Wrist Arthrodesis and Arthroplasty: Advanced Surgical Techniques

Key Takeaway
Wrist arthrodesis and arthroplasty are cornerstone reconstructive procedures for debilitating wrist arthritis. While arthrodesis provides definitive pain relief and stability, arthroplasty preserves functional motion. Procedure selection depends on bone stock, extensor tendon integrity, and patient demands. This guide details the biomechanical principles, surgical approaches, and implant considerations required to optimize outcomes in both rheumatoid and osteoarthritic patients, ensuring durable, pain-free wrist function and improved quality of life.
Comprehensive Introduction and Patho-Epidemiology
The reconstructive procedures available for the management of an arthritic wrist joint represent a complex, highly nuanced biomechanical compromise between the preservation of functional motion and the provision of absolute structural stability. The primary surgical options in the modern orthopedic armamentarium include partial carpal arthrodesis, total wrist arthrodesis (TWA), and total wrist arthroplasty (TWAp). The decision-making matrix for these procedures is heavily influenced by the underlying pathology, which most commonly includes rheumatoid arthritis (RA), primary osteoarthritis (OA), and post-traumatic arthritic conditions such as scapholunate advanced collapse (SLAC) or scaphoid nonunion advanced collapse (SNAC). Understanding the patho-epidemiology of these conditions is paramount for the treating orthopedic surgeon, as the natural history of the disease dictates both the timing and the nature of the surgical intervention.
Rheumatoid arthritis historically constituted the vast majority of indications for both total wrist arthrodesis and arthroplasty. The pathogenesis in RA is driven by an aggressive, proliferative synovitis that systematically destroys the extrinsic and intrinsic ligamentous restraints of the radiocarpal and midcarpal joints. This capsuloligamentous attenuation inevitably leads to the classic rheumatoid deformities: ulnar translation of the carpus, volar subluxation, and supination of the carpus relative to the distal radius, often accompanied by a reciprocal radial deviation of the metacarpals. The resultant biomechanical disadvantage places immense stress on the extensor tendons, frequently leading to attritional ruptures (Vaughan-Jackson syndrome) over prominent ulnar head osteophytes or the distal radius. While the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic agents has dramatically altered the epidemiological landscape—reducing the incidence of end-stage rheumatoid wrist destruction—there remains a substantial cohort of patients who present with medically recalcitrant, end-stage pancarpal arthritis requiring definitive surgical reconstruction.
Conversely, post-traumatic osteoarthritis follows a predictable, kinematic progression of degenerative changes. In the SLAC wrist, the dissociation of the scapholunate ligament disrupts the synchronous motion of the proximal carpal row. The scaphoid flexes, while the lunate extends (DISI deformity), fundamentally altering the contact mechanics at the radioscaphoid articulation. Degenerative changes predictably begin at the radial styloid, progress to the entire radioscaphoid fossa, and subsequently involve the capitolunate joint, characteristically sparing the radiolunate articulation until the absolute terminal stages of the disease. SNAC wrists follow a similar topographical progression of cartilage degradation. For these post-traumatic etiologies, the surgical algorithm often favors motion-preserving partial arthrodeses (e.g., four-corner fusion, proximal row carpectomy) in the earlier stages. However, once pancarpal arthritis ensues, the surgeon must choose between the absolute stability of a total wrist arthrodesis and the motion-preserving, yet complication-prone, total wrist arthroplasty.
Whether wrist arthrodesis or arthroplasty is the superior choice remains a subject of vigorous academic debate. Each procedure has distinct, evidence-based applications. Retention of wrist motion is highly desirable for activities of daily living (ADLs), particularly perineal care, feeding, and fine motor tasks. However, wrist arthroplasty historically carries a higher percentage of late complications, such as aseptic loosening, subsidence, and polyethylene wear, compared to arthrodesis. Conversely, arthrodesis provides a reliably painless, durable, and stable wrist once solid osseous fusion is achieved, though at the absolute cost of radiocarpal and midcarpal kinematics. In patients with bilateral incapacitating wrist arthritis, a hybrid approach is often the most functional solution. Arthrodesing one wrist provides a stable pillar (crucial if the patient requires crutches or a platform walker), while performing an arthroplasty on the contralateral wrist preserves the motion necessary for essential personal hygiene and dexterity.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Kinematics
The human wrist is an elegantly complex articulation comprising the distal radius, the distal ulna, and eight carpal bones arranged dynamically into proximal and distal rows. The proximal carpal row (scaphoid, lunate, triquetrum) functions as an intercalated segment; it possesses no direct tendinous insertions and its motion is entirely dictated by the mechanical forces exerted by the surrounding articular contour and ligamentous tethering. The distal carpal row (trapezium, trapezoid, capitate, hamate) is tightly bound by robust interosseous ligaments and functions as a single kinematic unit that moves synchronously with the metacarpals. Normal wrist motion occurs through a combination of radiocarpal and midcarpal articulations. Biomechanically, the radiocarpal joint is responsible for approximately 40% of flexion and 60% of extension, whereas the midcarpal joint contributes 60% of flexion and 40% of extension.
Crucially, functional wrist kinematics do not occur in pure orthogonal planes (flexion/extension or radial/ulnar deviation). Instead, the predominant axis of functional movement operates obliquely along the "dart-thrower's arc"—a coupled motion moving from radial deviation and extension to ulnar deviation and flexion. This arc predominantly utilizes the midcarpal joint, specifically the capitolunate articulation, while the scaphoid and lunate remain relatively stationary. This anatomical reality forms the biomechanical rationale for partial wrist arthrodeses, such as the radiolunate fusion, which stabilizes the ulnar-translating rheumatoid carpus while preserving the dart-thrower's motion at the midcarpal joint.
Load Transmission and Ligamentous Anatomy
Axial load transmission across the wrist is distributed asymmetrically. In a neutral, ulnar-variance-zero wrist, approximately 80% of the axial load is transmitted across the radiocarpal joint (primarily the scaphoid and lunate fossae), and 20% is transmitted across the ulnocarpal joint via the triangular fibrocartilage complex (TFCC). In the setting of carpal collapse or advanced arthritis, this load distribution is radically altered, leading to eccentric loading, rapid cartilage wear, and subchondral cyst formation.
The stability of the carpus relies on a complex network of intrinsic (interosseous) and extrinsic ligaments. The volar extrinsic ligaments are significantly thicker and stronger than their dorsal counterparts. The radioscaphocapitate (RSC), long radiolunate (LRL), and short radiolunate (SRL) ligaments provide the primary volar restraint against ulnar and volar translation of the carpus. In rheumatoid arthritis, the hypertrophic synovitis selectively targets these volar capsuloligamentous structures, leading to the characteristic volar-ulnar subluxation of the carpus. Dorsally, the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments form a critical "V" shaped stabilizing complex. Surgical approaches to the wrist, whether for arthrodesis or arthroplasty, must meticulously respect or meticulously reconstruct these ligamentous restraints. In total wrist arthroplasty, failure to adequately balance the soft tissues and restore the anatomical center of rotation inevitably leads to eccentric loading of the polyethylene bearing, accelerating wear and precipitating catastrophic aseptic loosening.
Exhaustive Indications and Contraindications
The selection of the appropriate surgical intervention for end-stage wrist arthritis demands a rigorous, individualized assessment of the patient's functional demands, bone stock, soft-tissue envelope, and systemic health. The decision matrix is rarely absolute and requires a thorough preoperative discussion regarding the trade-offs between motion preservation and long-term durability.
Most orthopedic authors and hand surgeons consider Total Wrist Arthrodesis (TWA) the gold standard and procedure of choice for high-demand patients. This includes manual laborers, young patients with post-traumatic arthritis, and individuals with profound neurological deficits (e.g., cerebral palsy, brachial plexus injuries) requiring rigid stabilization to facilitate hand function. TWA is also strictly indicated in the presence of marked, uncorrectable flexion deformities of the wrist and fingers, chronic carpal dislocation, or severe subluxation that cannot be anatomically reduced. Furthermore, painful wrists associated with multiple extensor tendon ruptures necessitate arthrodesis. This is especially critical for attritional ruptures of the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB), as these muscles are absolute prerequisites for the dynamic wrist balance required for a successful arthroplasty.
Total Wrist Arthroplasty (TWAp), conversely, is generally reserved for low-demand patients. The ideal candidate is an older individual with rheumatoid arthritis or low-demand osteoarthritis, who possesses adequate bone stock, intact wrist extensors, and a strong desire to maintain functional wrist motion for activities of daily living. Modern third-generation implants have expanded the indications slightly, but the fundamental prerequisite of a compliant, low-demand patient remains unchanged. A functional, stable distal radioulnar joint (DRUJ) or a planned concurrent DRUJ reconstruction (e.g., Darrach procedure or Sauvé-Kapandji) is also necessary, as DRUJ pathology will profoundly compromise the outcomes of wrist arthroplasty.
According to the seminal works of Carlson, Simmons, and Beckenbaugh, there are strict absolute and relative contraindications to total wrist arthroplasty that the surgeon must heed to avoid catastrophic failure.
| Parameter | Total Wrist Arthrodesis (TWA) | Total Wrist Arthroplasty (TWAp) |
|---|---|---|
| Primary Indications | High-demand patients (laborers, heavy lifters); Post-traumatic pancarpal arthritis; Failed partial fusions; Paralytic deformities. | Low-demand patients (elderly, sedentary); Rheumatoid arthritis with preserved bone stock; Bilateral disease (hybrid approach). |
| Soft Tissue Prerequisites | Can be performed in the setting of severe extensor tendon loss or profound soft-tissue compromise. | REQUIRES intact or reconstructable ECRL/ECRB; Requires competent soft-tissue envelope for balancing. |
| Bone Stock Requirements | Can tolerate significant bone loss (utilizing structural autograft/allograft and spanning plates). | REQUIRES adequate distal radial and carpal/metacarpal bone stock for component fixation and to prevent subsidence. |
| Absolute Contraindications | Active deep space infection; Amputation of the hand (relative). | Active infection; High-demand occupation/hobbies; Absent wrist extensors; Dependence on platform walkers/crutches (axial loading). |
| Relative Contraindications | Contralateral wrist arthrodesis (severely limits perineal care); Severe osteopenia (complicates hardware purchase). | Severe osteopenia; Uncorrectable carpal subluxation; History of prior deep joint infection; Poor patient compliance. |
Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Evaluation and Advanced Imaging
Meticulous preoperative planning is the cornerstone of successful wrist reconstruction. Standard radiographic evaluation must include zero-rotation posteroanterior (PA), true lateral, and oblique views of the wrist. On the PA radiograph, the surgeon must assess the degree of carpal collapse, ulnar translation, and the integrity of the radiocarpal and midcarpal joint spaces. The ulnar variance should be noted, as concurrent DRUJ pathology frequently requires addressing. On the lateral radiograph, the alignment of the capitate relative to the longitudinal axis of the radius is evaluated to determine the degree of dorsal or volar intercalated segment instability (DISI/VISI) or global subluxation.
For patients under consideration for total wrist arthroplasty, advanced imaging with computed tomography (CT) is highly recommended. CT provides a three-dimensional assessment of the distal radial bone stock and the volume of the carpal bones (specifically the capitate and third metacarpal), which is critical for determining whether the patient can support the distal component of the prosthesis. Severe cystic changes or profound osteopenia visualized on CT may prompt the surgeon to abandon arthroplasty in favor of arthrodesis.
Digital Templating and The Position of Fusion
Digital templating is mandatory for TWAp to determine the appropriate size of the radial and carpal components. The goal is to restore the anatomical center of rotation, which typically lies within the head of the capitate. Oversizing the radial component can lead to impingement and restricted motion, while undersizing can lead to subsidence.
For Total Wrist Arthrodesis, preoperative planning involves determining the optimal angle of fusion. The optimal position in which to fuse the wrist for maximal function remains controversial and must be tailored to the individual patient's anatomy and occupational needs. Historically, 10 to 30 degrees of dorsiflexion was favored to maximize the biomechanical advantage of the extrinsic flexor tendons, thereby optimizing grip strength. However, modern consensus increasingly prefers a neutral position—alignment of the axis of the third metacarpal coaxial with the axis of the radius in the lateral radiographic projection. This neutral alignment is particularly crucial if bilateral wrist fusions are planned, as it facilitates perineal care, feeding, and keyboard use.
A critical surgical warning must be heeded regarding bilateral arthrodeses: usually, both wrists should not be fused in extension. Fusing both wrists in extension makes it biomechanically impossible for the patient to reach their perineum, severely compromising personal hygiene. If bilateral fusions are mandatory, the surgeon should place the dominant wrist in slight extension (to maximize power grip) and the non-dominant wrist in slight flexion or neutral (to facilitate hygiene and ADLs).
Patient Positioning and Preparation
The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (brachial plexus block) is generally preferred, often supplemented with general anesthesia depending on patient comfort and the anticipated duration of the procedure. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation. The entire upper extremity, from the fingertips to the axilla, is prepped and draped in a standard sterile fashion. If autologous bone grafting from the iliac crest is anticipated for an arthrodesis, the ipsilateral hip is simultaneously prepped and draped.
Step-by-Step Surgical Approach and Fixation Technique
Volar Decompression and Synovectomy
In many rheumatoid patients, severe volar synovitis, flexor tendon compromise, and median nerve compression necessitate a comprehensive volar approach prior to, or in conjunction with, dorsal reconstructive procedures.
- Incision and Fascial Release: Make a longitudinal or slightly zig-zag volar incision, ending approximately 7.5 cm proximal to the wrist crease. Open the deep antebrachial fascia proximally and identify the median nerve.
- Nerve Protection: Stay strictly on the ulnar side of the median nerve during the dissection. Meticulously protect the palmar cutaneous branch (which branches radially proximal to the wrist crease) and the recurrent motor branch of the median nerve in the palm.
- Ligament Division: Divide the deep transverse carpal ligament to expose the flexor tendons within the carpal tunnel. Note that its distal border extends further distally into the palm than is usually realized; complete release is mandatory.
- Tenosynovectomy: Beginning proximally and proceeding distally—while keeping constantly in mind the location of the median nerve—dissect the hypertrophic, invasive synovium from each individual flexor tendon. Evaluate all flexor tendons for attritional ruptures, fraying, and erosions.
- Capsular Inspection and Osteophyte Excision: Retract the flexor tendons and inspect the volar capsule and ligaments over the carpal bones. Look for eroded areas caused by prominent osteophytes, particularly on the volar pole of the scaphoid or the prominent volar lip of the radius. Remove these osteophytes with a rongeur or high-speed burr to prevent future flexor tendon rupture.
- Closure: Close the capsule-ligament layer over the carpal bones to provide a smooth gliding surface for the flexor tendons. Do not close the deep transverse carpal ligament.
- Hemostasis and Splinting: Release the tourniquet, obtain meticulous hemostasis using bipolar electrocautery, insert a closed-suction drain, and close the skin. Apply a bulky compression dressing and a volar plaster splint from the proximal forearm to the distal palmar crease.
Total Wrist Arthroplasty (TWAp): Implant Evolution and Technique
The landscape of wrist arthroplasty has evolved significantly from early, high-failure silicone spacers to modern, semi-constrained, anatomically designed implants. Adequate muscle balance and correctable wrist contractures are paramount requirements for any implant to be successful.
The Meuli III Prosthesis
Fernandez reported excellent early results in wrists treated for rheumatoid or traumatic arthritis with the Meuli III wrist prosthesis. This implant utilizes a ball-and-socket design, attempting to replicate the universal joint motion of the normal carpus. Despite excellent early functional results and pain relief, aseptic loosening occurred at an unacceptably high rate in long-term follow-up, highlighting the biomechanical challenges of unconstrained designs in the wrist subjected to shear forces.
Correctly implanted Meuli III wrist prosthesis in a 55-year-old woman with rheumatoid arthritis. Note the reconstruction of carpal height and axial alignment. The prosthesis is firmly fixed in carpal bone stock with no palmar protrusion.
The Biaxial Total Wrist Implant
To address the shortcomings of earlier unconstrained designs, Beckenbaugh and Linscheid developed the semi-constrained "biaxial" wrist implant. It features an ellipsoidal articulation and a porous coating to improve cementless biological fixation or to enhance the cement-bone interface. Rettig and Beckenbaugh evaluated the use of the biaxial implant as a salvage procedure for failed total wrist arthroplasties, such as fractured Swanson Silastic implants. Although clinical improvement was achieved, loosening remained a persistent problem, especially in patients with aggressive rheumatoid disease. Takwale et al. found that out of 66 biaxial wrist replacements reviewed at an average of 52 months, five required revisions, yielding an 8-year survivorship probability of 83%.

Fracture of a Swanson Silastic implant (Preoperative radiographs) salvaged two years later with a biaxial total wrist arthroplasty.
The Universal Total Wrist Arthroplasty
Modern designs, such as the Universal total wrist implant, have shown highly promising results in early and mid-term cohorts of patients with rheumatoid arthritis, as reported by Menon, Divelbiss, Sollerman, and Adams. These implants focus on anatomical center-of-rotation matching, minimal bone resection, and modularity. The radial component is typically a titanium alloy with a polyethylene articulating surface, while the carpal component is fixed via a central peg into the capitate and screws into the surrounding carpus.
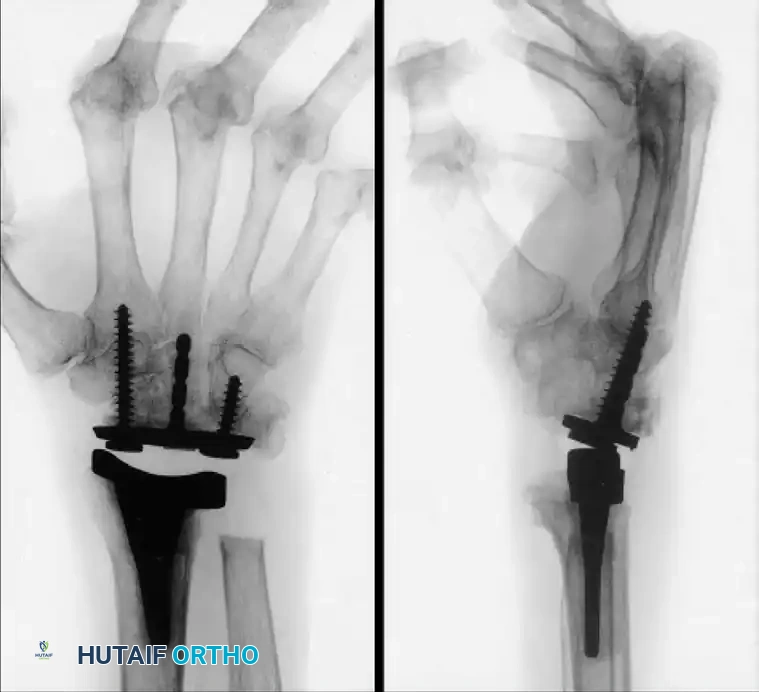
Long-standing rheumatoid disease and symptomatic wrist arthritis treated with a Universal total wrist arthroplasty, demonstrating excellent alignment and preservation of carpal height two years postoperatively.
The surgical technique for the Universal implant involves a dorsal longitudinal incision. The third extensor compartment is opened, and the EPL is transposed. A distally based capsular flap is elevated. The distal radius is resected perpendicular to its long axis. The proximal row of carpal bones (scaphoid, lunate, triquetrum) is excised. The capitate is prepared to receive the central stem of the carpal component. Trial components are inserted, and the wrist is taken through a full range of motion to assess stability, impingement, and soft-tissue tension. Once optimal sizing is confirmed, the definitive implants are impacted (with or without cement, depending on bone quality), and the dorsal capsule is meticulously repaired to prevent dorsal subluxation.
Total Wrist Arthrodesis (TWA): Surgical Techniques
Successful wrist arthrodesis reliably relieves pain, corrects deformity, and maintains absolute stability. Modern techniques almost exclusively utilize robust internal fixation via dorsal spanning plates and autologous bone grafting.
- Incision and Exposure: A longitudinal dorsal incision is made centered over Lister's tubercle, extending from the distal third of the radius to the midshaft of the third metacarpal.
- Extensor Retinaculum: The third extensor compartment is opened, and the extensor pollicis longus (EPL) is transposed radially. The second and fourth compartments are elevated subperiosteally. The dorsal radiocarpal ligaments and capsule are excised to expose the radiocarpal and midcarpal joints.
- Joint Preparation: The articular cartilage of the radiocarpal joint, midcarpal joint, and the carpometacarpal (CMC) joint of the third ray is meticulously denuded down to bleeding subchondral bone using a high-speed burr, curettes, or osteotomes. It is critical to preserve the contour of the bones to maximize the surface area for fusion.
- Bone Grafting: Cancellous bone graft (harvested from the distal radius, proximal ulna, or iliac crest) is densely packed into the decorticated spaces to promote osteogenesis.
- Fixation: A specialized pre-contoured dorsal wrist fusion plate (e.g., AO dynamic compression plate or a locking wrist fusion plate) is applied. The plate is secured proximally to the radial shaft and distally to the third metacarpal. The surgeon must ensure the wrist is positioned in the pre-planned degree of extension or neutral alignment before final tightening. Compression is applied across the carpus.
- Closure: The extensor retinaculum is repaired over the plate to protect the extensor tendons from hardware irritation, leaving the EPL transposed in the subcutaneous tissue. The skin is closed over a suction drain.
Partial Wrist Arthrodesis: The Radiolunate (Chamay) Fusion
Partial arthrodesis is highly useful to preserve motion in relatively uninvolved joints while stabilizing the wrist against pathological translation. Radiocarpal fusions are indicated when the midcarpal joint is spared. The Radiolunate (Chamay) Fusion is particularly effective for isolated radiolunate arthritis or to halt ulnar slide in the rheumatoid wrist while preserving the midcarpal articulation (capitolunate joint) for flexion and extension.


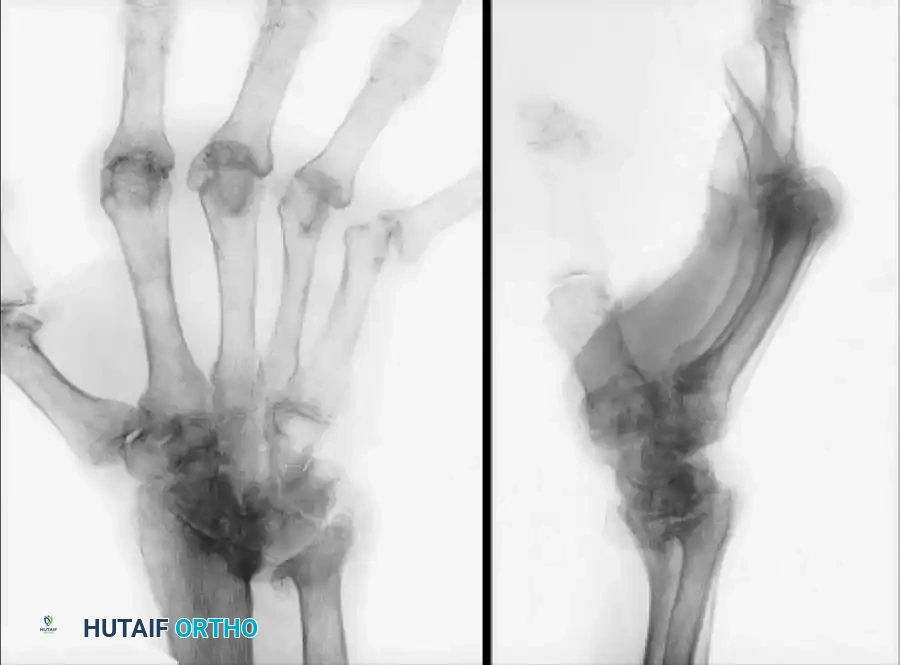
Ulnar subluxation in a 54-year-old woman with rheumatoid arthritis (Left), successfully stabilized and realigned after a radiolunate (Chamay) fusion (Right).
By fusing only the affected radiocarpal segment, the surgeon maintains the kinematic dart-thrower's motion arc, which is essential for many occupational and daily activities. The procedure involves a limited dorsal approach, decortication of the radiolunate articulation, and fixation typically utilizing headless compression screws or a low-profile dorsal plate.
Complications, Incidence Rates, and Salvage Management
The reconstructive wrist surgeon must be acutely aware of the potential complications associated with both arthrodesis and arthroplasty. Despite rigorous patient selection and meticulous surgical technique, complications occur and require decisive management.
| Complication | Procedure | Estimated Incidence | Etiology and Salvage Management |
|---|---|---|---|
| Aseptic Loosening | TWAp | 10% - 25% (at 10 years) | Driven by particulate wear debris (osteolysis) or eccentric loading due to soft-tissue imbalance. Salvage: Revision arthroplasty (if bone stock permits) or conversion to Total Wrist Arthrodesis with structural bone grafting. |
| Subsidence | TWAp | 5% - 15% | Failure of the distal component to find adequate cortical support in the capitate/metacarpals, common in severe RA osteopenia. Salvage: Conversion to TWA. |
| Symptomatic Hardware | TWA | 10% - 30% | Prominence of the dorsal fusion plate causing extensor tendon tenosynovitis or rupture. Salvage: Hardware removal after solid osseous union is confirmed via CT scan. |
| Nonunion / Pseudarthrosis | TWA | 2% - 5% | Inadequate decortication, insufficient bone graft, or failure of rigid fixation. Higher risk in smokers. Salvage: Revision osteosynthesis with iliac crest bone grafting and rigid locking plate fixation. |
| Periprosthetic Fracture | TWAp | 1% - 3% | Intraoperative fracture during stem impaction or postoperative trauma. Salvage: Open reduction internal fixation (ORIF) with spanning plates, or bypass with a longer revision stem. |
| Deep Space Infection | Both | 1% - 3% | Immunosuppression (RA biologics), poor soft-tissue envelope. Salvage: Aggressive I&D, hardware/implant removal, antibiotic spacer placement, and eventual definitive arthrodesis once infection is cleared. |
A critical pitfall in wrist arthroplasty is the failure to recognize an impending catastrophic failure. Regular radiographic surveillance is mandatory. Despite implant modifications, careful patient selection, close attention to meticulous surgical technique (especially soft-tissue balancing), and thoughtful consideration of salvage options (i.e., conversion to arthrodesis) are absolutely critical when implant arthroplasty is considered for a patient with incapacitating wrist arthritis.
Phased Post-Operative Rehabilitation Protocols
Arthrodesis Rehabilitation Protocol
The primary goal following a total wrist arthrodesis is to protect the osseous construct until solid clinical and radiographic union is achieved, while simultaneously preventing stiffness in the adjacent, non-fused articulations (digits, elbow, shoulder).
- Phase I (Weeks 0-2): Immediately postoperatively, the wrist is immobilized in a bulky, compressive dressing and a rigid volar plaster splint. Elevation is strictly enforced to minimize edema. Active range of motion (ROM) of the metacarpophalangeal (MCP) and interphalangeal (IP) joints is initiated immediately to prevent flexor and extensor tendon adhesions.
- Phase II (Weeks 2-6): At the first postoperative visit (10-14 days), sutures are removed. The patient is transitioned to a short-arm cast or a rigid, custom-molded thermoplastic splint. If the distal radioulnar joint (DRUJ) was not surgically addressed and is stable, gentle active forearm rotation (pronation/supination) is permitted.
- Phase III (Weeks 6-12): Radiographs are obtained at 6 weeks to assess early trabecular bridging. If clinical stability is apparent, the patient may begin weaning from the splint during sedentary activities.
- Phase IV (Months 3+): Clinical and radiographic union is typically definitively observed between 8 and 12 weeks. Once union is confirmed by the operating surgeon, all immobilization is discontinued, and progressive strengthening exercises for grip and forearm musculature commence.
Arthroplasty Rehabilitation Protocol
Rehabilitation following total wrist arthroplasty is a delicate balance between protecting the soft-tissue capsular repair and initiating early motion to maximize the functional kinematic arc of the prosthesis.
- Phase I (Weeks 0-2): The wrist is placed in a bulky dressing and volar splint in neutral alignment to protect the dorsal capsular repair. Absolute elevation and immediate digital ROM are instituted.
- Phase II (Weeks 2-6): At 10 to 14 days, sutures are removed, and a custom thermoplastic splint is fabricated holding the wrist in
