AAOS & ABOS Hip MCQs (Set 3): Anatomy, Pathology & Trauma | OITE Board Prep

Key Takeaway
This high-yield question set (Set 3) for the AAOS and ABOS orthopedic board exams provides in-depth coverage of the hip joint. It features questions on hip anatomy, biomechanics, prevalent pathologies like osteoarthritis and FAI, alongside traumatic injuries such as fractures and dislocations. Ideal for OITE prep.
AAOS & ABOS Hip MCQs (Set 3): Anatomy, Pathology & Trauma | OITE Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
Question 2
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of
Explanation
Question 3
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of
Explanation
Question 4
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 um/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Explanation
Question 5
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5 degrees to 55 degrees of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
Question 6
The most compelling clinical reason to convert a hip arthrodesis to a total hip arthroplasty is that the latter
Explanation
Question 7
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Question 8
Femoral osteotomy for dysplasia of the hip will most likely result in
Explanation
Question 9
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of
Explanation
Question 10
Which of the following is considered a physiologic effect of anemia?
Explanation
Question 11
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Question 12
A 70-year-old woman reports anterior knee pain after undergoing an uncomplicated total knee arthroplasty 6 months ago. Examination reveals prepatellar tenderness, with no extensor lag. The radiographs shown in Figures 25a through 25c reveal a well-fixed patellar component. Management should consist of
Explanation
Question 13
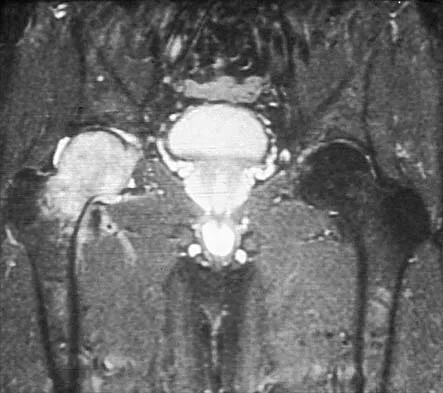
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
Explanation
Question 14
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
Question 15
What is the most likely late complication associated with cementless total knee replacement?
Explanation
Question 16
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
Question 17
Design factors that enhance the long-term survival of proximally coated cementless hip implants include both initial stability and
Explanation
Question 18
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Question 19
An obese patient undergoing total knee arthroplasty is at increased risk for which of the following complications?
Explanation
Question 20
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include
Explanation
Question 21
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Explanation
Question 22
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
Question 23
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Question 24
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
Question 25
The additional risk of complications in organ transplant patients receiving a total joint arthroplasty is attributed to
Explanation
Question 26
The medial femoral circumflex artery (MFCA) provides the primary blood supply to the femoral head. During a posterior approach to the hip, protecting this artery is critical. Which of the following anatomic landmarks best identifies the location of the deep branch of the MFCA?
Explanation
Question 27
A 25-year-old unrestrained driver is involved in a high-speed motor vehicle collision and presents with a posterior hip dislocation. Upon physical examination in the emergency department, what is the classic resting position of the affected lower extremity?
Explanation
Question 28
During an anterior ilioinguinal approach for an acetabular fracture, the surgeon must identify and ligate the corona mortis to prevent life-threatening hemorrhage. The corona mortis represents an anastomosis between which two vascular systems?
Explanation
Question 29
A healthy 32-year-old male sustains a displaced intracapsular femoral neck fracture after falling from a height.
What is the most appropriate definitive management for this patient?

Explanation
Question 30
The Smith-Petersen approach to the hip utilizes a true internervous plane. Which of the following accurately describes the muscular and neurologic intervals for the superficial dissection?
Explanation
Question 31
A 38-year-old female presents with persistent groin pain exacerbated by hip flexion. Radiographs demonstrate a crossover sign on the AP pelvis view. This radiographic finding is most strongly associated with which of the following pathologies?
Explanation
Question 32
A 40-year-old male with a history of corticosteroid use presents with bilateral hip pain.
Imaging confirms Ficat Stage II avascular necrosis of the femoral head with no evidence of subchondral collapse. Which of the following is the most appropriate initial surgical intervention?

Explanation
Question 33
In a highly comminuted subtrochanteric femur fracture, the proximal fragment typically assumes a predictable deformed position due to un-opposed muscular forces. What is the classic position of this proximal fragment?
Explanation
Question 34
During a total hip arthroplasty, the surgeon is inserting screws for supplemental acetabular shell fixation. According to the quadrant system described by Wasielewski, which quadrant represents the 'safe zone' to minimize risk of neurovascular injury?
Explanation
Question 35
Which of the following vessels is the primary contributor to the blood supply of the adult femoral head?
Explanation
Question 36
A patient with a posterior hip dislocation subsequently develops a sciatic nerve palsy. Which component of the sciatic nerve is most frequently and severely injured in this scenario, and what is the primary clinical manifestation?
Explanation
Question 37
When evaluating an intertrochanteric femur fracture for stability and implant choice, which of the following characteristics most strongly indicates the need for an intramedullary nail over a sliding hip screw?
Explanation
Question 38
A 28-year-old male presents with groin pain and decreased internal rotation of the hip. He has a history of a slipped capital femoral epiphysis (SCFE) treated with in situ pinning during adolescence. This patient is at highest risk for developing which of the following conditions?
Explanation
Question 39
On a Judet obturator oblique radiograph of the pelvis, the 'spur sign' is a pathognomonic finding for which specific type of acetabular fracture?
Explanation
Question 40
A 55-year-old female presents with chronic lateral hip pain that is refractory to conservative management. Physical examination reveals a positive Trendelenburg sign and weakness with resisted hip abduction. MRI is most likely to show pathology involving which structure?
Explanation
Question 41
During a direct anterior approach for total hip arthroplasty, the lateral femoral cutaneous nerve is at risk. To minimize injury, the surgeon should remember that the nerve typically courses:
Explanation
Question 42
A Pauwels type III femoral neck fracture is characterized by a high angle relative to the horizontal plane. Why do these fractures have a significantly higher rate of nonunion compared to Pauwels type I fractures?
Explanation
Question 43
When utilizing the ilioinguinal approach for an anterior acetabular fracture, three 'windows' are developed. The middle window provides access to the pelvic brim. What structures define the medial and lateral borders of this middle window?
Explanation
Question 44
A surgeon is performing a Kocher-Langenbeck approach for a posterior wall acetabular fracture. Which combination of intraoperative limb positioning is most effective for protecting the sciatic nerve from stretch injury during retraction?
Explanation
Question 45
A patient presents with a traumatic hip dislocation and is diagnosed with a Pipkin type IV fracture.
By definition, this injury includes a fracture of the femoral head combined with which of the following?

Explanation
Question 46
A 45-year-old male with a history of alcohol abuse presents with severe groin pain. AP pelvis and frog-leg lateral radiographs reveal a 'crescent sign' in the anterosuperior aspect of the femoral head. According to the Ficat classification, what does this sign represent?
Explanation
Question 47
During a posterior approach to the hip, protecting the medial circumflex femoral artery (MFCA) is critical. The main branch of the MFCA typically courses posterior to the obturator externus tendon and anterior to which of the following muscles?
Explanation
Question 48
A 65-year-old man presents with groin pain 15 years after an uncemented total hip arthroplasty.
Radiographs show extensive expansile radiolucencies around the acetabulum. Which of the following is the primary cell type responsible for initiating the bone resorption seen in this condition?
Explanation
Question 49
A 35-year-old man sustains a vertically oriented femoral neck fracture (Pauwels type III). Biomechanical studies suggest that which of the following fixation constructs provides the highest resistance to shear forces for this fracture pattern?
Explanation
Question 50
A surgeon is performing a direct lateral (Hardinge) approach to the hip. To avoid injury to the superior gluteal nerve, the proximal split in the gluteus medius should not extend beyond what distance from the tip of the greater trochanter?
Explanation
Question 51
A 28-year-old hockey player presents with chronic groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate an alpha angle of 70 degrees. This radiographic finding is most consistent with which of the following?
Explanation
Question 52
A 42-year-old woman with a history of systemic lupus erythematosus presents with progressive hip pain.
An MRI confirms early-stage avascular necrosis (Ficat Stage II) with no subchondral collapse. What is the most appropriate initial surgical intervention?
Explanation
Question 53
In a subtrochanteric femur fracture, the proximal fragment is typically deformed into flexion, abduction, and external rotation. Which muscle group is primarily responsible for the external rotation deformity?
Explanation
Question 54
A 55-year-old man who underwent a metal-on-metal total hip arthroplasty 8 years ago presents with new-onset groin pain and a palpable mass. Aspiration yields sterile, cloudy fluid. What is the most likely pathological mechanism?
Explanation
Question 55
A 30-year-old man is involved in a motor vehicle collision and sustains a pelvic injury.
Imaging reveals an acetabular fracture. The 'spur sign' on an obturator oblique plain radiograph is pathognomonic for which fracture pattern?

Explanation
Question 56
A patient is scheduled for surgical excision of heterotopic ossification (HO) following previous acetabular trauma. To prevent recurrence, postoperative prophylaxis is planned. Which of the following is the most standard prophylactic regimen?
Explanation
Question 57
A 25-year-old unrestrained driver sustains a dashboard injury during a collision. He presents with his right hip flexed, adducted, and internally rotated. Neurological examination reveals weak ankle dorsiflexion and decreased sensation over the dorsal foot. Which nerve division is most likely injured?
Explanation
Question 58
During an anterior intrapelvic (modified Stoppa) approach to the acetabulum, the surgeon must identify and ligate the 'corona mortis'. This structure represents an anastomosis between which two vascular systems?
Explanation
Question 59
A 40-year-old man with ankylosing spondylitis requires bilateral total hip arthroplasties for severe secondary osteoarthritis. Compared to osteoarthritis patients, this patient is at a significantly higher risk for which postoperative complication?
Explanation
Question 60
A 35-year-old man undergoes an open reduction and internal fixation for a displaced femoral neck fracture. To preserve the remaining blood supply to the femoral head, the surgeon must be mindful of the primary arterial supply. Which of the following vessels provides the primary blood supply to the adult femoral head?
Explanation
Question 61
A 28-year-old unrestrained driver is involved in a high-speed motor vehicle collision and sustains a posterior hip dislocation with an associated posterior wall acetabular fracture. Following reduction, the patient has a foot drop. Which of the following sensory deficits is most likely to be found on examination?
Explanation
Question 62
A surgeon utilizes the anterior (Smith-Petersen) approach for an open reduction of a developmental dysplasia of the hip. What is the superficial internervous plane utilized in this approach?
Explanation
Question 63
A 22-year-old male collegiate hockey player presents with chronic groin pain exacerbated by prolonged sitting and pivoting. Examination reveals pain with hip flexion, adduction, and internal rotation (FADIR). Radiographs demonstrate an alpha angle of 65 degrees. Which of the following is the most likely primary pathology?
Explanation
Question 64
A 65-year-old female presents with recurrent posterior instability of her total hip arthroplasty (THA). Radiographic evaluation reveals an anteversion angle of 5 degrees and an inclination angle of 40 degrees for the acetabular component. Which of the following is the most appropriate definitive management?
Explanation
Question 65
A 40-year-old woman with a history of systemic lupus erythematosus treated with corticosteroids presents with progressive hip pain. MRI reveals a double-line sign on T2-weighted images with no evidence of subchondral collapse or flattening of the femoral head. Which of the following joint-preserving interventions is most indicated?
Explanation
Question 66
When stabilizing an acute anteroposterior compression (APC) type pelvic ring injury in a hemodynamically unstable patient, a pelvic binder should be centered over which of the following anatomic landmarks?
Explanation
Question 67
A 78-year-old man sustains a reverse obliquity intertrochanteric femur fracture. Why is a cephalomedullary nail mechanically preferred over a sliding hip screw (SHS) for this fracture pattern?
Explanation
Question 68
During an ilioinguinal approach for an anterior column acetabular fracture, the surgeon must mobilize contents within three distinct surgical windows. Which of the following structures is primarily isolated and protected in the middle window?
Explanation
Question 69
When performing a direct lateral (Hardinge) approach to the hip, proximal extension of the incision into the gluteus medius must be strictly limited to avoid injury to which of the following nerves?
Explanation
Question 70
A 13-year-old obese boy undergoes in situ pinning with a single cannulated screw for a stable slipped capital femoral epiphysis (SCFE). Postoperatively, he develops severe, unrelenting hip stiffness and a dramatic loss of joint space on radiographs. Which of the following is the most likely cause of this complication?
Explanation
Question 71
A 60-year-old man presents with chronic lateral hip pain 5 years after a metal-on-polyethylene total hip arthroplasty. Serum inflammatory markers are normal, but a metal artifact reduction sequence (MARS) MRI reveals a large solid/cystic pseudotumor in the periprosthetic tissues. What is the most likely etiology of this finding?
Explanation
Question 72
During an intrapelvic (modified Stoppa) approach for acetabular fracture fixation, significant hemorrhage is encountered while dissecting over the superior pubic ramus. This bleeding is most likely originating from an anastomosis (corona mortis) between which two vascular systems?
Explanation
Question 73
A surgeon is counseling a young, active patient regarding bearing surface options for a planned total hip arthroplasty. If a ceramic-on-ceramic bearing is chosen, the patient should be counseled that compared to highly cross-linked polyethylene, ceramic-on-ceramic has a higher risk of which of the following?
Explanation
Question 74
Following a cementless total hip arthroplasty, a patient sustains a displaced periprosthetic femoral fracture localized around the tip of a well-fixed femoral stem (Vancouver Type B1). What is the gold standard of treatment for this specific injury?
Explanation
Question 75
A 28-year-old man sustains a displaced Pauwels type III femoral neck fracture. What is the most appropriate definitive management to minimize the risk of avascular necrosis and nonunion?
Explanation
Question 76
During a posterior approach to the hip, extreme external rotation of the femur places which of the following vascular structures at highest risk, potentially compromising the main blood supply to the adult femoral head?
Explanation
Question 77
A 65-year-old woman sustains a posterior hip dislocation 4 weeks after undergoing primary total hip arthroplasty via a posterior approach. Radiographs show the acetabular cup has 10 degrees of anteversion and 45 degrees of abduction. What is the most likely cause of this instability?
Explanation
Question 78
A 35-year-old man is brought to the emergency department after a high-speed motor vehicle collision. He has a shortened, internally rotated, and adducted right lower extremity. Following closed reduction of the hip, he is noted to have a foot drop and inability to extend his great toe. Which specific nerve division is most likely injured?
Explanation
Question 79
Which of the following radiographic findings is pathognomonic for a both-column acetabular fracture?
Explanation
Question 80
A 75-year-old woman presents with a reverse obliquity intertrochanteric femur fracture. Which of the following implants offers the most biomechanically stable fixation for this specific fracture pattern?
Explanation
Question 81
An obese 13-year-old boy presents with left knee pain and a slight limp for 3 weeks. Examination of the hip reveals obligatory external rotation of the thigh during passive flexion of the hip. What is the most appropriate initial management?
Explanation
Question 82
During an anterior (Smith-Petersen) approach to the hip, the superficial internervous plane lies between which two muscles?
Explanation
Question 83
A 45-year-old man undergoes total hip arthroplasty with an alumina ceramic-on-ceramic bearing. At his 3-year follow-up, he complains of a high-pitched squeaking noise when walking. Which of the following factors is most strongly associated with this phenomenon?
Explanation
Question 84
A 30-year-old woman with systemic lupus erythematosus on chronic corticosteroids presents with progressive groin pain. Radiographs show a subchondral lucent crescent in the anterosuperior aspect of the femoral head with mild flattening, but no joint space narrowing (Ficat Stage III). What is the most appropriate surgical treatment?
Explanation
Question 85
During an ilioinguinal approach to the acetabulum, severe bleeding occurs as the surgeon dissects near the superior pubic ramus. This is most likely due to an injury to an anastomotic vessel connecting the obturator system and the:
Explanation
Question 86
A 68-year-old man reports persistent lateral hip pain and a severe limp 6 months following a primary total hip arthroplasty via a direct lateral (Hardinge) approach. Examination reveals a positive Trendelenburg test. MRI with metal artifact reduction shows a complete, retracted tear of the abductor tendon insertion. What is the most appropriate next step after failing conservative care?
Explanation
Question 87
What is the biomechanical rationale for advising a patient with severe left hip osteoarthritis to hold a cane in their right hand?
Explanation
Question 88
A 55-year-old woman undergoes total hip arthroplasty. To achieve adequate soft tissue stability without over-lengthening the leg, the surgeon utilizes a high-offset femoral stem. Increasing femoral offset in total hip arthroplasty primarily achieves which of the following?
Explanation
Question 89
In evaluating a patient with persistent anterior thigh pain 1 year after receiving an uncemented total hip arthroplasty, radiographs reveal reactive cortical hypertrophy at the distal tip of the femoral stem. The porous-coated proximal region shows bone ingrowth without radiolucencies. What is the most likely diagnosis?
Explanation
Question 90
A 25-year-old male involved in a high-speed MVC sustains a type I Pipkin fracture-dislocation of the hip. Following closed reduction, a CT scan demonstrates a 1 cm displaced fracture fragment from the femoral head inferior to the fovea capitis, a concentrically reduced joint, and no intra-articular debris. What is the most appropriate management?
Explanation
Question 91
Which of the following vessels provides the primary blood supply to the weight-bearing portion of the adult femoral head?
Explanation
Question 92
A 32-year-old man sustains a displaced, vertical (Pauwels type III) femoral neck fracture. Which of the following fixation constructs offers the highest biomechanical stability against shear forces for this specific fracture pattern?
Explanation
Question 93
A 24-year-old male hockey player presents with groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a 'crossover sign' and prominent ischial spine.
These radiographic findings are most characteristic of which of the following conditions?

Explanation
Question 94
A 65-year-old woman undergoes a primary total hip arthroplasty via a direct lateral (Hardinge) approach. Postoperatively, she demonstrates a severe, persistent Trendelenburg gait. Iatrogenic injury to which of the following structures is the most likely cause?
Explanation
Question 95
A 28-year-old man presents following a high-speed motor vehicle collision with a posterior hip dislocation and an associated fracture of the femoral head.
A computed tomography (CT) scan reveals that the femoral head fracture fragment is located caudad (inferior) to the fovea centralis. According to the Pipkin classification, this injury is classified as:
Explanation
Question 96
During a posterior approach to the hip for a total hip arthroplasty, the surgeon releases the short external rotators. To minimize the risk of iatrogenic injury to the ascending branch of the medial femoral circumflex artery (MFCA), the surgeon should strictly protect the superior border of which of the following muscles?
Explanation
None
