AAOS & ABOS Orthopedic MCQs (Set 3): Hip & Knee Arthroplasty & Revision
Key Takeaway
This high-yield question set for AAOS and ABOS exams (Set 3) focuses on the diagnosis and advanced management of hip and knee reconstruction. It covers primary and revision arthroplasty techniques, implant selection, failure analysis, and strategies for common complications, preparing residents and surgeons for board certification.
AAOS & ABOS Orthopedic MCQs (Set 3): Hip & Knee Arthroplasty & Revision
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
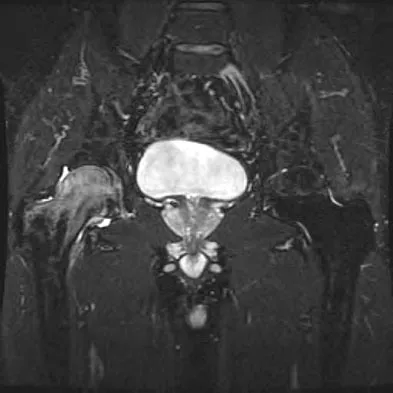
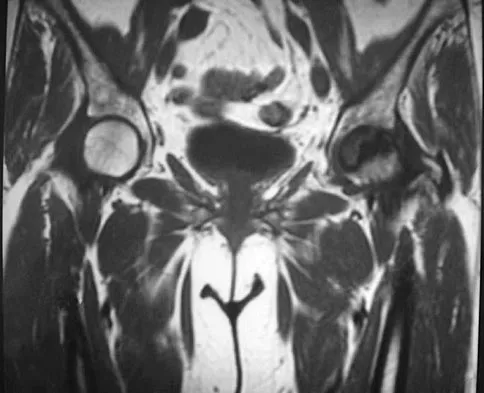
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
Explanation
Question 2
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
Explanation
Question 3
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
Question 4
When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides
Explanation
Question 5
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
Explanation
Question 6
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
Explanation
Question 7
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?
Explanation
Question 8
Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?
Explanation
Question 9
Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?
Explanation
Question 10
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
Question 11
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 12
Figure 37 reveals a periprosthetic fracture around a cemented femoral stem in an 81-year-old patient with Paget's disease and mild coagulopathy. What is the most appropriate reconstructive management on the femoral side?
Explanation
Question 13
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
Question 14
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
Question 15
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
Explanation
Question 16
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Question 17
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
Question 18
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?
Explanation
Question 19
A 67-year-old patient seen in the emergency department reports the acute onset of pain and is unable to ambulate. History reveals that the patient underwent surgical treatment for a periprosthetic femoral fracture 6 months ago. A radiograph is shown in Figure 41. What is the best treatment option at this time?
Explanation
Question 20
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
Question 21
Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
Explanation
Question 22
In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type
Explanation
Question 23
Figures 43a and 43b show the T1- and T2-weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
Question 24
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
Explanation
Question 25
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
Question 26
During a primary total knee arthroplasty trial reduction, the knee is well-balanced and stable in full extension but is excessively tight at 90 degrees of flexion. Which of the following intraoperative interventions is the most appropriate next step to specifically address the tight flexion gap?
Explanation
Question 27
A 68-year-old man undergoes primary total knee arthroplasty. Intraoperatively, with trial components in place, the knee is appropriately balanced and tight in extension but opens 4 mm symmetrically both medially and laterally when assessed at 90 degrees of flexion. What is the most appropriate next step to achieve a balanced knee?
Explanation
Question 28
A 65-year-old man presents with progressive groin pain 5 years after receiving a metal-on-polyethylene total hip arthroplasty. Radiographs demonstrate well-fixed components with no osteolysis. Serum cobalt is 8.5 ppb and chromium is 1.2 ppb. MARS MRI shows a mixed solid and cystic mass in the abductor musculature. What is the most likely etiology?
Explanation
Question 29
A 70-year-old woman presents with a painful "catching" sensation anteriorly when extending her knee from 45 degrees of flexion to full extension, 1 year after a posterior-stabilized total knee arthroplasty. What is the most likely diagnosis?
Explanation
Question 30
During a direct anterior (Smith-Petersen) approach to the hip for a primary total hip arthroplasty, the superficial surgical dissection passes between which of the following internervous muscle intervals?
Explanation
Question 31
According to current evidence and criteria for periprosthetic joint infection (PJI), which of the following synovial fluid biomarkers provides the highest sensitivity and specificity for diagnosing PJI?
Explanation
Question 32
To recreate a neutral mechanical axis during a primary total knee arthroplasty in a patient with a normal femoral bow, the distal femoral cut should typically be made at what angle relative to the anatomic axis of the femur?
Explanation
Question 33
To minimize the risk of dislocation following a primary total hip arthroplasty, the acetabular component should ideally be placed in which of the following "safe zone" target orientations?
Explanation
Question 34
In a cruciate-retaining total knee arthroplasty, over-resection of the posterior tibial slope can lead to which of the following kinematic abnormalities?
Explanation
Question 35
A 72-year-old woman requires revision THA for aseptic loosening.
Radiographs demonstrate a Paprosky Type IIIA acetabular defect with superior migration of the hip center by 2.5 cm and intact Kohler's line. Which of the following is the most appropriate reconstruction technique?

Explanation
Question 36
A 75-year-old woman sustains a displaced supracondylar femur fracture (Rorabeck Type II) directly proximal to a well-fixed posterior-stabilized total knee arthroplasty. The femoral component has a closed-box design. What is the most appropriate surgical management?
Explanation
Question 37
A 78-year-old man falls and sustains a periprosthetic femur fracture around his THA. Radiographs show a fracture at the tip of the stem. The stem is radiographically loose, but the proximal femoral bone stock remains robust (Vancouver B2). What is the standard of care?
Explanation
Question 38
A 69-year-old man presents with an inability to actively extend his knee 3 years after a primary total knee arthroplasty. Ultrasound confirms a complete mid-substance rupture of the patellar tendon. What is the most reliable surgical option for restoring extensor function?
Explanation
Question 39
A 60-year-old woman complains of new-onset, sharp groin pain with active hip flexion, such as getting into a car, 6 months after an uncomplicated THA. Radiographs show the acetabular cup is retroverted and prominent anteriorly. What is the most appropriate initial management?
Explanation
Question 40
During a two-stage exchange arthroplasty for a chronic periprosthetic joint infection of the knee, an articulating antibiotic spacer is placed. What is the primary advantage of an articulating spacer over a static spacer?
Explanation
Question 41
Following a total hip arthroplasty via a posterior approach, a patient exhibits a foot drop and inability to extend the great toe, but plantar flexion and foot inversion remain intact. Which specific nerve division is most likely injured?
Explanation
Question 42
During a primary total knee arthroplasty, failure to adequately resect the native patella before placing the patellar component results in an "overstuffed" patellofemoral joint. This technical error is most likely to cause which of the following complications?
Explanation
Question 43
During a posterior-stabilized total knee arthroplasty, trial reduction reveals that the knee is perfectly balanced in extension but significantly tight in flexion. Which of the following is the most appropriate surgical step to balance the gaps?
Explanation
Question 44
Highly cross-linked polyethylene (HXLPE) is widely used in total hip arthroplasty to reduce wear. Which of the following manufacturing processes is critical to eliminate free radicals and reduce in vivo oxidation of HXLPE?
Explanation
Question 45
A 62-year-old female presents with groin pain and a palpable mass five years after a metal-on-metal total hip arthroplasty. Aspiration of the hip yields aseptic fluid, and serum cobalt and chromium levels are elevated. Histological examination of the periprosthetic tissue is most likely to show which of the following?
Explanation
Question 46
A 75-year-old male sustains a fall and suffers a periprosthetic fracture around his cemented total hip arthroplasty.
Radiographs demonstrate a fracture around the tip of the stem with evidence of cement mantle fragmentation and subsidence of the femoral component. Which of the following is the most appropriate management?
Explanation
Question 47
According to the 2018 International Consensus Meeting on Periprosthetic Joint Infection, which of the following synovial fluid profiles strongly supports the diagnosis of an acute periprosthetic joint infection (within 4 weeks of surgery)?
Explanation
Question 48
A 68-year-old male presents with a painful catching sensation and an audible clunk as his knee extends from 40 degrees of flexion to full extension, 18 months after a posterior-stabilized total knee arthroplasty. What is the most common cause of this phenomenon?
Explanation
Question 49
A surgeon is performing a total hip arthroplasty via the direct anterior approach. When preparing the femur, excessive retraction is applied to the medial soft tissues. Which of the following structures is at greatest risk of injury?
Explanation
Question 50
A 70-year-old female presents with an inability to actively extend her knee 3 years following a total knee arthroplasty. Evaluation confirms a chronic, massive rupture of the patellar tendon with severe tissue retraction and poor host tissue quality. Which of the following is the most reliable reconstructive option?
Explanation
Question 51
During a primary total knee arthroplasty, the surgeon finds the joint is perfectly balanced in flexion but tight in extension. Which of the following is the most appropriate surgical step to correct this mismatch?
Explanation
Question 52
A 65-year-old man presents with progressive groin pain 5 years after receiving a metal-on-polyethylene total hip arthroplasty. Aspiration is negative for infection. Blood tests reveal serum cobalt levels that are significantly higher than chromium levels. What is the most likely etiology of his symptoms?
Explanation
Question 53
A 78-year-old woman presents with thigh pain after a ground-level fall. Radiographs demonstrate a fracture around her cemented polished taper-slip femoral stem. The fracture occurs at the level of the stem tip, and the stem is clearly loose within the cement mantle, but the proximal bone stock remains adequate. According to the Vancouver classification, what is the most appropriate management?
Explanation
Question 54
A 60-year-old man presents with a painful total knee arthroplasty 3 years postoperatively. His ESR is 45 mm/hr and CRP is 25 mg/L. Joint aspiration yields a white blood cell count of 3,500 cells/uL with 85% neutrophils. Synovial alpha-defensin testing is positive. Based on the 2018 ICM criteria, what is the definitive diagnosis?
Explanation
Question 55
When converting a standard offset femoral stem to a high offset femoral stem of the exact same neck angle during total hip arthroplasty, what is the expected biomechanical effect on the hip joint?
Explanation
Question 56
During a trial reduction for a posterior-stabilized total knee arthroplasty, the surgeon notes significant lateral patellar subluxation. Which of the following component positioning errors is the most likely cause of this maltracking?
Explanation
Question 57
A 45-year-old active man with a ceramic-on-ceramic total hip arthroplasty reports an audible squeaking noise from his hip when bending over. Which of the following factors is most strongly associated with the development of this phenomenon?
Explanation
Question 58
A 70-year-old woman is 1 year status post a posterior-stabilized total knee arthroplasty. She reports a sensation of giving way, especially when descending stairs. On examination, the knee is completely stable in full extension but exhibits excessive anterior-posterior laxity at 90 degrees of flexion. What is the most likely intraoperative cause of her symptoms?
Explanation
Question 59
A 68-year-old woman is undergoing revision total hip arthroplasty for aseptic loosening. Preoperative imaging
demonstrates superior migration of the hip center by 4 cm and medial migration past Kohler's line. Severe osteolysis of the ischium and teardrop is noted. What is the Paprosky classification of this acetabular defect?
Explanation
Question 60
Highly cross-linked polyethylene was introduced to drastically reduce wear rates in total joint arthroplasty. Which of the following thermal processing steps is specifically performed to eliminate residual free radicals, but results in a slight decrease in the material's mechanical yield strength?
Explanation
Question 61
A 62-year-old man presents with acute onset of severe knee pain, swelling, and a low-grade fever exactly 3 weeks after an uncomplicated primary total knee arthroplasty. Joint aspiration reveals frankly purulent fluid. What is the most appropriate initial surgical management?
Explanation
Question 62
A 55-year-old woman with a metal-on-metal total hip arthroplasty presents with new-onset groin pain and a palpable soft tissue mass. Radiographs show well-fixed components.
Metal artifact reduction sequence (MARS) MRI reveals a large cystic fluid collection. What histologic finding is most characteristic of this condition?

Explanation
Question 63
Six months after a posterior-stabilized total knee arthroplasty, a patient reports a painful catching and popping sensation at the anterior knee when extending from a flexed position. The catch typically occurs around 30 to 45 degrees of flexion. What is the most definitive surgical management for this condition if conservative measures fail?
Explanation
Question 64
During revision total hip arthroplasty for a massive acetabular defect, the surgeon evaluates the remaining bone and notes that the superior hemipelvis moves completely independently from the inferior hemipelvis upon applied stress. Which of the following is an essential biomechanical requirement when reconstructing this specific defect?
Explanation
Question 65
A patient presents for total knee arthroplasty with an extra-articular diaphyseal femoral deformity consisting of 15 degrees of varus bowing. According to established alignment principles, what is the best intra-articular adjustment to achieve a neutral postoperative mechanical axis without performing a corrective femoral osteotomy?
Explanation
Question 66
A patient presents with lateral patellar subluxation following a primary total knee arthroplasty. Which of the following component malpositions is the most likely cause?
Explanation
Question 67
A 72-year-old woman sustains a periprosthetic femur fracture 10 years after a cemented THA. Radiographs show a fracture around the tip of the stem. The stem is loose, but the proximal femoral bone stock is well preserved. According to the Vancouver classification, what is the most appropriate management?
Explanation
Question 68
What is the primary cellular mechanism of osteolysis induced by polyethylene wear debris in total joint arthroplasty?
Explanation
Question 69
A 55-year-old man who underwent a metal-on-metal THA 6 years ago presents with new-onset groin pain and a palpable anterior mass. Joint aspiration yields sterile fluid with elevated cobalt levels. What is the most likely histological finding of the periprosthetic tissue?
Explanation
Question 70
During a primary TKA, after making the initial bony cuts, the surgeon notices that the knee is tight in flexion but well-balanced in extension. Which of the following maneuvers is most appropriate to balance the knee?
Explanation
Question 71
A 65-year-old patient presents with a painful total knee arthroplasty 8 weeks postoperatively. The ESR is 45 mm/hr and CRP is 35 mg/L. Knee aspiration yields 45,000 WBC/uL with 92% neutrophils. What is the most appropriate next step in management?
Explanation
Question 72
When performing a primary total hip arthroplasty via the direct anterior (Smith-Petersen) approach, the superficial internervous plane lies between muscles supplied by which of the following nerves?
Explanation
Question 73
Which of the following is traditionally considered an absolute contraindication for a medial unicompartmental knee arthroplasty (UKA)?
Explanation
Question 74
A patient with a total hip arthroplasty is experiencing recurrent posterior dislocations. Radiographs reveal appropriate cup abduction and anteversion, but the femoral component has inadequate offset. What is the most likely clinical finding on physical examination?
Explanation
Question 75
Mechanically assisted crevice corrosion (MACC), or trunnionosis, is most frequently associated with which of the following total hip arthroplasty component combinations?
Explanation
Question 76
During a revision total hip arthroplasty, severe acetabular bone loss is encountered. Radiographs and intraoperative findings demonstrate a complete separation of the superior and inferior halves of the hemipelvis. What is the diagnosis and best reconstruction option?
Explanation
Question 77
In total knee arthroplasty, the posterior stabilized (PS) design utilizes a cam and post mechanism. Which of the following normal knee kinematics does this mechanism primarily replicate?
Explanation
Question 78
Highly cross-linked polyethylene (HXLPE) was developed to reduce wear in total hip arthroplasty. What is the primary purpose of the post-irradiation remelting or annealing step in the manufacturing process?
Explanation
Question 79
A 60-year-old male undergoes a ceramic-on-ceramic total hip arthroplasty. Two years postoperatively, he complains of a loud audible squeaking during normal ambulation. What factor is most strongly associated with this complication?
Explanation
Question 80
A 48-year-old female presents with complete disruption of her extensor mechanism 3 months following a primary TKA. Examination shows a palpable gap at the patellar tendon and an inability to actively extend the knee. What is the most reliable surgical treatment?
Explanation
Question 81
An 80-year-old female with a well-functioning TKA falls and sustains a supracondylar femur fracture. Radiographs show a displaced fracture, but the femoral component remains radiographically well-fixed (Rorabeck Type II). What is the most appropriate management?
Explanation
Question 82
During preoperative templating for a primary THA, the surgeon identifies a significant leg length discrepancy, with the operative side being 2 cm shorter. To lengthen the leg without excessively increasing the femoral offset, which intraoperative adjustment should be made?
Explanation
Question 83
A surgeon is performing a posterior-stabilized total knee arthroplasty. During trialing, the knee is tight in flexion and symmetrically balanced in extension. Which of the following is the most appropriate next step?
Explanation
Question 84
A 74-year-old woman sustains a fall 6 years after primary total hip arthroplasty. Radiographs reveal a spiral fracture around the tip of the femoral stem. The stem is subsided by 2 cm, but the proximal femoral bone stock remains adequate. According to the Vancouver classification, what is the most appropriate management?
Explanation
Question 85
A 65-year-old man presents with anterior knee pain and recurrent lateral patellar subluxation 6 months after a primary total knee arthroplasty. Which of the following component malpositions is the most likely cause of his patellar maltracking?
Explanation
Question 86
A 58-year-old woman presents with worsening groin pain and swelling 8 years after receiving a metal-on-metal total hip arthroplasty. Laboratory tests show elevated serum cobalt and chromium levels. A MARS MRI demonstrates a large solid and cystic mass communicating with the joint. What is the underlying histologic mechanism of this process?
Explanation
Question 87
A 66-year-old man presents with new-onset groin pain 6 years after a primary total hip arthroplasty using a metal-on-polyethylene bearing. Serum metal ion testing reveals a cobalt level of 12 ppb and a chromium level of 1.5 ppb. Which of the following implant characteristics most increases the risk of this condition?
Explanation
Question 88
A 72-year-old man develops erythema, swelling, and purulent drainage from his incision 14 days after a primary total knee arthroplasty. He is febrile. Joint aspiration yields 65,000 WBCs/mcL with 95% neutrophils. What is the most appropriate surgical management?
Explanation
Question 89
A 70-year-old woman with a history of an L2-pelvis posterior spinal fusion is scheduled for a total hip arthroplasty. Spino-pelvic evaluation reveals a stiff spine with less than 10 degrees of pelvic tilt change from standing to sitting. How should the surgeon adjust the acetabular component positioning to minimize the risk of posterior dislocation?
Explanation
Question 90
During a revision total knee arthroplasty for aseptic loosening, removal of the tibial component reveals an uncontained metaphyseal bone defect measuring 4 cm deep, compromising the cortical rim (AORI Type 3). What is the most reliable method for achieving durable fixation?
Explanation
Question 91
A 45-year-old man undergoes total hip arthroplasty using a ceramic-on-ceramic bearing. Three years later, he complains of a reproducible squeaking noise during deep flexion. Which of the following biomechanical factors is most strongly associated with this phenomenon?
Explanation
Question 92
A patient presents with mid-flexion instability 1 year after a primary posterior-stabilized total knee arthroplasty. Review of operative notes and radiographs indicates the use of an oversized femoral component and a thick polyethylene insert. What technical error is the most likely cause of this mid-flexion instability?
Explanation
Question 93
During preoperative templating for a total hip arthroplasty, the surgeon plans to use a high-offset femoral stem. Compared to a standard-offset stem, what is the primary biomechanical advantage of increasing femoral offset?
Explanation
Question 94
A 78-year-old woman presents with an inability to actively extend her knee 3 years following a primary total knee arthroplasty. Examination confirms a palpable gap over the patellar tendon. What is the most reliable surgical reconstruction method for this chronic disruption?
Explanation
Question 95
A 65-year-old man experiences recurrent anterior dislocations of his total hip arthroplasty. Radiographs reveal the acetabular component is placed in 45 degrees of inclination and 40 degrees of anteversion. The femoral stem is in 25 degrees of anteversion. What is the most appropriate surgical intervention?
Explanation
Question 96
A 79-year-old woman presents to the emergency department after a fall. Radiographs demonstrate a displaced supracondylar femur fracture above a well-fixed total knee arthroplasty femoral component (Lewis-Rorabeck Type II). What is the preferred definitive treatment?
Explanation
Question 97
A 62-year-old man presents with a painful total knee arthroplasty 3 years postoperatively. Serum CRP and ESR are mildly elevated. Aspiration yields a synovial WBC count of 2,500 cells/mcL with 60% PMNs. Cultures are negative at 5 days. To definitively diagnose periprosthetic joint infection, which synovial fluid biomarker is the most specific next step?
Explanation
None
