Orthopedic Hip 2026 MCQs: Board Review Questions & Answers (Part 2)

Key Takeaway
Here are the crucial details you must know about Orthopedic Hip 2026 MCQs: Board Review Questions & Answers (Part 2). Top-rated Orthopedic Hip 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Hip 2026 MCQs: Board Review Questions & Answers (Part 2)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?
Explanation
Question 2
Which of the following statements best characterizes polymethylmethacrylate (PMMA) when it is used to secure joint components in bone and to distribute the forces evenly across the bone-implant interface?
Explanation
Question 3
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?
Explanation
Question 4
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
Question 5
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
Question 6
Figures 10a through 10c show the radiographs of an 85-year-old man who underwent a revision total knee arthroplasty for loosening of the tibial component 6 months ago. He now reports a mildly uncomfortable mass on the anterior part of the knee joint. Examination reveals 95 degrees of motion and good quadriceps strength, and he can ambulate with minimal pain with a walker. History reveals chronic lymphocytic leukemia for which he is taking antineoplastic medication. Culture of the mass aspirate grew Candida albicans on two separate occasions. The patient and the family strongly prefer nonsurgical management. If long-term suppression is chosen as treatment, what advice should be given to the patient and family?
Explanation
Question 7
Consider the theoretic articulation shown in Figure 11 as femoral and tibial components of a total knee prosthesis in which the components fit like a "roller in trough." Which of the following best describes the articulation?
Explanation
Question 8
A 45-year-old man underwent unipolar hemiarthroplasty reconstruction using cementless fixation for nontraumatic osteonecrosis of the femoral head 5 years ago. He now reports buttock and groin pain that is associated with loading activities. What is the most likely cause of his pain?
Explanation
Question 9
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
Question 10
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
Question 11
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
Question 12
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient's pain?
Explanation
Question 13
A 65-year-old man who underwent cemented right total hip arthroplasty 6 years ago now reports acute pain for the past week. He denies any trauma, recent illnesses, or symptoms other than pain. Plain radiographs show possible loosening of the femoral component. A normal result from which of the following studies will most specifically rule out infection?
Explanation
Question 14
Which of the following procedures is included in third-generation cement technique?
Explanation
Question 15
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Explanation
Question 16
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
Question 17
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
Question 18
Which of the following findings is a relative contraindication to primary total knee arthroplasty?
Explanation
Question 19
Risk of fat embolism is greatest during what step of total hip arthroplasty?
Explanation
Question 20
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Question 21
Wear particles of ultra-high molecular weight polyethylene that are generated by total hip implants are predominantly of what diameter?
Explanation
Question 22
Osteoporosis is best diagnosed by
Explanation
Question 23
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
Question 24
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
Question 25
Metal-on-metal articulation has been reintroduced because of concern about polyethylene wear. This type of articulation is considered favorable because
Explanation
Question 26
A 65-year-old man undergoes an uncomplicated primary total hip arthroplasty. During templating and the procedure, the surgeon decides to increase the femoral offset by 10 mm compared to the contralateral native hip, while perfectly equalizing leg lengths. What is the expected biomechanical consequence of this specific modification?
Explanation
Question 27
A 68-year-old female presents with acute severe left hip pain and fever 3 weeks after a prolonged dental procedure. She underwent a left total hip arthroplasty 6 years ago. Aspiration of the hip yields purulent fluid with 70,000 WBC/uL and 94% neutrophils. Radiographs show well-fixed components with no osteolysis. What is the most appropriate management strategy?
Explanation
Question 28
A 26-year-old male collegiate hockey player presents with chronic anterior groin pain that is exacerbated by sitting in low chairs. Physical examination reveals a positive flexion, adduction, and internal rotation (FADIR) test. Radiographs demonstrate an alpha angle of 72 degrees on the lateral view with no evidence of acetabular retroversion. What is the primary pathophysiologic mechanism of cartilage damage in this condition?
Explanation
Question 29
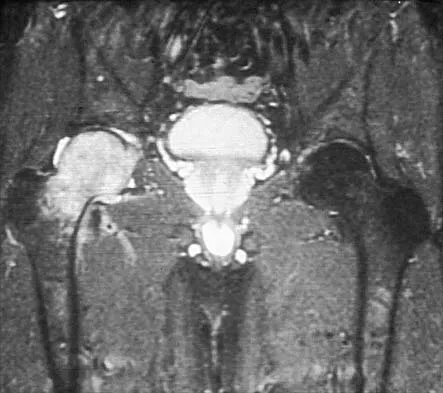
A 58-year-old woman with a metal-on-metal total hip arthroplasty performed 9 years ago presents with new-onset groin pain and a palpable mass. Radiographs show an acetabular component positioned in 55 degrees of abduction. Serum cobalt levels are markedly elevated. An MRI with metal artifact reduction sequence (MARS) demonstrates a solid and cystic mass communicating with the joint space. What is the characteristic histopathological finding associated with this mass?
Explanation
Question 30
During a primary total hip arthroplasty using a direct anterior approach (Hueter interval), the surgeon places a retractor anterior to the acetabulum to aid in exposure for reaming. In the recovery room, the patient demonstrates a profound inability to extend the knee and reports numbness over the anterior thigh. Which of the following technical errors most likely caused this complication?
Explanation
Question 31
A 32-year-old male sustains a high-energy closed fracture of the proximal femur. Radiographs reveal a completely displaced femoral neck fracture with a fracture line oriented 75 degrees from the horizontal plane (Pauwels Type III). What internal fixation construct provides the most biomechanically sound stabilization against the predominant deforming forces in this specific fracture pattern?

Explanation
Question 32
A 71-year-old female presents with recurrent posterior dislocations of her right total hip arthroplasty. Her primary surgery was performed 2 years ago via a posterior approach. CT scan evaluation demonstrates the acetabular component is fixed in 45 degrees of abduction and 5 degrees of retroversion. The femoral component is well-fixed in 15 degrees of anteversion. What is the most appropriate surgical treatment?
Explanation
Question 33
A 42-year-old woman with a history of systemic lupus erythematosus chronically managed with corticosteroids presents with 6 months of debilitating left hip pain. Radiographs demonstrate a sclerotic rim in the anterosuperior femoral head, a visible crescent sign, and slight flattening of the femoral head. The joint space is well preserved (Ficat Stage III). What is the most reliable definitive surgical management for this patient?
Explanation
Question 34
An 85-year-old non-ambulatory, nursing home resident sustains a minor fall. Radiographs show a periprosthetic femur fracture around the tip of a cemented femoral stem placed 15 years ago. The stem has subsided by 2 cm. There is severe, diffuse osteolysis with less than 2 mm of medial and lateral cortical bone remaining in the proximal femur, making it mechanically inadequate to support a newly implanted standard diaphyseal-engaging stem. Based on the Vancouver classification, what is the best surgical intervention?

Explanation
Question 35
A 48-year-old female with bilateral Crowe Type IV developmental dysplasia of the hip (DDH) is undergoing a primary total hip arthroplasty. The preoperative plan is to place the acetabular component in the anatomic true acetabulum. The femoral head is currently dislocated 6 cm superior to the true acetabulum. Which adjunctive surgical technique is most critical to perform during this reconstruction to avoid a devastating postoperative neurologic complication?
Explanation
Question 36
A 65-year-old woman undergoes a primary total hip arthroplasty (THA) via a direct anterior approach. Three weeks postoperatively, she sustains an anterior dislocation of the prosthetic hip while lying in bed and reaching behind her (hip in extension and external rotation). Which of the following acetabular component malpositions most likely contributed to this specific complication?
Explanation
Question 37
In the evaluation of a painful total hip arthroplasty, synovial fluid alpha-defensin testing is obtained to rule out periprosthetic joint infection (PJI). Which of the following best describes the biological origin and function of alpha-defensin in this clinical setting?
Explanation
Question 38
A 55-year-old man with a metal-on-metal (MoM) hip resurfacing presents with new-onset groin pain 5 years postoperatively. Blood cobalt and chromium levels are significantly elevated. An MRI with metal artifact reduction sequence (MARS) reveals a solid pseudotumor. If a biopsy of the periprosthetic tissue were performed, what is the most characteristic histological finding associated with this adverse local tissue reaction (ALTR)?
Explanation
Question 39
Figure 1 shows the radiograph of a 30-year-old man who sustained a displaced, highly vertical femoral neck fracture (Pauwels type III) after a motor vehicle accident. He is planned for open reduction and internal fixation. To biomechanically optimize fixation and resist the predominant shear forces, which of the following construct configurations is most appropriate?
Explanation
Question 40
During a total hip arthroplasty utilizing the direct anterior (Smith-Petersen) approach, the internervous plane is developed between the tensor fasciae latae (TFL) and the sartorius. Which of the following nerves is at greatest risk of iatrogenic injury during the superficial dissection and subsequent retractor placement?
Explanation
Question 41
Figure 4 demonstrates a periprosthetic fracture around a cemented femoral stem in an 82-year-old female. Radiographs show a spiral fracture around the stem with evidence of severe cement mantle disruption and stem subsidence of 1.5 cm. According to the Vancouver classification, what is the most appropriate surgical management?

Explanation
Question 42
A 45-year-old woman with Crowe type IV developmental dysplasia of the hip (DDH) is undergoing total hip arthroplasty. The femoral head is completely dislocated superiorly. During reconstruction, the surgeon intends to place the acetabular component in the true acetabulum. To safely reduce the hip and mitigate the risk of neurologic injury, which of the following surgical adjuncts is most frequently required?
Explanation
Question 43
A 28-year-old male athlete presents with chronic anterior groin pain exacerbated by hip flexion and internal rotation. A Dunn lateral radiograph of the hip reveals an alpha angle of 75 degrees with reduced femoral head-neck offset. This specific morphologic abnormality causes intra-articular damage via which of the following primary pathomechanical processes?
Explanation
Question 44
A 50-year-old highly active man underwent a primary total hip arthroplasty 3 years ago utilizing a ceramic-on-ceramic bearing surface. He presents complaining of an audible "squeaking" noise coming from the hip during bending activities. Radiographs demonstrate well-fixed components without signs of loosening. Which of the following biomechanical factors is most strongly associated with the onset of this phenomenon?
Explanation
Question 45
Figure 10 refers to a 40-year-old woman with systemic lupus erythematosus who presents with severe right groin pain. Radiographs reveal a subchondral radiolucent "crescent sign" and 2 mm of articular surface flattening in the weight-bearing dome of the femoral head. The joint space is preserved. To provide the most reliable long-term pain relief and functional improvement, what is the treatment of choice?
Explanation
Question 46
The direct anterior approach (Smith-Petersen) to the hip is frequently utilized in primary total hip arthroplasty to exploit a true internervous plane. Which of the following best describes the superficial internervous plane utilized in this approach?
Explanation
Question 47
A 68-year-old woman presents with aseptic loosening of her THA. Radiographs demonstrate superior migration of the acetabular component of 3.5 cm, osteolysis extending medially past the Kohler line, and complete destruction of the teardrop. According to the Paprosky classification for acetabular defects, what is the most appropriate management strategy for this specific pattern of bone loss?
Explanation
Question 48
A 24-year-old male hockey player presents with chronic groin pain exacerbated by hip flexion and internal rotation. Imaging reveals a prominent alpha angle of 75 degrees and a normal lateral center-edge angle. Which of the following best describes the primary pathomechanics of his articular cartilage injury?
Explanation
Question 49
A 55-year-old man who underwent a cementless total hip arthroplasty 5 years ago presents with an audible squeaking sound from his hip during walking. He currently has no pain. Radiographs are shown in Figure 4. Which of the following factors most significantly increases the risk of this complication?
Explanation
Question 50
A 72-year-old man presents with a painful total hip arthroplasty 3 years post-surgery. His serum CRP is 25 mg/L and ESR is 45 mm/hr. Hip aspiration yields synovial fluid with a white blood cell (WBC) count of 4,500 cells/µL with 85% polymorphonuclear leukocytes (PMNs). According to the 2018 Evidence-Based Consensus Meeting (ICM) criteria for PJI, which of the following additional tests would provide the most definitive diagnostic value to confirm periprosthetic joint infection?
Explanation
Question 51
A 35-year-old man sustains a completely displaced, vertically oriented femoral neck fracture after a high-speed motor vehicle accident. The fracture angle is 65 degrees relative to the horizontal (Pauwels Type III). Radiographs are shown in Figure 7. Regarding surgical fixation in this young adult, which of the following constructs provides the most biomechanically stable fixation to resist vertical shear forces?

Explanation
Question 52
A 70-year-old woman sustains a posterior dislocation of her total hip arthroplasty 6 weeks postoperatively. Closed reduction in the emergency department is successful. She originally had a posterior approach THA. Radiographs reveal the acetabular component is placed in 10 degrees of anteversion and 35 degrees of abduction. What is the most appropriate next step in management?
Explanation
Question 53
A 42-year-old man on chronic corticosteroids for systemic lupus erythematosus presents with severe left groin pain. Radiographs (Figure 11) show a subchondral radiolucent line (crescent sign) but no flattening of the articular surface. What is the most appropriate definitive management?

Explanation
Question 54
During the templating phase for a primary total hip arthroplasty, the surgeon evaluates the patient's native femoral offset. Which of the following is the most direct biomechanical consequence of inadvertently decreasing the femoral offset during the procedure?
Explanation
Question 55
A 13-year-old obese male presents with a 2-week history of right groin and knee pain. He walks with a noticeable limp but is able to bear weight. Physical examination reveals obligatory external rotation of the hip with passive flexion. Radiographs confirm a mild Slipped Capital Femoral Epiphysis (SCFE) (Figure 15). Following in situ single-screw fixation of the right hip, what is the primary clinical rationale for considering prophylactic fixation of the contralateral hip?

Explanation
Question 56
A 45-year-old active male underwent a ceramic-on-ceramic (CoC) total hip arthroplasty (THA) 3 years ago. He now complains of a new-onset, audible squeaking noise from his hip during walking. He denies any pain or mechanical symptoms. Radiographs show no evidence of loosening or osteolysis. Which of the following is the most significant risk factor associated with this specific complication?
Explanation
Question 57
Figure 1 shows the radiograph of a 72-year-old female who sustained a fall 5 years after an uncemented THA.
Intraoperative evaluation confirms that the femoral stem is grossly loose, but the surrounding proximal bone stock remains adequate to support a revision prosthesis. According to the Vancouver classification, what is the most appropriate definitive management?
Explanation
Question 58
During arthroscopic management of Femoroacetabular Impingement (FAI) for a symptomatic Cam lesion, the surgeon performs an osteochondroplasty at the femoral head-neck junction. Extending the resection too far posterosuperiorly places which of the following anatomic structures at the highest risk of iatrogenic injury?
Explanation
Question 59
Figure 2 shows the pelvis radiograph of a 45-year-old female with severe bilateral hip pain secondary to neglected developmental dysplasia of the hip (DDH).
She is planned for a primary right THA. The templating indicates a Crowe IV dislocation. To restore the hip's center of rotation to the true acetabulum without causing a nerve palsy, which surgical adjunct is most likely required?

Explanation
Question 60
Which of the following Magnetic Resonance Imaging (MRI) findings is considered highly specific for the early diagnosis of avascular necrosis (osteonecrosis) of the femoral head prior to the appearance of radiographic changes?
Explanation
Question 61
A 68-year-old male sustained a posterior dislocation of his right THA 6 weeks postoperatively after tying his shoes. Figure 3 shows his radiograph.
Assuming component malposition was the primary etiology, which combination most commonly predisposes to a posterior dislocation?

Explanation
Question 62
A 55-year-old female presents with new-onset groin pain and a palpable soft tissue mass 8 years after a metal-on-metal hip resurfacing arthroplasty. Serum cobalt and chromium levels are significantly elevated. Histological evaluation of the periprosthetic tissue is most likely to reveal which of the following hallmarks of an adverse local tissue reaction (ALVAL)?
Explanation
Question 63
Figure 4 shows the radiograph of a healthy 55-year-old male who sustained a vertical, displaced femoral neck fracture (Pauwels Type III) after a fall.
To best resist the high vertical shear forces associated with this fracture pattern, which construct is biomechanically superior for joint-preserving fixation?
Explanation
Question 64
A 42-year-old female complains of localized anterior groin pain 1 year following an uncemented THA. The pain is worst when actively lifting her leg to get into a car or actively performing a straight leg raise. A diagnostic injection of local anesthetic into the iliopsoas bursa provides complete, temporary relief. Which acetabular component factor is the most likely structural cause of this complication?
Explanation
Question 65
Tranexamic acid (TXA) is routinely utilized in total hip and knee arthroplasty to minimize perioperative blood loss and reduce transfusion requirements. Which of the following best describes the precise mechanism of action of tranexamic acid?
Explanation
Question 66
A 65-year-old man undergoes a primary total hip arthroplasty. During trialing, the surgeon decides to increase the femoral offset by 10 mm compared to the patient's native anatomy, while keeping the leg length unchanged. What is the expected biomechanical effect of this modification?
Explanation
Question 67
Figure 1 shows the radiograph of a 58-year-old man presenting with insidious onset of progressive groin pain 5 years after an uncomplicated, metal-on-polyethylene total hip arthroplasty. Radiographs show a well-fixed, uncemented stem and cup without evidence of osteolysis. Laboratory workup reveals a serum cobalt level of 14.5 ppb and a serum chromium level of 1.2 ppb. A MARS MRI demonstrates a large, thick-walled cystic periarticular collection. What is the most likely diagnosis?
Explanation
Question 68
A 70-year-old woman complains of a painful total hip arthroplasty that was performed 2 years ago. The pain has been constant for the past 6 months. Hip aspiration yields synovial fluid with a white blood cell count of 4,800 cells/µL and 80% polymorphonuclear leukocytes. An alpha-defensin test is positive. ESR is 55 mm/h, and CRP is 32 mg/L. According to MSIS criteria, the patient has a periprosthetic joint infection (PJI). What is the most appropriate surgical management?
Explanation
Question 69
A 72-year-old woman requires a revision THA for aseptic loosening. Intraoperative assessment, confirming findings on preoperative radiographs (Figure 2), demonstrates a mobile pelvic discontinuity with limited but viable remaining host bone and an intact posterior column structurally. Which of the following reconstructive options provides the most reliable long-term stability and biologic fixation?
Explanation
Question 70
An 8-year-old boy presents with a limp and groin pain. Radiographs confirm the diagnosis of Legg-Calve-Perthes disease. Which of the following radiographic "head-at-risk" signs described by Catterall is considered the most significant predictor of a poor long-term outcome because of its association with mechanical hinge abduction?
Explanation
Question 71
A 13-year-old obese boy with an open triradiate cartilage undergoes in-situ pinning for a stable, moderate slipped capital femoral epiphysis (SCFE) using a single cannulated screw. Six months postoperatively, he complains of severe, unrelenting global hip pain and marked stiffness. Radiographs demonstrate a sudden, severe narrowing of the joint space. What is the most likely diagnosis?
Explanation
Question 72
A surgeon utilizes the direct anterior approach for a primary total hip arthroplasty. To avoid denervating the tensor fasciae latae (TFL) during deep dissection and retractor placement, the surgeon must protect its nerve supply. Which nerve supplies the TFL, and where is it at greatest risk during this approach?
Explanation
Question 73
Figure 3 shows the radiograph of an 82-year-old woman who sustained a fall 10 years after a cemented total hip arthroplasty. The radiograph reveals a periprosthetic spiral fracture around the stem tip. The stem has subsided by 5 mm compared to previous films, and there is a radiolucent line surrounding the cement mantle. The patient has good proximal femoral bone stock. Based on the Vancouver classification, what is the most appropriate management?
Explanation
Question 74
A 6-week-old female infant is diagnosed with developmental dysplasia of the hip. Ultrasound confirms a completely dislocated but reducible left hip. She is treated with a Pavlik harness. After 3 weeks of strict harness wear, a repeat ultrasound reveals that the left hip remains persistently dislocated. What is the most appropriate next step in management?
Explanation
Question 75
A 25-year-old male athlete presents with chronic groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a crossover sign, a prominent ischial spine sign, and a center-edge angle of 42 degrees. These radiographic findings indicate a specific pathomorphology. What is the primary mechanism of articular cartilage damage associated with this condition?
Explanation
Question 76
A 68-year-old man undergoes an uncomplicated right primary total hip arthroplasty (THA). Three weeks postoperatively, he presents with acute onset of right hip pain, a draining sinus tract, and surrounding erythema. Aspiration of the hip joint yields synovial fluid with 45,000 white blood cells/μL and 92% polymorphonuclear neutrophils. Which of the following is the most appropriate initial management?
Explanation
Question 77
A 28-year-old female presents with anterior groin pain that is exacerbated by sitting in a low chair. An AP pelvis radiograph is obtained.
The radiograph demonstrates the anterior rim of the acetabulum crossing over the posterior rim in the superior aspect of the joint. This specific radiographic finding is most strongly associated with which of the following pathomorphologies?
Explanation
Question 78
A 55-year-old woman presents with vague groin pain and a palpable soft tissue fullness in the groin 6 years after undergoing a metal-on-metal THA. Her serum cobalt levels are elevated at 15 ppb. Conventional radiographs demonstrate well-fixed components with no evidence of osteolysis.
What is the most appropriate next step in the diagnostic workup to evaluate for an adverse local tissue reaction (ALTR)?

Explanation
Question 79
An 82-year-old woman falls and sustains a periprosthetic femur fracture around a cemented polished taper-slip stem.
Radiographs demonstrate a fracture at the tip of the stem. The cement mantle is fractured, and the stem has subsided 3 cm. The proximal femoral bone stock remains adequate. According to the Vancouver classification, what is the most appropriate definitive management?
Explanation
Question 80
A surgeon is performing a primary THA utilizing the direct anterior approach (DAA). To minimize the risk of injury to the lateral femoral cutaneous nerve (LFCN), the superficial internervous plane is developed between the tensor fasciae latae (TFL) and the sartorius. During the approach, understanding the variable anatomy of the LFCN is critical. The main trunk of the LFCN most typically crosses the inguinal ligament at what anatomic location?
Explanation
Question 81
A 60-year-old woman complains of new-onset anterior groin pain 6 months following an uncomplicated cementless THA. The pain is worst when lifting her leg to get into a car and is reproduced by an active straight leg raise. Cross-table lateral radiographs reveal the anterior edge of the acetabular cup protruding 8 mm beyond the anterior acetabular rim.
What is the most appropriate initial treatment?

Explanation
Question 82
A 45-year-old highly active man underwent a ceramic-on-ceramic (CoC) THA. Two years postoperatively, he presents complaining of a highly audible squeaking noise coming from his hip during the swing phase of gait. He denies any hip pain. Which of the following is the most significant biomechanical risk factor associated with squeaking in CoC bearings?
Explanation
Question 83
A 42-year-old woman with severe bilateral hip dysplasia presents for right THA. Preoperative standing AP pelvis radiographs demonstrate proximal migration of the femoral head such that it articulates with a false acetabulum. The proximal migration is measured at 110% of the normal vertical height of the femoral head. According to the Crowe classification, what is the appropriate diagnosis, and what adjunctive surgical technique is most likely required during THA?
Explanation
Question 84
A 32-year-old man sustains a completely displaced, high-energy intracapsular femoral neck fracture. In an adult, the viability of the femoral head following this injury is primarily dependent on which of the following arterial vessels?
Explanation
Question 85
A 55-year-old female presents with persistent, severe lateral right hip pain. She has failed 12 months of conservative management for presumed greater trochanteric pain syndrome. Examination reveals a positive Trendelenburg sign.
MRI demonstrates a full-thickness tear of the gluteus medius tendon with 2 cm of retraction and minimal fatty infiltration (Goutallier grade 1) of the muscle belly. What is the most appropriate next step in management?

Explanation
Question 86
A 62-year-old male presents with new-onset groin pain 6 years after a primary total hip arthroplasty. Operative records indicate he received a titanium stem, a cobalt-chromium head, and a highly cross-linked polyethylene liner. Radiographs show a well-fixed stem and cup with no osteolysis. Labs demonstrate an ESR of 12 mm/hr and a CRP of 0.4 mg/dL. Synovial aspirate yields a WBC of 600 cells/µL with 30% polymorphonuclear leukocytes. Metal ion testing reveals an elevated serum cobalt (14 ppb) and a normal chromium (1.2 ppb) level. MARS MRI demonstrates a cystic pseudotumor adjacent to the joint. What is the most likely source of the problem?
Explanation
Question 87
A surgeon utilizes the modified Hardinge (anterolateral) approach for a primary total hip arthroplasty. During the surgical exposure, the anterior portion of the abductor mechanism is detached from the greater trochanter. Injury to which of the following nerves is the most recognized neurological complication if the proximal split in the muscle belly extends too far superiorly?
Explanation
Question 88
An 82-year-old female sustains a fall and presents with severe thigh pain. She underwent a cementless total hip arthroplasty 10 years ago. Radiographs demonstrate a displaced spiral fracture around the tip of the femoral stem. Comparison with prior radiographs indicates the femoral component has subsided 15 mm and is in varus. Based on the Vancouver classification, what is the most appropriate surgical management?
Explanation
Question 89
During preoperative planning for a primary total hip arthroplasty in a patient with significant coxa vara, the surgeon decides to use a high-offset femoral stem. Compared to a standard-offset stem, what is the primary biomechanical advantage of increasing femoral offset?
Explanation
Question 90
A 68-year-old male presents with persistent right hip pain 3 years after a primary total hip arthroplasty. Serum CRP is 18 mg/L and ESR is 45 mm/hr. A diagnostic hip aspiration yields frankly purulent synovial fluid. The synovial fluid WBC count is 15,000 cells/µL with 88% neutrophils. Based on the 2018 International Consensus Meeting (ICM) criteria, what is the next appropriate step in diagnostic management?
Explanation
Question 91
A 32-year-old healthy male sustains a high-energy Pauwels type III (vertical) femoral neck fracture. Which of the following fixation constructs provides the most biomechanically sound stabilization against the significant shear forces inherent to this specific fracture pattern?
Explanation
Question 92
A 25-year-old male undergoes a surgical dislocation of the hip to treat a complex head-neck deformity (cam impingement). To preserve the primary blood supply to the femoral head, the surgeon must be meticulously careful to protect the profound branch of the medial femoral circumflex artery (MFCA). This critical vessel typically runs immediately posterior to which of the following structures?
Explanation
Question 93
A 28-year-old woman with symptomatic developmental dysplasia of the hip (DDH) is undergoing a Bernese periacetabular osteotomy (PAO). Which of the following best describes the key biomechanical advantage and anatomical characteristic of this specific osteotomy technique?
Explanation
Question 94
A 70-year-old male who underwent a total hip arthroplasty 15 years ago presents with progressive leg shortening. Radiographs demonstrate eccentric, superior placement of the femoral head within the acetabular cup and extensive endosteal scalloping with osteolysis in Gruen zones 1 and 7. The stem remains firmly fixed. What is the fundamental cellular mechanism driving this osteolysis?
Explanation
Question 95
A 34-year-old male is positioned for hip arthroscopy to address a symptomatic labral tear. The anterior portal is established under fluoroscopic guidance. To minimize the risk of iatrogenic injury to the lateral femoral cutaneous nerve (LFCN), the portal is placed slightly lateral to the longitudinal anatomical line connecting the ASIS and the center of the patella. In the proximal thigh, the LFCN primarily courses between which two muscles?
Explanation
Question 96
A 68-year-old woman presents to the emergency department with an anterior dislocation of her primary total hip arthroplasty (THA). The index procedure was performed 6 weeks ago via a standard posterior approach. Which of the following component malpositions is most likely responsible for this specific direction of dislocation?
Explanation
Question 97
Figure 1 shows the lateral radiograph of a 22-year-old male athlete with chronic groin pain exacerbated by hip flexion and internal rotation. Based on the most likely diagnosis, what radiographic measurement is most appropriate to quantify the underlying structural abnormality?
Explanation
Question 98
A 72-year-old man presents with severe pain in his right total hip arthroplasty 3 years postoperatively. Radiographs show stable components with no osteolysis. Aspiration of the hip yields synovial fluid with a WBC count of 4,800 cells/µL and 88% polymorphonuclear neutrophils (PMNs). Alpha-defensin testing is positive. Serum CRP is 35 mg/L and ESR is 55 mm/hr. Assuming adequate bone stock and soft tissue coverage, what is the most appropriate next step in management?
Explanation
Question 99
A 30-year-old man sustains a displaced, vertical femoral neck fracture (Pauwels Type III) following a high-energy motor vehicle collision. Open reduction and internal fixation is planned. Which of the following fixation constructs provides the greatest biomechanical stability against vertical shear forces for this specific fracture pattern?
Explanation
Question 100
A surgeon is performing a primary total hip arthroplasty utilizing the direct anterior approach (Smith-Petersen). Development of the superficial internervous plane is required for initial exposure. Which two muscles define this superficial plane, and what are their respective innervations?
Explanation
None
