Comprehensive Guide to Carpal Instability and Wrist Arthrodesis
Key Takeaway
Carpal instability encompasses a complex spectrum of ligamentous injuries, ranging from scapholunate dissociation to progressive perilunar dislocations. Accurate diagnosis relies on understanding carpal kinematics, recognizing radiographic patterns like DISI and VISI, and performing provocative clinical maneuvers such as the Watson shift test. Surgical management dictates precise anatomical reduction, rigid internal fixation, and robust ligamentous reconstruction to restore carpal alignment and prevent progressive radiocarpal arthrosis.
Comprehensive Introduction and Patho-Epidemiology
The human wrist is an incredibly complex, multi-articulated biomechanical engine that must simultaneously provide a vast arc of motion while maintaining the structural rigidity necessary for powerful grip and load transfer. End-stage carpal instability, neglected perilunate dislocations, and advanced radiocarpal arthrosis represent a continuum of catastrophic mechanical failures within this intricate system. These conditions often necessitate salvage procedures, such as total wrist arthrodesis, to provide a stable, pain-free wrist for patients who have exhausted all joint-preserving options. The modern understanding of these pathologies has evolved dramatically over the past century, transitioning from a simplistic view of the wrist as a generic hinge joint to a highly nuanced appreciation of its complex kinematics and ligamentous dependencies.
Carpal instability fundamentally represents a failure of the capsuloligamentous constraints to maintain normal articular alignment under physiological loads. The true incidence of carpal instability is likely underreported, as many acute injuries are initially misdiagnosed as simple sprains. High-energy trauma, such as falls from a height or motor vehicle collisions, frequently precipitates these injuries, particularly in young, active demographics. When these ligamentous disruptions are missed or inadequately treated, the uncoupling of the carpal bones leads to altered contact mechanics, focal cartilaginous overload, and the inevitable progression to predictable patterns of degenerative arthritis, most notably the Scapholunate Advanced Collapse (SLAC) or Scaphoid Nonunion Advanced Collapse (SNAC) wrist.
The socioeconomic impact of progressive carpal instability and subsequent pan-carpal arthritis is profound. Patients often present with debilitating pain, profound weakness, and a significant loss of vocational capacity, particularly those engaged in heavy manual labor. While motion-preserving salvage procedures, such as proximal row carpectomy (PRC) or four-corner arthrodesis (4CA), are viable for intermediate stages of arthritis, they are contraindicated in the presence of global radiocarpal and midcarpal destruction. In these advanced scenarios, total wrist arthrodesis remains the undisputed gold standard. It offers unparalleled predictability in pain relief and functional restoration of grip strength, allowing high-demand patients to return to heavy lifting and rigorous activities.
Detailed Surgical Anatomy and Biomechanics
Osseous Architecture and the Intercalated Segment
The structural foundation of the wrist relies on the unique geometric configuration of the proximal and distal carpal rows. The distal carpal row (trapezium, trapezoid, capitate, and hamate) functions as a rigid, tightly bound unit that moves synchronously with the metacarpals. The capitate serves as the keystone of this distal arch, articulating proximally with the scaphoid and lunate. In stark contrast, the proximal carpal row (scaphoid, lunate, and triquetrum) is a highly mobile intercalated segment. It lacks any direct tendinous insertions, meaning its spatial orientation is entirely dictated by the mechanical forces exerted upon it by the surrounding articular contours and the restraining forces of the intrinsic and extrinsic ligaments.
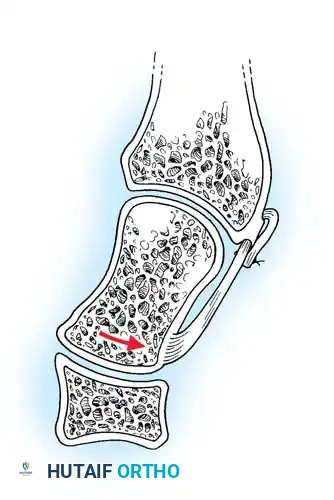
The scaphoid, bridging the proximal and distal rows, has an inherent biomechanical tendency to palmar-flex under axial loading due to its oblique orientation and the compressive forces from the trapezium and trapezoid. Conversely, the triquetrum, driven by the helicoidal shape of the hamate articular surface, has a natural tendency to dorsiflex and translate ulnarly. The lunate sits precariously between these two opposing forces. When the intrinsic ligamentous tethers (the scapholunate and lunotriquetral ligaments) are intact, the lunate balances these forces, maintaining a neutral posture. The disruption of these tethers uncouples the proximal row, allowing the individual carpal bones to follow their inherent, unresisted biomechanical trajectories, resulting in profound kinematic collapse.
Intrinsic and Extrinsic Ligamentous Complexes
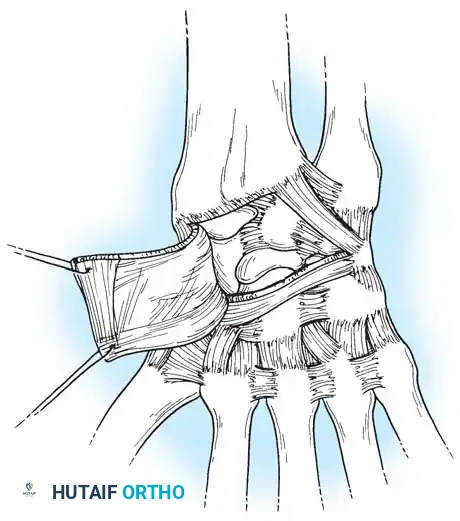
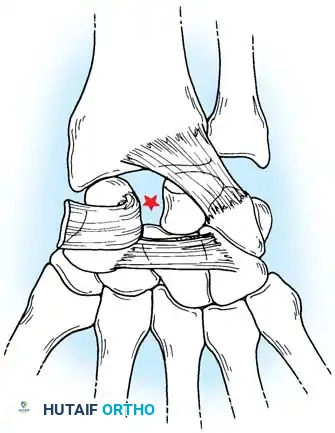
The stability of the carpus is governed by a robust network of intrinsic and extrinsic ligaments. The intrinsic ligaments connect adjacent carpal bones within the same row. The most critical of these is the scapholunate interosseous ligament (SLIL), a C-shaped structure divided into dorsal, membranous (proximal), and volar regions. The dorsal region of the SLIL is the thickest and most biomechanically critical component, composed of stout, transversely oriented collagen fibers that resist the primary translational and rotational forces between the scaphoid and lunate. The lunotriquetral interosseous ligament (LTIL) is similarly structured, but its volar component is the thickest and most critical for stability, resisting the natural dorsiflexion of the triquetrum.
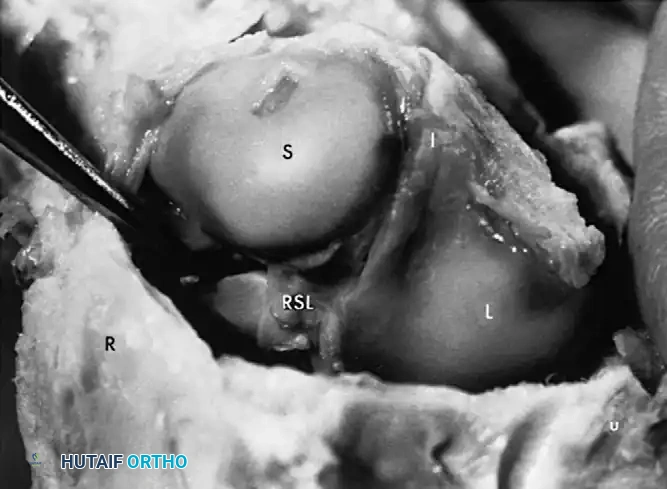
The extrinsic ligaments bridge the radius or ulna to the carpus, or span across the midcarpal joint. The palmar extrinsic ligaments are substantially thicker and stronger than their dorsal counterparts, forming a double-V configuration that converges on the lunate and capitate. The radioscaphocapitate (RSC) ligament acts as a critical sling supporting the scaphoid waist, while the long radiolunate (LRL) and short radiolunate (SRL) ligaments tether the lunate to the radius. Between the RSC and LRL lies the radioscapholunate (RSL) ligament, or ligament of Testut, which is predominantly a neurovascular conduit rather than a true mechanical restraint. On the dorsal side, the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments form a horizontal V-shape, providing vital secondary stabilization against volar translation and carpal supination.
Pathokinematics of Carpal Instability
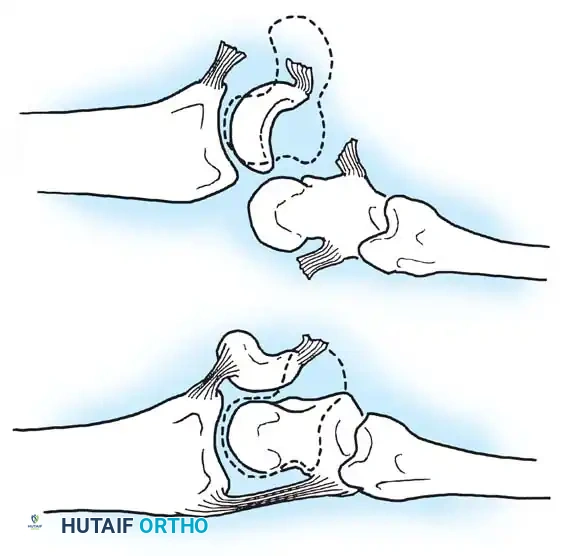
Carpal instability is broadly classified by the Dobyns and Cooney system into Carpal Instability Dissociative (CID), Carpal Instability Nondissociative (CIND), Carpal Instability Combined (CIC), and Adaptive Carpus. CID involves disruptions within a single carpal row, most commonly the proximal row. When the SLIL ruptures, the scaphoid palmar-flexes independently, while the lunate, now tethered only to the triquetrum via the intact LTIL, follows the triquetrum into profound dorsiflexion. This uncoupling produces the classic Dorsal Intercalated Segment Instability (DISI) deformity. Conversely, if the LTIL ruptures, the lunate remains tethered to the flexing scaphoid, resulting in a Volar Intercalated Segment Instability (VISI) deformity.
Progressive perilunar instability, as famously described by Mayfield, Johnson, and Kilcoyne, outlines the sequential failure of these ligaments under extreme loading (typically forced hyperextension, ulnar deviation, and intercarpal supination). Stage I involves SLIL and RSC rupture (scapholunate dissociation). As the energy propagates ulnarly, Stage II disrupts the space of Poirier, allowing the capitate to subluxate dorsally. Stage III involves LTIL rupture, leading to a dorsal perilunate dislocation. Finally, Stage IV represents the catastrophic failure of the dorsal radiocarpal ligament, forcing the capitate to drive the lunate volarly into the carpal tunnel, resulting in a frank lunate dislocation. Understanding these distinct pathokinematic stages is critical for both accurate radiographic interpretation and anatomical surgical reconstruction.
Exhaustive Indications and Contraindications
The decision to proceed with a total wrist arthrodesis versus a motion-preserving salvage procedure requires a meticulous assessment of the patient's functional demands, the extent of articular cartilage degradation, and the integrity of the surrounding soft tissue envelope. Total wrist arthrodesis is a definitive, irreversible procedure designed to sacrifice all radiocarpal and midcarpal motion in exchange for absolute stability and the eradication of articular pain. It is the procedure of choice for high-demand patients, heavy laborers, and individuals who require a powerful, pain-free grip for their livelihood.
Indications for total wrist arthrodesis encompass a broad spectrum of end-stage pathologies. The most common indication is advanced SLAC or SNAC wrist (Stage III), where degenerative changes have progressed beyond the radiocarpal joint to involve the capitolunate articulation, rendering limited intercarpal fusions or proximal row carpectomies ineffective. Pan-carpal arthritis secondary to inflammatory arthropathies, such as rheumatoid arthritis, is another frequent indication, particularly when profound carpal collapse, severe ulnar translation, or impending extensor tendon ruptures are present. Additionally, neglected perilunate dislocations, post-traumatic radiocarpal destruction following severe intra-articular distal radius fractures, and salvage of failed partial wrist fusions or failed total wrist arthroplasties strongly warrant total arthrodesis.
Contraindications must be rigorously evaluated to prevent catastrophic surgical failures. Absolute contraindications include active, uncontrolled local or systemic infection, which precludes the implantation of extensive hardware and bone grafting. Inadequate soft tissue coverage, particularly over the dorsal aspect of the wrist, is a critical barrier, as the bulky arthrodesis plate requires robust vascularized tissue to prevent hardware exposure and subsequent deep infection. Relative contraindications include open physes in pediatric patients, where fusion would arrest longitudinal growth, and specific neurological conditions, such as quadriplegia. In quadriplegic patients, preserving wrist mobility is absolutely essential to maintain the tenodesis effect, which allows for passive finger flexion and functional grip when the wrist is extended.
| Parameter | Total Wrist Arthrodesis | Motion-Preserving Salvage (e.g., PRC, 4CA) |
|---|---|---|
| Primary Indications | SLAC/SNAC Stage III, Pan-carpal arthritis, Rheumatoid arthritis with severe collapse, Failed arthroplasty, Heavy manual laborers. | SLAC/SNAC Stage II, Intact capitolunate cartilage (for PRC), Lower functional demands, Desire for preserved motion. |
| Absolute Contraindications | Active infection, Inadequate dorsal soft tissue coverage, Quadriplegia (reliance on tenodesis grip). | Capitolunate arthritis (for PRC), Radioscaphoid arthritis (for 4CA), Inflammatory arthropathy (relative for PRC). |
| Expected Outcomes | Complete loss of radiocarpal/midcarpal motion, Excellent pain relief, High grip strength, High durability. | Preservation of ~50% normal motion, Good pain relief, Decreased grip strength compared to normal, Potential for future degeneration. |
| Complication Profile | Hardware prominence, Nonunion (especially at 3rd CMC), Extensor tendon irritation. | Progressive arthritis, Impingement (radiocapitate in PRC), Nonunion (in 4CA), Hardware failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Provocative Maneuvers
A comprehensive clinical evaluation is the cornerstone of pre-operative planning for any carpal instability or advanced arthritis. The physical examination must meticulously localize the precise origin of the pain, differentiate between intra-articular pathology and extra-articular tendinopathies, and assess the functional status of the surrounding neurovascular structures. In cases of suspected scapholunate dissociation, the Watson scaphoid shift test is paramount. The examiner applies firm pressure to the scaphoid tuberosity while passively moving the wrist from ulnar to radial deviation. In an incompetent SL ligament scenario, the proximal pole of the scaphoid subluxates dorsally out of the radial fossa, producing a painful, palpable clunk as pressure is released.
Furthermore, dynamic instability patterns must be elicited through specific provocative maneuvers. The catch-up clunk is indicative of midcarpal instability; as the wrist is actively moved from radial to ulnar deviation, the proximal row remains abnormally flexed until the extrinsic ligaments suddenly snap taut, forcing the proximal row into extension with a palpable and audible clunk. Lunotriquetral instability is assessed via the LT ballottement test (Shuck test), where the examiner stabilizes the lunate and attempts to translate the triquetrum volarly and dorsally, noting excessive excursion and pain. Grip strength measurements, utilizing a Jamar dynamometer, are critical baseline metrics, as patients with advanced SLAC wrists often exhibit a 50% or greater reduction in grip strength compared to the contralateral limb.
Advanced Imaging and Radiographic Metrics
Radiographic evaluation begins with high-quality, standardized zero-rotation posteroanterior (PA), true lateral, and specific stress views (clenched-fist, radial, and ulnar deviation). On the PA view, the clinician must meticulously trace Gilula’s three radiographic arcs. Disruption of these arcs indicates significant intercarpal malalignment. The Terry Thomas sign—a scapholunate interval exceeding 2 mm (or 3 mm in some literature)—is the classic hallmark of SL dissociation. The cortical ring sign, created by the axially rotated scaphoid presenting its distal pole end-on, further confirms rotary subluxation.
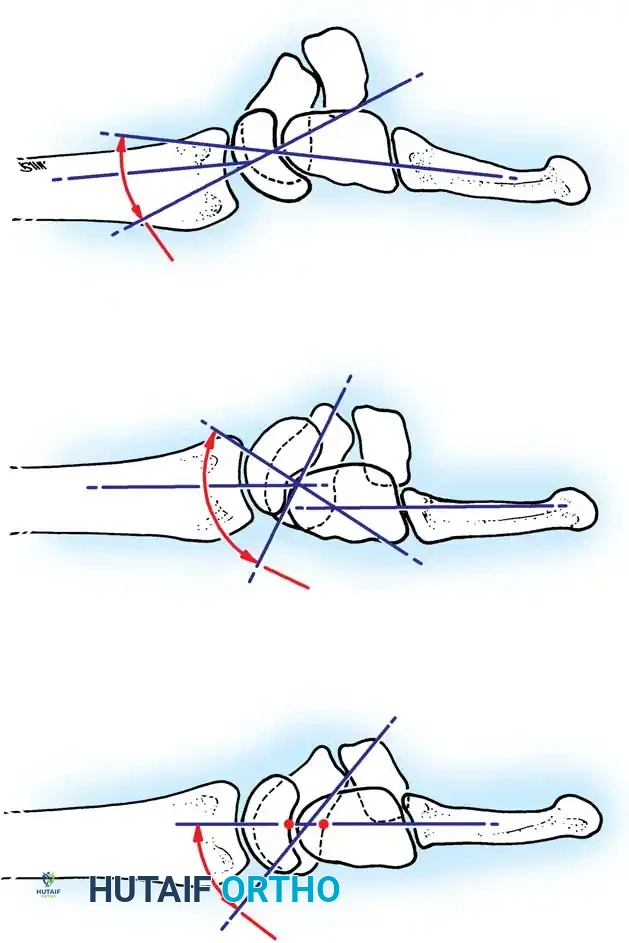
The true lateral radiograph is arguably the most critical imaging modality for assessing carpal collapse. In a normal wrist, the longitudinal axes of the radius, lunate, capitate, and third metacarpal should be collinear. The normal scapholunate angle ranges from 30° to 60° (mean 47°), and the capitolunate angle should be less than 20°. In a DISI deformity, the lunate tilts dorsally, driving the scapholunate angle above 60° (frequently >80°) and the capitolunate angle above 20°. In a VISI deformity, the lunate tilts volarly, resulting in a scapholunate angle of less than 30°. When plain radiographs are equivocal, advanced imaging such as high-resolution MRI or CT arthrography is indicated to evaluate the integrity of the interosseous ligaments and the precise extent of chondral degradation.
Templating and Operating Room Setup
Pre-operative templating is essential for total wrist arthrodesis to determine the optimal plate length and ensure adequate screw purchase in the distal radius and the third metacarpal. Modern dedicated wrist fusion plates are anatomically pre-contoured to provide 10 to 15 degrees of wrist extension, which is the optimal position for maximizing functional grip strength and facilitating activities of daily living. The plate must be long enough to allow for at least three to four bi-cortical screws in the radius and three screws in the diaphysis of the third metacarpal.
The operating room setup requires the patient to be positioned supine with the operative arm extended on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is critical for meticulous joint preparation and nerve identification. Intra-operative fluoroscopy (C-arm) must be readily available and positioned to easily obtain PA and lateral views without compromising the sterile field. The surgeon must also prepare for potential autologous bone graft harvesting, typically from the distal radius, though the iliac crest may be prepped if a massive structural defect is anticipated.
Step-by-Step Surgical Approach and Fixation Technique
Exposure and Joint Preparation
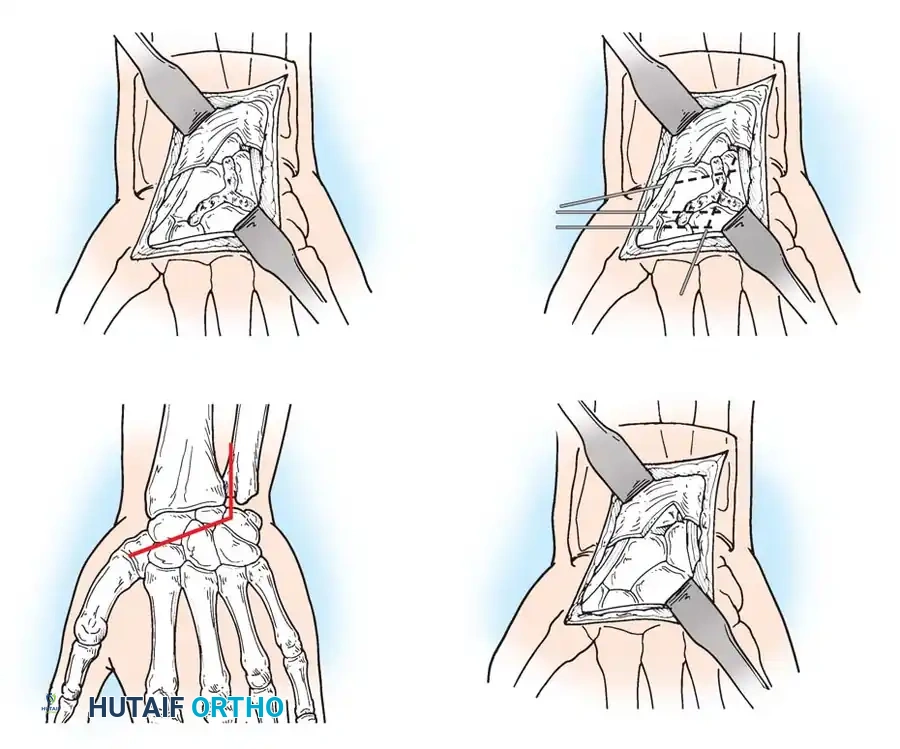
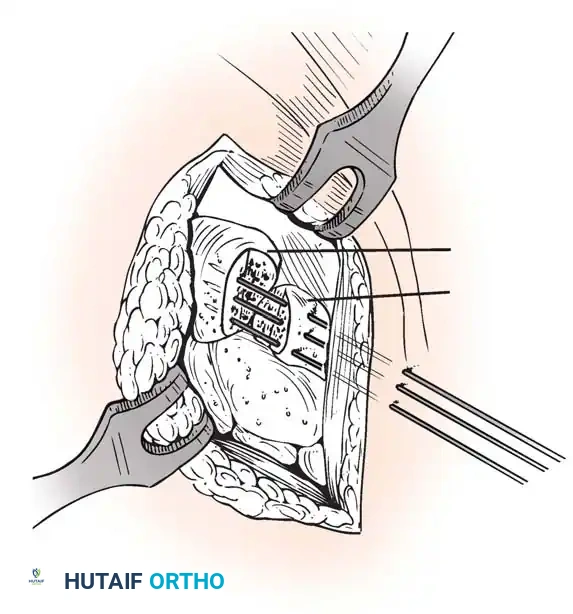
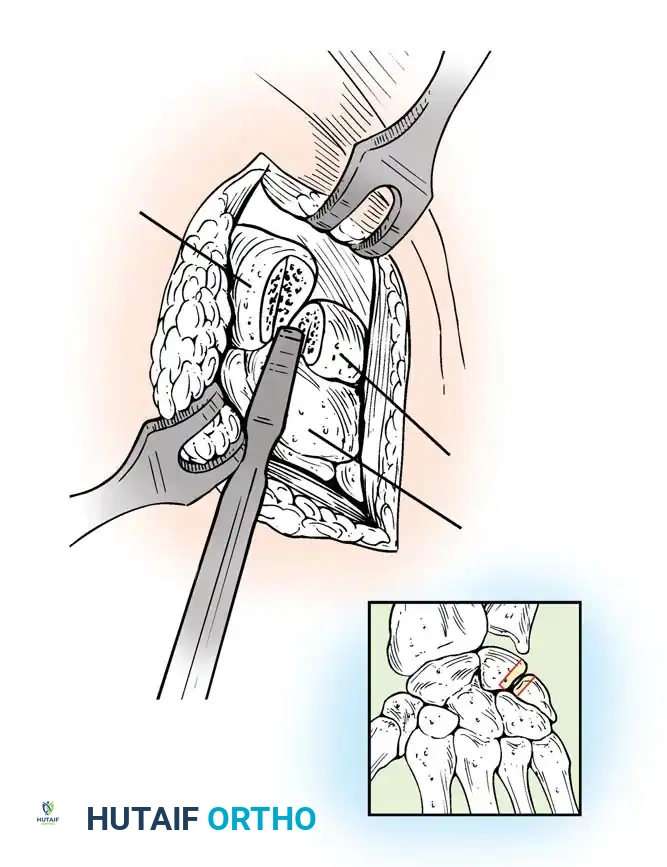
The surgical approach for a total wrist arthrodesis utilizes a longitudinal dorsal incision centered precisely over Lister’s tubercle, extending distally to the base of the third metacarpal. Meticulous subcutaneous dissection is performed to identify and protect the dorsal sensory branches of the radial and ulnar nerves. The extensor retinaculum is exposed, and the third extensor compartment is opened longitudinally. The extensor pollicis longus (EPL) tendon is mobilized and transposed radially to prevent impingement against the fusion plate. The retinaculum is then elevated as a radially based or ulnarly based flap, exposing the second and fourth extensor compartments, whose tendons are retracted to expose the dorsal wrist capsule.
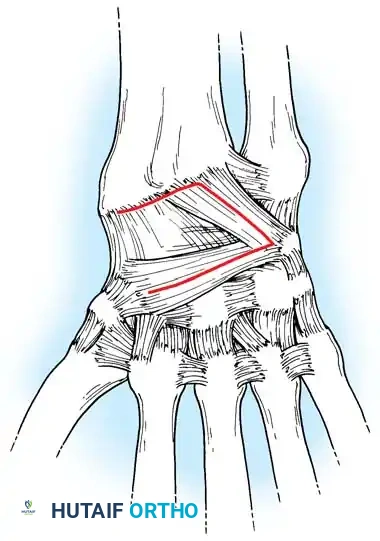
A robust, ligament-sparing dorsal capsulotomy is performed to expose the radiocarpal and midcarpal joints. A posterior interosseous nerve (PIN) neurectomy is routinely performed at the proximal aspect of the incision to provide profound regional analgesia. The critical phase of joint preparation involves the meticulous denudation of all articular cartilage down to bleeding subchondral bone. This includes the radiocarpal joint (radioscaphoid and radiolunate fossae), the midcarpal joint (scaphocapitate, lunocapitate, and triquetrohamate), and crucially, the second and third carpometacarpal (CMC) joints. The third CMC joint is notoriously difficult to fuse due to its rigid ligamentous constraints; thorough decortication using high-speed burrs and sharp curettes is mandatory to prevent nonunion.
Management of Scapholunate Dissociation and Perilunate Injuries
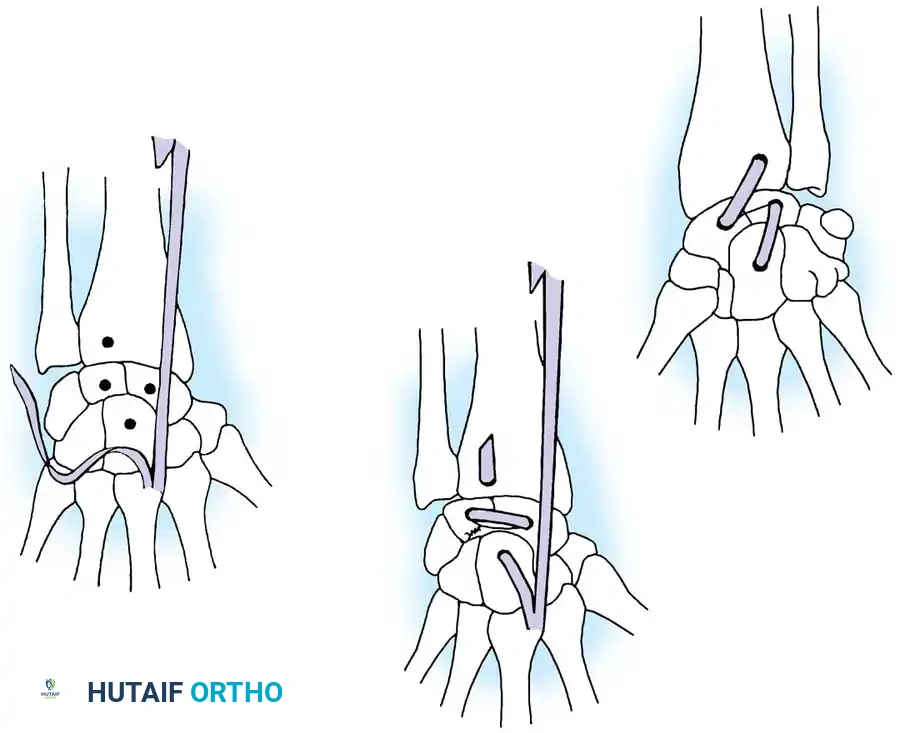
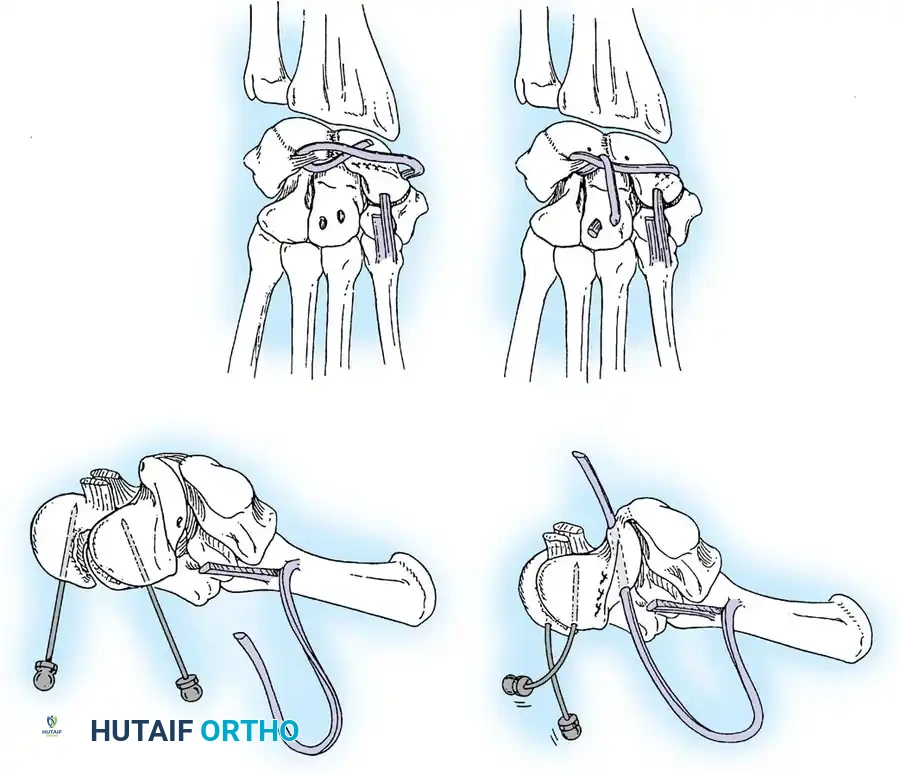
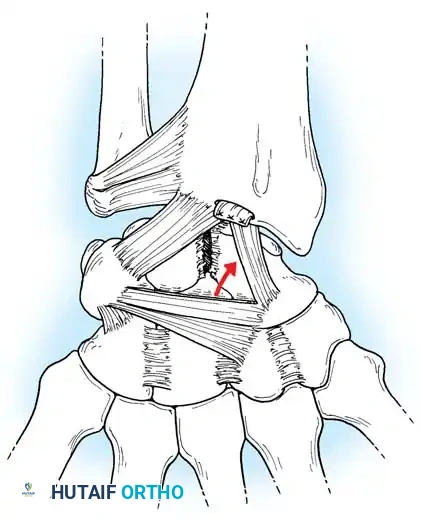
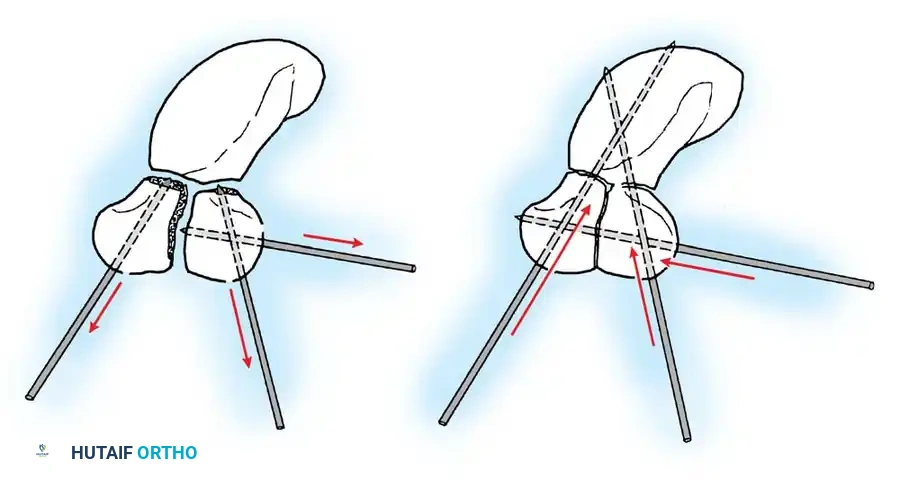
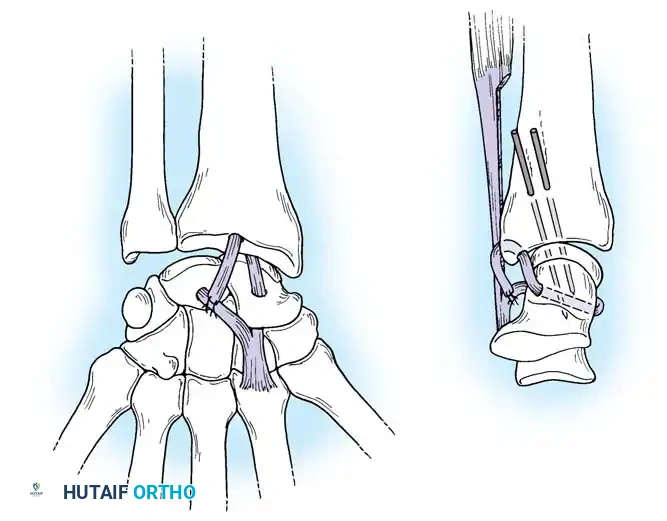
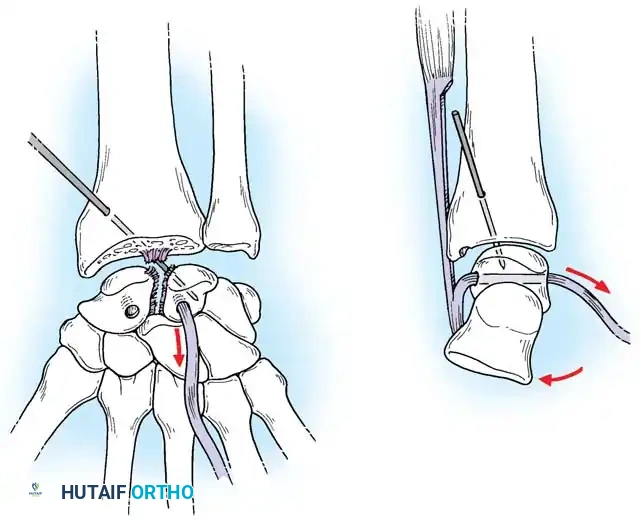
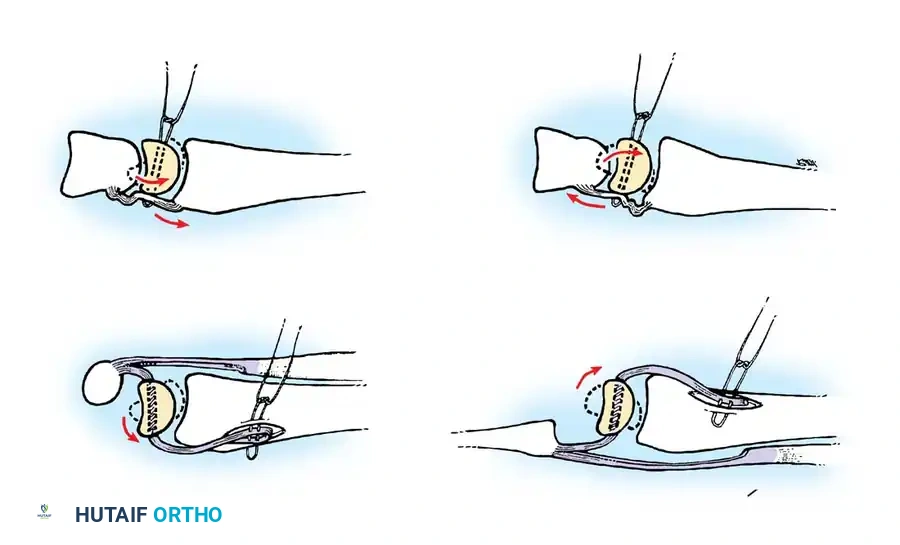
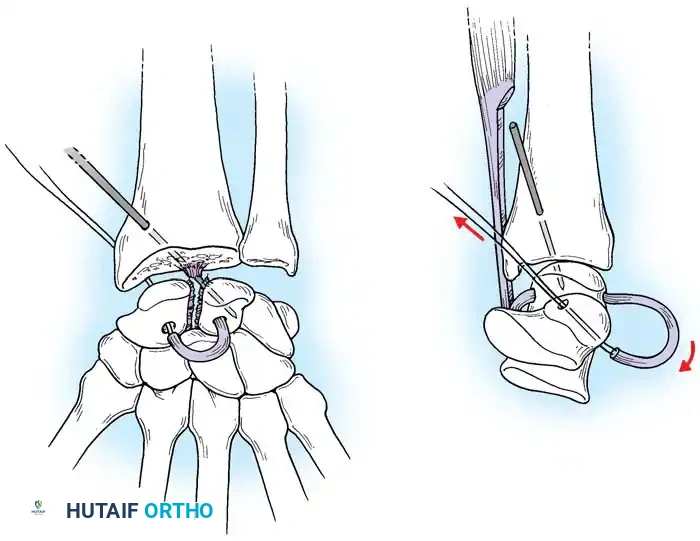
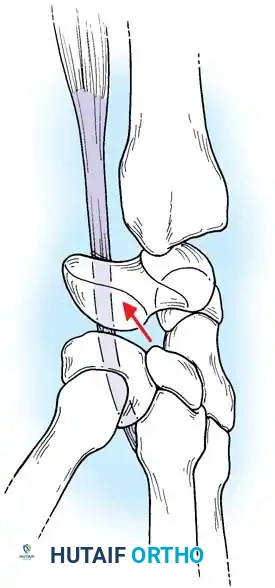
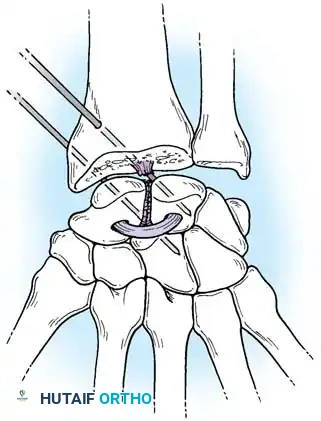
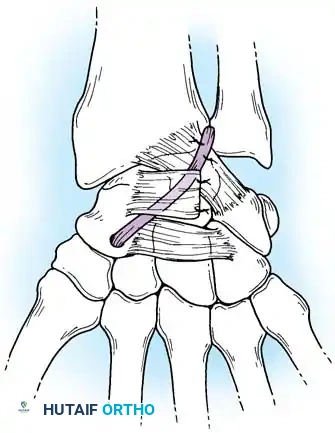
If the procedure is being performed for acute or subacute perilunate instability rather than end-stage arthritis, the surgical objectives shift from arthrodesis to precise anatomical reconstruction. In acute scapholunate dissociation (<4 weeks), open reduction through the dorsal approach allows for direct visualization of the SL interval. The scaphoid and lunate are reduced using joystick K-wires to correct the DISI deformity and close the diastasis. Once anatomic alignment is confirmed fluoroscopically, multiple 0.045-inch K-wires are driven from the scaphoid into the capitate and lunate to maintain the reduction.
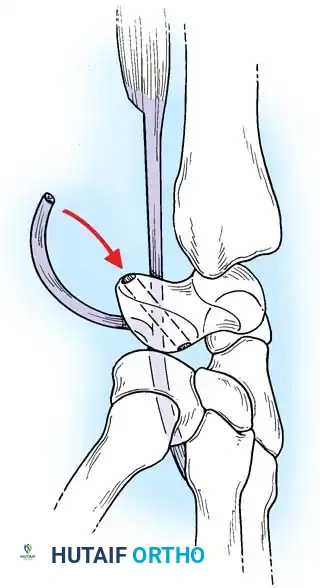
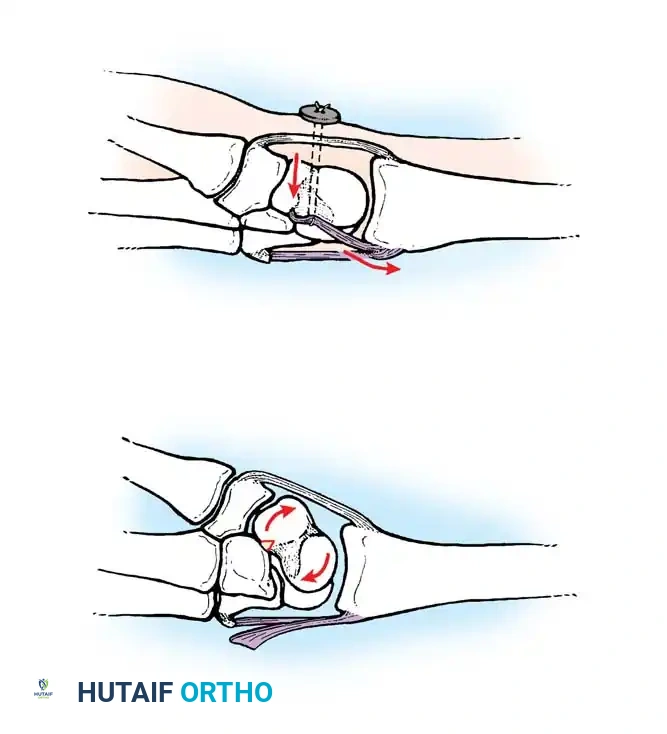
Primary repair of the dorsal SL interosseous ligament is then executed using micro-suture anchors placed into the scaphoid or lunate, depending on the avulsion site. In cases of chronic, irreparable SL tears without established arthritis, capsulodesis procedures (such as the Blatt capsulodesis or dorsal intercarpal ligament tenodesis) or bone-ligament-bone reconstructions may be attempted. For frank perilunate dislocations, a combined dorsal and volar approach is often necessary. The volar approach allows for decompression of the median nerve (carpal tunnel release) and direct repair of the critical volar extrinsic ligaments (RSC and LRL), while the dorsal approach facilitates the reduction of the intercalated segment and repair of the intrinsic ligaments.
Total Wrist Arthrodesis Technique
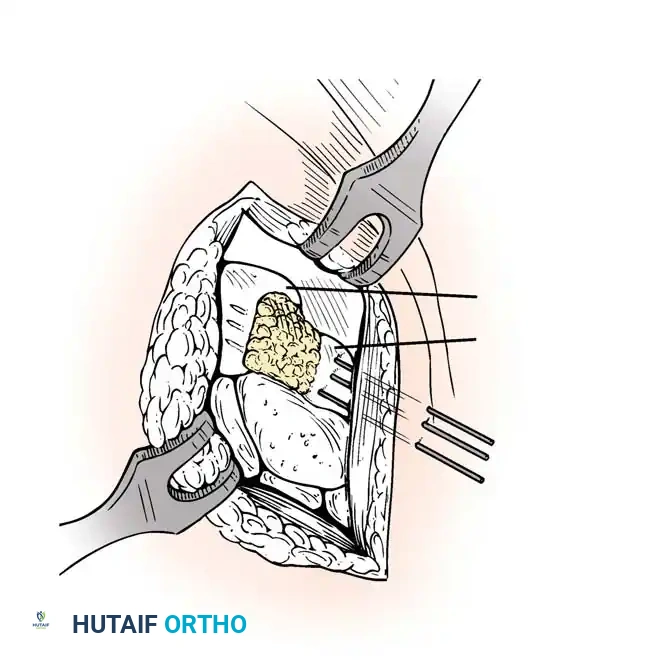
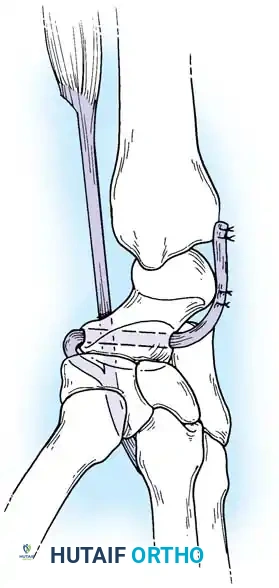
Following meticulous joint preparation for total wrist arthrodesis, the void spaces between the decorticated carpal bones must be densely packed with cancellous bone graft. A local distal radial bone graft portal, typically accessed through Lister's tubercle, provides an excellent source of highly osteogenic cancellous autograft. This graft is tightly impacted into the radiocarpal, midcarpal, and CMC joints. The pre-contoured wrist fusion plate (or a meticulously bent 3.5-mm dynamic compression plate) is then applied to the dorsal aspect of the radius, carpus, and third metacarpal.
Fixation begins distally. The plate is secured to the diaphysis of the third metacarpal using 3.5-mm cortical screws. Surgical Warning: It is imperative to ensure that these distal screws engage the dense diaphyseal bone without penetrating the palmar cortex. Prominent volar screws in the third metacarpal can severely tether the flexor tendons, leading to catastrophic loss of finger flexion. Once distal fixation is achieved, longitudinal traction is applied, and the plate is secured proximally to the distal radius, utilizing the dynamic compression holes to generate rigid compression across the radiocarpal fusion mass. Additional screws may be placed through the plate directly into the capitate to secure the midcarpal joint. The dorsal capsule and extensor retinaculum are then meticulously repaired over the plate to provide a soft tissue buffer, preventing EPL and extensor digitorum communis (EDC) tendon irritation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, total wrist arthrodesis and complex carpal reconstructions carry a significant risk profile. The most devastating complication is nonunion (pseudoarthrosis), which occurs in approximately 2% to 5% of cases. The most frequent site of nonunion is the third carpometacarpal joint, owing to inadequate decortication and the high biomechanical shear forces concentrated at this junction. Patients with nonunion typically present with persistent dorsal wrist pain and implant failure (screw breakage or plate fracture) months after the index procedure. Salvage requires revision surgery, removal of broken hardware, aggressive re-debridement of the nonunion site, massive structural bone grafting (often from the iliac crest), and revision plating with a longer, more robust construct.
Hardware prominence and extensor tendon irritation are the most common soft-tissue complications, occurring in up to 15% to 20% of patients. The dorsal subcutaneous border of the wrist has minimal adipose tissue, making the bulky fusion plates highly palpable. If the extensor retinaculum is not adequately interposed between the plate and the tendons, friction can lead to tenosynovitis and eventual extensor tendon rupture. Management involves hardware removal once solid osseous union is definitively confirmed on CT scan, typically no earlier than 12 to 18 months post-operatively. Tendon ruptures require staged reconstruction or tendon transfers (e.g., EIP to EPL transfer).
Infection and Complex Regional Pain Syndrome (CRPS) are less common but profoundly debilitating complications. Deep space infections require immediate surgical irrigation and debridement, targeted intravenous antibiotic therapy, and potentially hardware removal if the infection cannot be suppressed, though retaining stable hardware until union is preferred if possible. CRPS presents with severe, disproportionate pain, vasomotor instability, and joint stiffness. Aggressive early intervention with multimodal pain management, stellate ganglion blocks, and intensive hand therapy is required to prevent permanent dystrophic changes.
| Complication | Estimated Incidence | Etiology / Risk Factors |
Clinical & Radiographic Imaging Archive