AAOS & ABOS Orthopedic MCQs (Set 2): Hip Fractures & Arthroplasty | Board Prep

Key Takeaway
This high-yield question set (Set 2) targets the AAOS, ABOS, and OITE exams, focusing on critical hip orthopedic topics. It includes MCQs on femoral neck fracture classification and management, total hip arthroplasty complications, and traumatic hip dislocations.
AAOS & ABOS Orthopedic MCQs (Set 2): Hip Fractures & Arthroplasty | Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?
Explanation
Question 2
Which of the following statements best characterizes polymethylmethacrylate (PMMA) when it is used to secure joint components in bone and to distribute the forces evenly across the bone-implant interface?
Explanation
Question 3
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?
Explanation
Question 4
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
Question 5
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
Question 6
Figures 10a through 10c show the radiographs of an 85-year-old man who underwent a revision total knee arthroplasty for loosening of the tibial component 6 months ago. He now reports a mildly uncomfortable mass on the anterior part of the knee joint. Examination reveals 95 degrees of motion and good quadriceps strength, and he can ambulate with minimal pain with a walker. History reveals chronic lymphocytic leukemia for which he is taking antineoplastic medication. Culture of the mass aspirate grew Candida albicans on two separate occasions. The patient and the family strongly prefer nonsurgical management. If long-term suppression is chosen as treatment, what advice should be given to the patient and family?
Explanation
Question 7
Consider the theoretic articulation shown in Figure 11 as femoral and tibial components of a total knee prosthesis in which the components fit like a "roller in trough." Which of the following best describes the articulation?
Explanation
Question 8
A 45-year-old man underwent unipolar hemiarthroplasty reconstruction using cementless fixation for nontraumatic osteonecrosis of the femoral head 5 years ago. He now reports buttock and groin pain that is associated with loading activities. What is the most likely cause of his pain?
Explanation
Question 9
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
Question 10
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
Question 11
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
Question 12
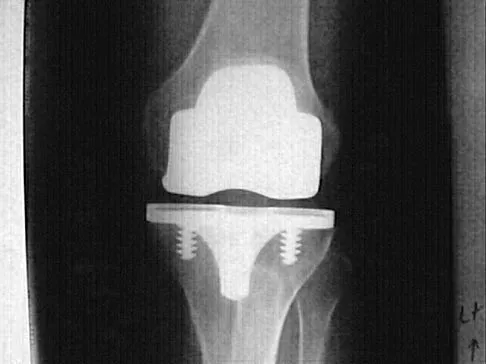
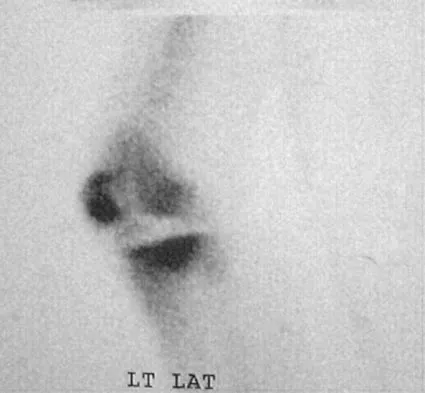
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient's pain?
Explanation
Question 13
A 65-year-old man who underwent cemented right total hip arthroplasty 6 years ago now reports acute pain for the past week. He denies any trauma, recent illnesses, or symptoms other than pain. Plain radiographs show possible loosening of the femoral component. A normal result from which of the following studies will most specifically rule out infection?
Explanation
Question 14
Which of the following procedures is included in third-generation cement technique?
Explanation
Question 15
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Explanation
Question 16
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
Question 17
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
Question 18
Which of the following findings is a relative contraindication to primary total knee arthroplasty?
Explanation
Question 19
Risk of fat embolism is greatest during what step of total hip arthroplasty?
Explanation
Question 20
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Question 21
Wear particles of ultra-high molecular weight polyethylene that are generated by total hip implants are predominantly of what diameter?
Explanation
Question 22
Osteoporosis is best diagnosed by
Explanation
Question 23
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
Question 24
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
Question 25
Metal-on-metal articulation has been reintroduced because of concern about polyethylene wear. This type of articulation is considered favorable because
Explanation
Question 26
What is the primary advantage of highly cross-linked polyethylene (HXLPE) compared to conventional polyethylene in total hip arthroplasty?
Explanation
Question 27
A 72-year-old man sustains a reverse obliquity intertrochanteric femur fracture. Which of the following fixation constructs provides the highest biomechanical stability for this fracture pattern?
Explanation
Question 28
A patient undergoes a primary total hip arthroplasty via a direct anterior approach. If this patient experiences a postoperative dislocation, in which position is the hip most likely to be unstable?
Explanation
Question 29
During preoperative templating for a total hip arthroplasty, increasing the femoral neck offset without changing the neck resection level or stem length will result in which of the following?
Explanation
Question 30
A 35-year-old man sustains a vertically oriented (Pauwels type III) displaced femoral neck fracture. What is the most appropriate internal fixation construct to minimize shear forces and prevent varus collapse?
Explanation
Question 31
A 68-year-old woman presents with persistent groin pain 2 years after a primary total hip arthroplasty. Aspiration of the hip joint yields synovial fluid with a white blood cell (WBC) count of 4,500 cells/mcL and 85% polymorphonuclear neutrophils (PMNs). What is the most appropriate next step in management?
Explanation
Question 32
In a proximal third subtrochanteric femur fracture, the proximal fragment is typically displaced into which of the following positions?
Explanation
Question 33
A 65-year-old man presents with progressive groin pain 5 years after receiving a total hip arthroplasty utilizing a 40-mm cobalt-chromium femoral head on a titanium stem. MRI with metal artifact reduction sequence (MARS) shows a solid cystic mass in the abductor musculature. Blood metal ion testing shows significantly elevated serum cobalt with normal chromium. What is the most likely diagnosis?
Explanation
Question 34
During acetabular component fixation in total hip arthroplasty, screw placement in the anterosuperior quadrant places which of the following structures at greatest risk of injury?
Explanation
Question 35
A 40-year-old woman undergoes closed reduction and percutaneous pinning for a displaced femoral neck fracture. Which of the following factors is most predictive of subsequent osteonecrosis of the femoral head?
Explanation
Question 36
Which of the following nerves is at greatest risk of injury during a direct lateral (Hardinge) approach to the hip?
Explanation
Question 37
A 78-year-old woman presents with thigh pain and inability to bear weight after a mechanical fall. Radiographs demonstrate a fracture around her cemented femoral stem just distal to the lesser trochanter. The stem has subsided 1.5 cm and there is a visible cement mantle fracture. What is the most appropriate surgical treatment?
Explanation
Question 38
A patient experiences recurrent posterior dislocations after a total hip arthroplasty. Radiographs and CT scans reveal the acetabular component is placed in 10 degrees of anteversion and 35 degrees of inclination. The femoral stem is in 15 degrees of anteversion. What is the most appropriate definitive management?
Explanation
Question 39
During a primary total knee arthroplasty, the trial components are evaluated. The knee is tight in both flexion and extension. What is the most appropriate next step to balance the gaps?
Explanation
Question 40
In an active, community-dwelling 70-year-old patient with a displaced femoral neck fracture, what is the primary advantage of total hip arthroplasty (THA) over bipolar hemiarthroplasty?
Explanation
Question 41
What is the predominant blood supply to the adult femoral head?
Explanation
Question 42
According to the AAOS clinical practice guidelines on venous thromboembolic disease prophylaxis after elective total hip arthroplasty, which of the following regimens is recommended for patients with standard risk profiles?
Explanation
Question 43
A 72-year-old woman sustains a fall. Radiographs reveal a displaced femoral neck fracture.
She is an active community ambulator and cognitively intact. Which of the following treatments provides the lowest rate of reoperation?

Explanation
Question 44
A 68-year-old man presents with an unstable intertrochanteric femur fracture.
A cephalomedullary nail is planned. To minimize the risk of hardware cut-out, what is the ideal tip-apex distance (TAD)?

Explanation
Question 45
During a direct anterior approach for a total hip arthroplasty, the surgeon dissects between the tensor fasciae latae and the sartorius. Which of the following nerves is at greatest risk of injury during this superficial dissection?
Explanation
Question 46
An 80-year-old woman with a history of severe osteoporosis undergoes a cemented total hip arthroplasty. During cement pressurization and stem insertion, her blood pressure drops precipitously. What is the primary pathophysiologic mechanism for bone cement implantation syndrome (BCIS)?
Explanation
Question 47
A 55-year-old woman presents with persistent anterior groin pain one year after a primary total hip arthroplasty. The pain is exacerbated by rising from a seated position and active straight leg raising. Radiographs demonstrate the acetabular component is placed in 15 degrees of anteversion, but the anterior edge extends 8 mm beyond the native anterior acetabular rim. What is the most likely diagnosis?
Explanation
Question 48
A 30-year-old male sustains a high-energy Pauwels type III (vertical) femoral neck fracture. He is medically stable. Which of the following biomechanical constructs provides the most stable fixation for this specific fracture pattern?
Explanation
Question 49
A 75-year-old patient falls and sustains a periprosthetic femur fracture around a fully porous-coated cementless stem.
Radiographs show a fracture at the tip of the stem. The stem is definitively loose, but there is excellent proximal bone stock. According to the Vancouver classification, what is the fracture subtype and optimal treatment?
Explanation
Question 50
A 65-year-old man is scheduled for primary total hip arthroplasty. He is healthy with no history of prior DVT, pulmonary embolism, or bleeding disorders. According to the latest AAOS guidelines, what is the most appropriate routine venous thromboembolism (VTE) prophylaxis postoperatively?
Explanation
Question 51
A patient with a metal-on-metal total hip arthroplasty presents with increasing pain and a large, sterile fluid collection around the hip. MRI with metal artifact reduction shows a solid and cystic mass. A biopsy is obtained. What is the most likely histologic finding of the periprosthetic tissue?
Explanation
Question 52
During a posterior approach to the hip for total hip arthroplasty, the short external rotators are detached. The primary blood supply to the native adult femoral head, which is sacrificed during the femoral neck osteotomy, arises from which of the following vessels?
Explanation
Question 53
A 65-year-old man sustains recurrent posterior dislocations following a primary total hip arthroplasty. Radiographs demonstrate an acetabular component in 10 degrees of retroversion and 40 degrees of abduction. Which of the following is the most appropriate definitive management?
Explanation
Question 54
A 25-year-old man sustains a vertically oriented (Pauwels type III) femoral neck fracture. Biomechanical studies indicate which of the following constructs provides the greatest stability against shear forces for this fracture pattern?
Explanation
Question 55
A 78-year-old woman with an intertrochanteric hip fracture is found to have a highly comminuted lateral wall on pre-operative imaging. Which fixation method is most appropriate?
Explanation
Question 56
In a direct anterior approach for total hip arthroplasty, the superficial internervous plane is utilized. Which two nerves supply the muscles defining this plane?
Explanation
Question 57
A 70-year-old man presents with a Vancouver B2 periprosthetic femur fracture 10 years after a cemented total hip arthroplasty. The fracture is located around the tip of the stem, and the stem is demonstrably loose. What is the recommended treatment?
Explanation
Question 58
A 25-year-old man sustains a completely displaced, vertically oriented femoral neck fracture (Pauwels type III). Which of the following fixation constructs offers the highest biomechanical stability for this specific fracture pattern?
Explanation
Question 59
A 72-year-old woman sustains the fracture shown in the radiograph, characterized as a reverse obliquity intertrochanteric fracture. What is the most appropriate definitive management?
Explanation
Question 60
A 68-year-old man presents with a painful THA 4 years postoperatively. Synovial fluid analysis reveals a WBC count of 4,500 cells/uL with 85% neutrophils. What is the next most appropriate step in management if a chronic periprosthetic joint infection is confirmed?
Explanation
Question 61
An 81-year-old woman sustains a periprosthetic fracture around her cementless THA stem. Radiographs show a fracture extending just distal to the stem tip with evidence of stem subsidence and loosening. Based on the Vancouver classification, what is the most appropriate treatment?
Explanation
Question 62
A patient experiences recurrent posterior dislocations of their THA. The acetabular component is evaluated on CT scan and found to be placed in 5 degrees of anteversion and 30 degrees of abduction. Which parameter falls outside the traditional Lewinnek safe zone and is contributing most to the instability?
Explanation
Question 63
What is the primary biological mechanism responsible for the aseptic loosening and osteolysis commonly seen in older generation polyethylene total hip replacements?
Explanation
Question 64
A 55-year-old man with a metal-on-metal THA presents with groin pain and a palpable mass. Serum cobalt and chromium levels are elevated. MARS MRI demonstrates a large solid and cystic mass. What is the most characteristic histological finding of the periprosthetic tissue in this scenario?
Explanation
Question 65
A 70-year-old woman on long-term alendronate therapy reports a 3-month history of vague thigh pain. Radiographs reveal lateral cortical thickening and a transverse radiolucent line in the subtrochanteric region. What is the most appropriate prophylactic surgical management for this impending fracture?
Explanation
Question 66
Medical optimization and surgical treatment of an acute hip fracture in a geriatric patient should ideally be completed within what timeframe to most significantly reduce 30-day and 1-year mortality rates?
Explanation
Question 67
A 45-year-old active male is undergoing a THA. The surgeon selects a ceramic-on-ceramic bearing surface. What is the most commonly reported specific complication associated with this bearing coupling compared to other options?
Explanation
Question 68
During the insertion of a cemented femoral stem for a femoral neck fracture, the patient develops sudden hypoxia, hypotension, and right heart strain. What is the most important step a surgeon can take during canal preparation to minimize the risk of this specific complication?

Explanation
Question 69
Following a primary THA using a posterior approach, a patient exhibits a foot drop and inability to extend the great toe. Which specific portion of the sciatic nerve is most vulnerable to injury during this procedure?
Explanation
Question 70
A 65-year-old man with a history of hypertrophic osteoarthritis and prior contralateral heterotopic ossification (HO) undergoes a THA. What is the most appropriate prophylactic regimen to prevent recurrence of HO in this high-risk patient?
Explanation
Question 71
A patient complains of groin pain starting 3 months after a cementless THA. The pain is worst when rising from a seated position. Examination shows pain with active hip flexion against resistance. Radiographs demonstrate an acetabular component in 10 degrees of retroversion with an overhanging anterior edge. What is the most likely diagnosis?
Explanation
Question 72
A 72-year-old woman with a prior multi-level lumbar spinal fusion (L2-Pelvis) is planned for a THA. How does her spinal fusion alter her spinopelvic mechanics, and what intraoperative adjustment should be considered?
Explanation
Question 73
A 28-year-old male sustains a displaced femoral neck fracture in a motor vehicle collision. He is hemodynamically stable. What is the most appropriate surgical management to minimize the risk of avascular necrosis and nonunion?
Explanation
Question 74
A 75-year-old female presents with an intertrochanteric femur fracture. Radiographs demonstrate an intact posteromedial cortex but a lateral wall thickness of 18 mm. Which of the following is the most appropriate implant choice to minimize the risk of construct failure?
Explanation
Question 75
A 65-year-old male complains of recurrent posterior dislocations following a primary total hip arthroplasty performed via a posterior approach. Radiographs show the acetabular cup is placed in 40 degrees of abduction and 0 degrees of anteversion. What is the most appropriate definitive management?
Explanation
Question 76
A 68-year-old woman with a 10-year history of alendronate use presents with thigh pain and sustains a low-energy subtrochanteric femur fracture. Radiographs reveal a transverse fracture with lateral cortical beaking. Which of the following surgical principles is critical in her management?
Explanation
Question 77
A 70-year-old male presents with a painful total hip arthroplasty that has been symptomatic for 18 months. Aspiration reveals 45,000 WBC/mcL with 90% polymorphonuclear cells. Radiographs show circumferential radiolucencies around a loose femoral stem. What is the gold standard surgical management?
Explanation
Question 78
A 74-year-old woman sustains a fall around her cemented total hip arthroplasty.
Radiographs demonstrate a periprosthetic fracture around a loose femoral stem, but the proximal femur bone stock remains adequate. According to the Vancouver classification, what is the most appropriate surgical treatment?
Explanation
Question 79
During a direct anterior approach for a total hip arthroplasty, the surgeon utilizes the internervous plane between which of the following muscles?
Explanation
Question 80
What is the primary clinical advantage of utilizing highly cross-linked polyethylene (HXLPE) compared to conventional polyethylene in total hip arthroplasty?
Explanation
Question 81
Current evidence suggests that in elderly patients undergoing hemiarthroplasty for a displaced femoral neck fracture, the use of a cemented femoral stem compared to an uncemented stem is associated with which of the following?
Explanation
Question 82
A 60-year-old male with a metal-on-metal total hip arthroplasty presents with increasing groin pain. MRI reveals a large, thick-walled cystic mass. Serum cobalt and chromium levels are significantly elevated. The pathogenesis of this complication is best described as:
Explanation
Question 83
A 52-year-old female complains of a high-pitched squeaking noise coming from her total hip arthroplasty during ambulation. The implant is a ceramic-on-ceramic bearing. Which of the following is the most significant risk factor for this phenomenon?
Explanation
Question 84
Trunnionosis, or mechanically assisted crevice corrosion, has emerged as a significant mode of failure in modern total hip arthroplasties. Which of the following implant characteristics most increases the risk of this complication?
Explanation
Question 85
The main blood supply to the adult femoral head is the lateral epiphyseal artery. This artery is a terminal branch of which of the following vessels?
Explanation
Question 86
A 55-year-old male complains of numbness and burning over the anterolateral aspect of his thigh following a primary total hip arthroplasty. Which surgical approach was most likely utilized?
Explanation
Question 87
A 68-year-old female presents with persistent anterior groin pain 6 months after a total hip arthroplasty. The pain is exacerbated by active straight leg raising and getting out of a car. Radiographs reveal the acetabular cup is in 45 degrees of abduction and 20 degrees of anteversion, with slight anterior overhang. What is the most appropriate initial management?
Explanation
Question 88
During a total hip arthroplasty via a posterior approach, the surgeon meticulously repairs the short external rotators and the posterior capsule to the greater trochanter. What is the primary established clinical benefit of this step?
Explanation
Question 89
A 78-year-old male with multiple medical comorbidities sustains a displaced femoral neck fracture. When counseling the family regarding prognosis, what is the approximate expected 1-year mortality rate for patients over age 65 following a hip fracture?
Explanation
Question 90
A 72-year-old male with an intertrochanteric femur fracture is treated with a sliding hip screw (DHS). Three months postoperatively, radiographs show cutout of the lag screw through the superior femoral head. Which of the following technical factors is most highly associated with this mode of failure?
Explanation
Question 91
A patient requires a revision total hip arthroplasty for massive osteolysis. Preoperative planning suspects pelvic discontinuity. Which of the following radiographic findings is most characteristic of this condition?
Explanation
Question 92
During surgical fixation of a displaced femoral neck fracture with three cannulated screws, an inverted triangle configuration is utilized. What is the primary biomechanical rationale for placing the inferior screw closely adjacent to the calcar?
Explanation
Question 93
A 55-year-old highly active man is undergoing a total hip arthroplasty (THA). He is particularly concerned about the longevity of the implants and volumetric wear. Which of the following bearing surface combinations is biomechanically proven to have the lowest volumetric wear rate?
Explanation
Question 94
A 72-year-old woman sustains a reverse obliquity intertrochanteric femur fracture (OTA 31-A3). Based on current biomechanical studies and clinical evidence, which of the following constructs provides the most stable fixation with the lowest rate of hardware failure?
Explanation
Question 95
A 68-year-old man presents with his third posterior dislocation of a primary THA performed 4 months ago. Radiographs demonstrate the acetabular component is in 35 degrees of abduction and 5 degrees of retroversion. The femoral stem is stable and in neutral version. What is the most appropriate definitive management?
Explanation
Question 96
A 32-year-old man sustains a completely displaced, vertically oriented femoral neck fracture (Pauwels Type III). What is the optimal fixation construct to minimize the risk of varus collapse, shear failure, and nonunion?
Explanation
Question 97
During a direct anterior approach for total hip arthroplasty, the surgeon dissects between the sartorius and the tensor fasciae latae. Which of the following neurologic structures is at highest risk of iatrogenic injury during the exposure of this specific internervous interval?
Explanation
Question 98
A 65-year-old woman presents with worsening right hip pain 2 years after a primary THA. Her inflammatory markers are elevated (ESR 45 mm/hr, CRP 3.2 mg/dL). Synovial fluid aspiration reveals a WBC count of 3,500 cells/uL with 75% PMNs. Which of the following synovial fluid biomarkers has the highest specificity for confirming a periprosthetic joint infection?
Explanation
Question 99
During a posterior approach THA, trial reduction reveals that the leg is lengthened by 1.5 cm and the offset is decreased by 1 cm compared to the preoperative template. Shuck testing shows significant soft tissue laxity. Which modular adjustment will best restore proper offset and soft tissue tension while minimizing further leg lengthening?
Explanation
Question 100
A 68-year-old woman on long-term alendronate for osteoporosis presents with a 3-month history of prodromal anterior thigh pain.
Radiographs demonstrate a transverse, nondisplaced radiolucency in the lateral cortex of the subtrochanteric region with localized periosteal "beaking." What is the most appropriate next step in management?
Explanation
None
