AAOS & ABOS Board Review (Set 4): Proximal Femur Fractures & Hip Dislocations MCQs

Key Takeaway
This high-yield MCQ set for AAOS, ABOS, and OITE board review critically evaluates knowledge of proximal femur fractures, covering classification and surgical fixation. It also tests understanding of hip dislocation types and reduction techniques, along with key aspects of avascular necrosis of the femoral head.
AAOS & ABOS Board Review (Set 4): Proximal Femur Fractures & Hip Dislocations MCQs
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the average linear wear rate of a conventional, noncross-linked ultra-high molecular weight polyethylene liner used in total hip arthroplasty?
Explanation
Question 2
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient's pain?
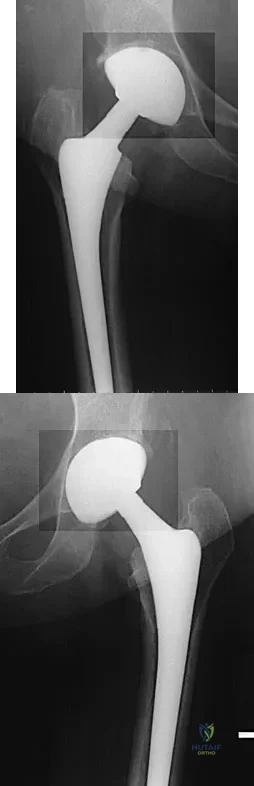
Explanation
Question 3
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
Question 4
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
Question 5
Which of the following surgical techniques is associated with an increased incidence of patellar complications after total knee arthroplasty?
Explanation
Question 6
A large circumferential proximal femoral allograft is to be used in the reconstruction of a failed femoral component in a total hip arthroplasty. To enhance fixation of the graft to the implant, which of the following strategies should be used?
Explanation
Question 7
Which of the following design features of a femoral component used in a total knee arthroplasty best minimizes the patellar component contact stresses?
Explanation
Question 8
Figure 22 shows the radiograph of a 67-year-old woman who has an infected left total hip arthroplasty. The most efficient means to remove the distal cement mantle includes the use of

Explanation
Question 9
Which of the following findings best describes the effects of increasing conformity of a fixed tibial bearing component and femoral component in total knee arthroplasty?
Explanation
Question 10
Figures 23a and 23b show the AP and lateral radiographs of a 67-year-old woman who has severe left knee pain when ambulating. History reveals that she underwent primary total knee arthroplasty 7 years ago. The patient reports increasing deformity over the past several years and uses a knee brace and a cane. Examination reveals that she walks with a varus thrust and has an uncorrectable varus deformity with valgus force. What is the primary reason for implant failure?
Explanation
Question 11
Which of the following bearing surface combinations has shown the lowest in vivo wear rates in total hip arthroplasty?
Explanation
Question 12
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of

Explanation
Question 13
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
Question 14
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of

Explanation
Question 15
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
Question 16
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
Question 17
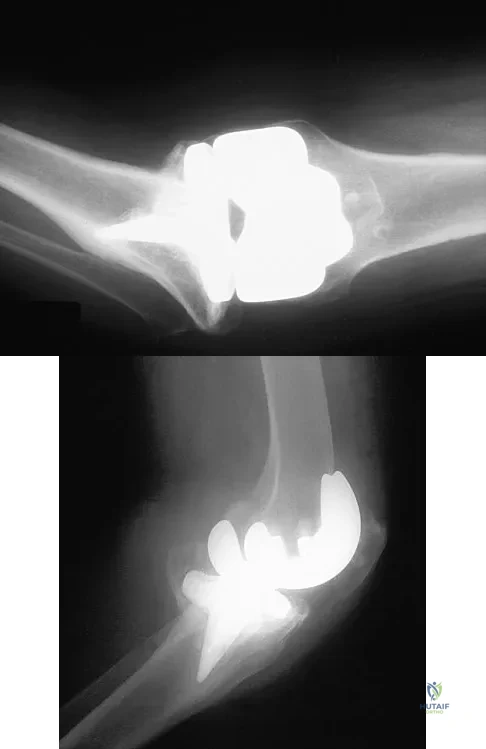
A 72-year-old woman with rheumatoid arthritis who underwent primary total knee arthroplasty 2 years ago has had diffuse knee pain that developed shortly after the surgery. The patient has difficulty with stair descent and arising from chairs. Evaluation for infection is negative. AP and lateral radiographs are shown in Figure 26. Management should now consist of
Explanation
Question 18
A homebound 75-year-old woman with diabetes mellitus has had progressive left knee pain and swelling for the past 6 weeks. She is febrile with a temperature of 103 degrees F (39.5 degrees C). History reveals that she underwent arthroplasty 5 years ago. Examination shows passive range of motion of 0 to 100 degrees with no active extension. Knee aspiration reveals purulent fluid with a Gram stain showing gram-negative rods. A radiograph is shown in Figure 27. In addition to IV antibiotics, which of the following management options offers the best chance of a successful outcome?

Explanation
Question 19
Design and manufacturing of a metal-on-metal articulation has an important influence on the tribology. Which of the following statements best characterizes the type of contact that is best for metal-on-metal articulations?
Explanation
Question 20
A 52-year-old man has had groin and deep buttock pain for the past 2 months. Examination reveals that hip range of motion is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 28. Management should consist of

Explanation
Question 21
Polyethylene wear of the bearing surface has been recognized as a mode of failure in total knee arthroplasty; therefore, many patients are offered polyethylene exchange. In terms of success rates, this surgical procedure has been reported to have a
Explanation
Question 22
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Explanation
Question 23
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
Question 24
During the implantation of a cementless acetabular component in total hip arthroplasty, placement of a screw in the anterior superior quadrant puts which of the following structures at risk for damage?
Explanation
Question 25
What is the most frequent complication following primary total hip arthroplasty?
Explanation
Question 26
A 32-year-old man sustains a highly displaced, Pauwels type III femoral neck fracture in a motor vehicle collision. Which of the following fixation constructs provides the greatest biomechanical stability against vertical shear forces for this fracture pattern?
Explanation
Question 27
A 45-year-old man is brought to the emergency department after a dashboard injury. Radiographs reveal a posterior hip dislocation associated with a femoral head fracture extending cephalad to the fovea capitis. According to the Pipkin classification, what is the most appropriate definitive management for the femoral head injury?
Explanation
Question 28
In a substantially displaced subtrochanteric femur fracture, the proximal fragment typically assumes a characteristic position of flexion, abduction, and external rotation. Which muscle is primarily responsible for the abduction deformity?
Explanation
Question 29
A 28-year-old woman sustains a posterior hip dislocation during a high-speed collision. After closed reduction, she exhibits a foot drop and decreased sensation over the dorsum of her foot. Which portion of the sciatic nerve is most vulnerable in this injury, and what specific area of sensory loss is most diagnostic for its isolated injury?
Explanation
Question 30
A 75-year-old community-ambulating woman with no significant medical comorbidities sustains a displaced, acute intracapsular femoral neck fracture. Based on current literature, what is the primary advantage of treating this patient with a total hip arthroplasty (THA) compared to a hemiarthroplasty?
Explanation
Question 31
Radiographs of an 82-year-old man who fell from standing reveal an intertrochanteric femur fracture with a fracture line extending from the medial cortex proximal to the lesser trochanter diagonally to the lateral cortex distal to the greater trochanter. What is the most appropriate implant for this fracture pattern?
Explanation
Question 32
A 22-year-old athlete presents with an acute anterior hip dislocation following a rugby tackle. To minimize the risk of osteonecrosis of the femoral head, closed reduction should ideally be performed within what maximum timeframe from the time of injury?
Explanation
Question 33
A 68-year-old woman with a 9-year history of alendronate therapy reports an insidious onset of right thigh pain. Radiographs reveal focal lateral cortical thickening of the proximal femoral diaphysis with a subtle, transverse radiolucent line extending through the lateral cortex. What is the most appropriate management?
Explanation
Question 34
Which of the following clinical postures is most characteristic of a patient presenting with an obturator-type anterior hip dislocation?
Explanation
Question 35
A 35-year-old man underwent closed reduction and percutaneous pinning of a femoral neck fracture 9 months ago. He now presents with persistent groin pain. Imaging reveals a nonunion with varus collapse, but MRI confirms the femoral head remains entirely viable. What is the most appropriate joint-preserving surgical intervention?
Explanation
Question 36
Which of the following fracture patterns inherently lacks cancellous bone interdigitation across the fracture site, making multiple cannulated screws an inferior biomechanical choice compared to a sliding hip screw?
Explanation
Question 37
When utilizing a trochanteric entry portal for a cephalomedullary nail to treat a standard intertrochanteric femur fracture, starting the guidewire too laterally on the greater trochanter is most likely to result in which of the following intraoperative complications?
Explanation
Question 38
A 40-year-old man undergoes successful closed reduction of a posterior hip dislocation in the emergency department. Post-reduction anteroposterior pelvis radiographs demonstrate an asymmetric widening of the medial joint space on the injured side. What is the most appropriate next step in management?
Explanation
Question 39
Which anatomic structure is most frequently implicated in blocking the successful closed reduction of an acute posterior hip dislocation?
Explanation
Question 40
In the surgical treatment of intertrochanteric femur fractures using a dynamic hip screw, achieving a Tip-Apex Distance (TAD) of less than 25 mm is critical. What is the primary purpose of adhering to this measurement?
Explanation
Question 41
A 13-year-old boy sustains a displaced subtrochanteric femur fracture. Intramedullary nailing using a piriformis fossa entry point is considered. What is the most significant risk associated with this specific entry portal in the adolescent population?
Explanation
Question 42
An 80-year-old woman is diagnosed with a Garden I femoral neck fracture. Which of the following best describes the radiographic appearance and optimal management of this injury?
Explanation
Question 43
The predominant blood supply to the adult femoral head, which is highly vulnerable during a displaced intracapsular femoral neck fracture, is derived primarily from which of the following vessels?
Explanation
Question 44
A surgeon is evaluating a patient with an intertrochanteric fracture to determine the risk of postoperative lateral wall fracture if a dynamic hip screw (DHS) is used. According to the literature, an intact lateral wall thickness below what threshold on the preoperative anteroposterior radiograph strongly contraindicates the use of a DHS?
Explanation
Question 45
Which of the following parameters is an absolute indication for open reduction of a posterior hip dislocation rather than proceeding with an initial closed reduction attempt in the emergency department?
Explanation
Question 46
A 28-year-old unrestrained driver is involved in a motor vehicle collision. In the emergency department, his right lower extremity is shortened, adducted, and internally rotated. He is unable to dorsiflex his right foot or extend his toes. What is the most likely direction of his hip dislocation and the specific injured nerve branch?
Explanation
Question 47
A 72-year-old man falls and sustains a reverse obliquity intertrochanteric fracture of the left femur. Which of the following fixation constructs offers the highest biomechanical stability and lowest risk of failure for this specific fracture pattern?
Explanation
Question 48
During closed reduction of a subtrochanteric femur fracture in a 35-year-old man, the proximal fragment remains persistently flexed, abducted, and externally rotated. Which muscle is primarily responsible for the flexion and external rotation of the proximal segment?
Explanation
Question 49
When treating an intertrochanteric femur fracture with a sliding hip screw or cephalomedullary nail, the tip-apex distance (TAD) is a critical predictor of lag screw cut-out. According to Baumgaertner, what is the recommended maximum TAD to minimize this complication?
Explanation
Question 50
A healthy, independent 70-year-old woman sustains a displaced femoral neck fracture. She is an avid golfer and walks two miles daily. Comparing total hip arthroplasty (THA) to bipolar hemiarthroplasty for this specific patient, THA is associated with which of the following?
Explanation
Question 51
A 40-year-old man sustains a posterior hip dislocation with an associated fracture of the femoral head and a posterior wall acetabular fracture. According to the Pipkin classification, what type of fracture-dislocation is this?
Explanation
Question 52
A 25-year-old skier crashes and presents to the emergency department with severe groin pain. On examination, his right hip is held in a position of marked flexion, abduction, and external rotation. Radiographs confirm an anterior hip dislocation. Which anatomical structure is most at risk of injury in this specific dislocation pattern?
Explanation
Question 53
A 78-year-old woman presents with severe hip pain and an inability to bear weight after a mechanical fall from standing height. Anteroposterior and cross-table lateral radiographs of the hip are entirely negative for fracture. What is the most appropriate next step in diagnosis?
Explanation
Question 54
A 32-year-old man sustains a vertically oriented, displaced femoral neck fracture (Pauwels Type III) after a fall from a height. Which of the following internal fixation constructs is biomechanically superior for resisting the high shear forces associated with this fracture pattern?
Explanation
Question 55
The primary blood supply to the weight-bearing dome of the adult femoral head is derived from which of the following vessels?
Explanation
Question 56
A 45-year-old man presents with groin pain 8 months after internal fixation of a displaced femoral neck fracture with three cannulated screws. Radiographs reveal a nonunion with screw back-out, but MRI confirms the femoral head is fully viable with no osteonecrosis. What is the most appropriate surgical treatment?
Explanation
Question 57
A 30-year-old man suffers a posterior hip dislocation. Two attempts at closed reduction under conscious sedation are unsuccessful. During the subsequent open reduction via a posterior Kocher-Langenbeck approach, which of the following structures is most likely found to be obstructing the reduction?
Explanation
Question 58
A 65-year-old woman on long-term alendronate therapy complains of a dull ache in her right thigh. Radiographs reveal focal lateral cortical thickening and a transverse radiolucent line in the subtrochanteric region. What is the pathognomonic radiographic feature of a complete fracture of this type if it were to displace?
Explanation
Question 59
A 35-year-old man presents to the emergency department following a high-speed motor vehicle collision with his knee striking the dashboard. On physical examination, his right lower extremity is shortened, flexed, adducted, and internally rotated. Which of the following neurologic deficits is most commonly associated with this specific injury pattern?
Explanation
Question 60
A 75-year-old woman sustains a ground-level fall. Radiographs demonstrate a reverse obliquity intertrochanteric fracture of the proximal femur. Which of the following implants is biomechanically most appropriate for this fracture pattern?
Explanation
Question 61
To minimize the risk of lag screw cut-out when using a sliding hip screw or cephalomedullary nail for intertrochanteric fracture fixation, the Tip-Apex Distance (TAD) as described by Baumgaertner should be maintained below what value?
Explanation
Question 62
A 28-year-old woman sustains a high-energy, vertically oriented, displaced femoral neck fracture (Pauwels type III). If internal fixation is chosen, which of the following constructs provides the greatest biomechanical stability against the predominant deforming shear forces?
Explanation
Question 63
A healthy, independent, 72-year-old community-dwelling man who regularly plays golf sustains a displaced femoral neck fracture. He is discussing surgical options, specifically hemiarthroplasty versus total hip arthroplasty (THA). What is a well-documented long-term advantage of THA in this specific demographic?
Explanation
Question 64
A 25-year-old man presents with a posterior hip dislocation associated with a fracture of the femoral head. A computed tomography scan shows the fracture involves the superior aspect of the femoral head, cephalad to the fovea capitis. What is the correct Pipkin classification for this injury?
Explanation
Question 65
In a patient presenting with an obturator-type anterior hip dislocation, what is the classic resting position of the affected lower extremity?
Explanation
Question 66
A 30-year-old man sustains a transverse subtrochanteric femur fracture. Due to the muscular attachments in this region, the proximal fragment is typically displaced into which of the following positions?
Explanation
Question 67
Which of the following vessels provides the predominant blood supply to the adult femoral head, placing it at the greatest risk for avascular necrosis following a displaced femoral neck fracture?
Explanation
Question 68
A 40-year-old man sustains a traumatic posterior hip dislocation without associated fractures. To minimize the risk of developing avascular necrosis of the femoral head, a closed reduction should ideally be successfully performed within what maximum timeframe?
Explanation
Question 69
A 65-year-old woman undergoes fixation of a stable intertrochanteric fracture with a sliding hip screw. Intraoperative fluoroscopy reveals an intact lateral wall thickness of 15 mm. Based on this measurement, what is the most likely biomechanical complication of this construct?
Explanation
Question 70
A 68-year-old woman with a 10-year history of daily alendronate use presents with progressive, severe right thigh pain with weight-bearing. Radiographs demonstrate focal lateral cortical thickening (beaking) and a transverse radiolucent line involving 60% of the lateral cortex in the subtrochanteric region. What is the most appropriate management?
Explanation
Question 71
A 33-year-old man undergoes a successful closed reduction of a traumatic posterior hip dislocation. The post-reduction CT scan demonstrates a congruent hip joint without intra-articular step-off, but reveals a 2 mm osteochondral fragment in the inferior, dependent aspect of the joint. The patient has a full, unrestricted range of motion. What is the most appropriate management?
Explanation
Question 72
An 82-year-old woman with osteoporosis sustains a displaced femoral neck fracture. The surgeon elects to perform a hemiarthroplasty. Compared to an uncemented stem, what is a well-documented advantage of using a cemented femoral stem in this patient?
Explanation
Question 73
A 24-year-old man is brought to the OR with an irreducible posterior hip dislocation after closed reduction attempts in the emergency department and under general anesthesia fail. What is the most common anatomic structure preventing closed reduction in this scenario?
Explanation
Question 74
Which of the following intraoperative factors is most predictive of failure (nonunion or loss of fixation) after closed reduction and percutaneous pinning of a displaced femoral neck fracture in a young adult?
Explanation
Question 75
A 45-year-old woman sustained a posterior hip dislocation with an associated posterior wall acetabulum fracture. After closed reduction, she is taken for dynamic fluoroscopic stress testing. Which specific maneuver is most appropriate to evaluate for posterior hip instability that would necessitate open reduction and internal fixation of the posterior wall?
Explanation
Question 76
An 80-year-old woman with end-stage dementia who is chronically bedbound presents with a closed, displaced femoral neck fracture after rolling out of bed. The family requests the least invasive approach focused solely on pain control. What is an acceptable orthopedic management strategy for this specific patient profile?
Explanation
Question 77
Which of the following fracture patterns is widely considered an absolute contraindication to the use of a standard sliding hip screw (DHS) for definitive fixation?
Explanation
Question 78
A 35-year-old man sustains a subtrochanteric femur fracture following a high-speed motorcycle collision. Which of the following describes the characteristic position of the proximal fracture fragment secondary to the muscular deforming forces?
Explanation
Question 79
When treating an intertrochanteric femur fracture with a sliding hip screw, the tip-apex distance (TAD) is measured to assess the adequacy of lag screw placement. A TAD greater than what threshold value is associated with a significantly increased risk of lag screw cut-out?
Explanation
Question 80
A 28-year-old restrained driver presents after a motor vehicle collision with a posterior hip dislocation. Which neurologic deficit is most commonly associated with this specific injury?
Explanation
Question 81
A 40-year-old man presents with a posterior hip dislocation and an associated femoral head fracture located cephalad to the fovea capitis. According to the Pipkin classification, what type of fracture does this represent?
Explanation
Question 82
A 22-year-old skier crashes and sustains an inferior anterior hip dislocation. On physical examination in the emergency department, his affected lower extremity is classically positioned in:
Explanation
Question 83
A 72-year-old woman sustains a reverse obliquity intertrochanteric femur fracture. Which of the following fixation constructs is biomechanically most appropriate for this specific fracture pattern?
Explanation
Question 84
When evaluating an intertrochanteric fracture for surgical fixation, the lateral wall thickness is a critical factor. Below what threshold of intact lateral wall thickness is the fracture considered highly unstable, thus increasing the failure risk of a standard sliding hip screw?
Explanation
Question 85
In a 30-year-old patient with an acute, displaced, transcervical femoral neck fracture, what is the most appropriate surgical management?
Explanation
Question 86
During a posterior approach to the hip for a displaced femoral neck fracture, care must be taken to protect the primary blood supply to the femoral head. Which artery provides the majority of the blood supply to the adult femoral head?
Explanation
Question 87
A 68-year-old woman on long-term bisphosphonate therapy presents with weeks of vague anterior thigh pain, followed by an acute inability to bear weight. Radiographs show a transverse subtrochanteric fracture with lateral cortical thickening. What is the underlying mechanism of this atypical fracture?
Explanation
Question 88
A 25-year-old man presents with a posterior hip dislocation after a high-speed collision. Closed reduction under conscious sedation in the emergency department is unsuccessful. A CT scan demonstrates an empty acetabulum with no large bony fragments. What is the most likely soft-tissue structure blocking closed reduction?
Explanation
Question 89
A 75-year-old man presents with groin pain after a fall. Imaging demonstrates a basicervical femoral neck fracture. Which of the following best describes the biomechanical characteristics and optimal fixation of this fracture pattern compared to a transcervical fracture?

Explanation
Question 90
A healthy, community-ambulating 70-year-old woman sustains a displaced femoral neck fracture. When comparing total hip arthroplasty (THA) to bipolar hemiarthroplasty for her definitive treatment, THA is associated with:
Explanation
Question 91
When performing closed reduction and percutaneous pinning for a nondisplaced femoral neck fracture in an adult, what is the biomechanically optimal configuration for the three cannulated screws?
Explanation
Question 92
A 6-year-old boy sustains a traumatic posterior hip dislocation following a low-energy fall from a playground structure. Reduction is performed urgently under conscious sedation. Which of the following best describes the prognosis and management regarding avascular necrosis (AVN) in this pediatric patient?
Explanation
None
