Orthopedic Board Review: Set 249 - 100 MCQs on Pelvic Ring Injuries & More

Key Takeaway
This page offers Mock Exam Set 249, featuring 100 high-yield orthopedic surgery multiple-choice questions. Tailored for ABOS, OITE, and FRCS board review, these MCQs cover critical topics like pelvic ring injuries. It's designed to help orthopedic surgeons effectively master their upcoming exams.
Comprehensive Surgical Anatomy of the Bony Pe...
00:00
Start Quiz
The radiograph shown in Figure 27 shows measurement of what angle?

Explanation
The relationship between the distal articular surface of the first metatarsal head and the long axis of the first metatarsal is called the distal metatarsal articular angle. This angle has been validated by Richardson and associates to measure and determine the congruence of the first metatarsophalangeal joint. This angle is critical in determining the appropriate surgical procedure to perform on a patient with a bunion deformity because a congruent joint requires a procedure to maintain congruence of the articular surfaces following osteotomy. Therefore, a chevron becomes a biplanar chevron, and a Lapidus procedure adds a second osteotomy of the distal metatarsal to tilt the metatarsal head into a congruent location. Coughlin MJ: Juvenile hallux valgus: Etiology and treatment. Foot Ankle Int 1995;16:682-697. Steel MW III, Johnson KA, DeWitz MA, et al: Radiographic measurements of the normal foot. Foot Ankle 1980;1:151-158.
Question 3High Yield
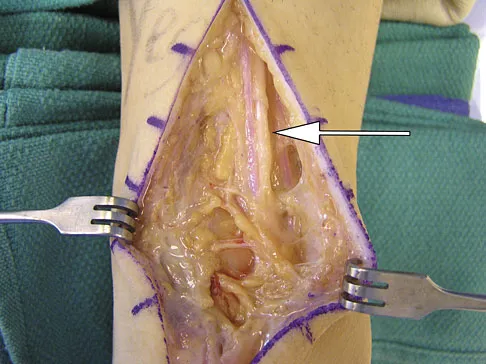
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
Explanation
The sural nerve runs with the small saphenous vein on the posterior leg just lateral to the Achilles tendon. It is formed by contributions from both the tibial and common peroneal nerves and provides sensation on the dorso-lateral aspect of the foot. Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Question 4High Yield
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of

Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 5High Yield
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35 degrees. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Explanation
Because the patient is skeletally mature with a curve of less than 40 degrees, there is no benefit to bracing and surgery is not indicated. Management should consist of observation and follow-up radiographs in 6 months. Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Question 6High Yield
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20 degrees of valgus at the knee. Knee range of motion shows 10 degrees to 90 degrees of flexion. Treatment should consist of
Explanation
Children with JRA frequently have valgus in association with hypervascularity because of chronic inflammation. This is normally caused by overgrowth of the medial femoral epiphysis. Staple hemiepiphyseodesis, if done early, can reverse the deformity. Osteotomy is usually unnecessary at this age, and there is a risk of stiffness of the knee following the procedure. Synovectomy may be helpful but will not prevent or correct a deformity.
Question 7High Yield
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of

Explanation
The patient has aseptic loosening of the original semiconstrained prosthesis and significant proximal ulnar bone destruction; therefore, the treatment of choice is revision arthroplasty using a semiconstrained design. Although orthotic stabilization could be used, it will not provide long-term pain relief. Resection arthroplasty after removal of the components may lead to painful instability. Elbow arthrodesis would be difficult with the bone stock loss and is not considered the best option. Two main contraindications to the use of an unconstrained prosthesis are significant bone loss and previous use of a hinged or semiconstrained prosthesis. An ulnar allograft could be combined with the use of a semiconstrained long-stemmed ulnar prosthesis as a treatment modification. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 8High Yield
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
The iliacus muscle is a frequent site of hemorrhage in patients with severe or moderate hemophilia. In patients with moderate hemophilia, hemorrhage into the iliacus muscle often follows play or sporting events that include forceful contraction of the hip flexor muscles. An expanding iliacus hematoma compresses the adjacent femoral nerve, with one study reporting 60% complete femoral nerve palsy in hemophiliacs with an iliacus or iliopsoas hemorrhage. Femoral nerve compression typically includes paresthesias in the distribution of the terminal saphenous nerve branch. Hip joint hemarthrosis may occur, but this condition is not as frequent in hemophiliacs as muscle hemorrhage into the iliacus muscle. More importantly, a hip joint hemarthrosis is not associated with significant compression of the femoral nerve. Avulsion fractures of the anterior superior iliac spine typically occur during adolescence and are not associated with saphenous nerve paresthesias. Slipped capital femoral epiphysis does not have an increased association with hemophilia and usually occurs during the adolescent years. Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 379-426.
Question 9High Yield
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?

Explanation
Osteonecrosis of the femoral head is the most devastating complication of SCFE. There is a 47% incidence of ischemic necrosis associated with an unstable SCFE. By definition, the patient with an unstable SCFE is unable to bear weight even with crutches. Osteonecrosis is most likely associated with the initial femoral head displacement rather than the result of either tamponade from hemarthrosis or from gentle repositioning prior to stabilization. Age, sex, and obesity are not risk factors for osteonecrosis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 10High Yield
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of

Explanation
Following a severe crush injury, the patient has an acute compartment syndrome. Even though there is an open fracture, this is not sufficient to decompress the compartment syndrome. Therefore, splinting and observation are not appropriate. The surgical treatment of choice is fasciotomy with fixation of the multiple fractures. A primary amputation is not indicated because there is potential for salvage of this devastating injury. Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228. Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Question 11High Yield
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of

Explanation
The most likely diagnosis is transient synovitis. Initial management should consist of bed rest and serial observation to rule out atypical septic arthritis of the hip. In an unreliable family situation, hospitalization for bed rest and observation may be indicated. Other disorders such as proximal femoral osteomyelitis, leukemia, juvenile rheumatoid arthritis, pelvic osteomyelitis, diskitis, and arthralgia secondary to other inflammatory disorders should be considered. However, these disorders are unlikely because of the paucity of abnormal clinical signs exhibited by the patient. On the other hand, transient synovitis of the hip in children is a diagnosis of exclusion; other possibilities should be explored if the patient's symptoms do not follow a typical course and resolve in 4 to 21 days.
Question 12High Yield
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d 32e Fibromatosis is a benign but aggressive fibrous lesion that principally arises from the connective tissue of muscle and the overlying fascia. The peak incidence is between the ages of 25 and 35 years. Most patients have a deep-seated, firm, poorly circumscribed mass that has grown insidiously and causes little or no pain. MRI is helpful in diagnosing the lesion and in assessing the extent of disease prior to surgical intervention. Histologically, the lesion is poorly circumscribed and infiltrates the surrounding tissue. The lesion appears bland with uniform spindle cells separated by abundant collagen, with little or no cell-to-cell contact. Despite its bland microscopic appearance, the tumor frequently behaves in an aggressive manner. These lesions do not metastasize but have a high incidence of recurrence. Treatment options consist of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
References:
- Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 13High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 14High Yield
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
The insertion of the pectoralis minor is on the base of the coracoid process. The coracoid helps define the interval between the subscapularis and supraspinatus muscles but neither attaches to it. The coracobrachialis and short head of biceps attach to the tip of the coracoid but are not listed as options. The long head of the biceps attaches to the supraglenoid tubercle. The serratus arises from the vertebral border of the scapula. Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Question 15High Yield
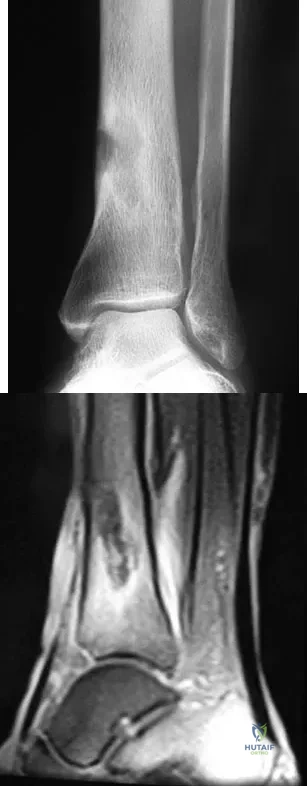
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
Explanation
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful. Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Question 16High Yield
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
Both the AAOS and AdvaMed, the medical device manufacturer's trade organization, have written guidelines that address potential conflicts of interest regarding interactions between physicians and manufacturer's representatives when it comes to patients' best interest. The AAOS feels that the orthopaedic profession exists for the primary purpose of caring for the patient and that the physician-patient relationship is the central focus of all ethical concerns. When an orthopaedic surgeon receives anything of significant value from industry, a potential conflict of interest exists. The AAOS believes that it is acceptable for industry to provide financial and other support to orthopaedic surgeons if such support has significant educational value and has the purpose of improving patient care. All dealings between orthopaedic surgeons and industry should benefit the patient and be able to withstand public scrutiny. A gift of any kind from industry should in no way influence the orthopaedic surgeon in determining the most appropriate treatment for his or her patient. Orthopaedic surgeons should not accept gifts or other financial support with conditions attached. Subsidies by industry to underwrite the costs of educational events where CME credits are provided can contribute to the improvement of patient care and are acceptable. A corporate subsidy received by the conference's sponsor is acceptable; however, direct industry reimbursement for an orthopaedic surgeon to attend a CME educational event is not appropriate. Special circumstances may arise in which orthopaedic surgeons may be required to learn new surgical techniques demonstrated by an expert or to review new implants or other devices on-site. In these circumstances, reimbursement for expenses may be appropriate. AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf The Orthopaedic Surgeon's Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. www.aaos.org/about/papers/ethics/1204eth.asp
Question 17High Yield
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?

Explanation
Cubitus varus is a common complication of displaced supracondylar humeral fractures that are treated with closed reduction and cast immobilization. Treatment with closed reduction and percutaneous pinning decreases the incidence of this complication. Cubitus varus also can occur in minimally displaced fractures when unrecognized collapse of the medial column of the distal humerus is not corrected with manipulation. This can be detected on physical examination of the carrying angle or on radiographs measuring Baumann's angle, both in comparison to the opposite side. Cubitus varus may result in unacceptable cosmesis and may predispose the patient to fractures of the lateral condyle. The lateral radiograph demonstrates the crescent sign from overlap of the distal humerus with the olecranon seen in patients with cubitus varus. Patients with growth arrest to the medial trochlear physis would have atrophy of the trochlea on radiographs. Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45. Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Question 18High Yield
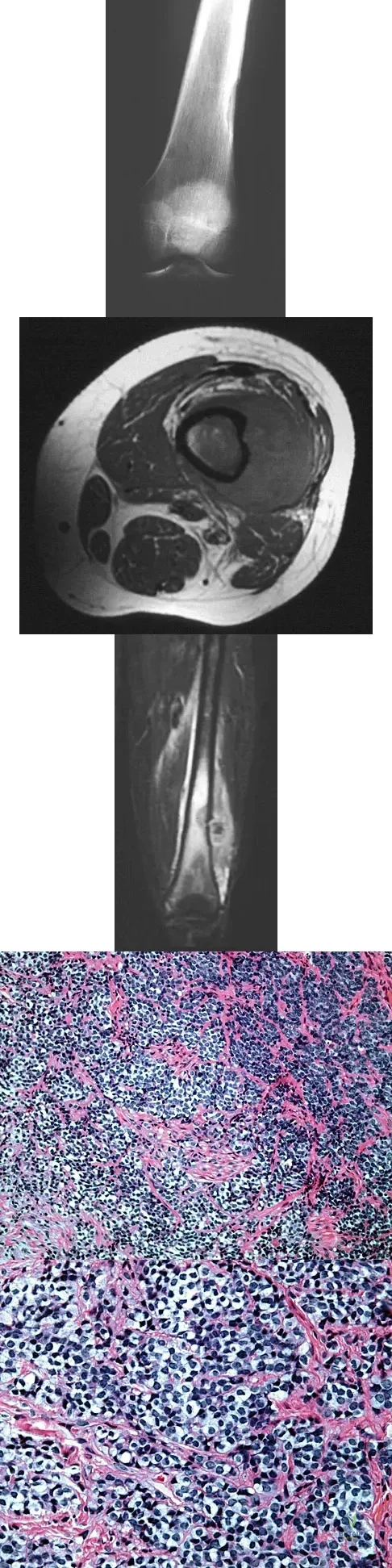
A 16-year-old boy has had left knee pain and swelling after sustaining a minor twisting injury while playing basketball 2 weeks ago. Figures 5a through 5e show the radiograph, MRI scans, and biopsy specimens. What is the most likely diagnosis?
Explanation
The imaging studies and histology are most consistent with Ewing's sarcoma. Tuberculosis can show small round blue cells on histology (lymphocytes associated with chronic infection) but would more typically involve the knee joint and periarticular bone. Osteosarcoma and MFH do not have small round blue cells histologically. Sissons HA, Murray RO, Kemp HBS: Orthopaedic Diagnosis. Berlin, Springer-Verlag, 1984, pp 254-256.
Question 19High Yield
Soft-tissue sarcomas most commonly metastasize to the
Explanation
Explanation
The most common location for soft-tissue tumors to metastasize is the lungs. Depending on the grade of the sarcoma, metastases develop in as many as 50% of patients with soft-tissue sarcomas. Tumor grade is considered the most significant prognostic factor in predicting risk of metastases, with high-grade lesions at greatest risk. Staging CT of the chest should be performed once the diagnosis of a soft-tissue sarcoma is suspected or confirmed. Regular surveillance of patients treated for soft-tissue sarcomas includes follow-up CT scans at regular intervals. Intra-abdominal metastases are uncommon but may occur, particularly in patients with myxoid liposarcoma. Regional metastases are relatively uncommon and occur in approximately 5% of all patients with soft-tissue sarcoma. The incidence of regional nodal metastases is higher for synovial sarcoma and epithelioid sarcomas than other soft-tissue sarcomas. Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
References:
- Enzinger FM, Weiss SW, Goldblum F: Soft Tissue Tumors, ed 4. Washington, DC, Mosby/AFIP, 2001.
Question 20High Yield
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
Complications of elbow arthroscopy are usually minor or temporary. However, serious complications include nerve injuries. The deep radial nerve is the closest to any of the portals, resting as close as 1 mm away from the scope inserted in the anterolateral portal. The capsule can be displaced anteriorly by distending the joint with about 25 mL of saline solution, thus moving the deep radial nerve approximately 1 cm anteriorly and decreasing the risk of injuring it while establishing the anterolateral portal. Keeping plastic cannulae in the portals may help to diminish fluid extravasation and swelling, which is more of an impediment than a serious complication. The image intensifier has no documented role in guiding loose body removal. While the proximal anteromedial portal is probably the safest anterior portal to establish, it is actually easier to remove a large loose body from this portal while viewing it from an anterolateral position. There is less tendon and muscle bulk to pass through at the site of the proximal anteromedial portal than at the anterolateral portal, making it less likely for the loose body to get stuck in the soft tissues. Techniques have been developed to permit removal of loose bodies as large as 2 cm in diameter without breaking them up into pieces. If it is possible to remove a large loose body intact, doing so greatly simplifies and shortens the procedure. Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 21High Yield
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter "A"?
Explanation
Explanation
The nerve labeled A is the axillary nerve, a branch from the posterior cord. The posterior cord innervates the subscapularis, latissimus dorsi, teres major and minor, deltoid, triceps, anconeus, brachioradialis, and extensors of the forearm. The axillary nerve innervates the teres minor and deltoid. The pectoralis minor is innervated by the medial cord. The supraspinatus and the subclavius are innervated by the superior trunk. The brachialis is innervated by the lateral cord. Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
References:
- Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 400, 405, 407, 450.
Question 22High Yield
What is the most common foot deformity associated with myelomeningocele?
Explanation
Explanation
All of the above can be associated with myelomeningocele, but talipes equinovarus occurs in 50% to 90% of patients with myelomeningocele. Congenital vertical talus is rarely associated with any neuromuscular diseases other than myelomeningocele but is not the most common deformity in myelomeningocele. Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
References:
- Lindseth RE: Myelomeningocele, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 622-628.
Question 23High Yield
What is the reported failure rate for surgical treatment of a Morton's neuroma?
Explanation
Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
References:
- Mann RA, Reynolds JC: Interdigital neuroma: A critical clinical analysis. Foot Ankle 1983;3:238-243.
Question 24High Yield
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
Explanation
Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
References:
- Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 25High Yield
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
Explanation
A discrete or focal callus is a response to excessive weight-bearing stress beneath the lateral (fibular) condyle of a lesser metatarsal head (most commonly second). The other structures generally have not been associated with a discrete callus. Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
References:
- Cracchiolo A: Surgical procedures of the lateral metatarsals, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1269-1283.
Question 26High Yield
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 27High Yield
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?

Explanation
The patient's symptoms are typical for gouty arthropathy, and the diagnosis can only be confirmed with aspiration and visualization of the crystals. A concomitant infection also must be ruled out; therefore, it is important to obtain a cell count and culture. Colchicine may have a role in gouty management, but the diagnosis must be confirmed. Allopurinol is not effective in acute gouty arthropathy. Measurement of serum uric acid levels is often not helpful in making a definitive diagnosis. Steroid injections should be deferred until cell count and culture results indicate no accompanying infection. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 28High Yield
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?

Explanation
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior. Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Question 29High Yield
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?
Explanation
Explanation
Kramer and associates conducted a retrospective review during an "epidemic" period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications. Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Question 30High Yield
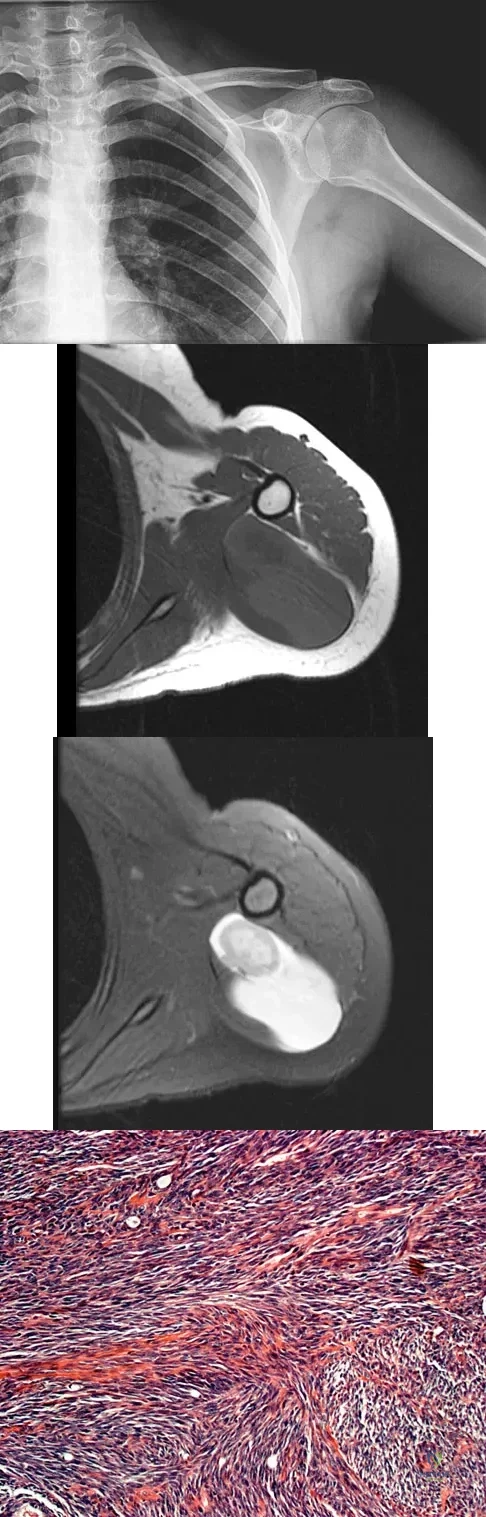
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?
Explanation
This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T2-weighted images and low signal on T1-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing's sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Question 31High Yield
Which of the following assessment tools most accurately reflects outcomes of well-being, daily function, and general health in a patient treated for cervical myelopathy?
Explanation
Explanation
The short-form 36 is an excellent tool for measuring the patient's perception of treatment outcome because it is a patient-generated, validated assessment of physical, social, and role function, emotional and mental health, energy/fatigue, pain, health perception, and health change. The Nurick criteria is an evaluation of physical function with gradations of ambulation and daily function. The Japanese Orthopaedic Association score gives points for function in activities of daily living but does not assess perception of general health. The neck disability index assesses the impact of neck pain on daily life, and the Odom criteria are the surgeon's evaluations of degree of radicular pain and deficit. Albert TJ, Mesa JJ, Eng K, McIntosh TC, Balderston RA: Health outcome assessment before and after lumbar laminectomy for radiculopathy. Spine 1996;21:960-963. Swiontkowski MF, Buckwalter JA, Keller RB, Haralson R: The outcomes movement in orthopaedic surgery: Where we are and where we should go. J Bone Joint Surgery Am 1999;81:732-740.
References:
- Ludwig SC, Albert TJ: Measuring outcomes in cervical myelopathy and radiculopathy. Instr Course Lect 1999;48:417-421.
Question 32High Yield
Where is the watershed zone for tarsal navicular vascularity?
Explanation
Explanation
The central one third has been established as the watershed zone by angiographic studies, and has been borne out in clinical conditions involving the navicular, such as stress fractures and osteonecrosis. These findings account for the susceptibility to injury at this level. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 239-242.
References:
- Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, pp 299-302.
Question 33High Yield
A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
Explanation
Explanation
30b 30c The patient has an atypical adult flatfoot deformity. The radiographs reveal forefoot abduction, mild loss of calcaneal pitch, and marked plantar flexion sag through the naviculocuneiform joint. The inability to perform a single limb heel rise indicates that the posterior tibial tendon is nonfunctional; however, the deformity remains flexible. In this patient, surgical treatment should include a tendon transfer, lateral column lengthening, medial column arthrodesis, and heel cord lengthening. Because a substantial portion of the deformity stems from the naviculocuneiform joint in this instance, tendon transfer and lateral column lengthening alone provide insufficient deformity correction. Triple arthrodesis and heel cord lengthening is best reserved for fixed flatfoot deformities. Soft-tissue procedures alone are associated with a high failure rate, as are attempted tendon repairs. Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.
Question 34High Yield
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
There is no evidence of increased polyethylene wear in constrained acetabular components. The rates of wear appear to be the same using standard or constrained liners. Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238. Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Question 35High Yield
Which of the following clinical disorders is the result of a mutation in fibroblast growth factor recepter 3 (FGFR3)?
Explanation
Explanation
Camptomelic dysplasia is caused by a heterozygous loss of function of the Sox9 gene. The alternatives have genetic causes, but are not linked to Sox9. Cleidocranial dysplasia is related to a defect in Cbfa-1 (Osf-2, Runx2). Schmid metaphyseal chondrodysplasia is related to Type X collagen. Fibrous dysplasia is related to a defect in the alpha subunit of stimulatory guanine-nucleotide-binding protein (Gs). Achondroplasia is related to a defect in fibroblast growth factor receptor 3. Wagner T, Wirth J, Meyer J, et al: Autosomal sex reversal and camptomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell 1994;79:1111-1120. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
References:
- Dietz FR, Murray JC: Update on the genetic bases of disorders with orthopaedic manifestations, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 36High Yield
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of

Explanation
An exercise program to strengthen the deltoid and remaining rotator cuff will most likely offer the best results. Revision rotator cuff surgery yields better results in decreasing pain than improving strength and function, and this patient has only minimal pain. Tendon transfers, involving the use of the latissimus dorsi or teres major, have been used when the rotator cuff is deemed irreparable but are not indicated in elderly patients with minimal symptoms. Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515. DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Question 37High Yield
A 50-year-old laborer sustained an isolated closed injury to his heel after falling 11 feet off a wall. A radiograph and a CT scan are shown in Figures 4a and 4b. To minimize the patient's temporary disability and allow him to return to work most rapidly, management should consist of

Explanation
With a severe articular injury to the calcaneus, the ability to achieve satisfactory results with open reduction and internal fixation diminishes. An arthrodesis is often needed to allow a person who works as a laborer to return to work. Recent literature suggests that this can be successfully performed primarily, improving the odds of an earlier return to the labor force at 1 year. Huefner T, Thermann H, Geerling J, Pape HC, Pohlemann T: Primary subtalar arthrodesis of calcaneal fractures. Foot Ankle Int 2001;22:9-14. Coughlin MJ: Calcaneal fractures in the industrial patient. Foot Ankle Int 2000;21:896-905.
Question 38High Yield
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?
Explanation
Explanation
23b 23c 23d 23e The radiographs reveal a lytic subchondral lesion that has a poorly defined margin and lacks mineralization. The bone scan confirms an active lesion that has central photopenia, producing the characteristic doughnut configuration. The MRI scans confirm the presence of a subchondral lesion that is modestly expansile at the lateral plateau and has low signal intensity on the T1-weighted image and a mixed high signal on the T2-weighted image. These features strongly suggest giant cell tumor of bone, more than 50% of which appear around the knee. Simple cyst is excluded by the MRI characteristics. Fibrous dysplasia is unlikely to be in a subchondral location and typically does not show this intensity of uptake on bone scan. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
References:
- Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3939-3962.
Question 39High Yield
A 19-year-old man who sustained a spinal cord injury in a motor vehicle accident 3 days ago has 5/5 full strength in the deltoids and biceps bilaterally, 4/5 strength in wrist extension bilaterally, 1/5 triceps function on the right side, and 2/5 triceps function on the left side. The patient has no detectable lower extremity motor function. Based on the American Spinal Injury Association's classification, what is the patient's functional level?
Explanation
Explanation
By convention when determining the motor level, the key muscle must be at least 3/5. The next most rostral level must be 4/5. Therefore, this patient's functional level is C6.
References:
- International Standards for Neurological and Functional Classification of Spinal Cord Injury. Chicago, IL, American Spinal Injury Association Publication, 1996.
Question 40High Yield
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
The patient has a posterolateral rotatory instability (PLRI) of the elbow that is most likely the result of iatrogenic injury to the lateral ulnar collateral ligament, the main ligament implicated in PLRI. The anterior band of the medial collateral ligament is implicated in valgus instability. Injury to the radial nerve is unlikely, and the lateral radial collateral ligament makes less of a contribution to elbow stability than does the ulnar component. While the origin of the extensor carpi radialis brevis may contribute to elbow stability, it is not as important a stabilizer as the lateral ulnohumeral ligament. O'Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
Question 41High Yield
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
Explanation
Ford and associates studied 81 high school basketball players and found that females landed with greater total valgus knee loading and a greater maximum valgus knee angle than male athletes. Hewett and associates reported in a study of 205 female athletes that those with increased dynamic valgus and high abduction loads were at increased risk of anterior cruciate ligament injury. Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
References:
- Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 42High Yield
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?

Explanation
The patient has symptomatic primary osteoarthritis of the elbow with multiple loose bodies. Given his age and occupation, an elbow arthroplasty is not an option. Arthroscopic debridement and removal of loose bodies has been shown to be effective for osteoarthritis of the elbow. Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Question 43High Yield
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?

Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 44High Yield
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of

Explanation
The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 45High Yield
What is the most common foot and ankle deformity in patients with arthrogryposis?
Explanation
Explanation
Clubfoot (talipes equinovarus) in patients with arthrogryposis is a rigid and resistant deformity. However, multiple studies document limited success with nonsurgical management. Manipulation and casting are generally a preliminary treatment before surgery; successful correction will most like require a talectomy. Guidera KJ, Drennan JC: Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop 1985;194:93-98. Handelsman JE, Badalamente MA: Neuromuscular studies in clubfoot. J Pediatr Orthop 1981;1:23-32.
References:
- Dias LS, Stern LS: Talectomy in the treatment of resistant talipes equinovarus deformity in myelomeningocele and arthrogryposis. J Pediatr Orthop 1987;7:39-41.
Question 46High Yield
A 68-year-old woman stepped on a needle while walking barefoot 10 days ago. She is not certain but thinks it is imbedded in her foot, and she notes local tenderness at the puncture site and drainage. Her primary care physician has been treating her with oral antibiotics. A plain radiograph is shown in Figure 38. What is the best course of action?

Explanation
Based on the radiographic findings, the patient has a metallic foreign body in her foot that is consistent with a needle. She has local infection secondary to the continued presence of the foreign body. CT is not necessary to localize the foreign body as it is adequately visualized on the plain radiographs. The infection cannot be adequately treated until the foreign body is removed. Attempted removal of foreign bodies without proper anesthesia and fluoroscopy frequently results in frustration because of the inability to localize the foreign body. Removal in a surgical suite with proper anesthesia and fluoroscopy is the preferred option. Once the foreign body is removed, the local infection will resolve rapidly. Combs AH, Kernek CB, Heck DA: Orthopedic grand rounds: Retained wooden foreign body in the foot detected by computed tomography. Orthopedics 1986;9:1434-1435.
Question 47High Yield
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation. Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Question 48High Yield
Which of the following agents have been shown to reduce the incidence of skeletal events in patients with multiple myeloma?
Explanation
Bisphosphonates are a class of drugs that act to inhibit osteoclast resorption of bone. It has been shown that patients with multiple myeloma who are treated with bisphosphonates have fewer pathologic fractures than patients who are not treated with bisphosphonates. Vitamin D and calcium are considered appropriate for patients who are at risk for the development of osteoporosis, as is estrogen in selected women. Chelating agents and progesterones have no use in the treatment of patients with multiple myeloma or osteoporosis. Berenson JR: Bisphosphonates in multiple myeloma. Cancer 1997;15:1661-1667.
Question 49High Yield
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of

Explanation
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Question 50High Yield
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
Explanation
Explanation
23b The radiographs show the osteophytic build-up of the posteromedial corner of the elbow that occurs with valgus extension overload in the pitching elbow. This is the result of excessive valgus forces during the acceleration and deceleration phases of throwing. These forces, coupled with medial elbow stresses, cause a wedging of the olecranon into the medial wall of the olecranon fossa. Valgus instability of the elbow may further stimulate osteophyte formation. Repetitive impact of a spur within the olecranon fossa may cause fragmentation and eventual formation of loose bodies. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99. Field LD, Savoie FJ: Common elbow injuries in sport. Sports Med 1988;26:193-205.
References:
- Wilson FD, Andrews JR, Blackburn TA, et al: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 51High Yield
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 52High Yield
A Canale view best visualizes which of the following structures?

Explanation
The Canale view, which visualizes the talar neck, is taken with the ankle in maximum plantar flexion and the foot pronated 15 degrees. The radiograph is directed at a 75 degree angle from the horizontal plane in the anteroposterior plane. The Broden view, which is different from the Canale view, is best for imaging the posterior facet of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Question 53High Yield
A 16-year-old boy has a symptomatic flatfoot deformity that is causing pain, skin breakdown, and shoe wear problems. Shoe modification and an orthosis have failed to provide relief. Examination reveals hindfoot valgus, talonavicular sag, and forefoot abduction that are all passively correctable. Treatment should consist of
Explanation
Explanation
The patient has a supple planovalgus deformity that is passively fully correctable, and nonsurgical management has failed to provide relief. Lateral column lengthening with medial soft-tissue tightening will correct the deformity and maintain a flexible foot. Arthrodesis is not recommended for a supple, correctable deformity because of loss of motion and long-term degeneration of surrounding joints. Medial displacement calcaneal osteotomy is generally reserved for an adult-acquired flexible flatfoot. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631. Evans D: Calcaneo-valgus deformity. J Bone Joint Surg Br 1975;57:270-278.
References:
- Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot: Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995;77:500-512.
Question 54High Yield
Which of the following diagnostic studies best distinguishes Ewing's sarcoma from small cell osteosarcoma?
Explanation
Explanation
Cytogenetics best demonstrates the 11;22 translocation characteristic of Ewing's sarcoma. The translocation also can be detected with polymerase chain reaction and fluorescent in situ hybridization. The Ewing antibody is used for immunostaining to check for cell membrane (surface) staining of a marker unrelated to the translocation; this could also help distinguish Ewing's sarcoma from small cell osteosarcoma. A bone scan will show increased uptake with both types of tumors. Although most Ewing's sarcoma tumors are diploid, some are polyploid as are most osteosarcomas. Flow cytometry is used to sort cells, sometimes based on antibody binding. LDH can be elevated in both Ewing's sarcoma and osteosarcoma and is a poor prognostic indicator when elevated. Lymph node metastases are uncommon in both of these tumors. Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498. Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing's sarcoma family. Eur J Cancer 2003;39:19-30.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 55High Yield
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?
Explanation
Explanation
Increasing articular conformity increases the surface area for contact between the polyethylene and the femoral component. Advantages of this include lower peak contact stress within the polyethylene and less risk of polyethylene fatigue failure. Patellofemoral tracking is unchanged by increasing conformity unless gross component apposition is present. A potential disadvantage of increasing conformity includes some restriction in tibial rollback. Modest changes in conformity have not been shown to alter the rate of mechanical loosening. If conformity was increased to the extent of significant constraint, a potential increased risk of loosening would be expected, not a decrease. Design of modern TKAs includes a compromise in achieving enough constraint to lower polyethylene stress, without providing so much constraint as to limit kinematics and stress the fixation interfaces. D'Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 56High Yield
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
Explanation
21b 21c 21d 21e The projection of the sacroiliac joint on the outer surface of the ilium should be well understood to avoid violation of the joint during bone graft harvesting and to help in insertion of the screw across the joint. The sacroiliac joint has superior and inferior limbs. The average lengths of the superior and inferior limbs are 4.4 cm and 5.6 cm, respectively. The average width of each limb is 2.0 cm. The average distance from the longitudinal axis of the superior limb to the posterior superior iliac spine is 5.5 cm. The average longitudinal axis of the inferior limb is 1.2 cm superior to the inferior margin of the posterior inferior iliac spine. The average angle between the two axes is 93 degrees. Figure 21c most closely shows the projection of the sacroiliac joint on the outer table of the ilium. Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
References:
- Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 57High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 58High Yield
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer's representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture's representative suggests a partnership in a boat costing $200,000. The manufacture's representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
Explanation
Rejecting this proposal is the only appropriate course of action. Accepting it would, in essence, be receiving a huge gift from industry in the form of a sailboat. Physicians frequently assert that they are not influenced by gifts and relationships with industry representatives, but evidence is to the contrary. Such an arrangement constitutes a tremendous incentive to use the manufacturer's products. The fact that the boat partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest. AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6-8. www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf Opinions on Ethics and Professionalism: The Orthopaedic Surgeon's Relationship with Industry (Document 1204), in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 36-40. www.aaos.org/about/papers/ethics/1204eth.asp AdvaMed Code of Ethics on Interactions with Health Care Professionals, Advanced Medical Technology Association, Washington, DC. www.AdvaMed.org
Question 59High Yield
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?

Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 60High Yield
Which of the following antibiotics is contraindicated in children?
Explanation
The tetracycline family of medications can stain teeth and bone in skeletally immature patients and as a result should be avoided in those patients. The remaining antibiotics have no known specific contraindication to use in children.
Question 61High Yield
A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of
Explanation
Explanation
Most subtalar dislocations can be easily reduced by closed methods. If no fractures or defects are seen on the postreduction radiographs, then the success rate with cast immobilization is good. Medial dislocations have a better prognosis than lateral dislocations. Late instability is rare; therefore, the duration of immobilization should not be excessive. Most subtalar dislocations result in some stiffening of the hindfoot, and painful degenerative arthrosis is the most common serious complication.
References:
- Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 62High Yield
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?

Explanation
Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined. Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Question 63High Yield
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to increase the risk of pseudarthrosis. In a controlled rabbit study, nonunions were reported with the use of toradol and indomethacin. NSAIDs are commonly used medications with the potential to diminish osteogenesis. Studies clearly have demonstrated inhibition of spinal fusion following the postoperative administration of several NSAIDs, including ibuprofen. Cigarette smoking is another potent inhibitor of spinal fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 64High Yield
A 32-year-old woman with systemic lupus erythematosus treated with methotrexate and oral corticosteroids reports right groin pain with ambulation and night pain. Examination reveals pain with internal and external rotation and flexion that is limited to 105 degrees because of discomfort. Laboratory studies show a serum WBC of 9.0/mm3 and an erythrocyte sedimentation rate of 35 mm/h. Figures 5a and 5b show AP and lateral radiographs of the right hip. Further evaluation should include

Explanation
The radiographs show Ficat and Arlet stage 2 osteonecrosis. The femoral head remains round, and there are sclerotic changes in the superolateral quadrant. Patients with systemic lupus erythematosus are at risk for osteonecrosis because of prednisone use and the underlying metabolic changes associated with the condition (hypofibrinolysis and thrombophilia). MRI is the best diagnostic method for detecting osteonecrosis, with a greater than 98% sensitivity and specificity. For this patient, an MRI can assess the contralateral hip for any involvement and can quantify the extent of the lesion. Mont MA, Jones LC, Sotereanos DG, Amstutz HC, Hungerford DS: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 65High Yield
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
Explanation
The paravertebral musculature, the intervertebral disks, and the normal lordotic curvature of the cervical spine can absorb much of the imparted energy of collision. However, when the neck is flexed approximately 30 degrees, the normal lordotic curvature is flattened and the forces applied to the vertex of the head are directed at a straight segmented column. In this situation, the cervical spine is less able to absorb the applied force. With mounting axial load, compressive deformation occurs within the intervertebral disks, causing angular deformation and buckling. The spine will fail in flexion, with resultant fracture, subluxation, or dislocation. A rotatory component added to axial compression can cause concomitant extension, rotation, and shear injury patterns. The National Football Head and Neck Injury Registry has made two recommendations to the NCAA Football Rules Committee to minimize the risk of such injuries: (1) No player should intentionally strike an opponent with the crown or top of the helmet; and (2) No player should deliberately use his helmet to butt or ram an opponent. Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
- Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978.
- JAMA 1979;241:1477-1479.
Question 66High Yield
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 67High Yield
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?

Explanation
Tooth avulsions can occur in contact or collision sports. An avulsed tooth is a medical emergency. The likelihood of survival of the tooth depends on the length of time that the tooth is out of the socket and the degree to which the periodontal ligament is damaged. The tooth should be handled only by the crown end and not the root end. It can be rinsed of debris with water or normal saline solution. The tooth should not be brushed or cleaned otherwise. During transport, the tooth must be kept moist. An avulsed tooth can be transported in whole milk, saliva, sterile saline solution, or commercially available kits with physiologic buffer solutions. The tooth and the athlete should be transported to the dentist for reinsertion as soon as possible and preferably within an hour. Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135. Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Question 68High Yield
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was
Explanation
Explanation
25b 25c The radiographs show L5 spondylolysis without spondylolisthesis (slip). The bone scan is normal, indicating that the pars interarticularis fractures are not acute. The incidence of spondylolysis is approximately 5% in the general population. The lesion generally develops in children age 5 to 6 years, and there is a second peak in the adolescent population. There is a familial predisposition, with reported rates of 27% to 69% in close relatives. A recent long-term follow-up study found that 90% of the spondylolisthesis had occurred before the patient's first visit to the physician. Spondylolisthesis tends to progress during the initial growth spurt and is similar in some respects to idiopathic scoliosis. Progression of a lytic spondylolysis to spondylolisthesis in adulthood has been reported; however, this is exceedingly rare. Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208. Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Am 1989;71:1098-1107. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
References:
- Fredrickson BE, Baker D, McHolik WJ, Yuan HA, Lubicky JP: The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 1984;66:699-707.
Question 69High Yield
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c The radiographs show a posterior glenoid osteophyte, often termed a "thrower's exostosis." These exostoses are best visualized on the Stryker notch view and may be missed on other more standard radiographic views of the shoulder. CT and MRI scans may be used, but usually add little information to the radiographic findings. Arthroscopic examination of patients with this condition commonly reveals undersurface tearing of the rotator cuff and posterior labrum. Treatment of this condition remains somewhat controversial, with avocation of both nonsurgical and surgical techniques. Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower's exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136. Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
References:
- Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 70High Yield
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a "primed" immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered. Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Question 71High Yield
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?

Explanation
The child has Kohler's disease. This is a self-limiting osteochondritis of the navicular. It is treated symptomatically with initial cast immobilization for 6 to 12 weeks, followed possibly by orthotic management. Findings shown in the radiograph usually will normalize within 1 year, and there are no long-term sequelae. Borges JL, Guille JT, Bowen JR: Kohler's bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Question 72High Yield
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
Explanation
Explanation
The cervical spine may be involved in a child with polyarticular or systemic JRA; fusion or instability can occur. Radiographic assessment of the cervical spine should include lateral flexion-extension views. The potential exists for spinal cord injury during intubation or positioning in the presence of an unstable cervical spine. Limitations of the TMJ and micrognathia may affect ease of intubation and administration of anesthesia via a mask. If the TMJ and jaw are involved, some patients may have dental findings such as dental caries and even abscesses which can affect surgery. Some children, particularly those with systemic arthritis, may be taking corticosteroids long-term and may need stress dosing with complex surgeries. Although it is important to routinely check for uveitis and iritis in children with JRA, this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA. Cassity JT, Petty RE (eds): Textbook of Pediatric Rheumatology, ed 5. Philadelphia, PA, WB Saunders, 2005. Ilowite N: Current treatment of juvenile rheumatoid arthritis. Pediatrics 2002;109:109-115. Ruddy S, Harris ED, Sledge CB (eds): Kelley's Textbook of Rheumatology, ed 6. Philadelphia, PA, WB Saunders, 2001.
References:
- Hamalainen M: Surgical treatment of juvenile rheumatoid arthritis. Clin Exp Rheumatol 1994;12:S107-S112.
Question 73High Yield
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?

Explanation
Any patient who is severely symptomatic this quickly after surgery must be evaluated for infection. Loosening is also a possible cause, but infection must be ruled-out. Bone scans are not helpful at this early postoperative stage. Normal laboratory values argue strongly against infection, but when abnormal, need to be supplemented with a hip aspiration. Aspiration remains the most selective and sensitive measure, especially when linked to a WBC count of the synovial tissues in the joint. There is no indication for an antiobiotic trial because it may make future culture sensitivity more difficult. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Question 74High Yield
During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
Explanation
Explanation
The surgeon perforated the anterior longitudinal ligament and injured the common iliac artery. Bingol and associates described injuries to the vascular structures during lumbar disk surgery. The common iliac artery was most commonly affected and constituted 76.9% of injuries.
Question 75High Yield
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
Numerous surgical approaches have been used for thoracic diskectomy, including the most recent VATS. One of the first approaches described, posterior laminectomy, involves manipulation of the spinal cord, which the other approaches avoid. The posterior approach had dismal results, including further neurologic deterioration and even paralysis. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864. Benjamin V: Diagnosis and management of thoracic disc disease. Clin Neurosurg 1983;30:577-605. Russell T: Thoracic intervertebral disc protrusion: Experience of 67 cases and review of the literature. Br J Neurosurg 1989;3:153-160.
Question 76High Yield
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression. Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Question 77High Yield
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
The vascularity of the dorsal portion of the digital flexor tendons is considerably richer than the volar portion. The other regions are not preferentially more vascular. Hunter JM, Scheider LH, Makin EJ (eds): Tendon Surgery in the Hand. St Louis, MO, Mosby, 1987, pp 91-99.
Question 78High Yield
Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
Explanation
Complications of medial sesamoidectomy include stiffness, claw toe, and hallux valgus. Each sesamoid sits within its respective head of the flexor hallucis brevis tendon. Excision of one sesamoid can result in slack in its flexor hallucis brevis tendon; therefore, it is imperative to preserve or repair the flexor hallucis brevis tendon when removing the medial sesamoid. Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.
Question 79High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of

Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting. Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Question 80High Yield
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play?
Explanation
Explanation
Infectious mononucleosis commonly affects adolescents and young adults. It is a febrile illness accompanied by acute pharyngitis. Splenomegaly may occur and predispose the athlete to splenic rupture. Splenic rupture has been reported in nonathletes as well as in patients with normal-sized spleens. Clinical evidence supports a return to all sports 4 weeks after the onset of symptoms provided that the spleen has returned to normal size. Auwaerter PG: Infectious mononucleosis: Return to play. Clin Sports Med 2004;23:485-497.
References:
- Kinderknecht JJ: Infectious mononucleosis and the spleen. Curr Sports Med Rep 2002;1:116-120.
Question 81High Yield
A patient who has recalcitrant medial plantar heel pain and pain directly over the medial side of the heel undergoes open release of the plantar fascia. After releasing a portion of the plantar fascia, the deep fascia of the abductor hallucis muscle is released to relieve pressure on which of the following structures?
Explanation
Explanation
The deep fascia of the abductor hallucis muscle is released to relieve pressure on the first branch of the lateral plantar nerve. The tibial nerve lies more proximal to this area. The medial plantar nerve has already passed dorsally and medially, while the sural nerve lies on the lateral side of the foot. The flexor hallucis brevis muscle lies deep to the plantar fascia, not the abductor fascia. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
References:
- Davies MS, Weiss GA, Saxby TS: Plantar fasciitis: How successful is surgical intervention? Foot Ankle Int 1999;20:803-807.
Question 82High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 83High Yield
The primary function of structure "A" in Figure 29 is to limit
Explanation
Explanation
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur. Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
References:
- Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 84High Yield
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5 degrees to 55 degrees of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
Esler and associates evaluated the use of manipulation under anesthesia in 47 knees. Manipulation was considered when intensive physical therapy failed to increase flexion to more than 80 degrees. The mean time from arthroplasty to manipulation was 11.3 weeks, and the mean active flexion before manipulation was 62 degrees. One year later, the mean gain was 33 degrees. Definite sustained gains in flexion were achieved even when manipulation was performed 4 or more months after arthroplasty. An additional 21 patients who met the criteria for manipulation declined the procedure, and despite continued physical therapy, they showed no significant increase in knee flexion.
Question 85High Yield
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
Explanation
The bright signal on the T2-weighted MRI scan suggests fluid. The multiloculated appearance in proximity to the proximal tibiofibular joint suggests that the most likely diagnosis is a ganglion. They typically increase and decrease in size and can be diagnosed by the classic gelatinous fluid obtained through needle aspiration. Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
References:
- Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 86High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 87High Yield
A 78-year-old woman has had activity-limiting cervical pain and occipital headaches for the past 4 years. Management consisting of injections, analgesics, and part-time collar wear has provided temporary relief. Examination reveals that her neck pain seems to be primarily located immediately below the skull and is aggravated by long periods of sitting and rotation of her head. Plain radiographs are shown in Figures 36a through 36c. What is the best course of action?
Explanation
Explanation
36b 36c Posterior atlantoaxial arthrodesis predictably relieves pain associated with arthrosis of the atlantoaxial joints. Typically, these patients have pain at the base of the occiput and in the most cephalad portion of the posterior aspect of the neck. Associated headache is common and often severe. Pain is aggravated by rotation but usually not by flexion and extension. Diagnostic blocks of the C1-C2 joint and the greater occipital nerve may be helpful to confirm the diagnosis preoperatively. Ghanayem AJ, Leventhal M, Bohlman HH: Osteoarthrosis of the atlanto-axial joints: Long-term follow-up after treatment with arthrodesis. J Bone Joint Surg Am 1996;78:1300-1307.
References:
- Star MJ, Curd JG, Thorne RP: Atlantoaxial lateral mass osteoarthritis: A frequently overlooked cause of severe occipitocervical pain. Spine 1992;17:S71-S76.
Question 88High Yield
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
Explanation
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303. Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
References:
- Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 89High Yield
The insurance carrier of a patient who underwent total knee arthroplasty 4 days ago is now demanding that the patient be discharged from the hospital. However, examination reveals that the patient has a range of motion of only 10 degrees to 55 degrees, and the patient is concerned whether she will ever move her knee normally. The insurance company representative should be advised that
Explanation
Explanation
Examination findings that show flexion of only 55 degrees at discharge should alert the surgeon that the patient will require close scrutiny and follow-up. Mauerhan and associates examined the records of 745 patients who had a primary total knee arthroplasty from 1993 to 1996. At their institution, development and implementation of clinical pathways resulted in a significant decrease in the average length of stay, beginning in 1993 with 6.4 days +/- 1.8 days and progressively decreasing to 4.4 days +/- 1.0 days in 1996. The rate of manipulation (patients manipulated at 6 weeks/total number of patients receiving total knee arthroplasty) was 6.0% in 1993, 11.3% in 1994, 13.5% in 1995, and 12.0% in 1996. In the period of 1993 to 1996, patients requiring manipulation consistently had a lower range of motion of 69.0 degrees +/- 10 degrees at the time of discharge compared with patients not requiring manipulation who had a range of motion of 80.7 degrees +/- 10.6 degrees. In this era of outpatient services, however, another solution would be to arrange for outpatient physical therapy on a more frequent basis and to see the patient more frequently in the office until an acceptable range of motion is established.
References:
- Mauerhan DR, Mokris JG, Ly A, Kiebzak GM: Relationship between length of stay and manipulation rate after total knee arthroplasty. J Arthroplasty 1998;13:896-900.
Question 90High Yield
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of
Explanation
Explanation
Proximal humeral fractures in children are classified as metaphyseal or Salter-Harris type I or II fractures, and most of these fractures are treated with closed methods. Eighty percent of the growth of the humerus comes from the proximal physis; therefore, tremendous remodeling potential is present. Indications for open reduction include open fractures or severely displaced fractures in adolescents with minimal growth remaining. Acceptable limits of reduction in adolescent proximal humeral fractures include bayonet apposition and angulation of less than 35 degrees. Common blocks to reduction in adolescents include the biceps tendon and periosteum. For this fracture, use of a shoulder sling without reduction will lead to healing and an excellent result as the proximal humerus remodels. Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332. Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372. Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
References:
- Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.
Question 91High Yield
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
Explanation
15b 15c The biopsy specimen shows a wavy collagenous matrix with elongated cells; this is most consistent with neurofibroma. The patient has a mass in the region of the sciatic nerve. Imaging characteristics, homogeneous and very low signal on T1-weighted and very high signal on the T2-weighted sequences, are consistent with a myxoid-type lesion. These include myxoma, myxoid sarcomas, and nerve sheath tumors. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
References:
- Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 92High Yield
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
Results have been satisfactory in many patients; however, at long-term follow-up, examination of the affected shoulder often shows some decrease in range of motion compared with the contralateral side. Although range of motion often improves over time, it does not return to normal in 60% of patients. Pain improves but is often increased compared with the contralateral side. Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Question 93High Yield
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
Explanation
The radiograph shows a volarly dislocated lunate. Initial emergent treatment of perilunate dislocations should consist of closed reduction and splinting, especially if the patient exhibits median nerve compression. Open reduction and pinning or ligament repair are necessary but are not emergent. A dorsal approach is sometimes required for ligament repair or bony visualization; however, this can be done in a more semi-elective manner. Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
References:
- Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 94High Yield
Following its exit from the sciatic notch, the sciatic nerve passes between what two muscles?
Explanation
Explanation
Though anatomic variations exist, both divisions of the sciatic nerve most commonly pass between the piriformis and superior gemellus. This anatomic consideration is relevant during the posterior approach to the hip, where careful retraction of the rotators avoids sciatic nerve injury. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 335-348.
References:
- Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Williams, 1978, Figure 4-34.
Question 95High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 96High Yield
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?

Explanation
The patient sustained an injury to the long thoracic nerve, which supplies the serratus anterior. Branches of C5 and C6 enter the scalenus medius, unite in the muscle, and emerge as a single trunk and pass down the axilla. On the surface of the serratus anterior, the long thoracic nerve is joined by the branch from C7 and descends in front of the serratus anterior, providing segmental innervation to the serratus anterior.
Question 97High Yield
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Explanation
Explanation
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome. Shafi S, Elliot AC, Gentilello L: Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry. J Trauma 2005;59:1081-1085. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 98High Yield
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of
Explanation
Explanation
37b 37c Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse. Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
References:
- Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
Question 99High Yield
A favorable outcome following nonsurgical management of a partial tear of the posterior cruciate ligament (PCL) is best associated with
Explanation
Explanation
Rehabilitation of the quadriceps muscle following a partial tear of the PCL has been associated with a favorable outcome. The quadriceps acts an antagonist to the PCL because its contraction results in anterior tibial translation, which reduces the tensile stress on the injured ligament. Strengthening of the hamstring musculature increases posterior tibial translation and is contraindicated during the early rehabilitative phase following a PCL injury. Brace use has not been found to significantly alter the outcome following nonsurgical management of PCL tears. Parolie JM, Bergfeld JA: Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med 1986;14:35-38.
References:
- Griffin JR, Annunziata CC, Harner CD: Posterior cruciate ligament injuries in the adult, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2083-2106.
Question 100High Yield
Stiffness relates the amount of load applied to a structure like a long bone or an intramedullary nail to the amount of resulting deformation that occurs in the structure. What is the most important material property affecting the axial and bending stiffness of a structure?
Explanation
The amount of deformation resulting in response to an applied load depends on the stress distribution that the load creates in the structure and the stress versus strain behavior of the material that makes up the structure. Axial and bending loads create stress distributions that involve normal stresses and normal strains. Although all five responses are indeed material properties, only one, elastic modulus, relates normal stresses to normal strains. In fact, axial and bending stiffness are directly proportional to modulus, so that a nail made from stainless steel will have nearly twice the stiffness of a nail made from titanium alloy (because their respective elastic moduli differ by about a factor of two). Hayes WC, Bouxsein ML: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 74-82. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 159-165.
