoclaudication caused by underlying stenosis. Whereas studies have shown improvement in patients with sciatica from a lumbar disk herniation treated either nonsurgically or surgically, those undergoing surgical treatment had an overall greater improvement of symptoms. Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 43High Yield
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?

Explanation
Most leaders in orthopaedic surgery support Jacqueline Perry's theory that the postpolio syndrome is an attritional degenerative process that is the result of overuse of muscles and joints that are unable to adequately tolerate overload, and have little functional reserve. For that reason, aerobic conditioning and exercise are important. Overload and exhaustion of involved muscles should be avoided.
Question 44High Yield
Figures 40a and 40b show the pre- and postoperative radiographs of an 82-year-old woman with bilateral hip pain who has had staged total hip arthroplasties. To minimize potential injury to the sciatic nerve at the time of surgery, the surgeon should

Explanation
To improve hip biomechanics and secure more suitable bone for acetabular fixation, the true acetabulum is often resurfaced in patients who have developmental dysplasia of the hip, thus lowering the hip center and lengthening the leg. Acute lengthening of more than 3 cm will place excessive tension on the sciatic nerve and require a femoral shortening to avoid sciatic nerve injury. The other maneuvers will not relieve sciatic nerve tension because of limb lengthening. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 430-431.
Question 45High Yield
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of

Explanation
Arthroscopic capsular release is an effective means of treating stiffness that is the result of capsular contractures, such as in the case of a tight Bankart repair. Open release allows lengthening of a surgically shortened subscapularis, such as after a tight Putti-Platt repair. Additional physical therapy is unlikely to be effective because 8 months of treatment has failed to result in improvement. Accepting this degree of asymptomatic limited motion is not advisable because of the functional limitations for the patient and the increased risk of postoperative degenerative arthritis. Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 46High Yield
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?
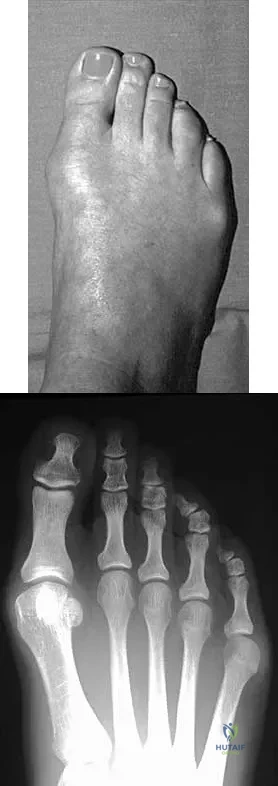
Explanation
Based on her symptoms and prior shoe wear modifications, the treatment of choice is surgical correction of the hallux valgus with a chevron osteotomy. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Steroid injection would only risk infection, as well as joint and capsule damage. Extra-depth shoes are an option; however, the patient is interested in surgical options. Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584. Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Question 47High Yield
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?

Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 48High Yield
One advantage of using onlay strut allograft in femoral revision surgery is that it can

Explanation
Onlay grafts can provide more structural support than morcellized grafts. They are more easily incorporated into the host femur than bulk segmental total femur allografts; however, the incorporation is never complete. The use of onlay grafts is principally directed at addressing segmental defects of the femur; their use can be applied with either cementless or cement fixation of the femoral stem. Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44. Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Question 49High Yield
Figures 48a through 48c show the lateral radiograph and MRI scans of a 60-year-old man who has had pain in his thigh for 1 month. The next most appropriate step in management should consist of
Explanation
The patient has a presumed metastatic bone tumor. The approach to evaluating a patient with a bone tumor of unknown primary origin is to obtain laboratory studies that include a CBC, an erythrocyte sedimentation rate, a serum protein electrophoresis, a calcium level, a urinalysis, and a prostate-specific antigen. In addition, a bone scan, a radiograph of the chest, and CT scans of the chest and abdomen should be obtained. These evaluations can identify the primary site in 85% of patients. GI studies rarely are of diagnostic value. Prophylactic stabilization is contraindicated until a diagnosis is confirmed by histology. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 50High Yield
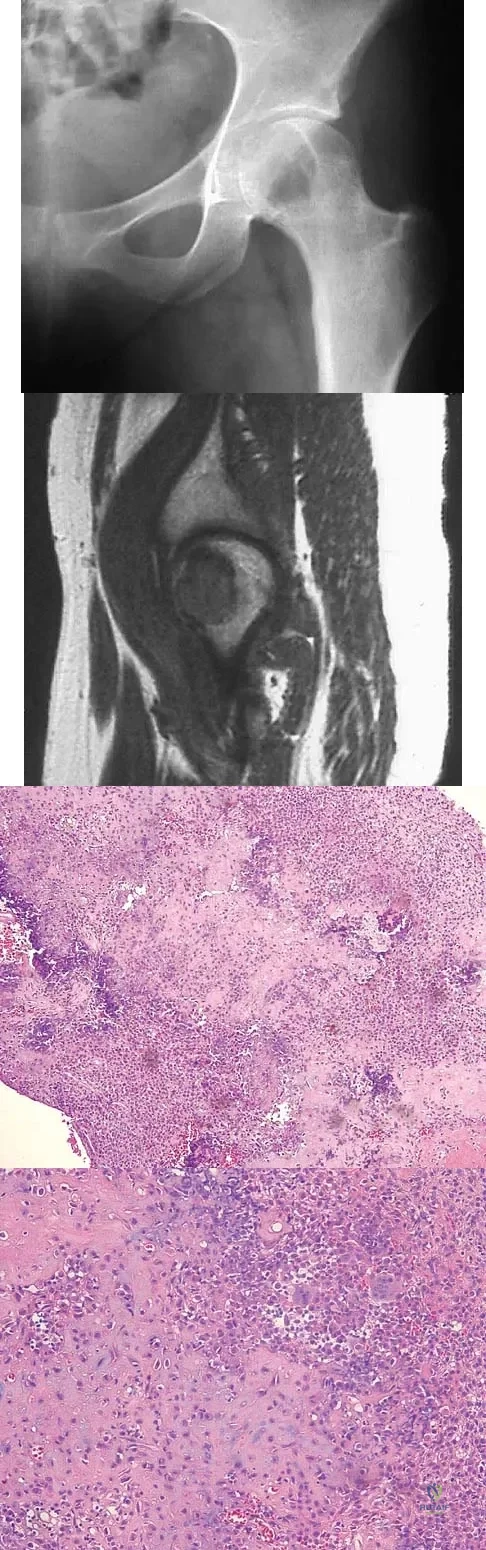
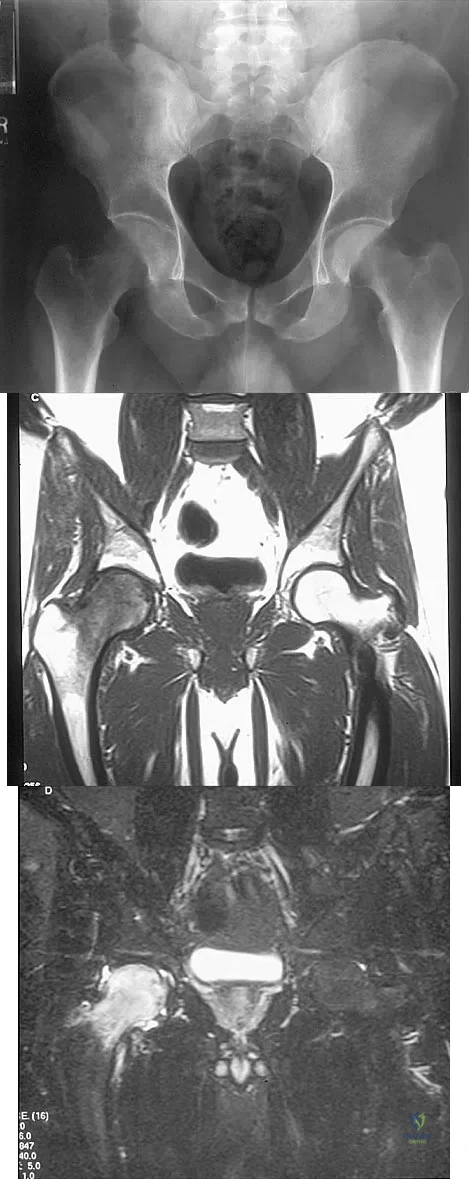
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?
Explanation
Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, "chicken-wire calcification" with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755. Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 51High Yield
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
The major determinant of ALS (Lou Gehrig disease) is progressive loss of motor neurons. The loss usually begins in one area, is asymmetrical, and later becomes evident in other areas. The first signs of ALS may include either upper or lower motor neuron loss. Recognition of upper motor neuron involvement depends on clinical signs, but electromyography and nerve conduction velocity studies can help identify lower motor neuron involvement. Electrodiagnostic abnormalities in three or more areas are required to make a definitive diagnosis. The motor unit potentials (MUPs) changes in ALS include impaired MUPs recruitment, unstable MUPs, and abnormal MUPs size and configuration. A number of abnormal spontaneous discharges can occur with ALS, especially fibrillation potentials and fasciculation potentials. In ALS, the motor nerve conduction study will be abnormal, but a co-existing normal sensory study is definitive for this disease. de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348. Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
References:
- Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 52High Yield
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of

Explanation
Following a CVA and with the resumption of upright posture, downward subluxation of the glenohumeral joint may occur. Although usually painless, some patients may report pain secondary to stretching of the brachial plexus. This is the result of flaccid paralysis of the deltoid muscle, and it will persist until some motor tone or spasticity returns to the shoulder girdle musculature. Early sling support and range-of-motion exercises to prevent contracture will provide the best relief. Surgical procedures are not indicated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 53High Yield
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
Explanation
Repetitive overhead slams and serves may produce a traction injury to the distal branch of the suprascapular nerve. Bankart, biceps, and superior labrum anterior and posterior injuries can occur but usually do not produce visible atrophy. Muscle avulsion is uncommon. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
References:
- Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 54High Yield
Which of the following findings is considered a poor prognostic factor for postoperative neurologic recovery in patients with rheumatoid arthritis?
Explanation
When markedly diminished space available for the cord (demonstrated by a posterior atlantoaxial interval of less than 10 mm) is seen, there is a poor prognosis for recovery (25% of Ranawat class IIIb patients) following surgery. A posterior atlantoaxial interval of 14 mm or less is a predictor of increased risk of paralysis, but patients with an interval between 10 mm and 14 mm have a greater chance of recovery. Space available for the cord that is at least 14 mm is not associated with an increased risk of neurologic deficit. Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 55High Yield
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
In the study done by Pevny and associates, 35% of patients older than age 40 years sustained rotator cuff tears and 8% had axillary nerve palsies. All of the patients with axillary nerve palsy also had rotator cuff tears. Imaging of the rotator cuff is indicated in this age group. The incidence of recurrent instability in patients older than age 40 years is 10% to 15%. Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294. Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Question 56High Yield
Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?
Explanation
Explanation
The factors that are independently prognostic of patient survival are tumor size, tumor grade, and tumor depth (ie, subfascial versus superficial). These factors are the basis for the American Joint Committee on Cancer staging criteria. Patient age and neurovascular invasion are not prognostic. Surgical margin is prognostic for local recurrence but not conclusively for patient survival or metastasis. Metastatic disease is also predictive of survival. Cheng EY, Thompson RC Jr: New developments in the staging and imaging of soft-tissue sarcomas. Instr Course Lect 2000;49:443-451.
References:
- Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 57High Yield
Examination of a 23-year-old female college basketball player who has had anterior knee pain for the past 3 weeks reveals tenderness and fullness over the inferior patella and proximal patellar tendon. There is no patellofemoral crepitus, patella apprehension sign, or anterior or posterior instability. Initial management should include
Explanation
The patient has patellar tendinitis (jumper's knee). It is a common overuse condition seen in runners, volleyball players, soccer players, and jumpers but can be seen in any activity in which repeated extension of the knee is required. In the acute setting, the pain is well localized and there is tenderness and sometimes swelling of the tendon. MRI is recommended for evaluating chronic cases and for surgical planning. In the acute phases, ice, rest, and avoidance of the offending activity are recommended. Weakness of the quadriceps and hamstring muscle are thought to contribute to this problem; therefore, stretching and isometric exercise in a limited range of motion are important. Complete rest and intratendinous injections of steroids are detrimental to tendon physiology. Stanish WD, Rubinovich RM, Curwin S: Eccentric exercise in chronic tendinitis. Clin Orthop 1986;208:65-68.
Question 58High Yield
What is the best approach to reduce and stabilize a displaced volar lunate facet fracture of the wrist?
Explanation
Explanation
A volar lunate fragment of a distal radial fracture is considered a critical component to overall joint stability and function. Obtaining a reduction is difficult through a standard volar approach to the radius between the flexor carpi radialis and radial artery. Visualization and reduction of the ulnar volar facet is not possible from this approach. An extended carpal tunnel incision provides access to the entire articular surface, except for the distal radial styloid component. Hanel DP, Jones MD, Trumble TE: Wrist fractures. Orthop Clin North Am 2002;33:35-57.
References:
- Trumble TE, Culp RW, Hanel DP, et al: Intra-articular fractures of the distal aspect of the radius. Instr Course Lect 1999;48:465-480.
Question 59High Yield
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include

Explanation
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 60High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 61High Yield
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
Explanation
Explanation
The transfemoral approach, also known as the extended trochanteric osteotomy, is an important technique to master for revision hip surgery. When performed correctly, it allows excellent exposure of the femoral canal and aids in exposure of the acetabulum. As demonstrated in the study cited, however, it markedly reduces the torque that the composite can withstand without failure. This type of basic science study is important to guide postoperative rehabilitation.
References:
- Noble AR, Branham D, Willis M, et al: Mechanical effects of the extended trochanteric osteotomy. J Bone Joint Surg Am 2005;87:521-529.
Question 62High Yield
In the setting of a proximal tibial plateau fracture and its repair, which of the following materials is an isotropic material?
Explanation
Explanation
An isotropic material is one that has similar mechanical properties regardless of the orientation of the material. Examples of isotropic materials include metals, plastics, and methacrylate. Most biologic tissues are anisotropic, meaning their mechanical properties alter depending on the materials' orientation to the applied stress.
Question 63High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 64High Yield
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of
Explanation
Explanation
The patient has arthritis and supracondylar nonunion of the elbow. Total elbow replacement has been shown to give almost immediate return of function as it can be performed while leaving the triceps intact and resecting the distal humerus fragment. Attempts at osteosynthesis are indicated in younger individuals with good joint surface. Resection arthroplasty yields poor function and is reserved as a salvage procedure. Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
References:
- Sim FH, Morrey BF: Nonunion and delayed union of distal humeral fractures, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Question 65High Yield
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of
Explanation
Explanation
3b 3c The radiographs show polyethylene wear, but exchange of this will not necessarily provide pain relief. The presence of pain suggests the possibility of occult loosening, and the surgeon must be prepared for this option intraoperatively. There is little evidence of infection. Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
References:
- Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
Question 66High Yield
When compared with a patient who has a subluxated hip, a patient with a dislocated hip who is undergoing acetabular reconstruction for developmental dysplasia of the hip will most likely have
Explanation
Explanation
The rate of revision has been found to be significantly increased in patients with a dislocated hip preoperatively compared with patients with a subluxated hip. This may be the result of compromised acetabular bone stock. The rate of nerve palsy may be increased because of the greater degree of lengthening required to reduce the reconstructed hip. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
References:
- Schmalzried TP, Noordin S, Amstutz HC: Update on nerve palsy associated with total hip replacement. Clin Orthop 1997;344:188-206.
Question 67High Yield
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
Explanation
If a woman has two or more osteoporotic compression fractures, her risk of another is increased 12 fold. A decrease of two standard deviations in bone mineral density increases the risk four to six fold, a positive family history 2.7 fold, premature menopause 1.6 fold, and smoking 1.2 fold. It should be noted that these studies were carried out in Caucasian and Asian women. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-11S.
References:
- Ross PD, Davis JW, Epstein RS, Wasnich RD: Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 1991;114:919-923.
Question 68High Yield
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
Explanation
A discrete or focal callus is a response to excessive weight-bearing stress beneath the lateral (fibular) condyle of a lesser metatarsal head (most commonly second). The other structures generally have not been associated with a discrete callus. Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
References:
- Cracchiolo A: Surgical procedures of the lateral metatarsals, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1269-1283.
Question 69High Yield
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of

Explanation
Based on the mechanism of injury and findings of medial laxity, the most likely diagnosis is injury to either the growth plate or the medial collateral ligament. With the open physeal plate, this area of injury is presumed present until proven otherwise; therefore, stress radiographs should be obtained before implementing any treatment or ordering more extensive and expensive tests. DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 406-432. Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Question 70High Yield
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
Explanation
The lesion is typical of a subungual exostosis, which is most often found on the medial aspect of the great toe in children and young adults. The diagnosis is confirmed on radiographs and usually requires excision for relief. Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79. Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
References:
- Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 71High Yield
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?

Explanation
A chordoma is a malignant neoplasm originating from remnants of the notochord. It is usually localized to the midline with 50% at the sacrococcygeal area, 35% at the skull base, and 15% at the mobile portion of the spine. Large vacuolated cells (physaliferous cells) are a characteristic of the tumor. Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Question 72High Yield
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
Explanation
Gamma irradiation has long been used as a sterilization method for polyethylene. Exposure to gamma irradiation causes breakage of the chemical bonds in the polyethylene, and oxidation will occur if the material is subsequently exposed to air. The amount of oxidation and decrease in wear performance is also related to the length of time that the gamma-irradiated polyethylene is exposed to oxygen. Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86. McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 73High Yield
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
Explanation
The anterior cruciate ligament can be visualized on an axial MRI scan as a low-signal structure lying in the lateral aspect of the intercondylar notch. Visualization in multiple planes increases the accuracy of MRI to view the anterior cruciate ligament. The posterior cruciate ligament and ligament of Wrisberg are located on the medial wall of the notch. The ligamentum mucosum is anterior to the notch, and the popliteus tendon is posterior to the lateral femoral condyle. Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
References:
- Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 74High Yield
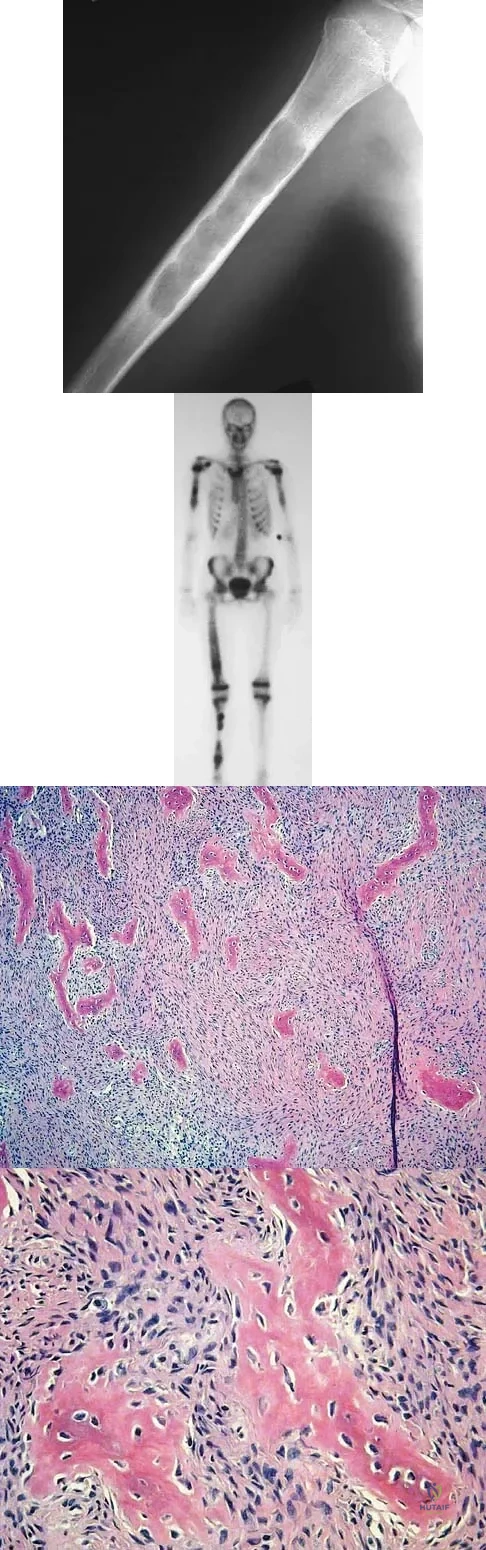
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?
Explanation
Based on these findings, the most likely diagnosis is fibrous dysplasia. Twenty percent of patients with fibrous dysplasia have multifocal disease. The lesions show a typical ground glass appearance. Fibrous dysplasia frequently involves the diaphysis of the long bones. There is no associated soft-tissue mass and no periosteal reactions to these lesions, suggesting a benign lesion. The histology shows proliferating fibroblasts in a dense collagen matrix. Trabeculae are arranged in an irregular or "Chinese letter" appearance. Osteogenic sarcoma and Ewing's sarcoma have a much different radiographic appearance of malignant osteoid and small round blue cells. Periosteal chondroma does occur in the proximal humerus but is not typically multifocal. It appears as a surface lesion with saucerization of the underlying bone and a bony buttress adjacent to the lesion. Some patients with multifocal lesions have associated endocrine abnormalities (McCune-Albright syndrome). Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Question 75High Yield
Pain associated with a proximal medial tibial osteochondroma in a 10-year-old patient is most commonly the result of
Explanation
Pain secondary to an osteochondroma is usually from soft-tissue irritation and bursal formation. This is particularly common for proximal medial tibia osteochondromas that irritate the pes anserine tendons. Malignant degeneration into a chondrosarcoma rarely occurs, is usually associated with multiple hereditary exostoses, and usually occurs after skeletal maturity. Borges AM, Huvos AG, Smith J: Bursa formation and synovial chondrometaplasia associated with osteochondromas. Am J Clin Pathol 1981;75:648-653.
Question 76High Yield
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Explanation
Explanation
The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal. Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
References:
- McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
Question 77High Yield
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren's contracture?
Explanation
The normal fascial components that become diseased and compose the spiral cord include the pretendinous band, spiral band, lateral digital sheet, and Grayson's ligament. Cleland's ligament lies dorsal and is not involved with spiral cord formation. The intrinsic muscle and tendon, the natatory ligament, and the intermetacarpal ligament are well proximal to the digit and are not involved in spiral cord formation. McGrouther D: Dupuytren's contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 1, pp 565-569.
Question 78High Yield
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling's test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?

Explanation
The definition of brachial neuritis or Parsonage-Turner syndrome is a rare disorder of unknown etiology that causes pain or weakness of the shoulder and upper extremity. The loss of active motion excludes cervical C6-7 radiculopathy and impingement. A normal MRI scan and full passive motion exclude a rotator cuff tear and adhesive capsulitis, respectively. Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Question 79High Yield
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?
Explanation
Transient osteoporosis is a self-limited painful but reversible disorder. Although first described in pregnant women, it is more common in young to middle-aged men. The radiograph shows loss of mineralization in the right hip relative to the left side. There is no osseous destruction or cortical expansion typical of metastasis or giant cell tumor. The process is confined to the femoral side of the joint unlike rheumatoid arthritis, which would be centered in the joint. Osteonecrosis is better defined with sharp but irregularly shaped margins, and there is no double-line sign. The MRI scans reveal diffuse edema in the femoral head and neck that is atypical for osteonecrosis. Transient osteoporosis may recur in the same or opposite hip.
Question 80High Yield
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?

Explanation
The work-up for a patient with an unknown primary lesion that is metastatic to bone includes a search for the primary tumor and other sites of metastasis. This involves conducting a thorough history and physical examination, appropriate laboratory studies, bone scan, chest radiograph, and CT of the chest, abdomen, and pelvis. In women, a mammogram may be indicated. CT of the brain is not necessary in the early stages of a metastatic work-up. Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Question 81High Yield
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Explanation
Explanation
Suprascapular nerve injuries are more commonly seen in athletes who participate in overhead activities. When a patient is evaluated for posterior shoulder pain and infraspinatus muscle weakness or atrophy, electrodiagnostic studies are an essential part of the evaluation. In addition, imaging studies are indicated to exclude other diagnoses that can mimic a suprascapular nerve injury. Initial management should consist of cessation of the aggravating activity along with an organized shoulder rehabilitation program. If nonsurgical management fails to provide relief within 6 months to 1 year, surgical exploration of the suprascapular nerve should be considered. Release of the spinoglenoid ligament with resultant suprascapular nerve decompression may result in pain relief and a return of normal shoulder function. In this patient, who has a chronic neuropathy and mild symptoms, surgery is indicated only if nonsurgical management fails to provide relief and he is unable to perform at his position. Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
References:
- Ferretti A, De Carli A, Fontana M: Injury of the suprascapular nerve at the spinoglenoid notch: The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med 1998;26:759-763.
Question 82High Yield
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are
Explanation
Explanation
Retrieval studies have shown that the debris particles produced by metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations. Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J Bone Joint Surg Am 2005;87:18-27.
References:
- Firkins PJ, Tipper JL, Saadatzadeh MR, et al: Quantitative analysis of wear and wear debris from metal-on-metal hip prostheses tested in a physiological hip joint simulator. Biomed Mater Eng 2001;11:143-157.
Question 83High Yield
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?
Explanation
The incidence of injury associated with horseback rising is estimated to be one per 350 riding hours to one per 1,000 riding hours. Of these injuries, approximately 15% to 27% are severe enough to warrant hospital admission. Significant and serious injuries in equestrian activities are associated with recreational riders and those not wearing a helmet. Head and spine injuries are more common in recreational and nonhelmeted riders. Extremity injuries are more common in professional and helmeted riders. Professional riders are less likely to be admitted to the hospital than recreational riders, and are about half as likely to be disabled at 6 months after injury as recreational riders. Lim J, Puttaswamy V, Gizzi M, et al: Pattern of equestrian injuries presenting to a Sydney teaching hospital. ANZ J Surg 2003;73:567-571.
Question 84High Yield
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Explanation
Explanation
Acetabular component loosening has been reported as the most common mode of failure following total hip arthroplasty in patients with a previous acetabular fracture. Following acetabular fracture and subsequent open reduction and internal fixation, the bone quality and vascularity are compromised, thus reducing the success rate of acetabular component cementless fixation. Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
References:
- Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 85High Yield
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of
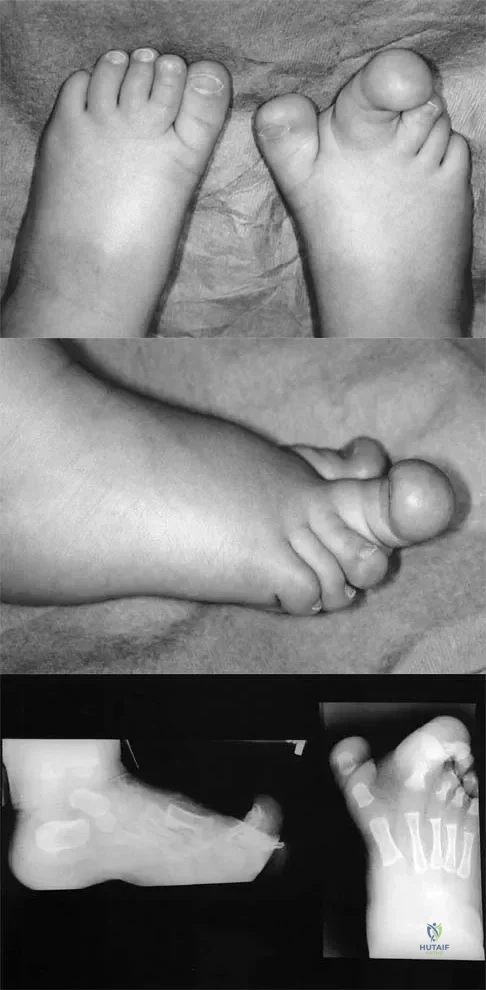
Explanation
The patient has macrodactyly involving the second ray, with significant enlargement of the width and height of the foot. The radiographs show widening of the interval between the first and second metatarsal and between the second and third metatarsal. With this degree of involvement, amputation of the second ray with excision of the overgrowth of affected soft tissue provides the most consistent desired reduction in foot size. A threaded Steinmann pin should be inserted across the remaining metatarsals until healing has occurred. Patients with macrodactyly should be examined to exclude neurofibromatosis type 1 and Klippel-Trenaunay-Weber syndrome.
Question 86High Yield
A 44-year-old woman has bilateral knee pain, and history reveals bilateral hip replacements. Radiographs are seen in Figure 28a, and histopathologic specimens from the total hip replacement are shown in Figures 28b and 28c. Laboratory studies reveal anemia. What is the most likely diagnosis?
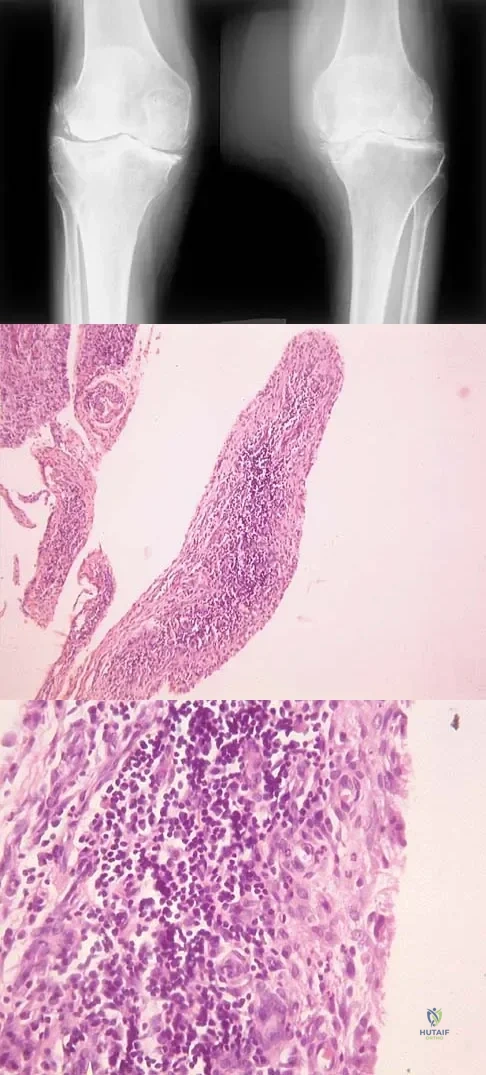
Explanation
Rheumatoid arthritis is an inflammatory arthritis that usually involves multiple joints. Radiologic findings of periarticular erosion, osteopenia, and minimal osteophyte formation favor rheumatoid arthritis over osteoarthritis. Pigmented villonodular synovitis and Charcot arthropathy are more often considered monoarticular diseases. There are no radiographic findings of Paget's disease.
Question 87High Yield
The condition shown in Figures 9a and 9b is most likely the result of

Explanation
The clinical photograph and radiograph show gout, which is the result of urate deposition in the joint and soft tissues. Radiographs frequently reveal periarticular erosions. The crystals are intracellular and negatively birefringent under the polarized microscope. Treatment for acute flares include colchicines, indomethacin, and corticosteroids (including injections). Medications such as allopurinol help prevent recurrent flares. Tophi such as that seen in this patient are often confused with and associated with infection. Wortmann RL, Kelley WM: Crystal-induced inflammation: Gout and hyperuricemia, in Harris ED, Budd RC, Firestein GS, et al (eds): Kelley's Textbook of Rheumatology, ed 7. New York, NY, Elsevier Science, 2005, pp 1402-1429. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 88High Yield
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the
Explanation
Explanation
Capsular exposure for an inside-out lateral meniscal repair is performed by developing the interval between the iliotibial band and biceps tendon. Posterior retraction of the biceps tendon exposes the lateral head of the gastrocnemius. Posterior retraction of the gastrocnemius provides access to the posterolateral capsule. Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
References:
- Nawab A, Hester PW, Caborn DN: Arthroscopic meniscus repair, in Miller MD, Cole BJ (eds): Textbook of Arthroscopy. Philadelphia, PA, WB Saunders, 2004, pp 517-537.
Question 89High Yield
The lower extremity motor dysfunction in Charcot-Marie-Tooth disease most commonly involves which of the following muscles?
Explanation
Explanation
The motor dysfunction in Charcot-Marie-Tooth disease involves the tibialis anterior muscle. Charcot-Marie-Tooth disorders most commonly cause distal motor dysfunction in the foot intrinsics, anterior compartment musculature, and peroneals. There is evidence that the peroneus brevis is affected selectively and the peroneus longus is spared. This is based on clinical muscle testing, muscle cross-sections on MRI, and electrodiagnostic testing. Mann RA, Missirian J: Pathophysiology of Charcot-Marie-Tooth disease. Clin Orthop 1988;234:221-228.
References:
- Tynan MC, Klenerman L, Helliwell TR, Edwards RH, Hayward M: Investigation of muscle imbalance in the leg in symptomatic forefoot pes cavus: A multidisciplinary study. Foot Ankle 1992;13:489-501.
Question 90High Yield
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a "pop" in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
Explanation
Injury to the latissimus dorsi tendon recently has been reported as a cause of pain in the thrower's shoulder. The etiology of this injury is felt to be eccentric overload during the follow-through of the throwing motion. Recommended management for this unusual injury consists of a short period of rest, followed by physical therapy to restore shoulder motion and strength. Throwing is allowed when the athlete demonstrates full, pain-free motion and good strength and balance of the rotator cuff and scapular rotator muscles. Currently there are no defined indications for surgical repair. Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
References:
- Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
Question 91High Yield
Intradiskal electrothermal therapy (IDET) uses an intradiskal catheter to deliver controlled thermal energy to the inner periphery of the annulus fibrosis of a chronically painful intervertebral disk. Lumbar diskography is used diagnostically to identify the presumed pain generator to be targeted with IDET. Based on the medical literature, what can be said about the current status of IDET?
Explanation
Intradiskal electrothermal therapy (IDET) initial clinical results were reported in 2000. The early case series were quite encouraging with reported therapeutic success rates of 60% to 80%. Early enthusiasm was high as IDET provided a nonsurgical treatment option for an otherwise complex and difficult clinical entity, chronic diskogenic low back pain. The actual mechanism of action was not well understood, and while the theoretic explanation made good sense, it did not hold up under laboratory testing. Soon clinical results from the field did not meet the high expectations set by the developers of the technique. Since those early case studies, a few level I evidence studies have been conducted, one by Freeman and associates and one by Pauza and associates. These randomized, placebo-controlled trials demonstrated no significant benefit of IDET over the placebo. Freeman BJ, Fraser RD, Cain CM, et al: A randomized, double-blind, controlled trial: Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 2005;30:2369-2377. Pauza KJ, Howell S, Dreyfuss P, et al: A randomized, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 2004;4:27-35.
Question 92High Yield
What is the first ossification center to appear radiographically in the pediatric elbow?
Explanation
Explanation
The first ossification center to appear in the pediatric elbow is the capitellum. This ossification center generally appears between the first month and the 11th month in girls and between the first month and the 26th month in boys. The other ossification centers in the elbow appear in the following progression: radial head (3.8 to 4.5 years), medial epicondyle (5 to 6 years), olecranon (6 to 7 years), trochlea (9 to 10 years), and the lateral epicondyle (10 years). Wilkins KE, Beaty JH, Chambers HG, et al: Fractures and dislocation of the elbow region, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 657-662.
References:
- Haraldsson S: On osteochondrosis deformans juvenilis capituli humeri including investigation of the intra-osseous vasculature in the distal humerus. Acta Orthop Scand 1959;38:1-232.
Question 93High Yield
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?
Explanation
Explanation
31b The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
References:
- Kier R, McCarthy SM: Lipohemarthrosis of the knee: MR imaging. J Comput Assist Tomogr 1990;14:395-396.
Question 94High Yield
A 38-year-old man reports a 2-week history of acute lower back pain with radiation into the left lower extremity. There is no history of trauma and no systemic signs are noted. Examination reveals a positive straight leg test at 35 degrees on the left side and a contralateral straight leg raise on the right side. Motor testing demonstrates mild weakness of the gluteus medius and weakness of the extensor hallucis longus of 3+/5. Sensory examination demonstrates decreased sensation along the lateral aspect of the calf and top of the foot. Knee and ankle reflexes are intact and symmetrical. Radiographs demonstrate no obvious abnormality. MRI scans show a posterolateral disk hernation. The diagnosis at this time is consistent with a herniated nucleus pulposus at
Explanation
Explanation
The patient's history and physical examination findings are consistent with a lumbar disk herniation at the L4-5 level. Weakness of the extensor hallucis longus and gluteus medius are consistent with an L5 lumbar radiculopathy. Nerve root tension signs are also consistent with sciatica from a lumbar disk herniation. The MRI scans confirm a posterolateral disk herniation at L4-5, which typically affects the exiting L5 nerve root. Hoppenfeld S: Orthopedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 45-74.
Question 95High Yield
Figure 44 shows the AP radiograph of the hip of a patient who underwent screw fixation of the acetabulum. Which of the following structures is at least risk for injury during screw placement in the acetabular component?

Explanation
Acetabular screws are inserted to supplement fixation. The acetabular component can be divided into four quadrants. Anatomic studies have shown that screws placed in the anterior superior and anterior inferior quadrants of the cup may injure the external iliac vein and obturator artery, respectively. Posterior superior and posterior inferior placement (in screws greater than 25 mm) may injure the sciatic nerve or the superior gluteal artery. The common iliac artery is proximal to the acetabulum and is at least risk for injury from acetabular screw placement.
Question 96High Yield
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
Explanation
The tendon most prone to rupture in a patient with rheumatoid arthritis of the wrist is the extensor digiti quinti. It can be a silent injury since the extensor digitorum communis can provide extension to the fifth finger. The extensor digiti quinti is at high risk since it is overlying the ulnar head where it is prone to attritional rupture (Vaughan-Jackson syndrome). Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
References:
- Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg 2006;14:65-77.
Question 97High Yield
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 98High Yield
A 47-year-old man with Charcot-Marie-Tooth (CMT) disease was treated with a fifth metatarsal head resection for a symptomatic bunionette 2 years ago. What is the most likely complication seen at this time?
Explanation
Explanation
CMT is characterized by a cavovarus foot position that increases weight-bearing stresses along the lateral border. Removal of the fifth metatarsal head carries the risk of creating a transfer lesion at the fourth metatarsal head, particularly with a cavovarus foot. Claw toes are common in CMT, but the fifth toe would be flail in this situation. Ulceration is unlikely given the lack of underlying bone. Peroneal atrophy is associated with CMT but would not be a complication of this procedure. Charcot arthropathy is a neuropathic process frequently seen in individuals with diabetes mellitus. Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term followup. Foot Ankle 1991;11:345-349.
References:
- Coughlin MJ, Mann RA, Saltzman CL: Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 1312-1315.
Question 99High Yield
An obese 10-year-old boy has had left groin pain and a limp for the past 2 months. Examination reveals decreased abduction and internal rotation. Laboratory studies show normal renal function and an elevated thyroid-stimulating hormone (TSH) level. AP and frog lateral radiographs of the pelvis are shown in Figures 30a and 30b. What is the best course of action?
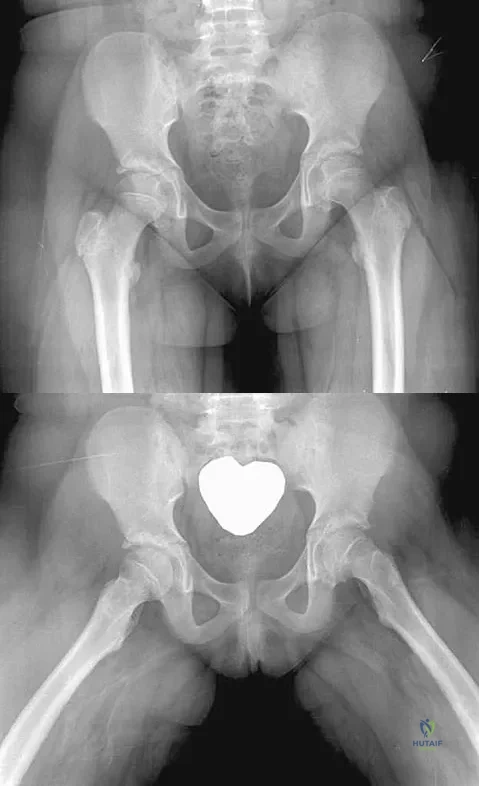
Explanation
The radiographs show a grade I slipped capital femoral epiphysis (SCFE) that is classified as stable because the child is able to bear weight. The elevated TSH level indicates possible hypothyroidism. SCFE usually occurs in boys age 12 to 14 years. Because of the patient's young age and hypothyroidism, he is at increased risk for slippage of the contralateral hip; therefore, prophylactic pinning of the uninvolved side also should be considered. Because of the risk of slip progression, crutch treatment and nonsteroidal anti-inflammatory drugs are not indicated. Realignment osteotomy is not indicated for grade I SCFE. Traction to reduce the slip, followed by pinning, has been advocated for unstable slips but is not indicated here. Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 100High Yield
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?

Explanation
Instability is a leading cause of failure following total knee arthroplasty. Instability can present as global instability, extension gap (varus/valgus) instability, or flexion gap (anterior/posterior) instability. Treatment options are numerous based on the exact pathology. The radiograph reveals anterior/posterior instability with dislocation consistent with flexion gap instability. A loose flexion gap can allow the femoral component to ride above the tibial cam post mechanism, resulting in dislocation. Distal femoral augments treat extension gap instability, whereas tibial augments can treat both flexion and extension gap instability. Posterior condyle augments at the distal femur can also be used to treat flexion gap instability. Flexion gap instability is further aggravated by extension mechanism incompetence. Note the excessively thin patella on the lateral radiograph. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding applied-surgical-anatomy-of-the-posterior-approaches-to-the-hip-and-the-acetabulum