Peroneus Brevis Tenodesis and Complex Hindfoot Arthrodesis: A Master Surgical Guide

Key Takeaway
The Myerson peroneus brevis tenodesis is a highly effective surgical intervention for chronic lateral ankle instability and hindfoot varus. By utilizing the non-essential peroneus brevis tendon, surgeons can reconstruct the lateral ligamentous complex. This comprehensive guide details the biomechanical rationale, precise surgical steps, tendon routing, calcaneal fixation, and adjunctive triple arthrodesis techniques required to correct severe cavovarus and calcaneocavus deformities in both neuromuscular and non-neuromuscular patients.
Comprehensive Introduction and Patho-Epidemiology
Chronic lateral ankle instability (CLAI), particularly when complicated by a progressive varus hindfoot deformity and concomitant peroneal tendon weakness, presents a formidable and multi-layered challenge to the reconstructive orthopaedic surgeon. When the ankle and subtalar joints are chronically unstable in a varus alignment due to the insidious insufficiency of both the static lateral ligamentous complex (anterior talofibular ligament [ATFL] and calcaneofibular ligament [CFL]) and the dynamic peroneal stabilizers, isolated anatomic repair (such as the Broström-Gould procedure) is virtually guaranteed to fail. The prevailing biomechanical forces in a varus hindfoot exponentially increase the tensile load on the lateral soft tissue structures, leading to rapid attenuation of any standard capsuloligamentous plication. In these highly complex scenarios, particularly those underscored by neuromuscular pathology, Myerson recommended a robust, non-anatomic tenodesis utilizing the peroneus brevis tendon to provide a rigid, structural checkrein against varus tilt and anterior talar translation.
The patho-epidemiology of this condition is broadly dichotomized into traumatic and neuromuscular etiologies. In the traumatic cohort, patients often suffer from decades of recurrent inversion injuries, leading to microvascular compromise of the peroneal tendons, longitudinal split tears, and eventual dynamic failure. Conversely, the neuromuscular cohort—encompassing conditions such as Charcot-Marie-Tooth (CMT) disease, poliomyelitis, and other hereditary sensorimotor neuropathies (HSMN)—presents a more insidious progression. In CMT, the intrinsic muscle imbalance, specifically the overpowering of the tibialis anterior and peroneus brevis by the peroneus longus and tibialis posterior, drives the first ray into rigid plantarflexion. This plantarflexed first ray acts as a kickstand, driving the hindfoot into an obligatory varus position during the stance phase of gait, which subsequently stretches and destroys the lateral ligamentous complex.
The rationale for utilizing the peroneus brevis in these advanced reconstructive efforts is deeply rooted in its expendability in specific pathologic states. In patients with profound neuromuscular weakness, the peroneus brevis often possesses negligible active motor function, rendering it an ideal, robust autograft for structural stabilization without sacrificing dynamic eversion strength. This comprehensive masterclass details the preoperative evaluation, biomechanical principles, and step-by-step surgical execution of the Myerson peroneus brevis tenodesis. Furthermore, it explores the critical adjunctive bony procedures—namely the Siffert, Forster, and Nachamie triple arthrodesis, and the Dunn arthrodesis—required to correct severe cavovarus and calcaneocavus deformities when soft tissue reconstruction alone is insufficient.
Understanding the interplay between soft tissue balancing and osseous architecture is the cornerstone of successful hindfoot reconstruction. A meticulously executed tenodesis will invariably fail if placed on a foundation of uncorrected bony malalignment. Therefore, the surgeon must approach these deformities with a comprehensive armamentarium, prepared to transition from joint-sparing osteotomies to complex, multi-planar arthrodeses to achieve the ultimate goal: a plantigrade, stable, and painless foot.
Detailed Surgical Anatomy and Biomechanics
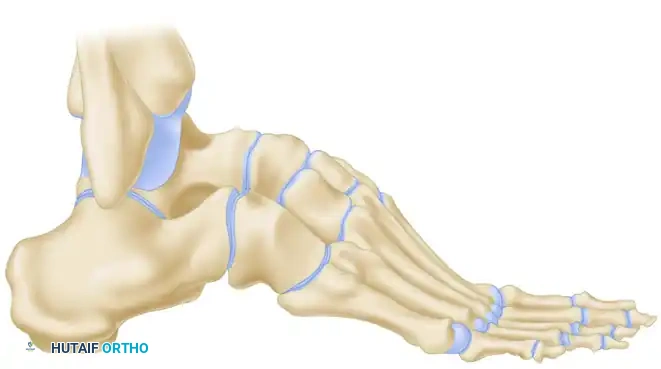
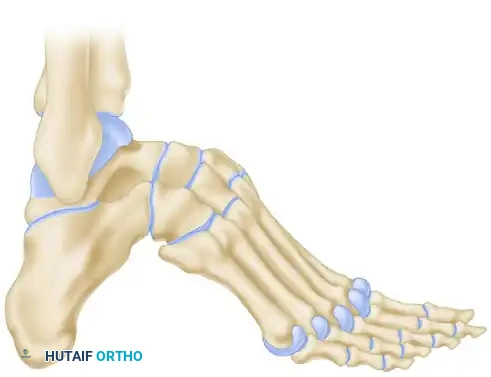
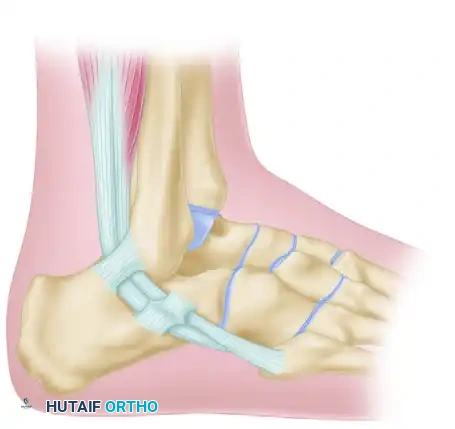
A profound understanding of the spatial relationship and intrinsic biomechanics of the peroneal tendons, lateral ligamentous complex, and hindfoot osseous anatomy is paramount for safe harvest, precise routing, and successful reconstruction. The peroneus longus and brevis muscles originate from the lateral compartment of the leg, innervated by the superficial peroneal nerve. Proximal to the lateral malleolus, the muscle belly of the peroneus brevis extends significantly further distally than that of the peroneus longus. This anatomic distinction is a critical surgical landmark; the brevis tendon can be easily identified proximally because its muscle fibers extend almost to the level of the superior peroneal retinaculum (SPR), whereas the peroneus longus tendon is completely tendinous at this level.
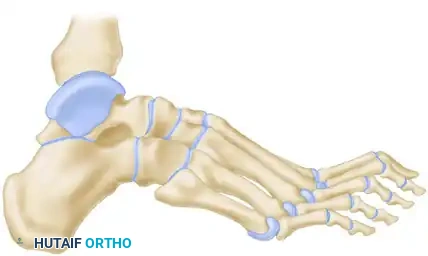
As the tendons descend into the retromalleolar groove of the fibula, they share a common synovial sheath. At the level of the fibula, immediately posterior to the lateral malleolus, the peroneus longus lies anterior, or superficial, to the brevis tendon. The retromalleolar groove is deepened by a fibrocartilaginous ridge and roofed by the SPR, which is the primary restraint against peroneal tendon subluxation. During tendon harvest, meticulous preservation of the SPR is mandatory to prevent iatrogenic subluxation of the remaining peroneal structures. Distal to the tip of the fibula, the spatial relationship of the tendons undergoes a 90-degree rotation. As they pass the peroneal tubercle of the calcaneus, the brevis tendon becomes superior and superficial, progressing to its insertion at the styloid process of the base of the fifth metatarsal. The longus tendon dives deep, entering the cuboid groove to traverse the plantar aspect of the foot, ultimately inserting on the plantar-lateral aspect of the medial cuneiform and the base of the first metatarsal.

Biomechanically, the lateral ankle is stabilized by a synergistic relationship between static ligaments and dynamic muscle forces. The ATFL is the primary restraint to anterior translation of the talus and internal rotation in plantarflexion, while the CFL restrains inversion in neutral and dorsiflexed positions. In chronic instability, the CFL is often completely obliterated, leading to profound subtalar instability. The Myerson tenodesis is designed to recreate the vectors of both the ATFL and the CFL. By routing the peroneus brevis through the distal fibula and securing it to the lateral calcaneal wall, the surgeon establishes a robust, non-yielding tether that spans both the tibiotalar and talocalcaneal joints, effectively neutralizing the pathologic varus and anterior translational forces.
In the setting of a cavovarus deformity, the biomechanics of the entire foot and ankle are severely perturbed. The elevated longitudinal arch (cavus) decreases the shock-absorbing capacity of the midfoot, transmitting immense ground reaction forces directly to the lateral column. The varus alignment of the calcaneus shifts the mechanical axis of the lower extremity medial to the subtalar joint axis, creating a massive inversion moment during heel strike and midstance.

If this bony architecture is not corrected via osteotomy or arthrodesis, the constant inversion moment will inevitably stretch and rupture any lateral soft tissue reconstruction, regardless of the graft's initial tensile strength. Therefore, the biomechanical goal of surgery is twofold: realign the osseous structures to neutralize the mechanical axis, and reconstruct the soft tissue restraints to provide dynamic and static stability.
Exhaustive Indications and Contraindications
Patient selection and the precise delineation of surgical indications are the most critical determinants of long-term success in complex lateral ankle and hindfoot reconstruction. The decision to proceed with a Myerson peroneus brevis tenodesis, with or without a concomitant complex arthrodesis, requires a nuanced synthesis of the patient's clinical history, neurologic status, and radiographic parameters.
Patients typically present with a protracted history of recurrent inversion injuries, subjective sensations of the ankle "giving way" on uneven terrain, and chronic lateral-sided ankle pain. The pain is often multifactorial, arising from anterolateral soft tissue impingement, peroneal tendinopathy, and early degenerative changes in the medial tibiotalar joint due to chronic varus tilt. A thorough biomechanical examination must assess hindfoot alignment, midfoot mobility, and forefoot-driven hindfoot deformities. The Coleman block test is indispensable in this regard; it differentiates a flexible, forefoot-driven hindfoot varus (which corrects when the plantarflexed first ray is allowed to drop off the block) from a rigid, fixed hindfoot varus (which remains in varus despite neutralizing the forefoot).
Neurologic evaluation is absolutely critical. The surgeon must differentiate between isolated ligamentous insufficiency secondary to trauma and underlying neuromuscular disorders, such as CMT, poliomyelitis, or other forms of HSMN. This distinction directly dictates the surgical strategy: in patients with HSMN, the entire peroneus brevis tendon can be harvested because it lacks functional motor capacity, whereas in non-neuromuscular instability, only a split graft (anterior half) should be harvested to preserve dynamic eversion strength.

If the patient presents with a severe, multi-planar calcaneocavovarus deformity, soft tissue reconstruction is entirely secondary to the massive bony realignment required.
| Parameter | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Ligamentous Status | Chronic, symptomatic lateral ankle instability failing >6 months of conservative management (PT, bracing). | Acute lateral ankle sprains; instability manageable with conservative care. |
| Deformity Type | Flexible or rigid varus hindfoot; cavovarus; calcaneocavus. | Severe, uncorrectable valgus deformity (requires medial column stabilization). |
| Neuromuscular Status | CMT, Poliomyelitis, HSMN (ideal for full PB harvest); Traumatic laxity (ideal for split PB harvest). | Active, progressive, rapidly deteriorating neurologic disease (relative contraindication). |
| Joint Articular Cartilage | Mild to moderate asymmetric narrowing; reducible talar tilt. | End-stage, rigid pantalar arthritis; fixed tibiotalar varus with severe bone loss (requires pantalar arthrodesis). |
| Vascular/Soft Tissue | Intact peripheral pulses; adequate lateral skin envelope. | Severe peripheral vascular disease; active lateral ulceration or infection. |
Myerson emphasized that mild degenerative changes within the tibiotalar joint are not an absolute contraindication for joint-sparing procedures, provided the hindfoot can be realigned to offload the degenerative medial compartment. However, if the talar tilt is fixed, rigid, and accompanied by severe articular pain and subchondral sclerosis, joint-sparing tenodesis will fail to relieve pain, and a formal ankle or pantalar arthrodesis must be considered as the definitive salvage procedure.

Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of complex hindfoot reconstruction. The clinical assessment must be correlated with high-quality, weight-bearing radiographic imaging. Standard weight-bearing anteroposterior (AP), lateral, and mortise views of the foot and ankle are mandatory. The lateral view is scrutinized for Meary’s angle (talo-first metatarsal angle) to assess the severity of the cavus, and the calcaneal pitch to differentiate between standard cavovarus and calcaneocavus deformities.

Stress radiographs, including anterior drawer and talar tilt views, are obtained to quantify the degree of mechanical instability, though in severe neuromuscular cases, the gross clinical instability often renders stress views redundant.
Advanced imaging is frequently utilized. Magnetic Resonance Imaging (MRI) is invaluable for assessing the structural integrity of the peroneal tendons. The surgeon must identify pre-existing longitudinal split tears, tenosynovitis, or tendinosis, as severely degenerated tendons may not possess the tensile strength required for a robust tenodesis. Furthermore, MRI provides high-resolution evaluation of the articular cartilage of the tibiotalar and subtalar joints. Computed Tomography (CT) with 3D reconstruction is highly recommended when planning complex triple arthrodeses (such as the Dunn or Siffert procedures), as it allows for precise volumetric templating of the bony wedge resections required to achieve a plantigrade foot.
Patient positioning and anesthesia are critical for optimizing surgical exposure and minimizing intraoperative complications. The patient is placed in the strict lateral decubitus position. A vacuum bean bag is utilized to secure the torso, and an axillary roll is placed to protect the dependent brachial plexus. All bony prominences, particularly the contralateral fibular head and greater trochanter, must be meticulously padded to prevent compressive neuropathies.
A well-padded thigh tourniquet is applied to provide a bloodless surgical field, which is essential for identifying the delicate sural nerve and the intricate fascial layers of the lateral ankle. Regional anesthesia, specifically a continuous popliteal sciatic nerve block combined with a saphenous nerve block, is the gold standard. This is typically supplemented with general anesthesia or deep intravenous sedation. The regional block provides profound intraoperative muscle relaxation and exceptional postoperative analgesia, significantly reducing the requirement for systemic opioids and facilitating earlier discharge.
Step-by-Step Surgical Approach and Fixation Technique
The Myerson Peroneus Brevis Tenodesis
The surgical execution of the Myerson tenodesis demands meticulous soft tissue handling and precise biomechanical tensioning.
Step 1: Incision and Exposure
A generous curvilinear incision is made posterolateral to the fibula. The incision begins 8 to 10 cm proximal to the tip of the lateral malleolus, tracking just posterior to the palpable course of the peroneal tendons.
The incision is carried distally, curving gently around the tip of the fibula and extending along the lateral border of the hindfoot toward the calcaneocuboid joint. The subcutaneous tissues are sharply dissected. It is imperative to identify, mobilize, and protect the sural nerve, which typically crosses the surgical field from posterior to anterior at the level of the lateral calcaneal wall. Retraction of the nerve should be gentle, utilizing vessel loops to prevent traction neuropraxia.
Step 2: Tendon Identification and Harvest
The investing fascia of the lateral compartment is incised proximally. The peroneal tendon sheath is opened above the level of the superior peroneal retinaculum (SPR). The surgeon must take great care not to divide the SPR itself, as preserving this robust retinacular tissue is critical to prevent postoperative subluxation of the peroneus longus. The peroneus brevis tendon is identified by its muscular fibers extending distally.
For Patients with Hereditary Sensorimotor Neuropathy (HSMN):
In the absence of functional motor capacity, the entire peroneus brevis tendon is utilized. The tendon is transected 8 to 10 cm proximal to the tip of the fibula. The muscle belly is sharply peeled off the tendon using a periosteal elevator or a #15 blade, maximizing the length and girth of the graft.
For Patients Without Motor Neuropathy:
To preserve dynamic eversion, the tendon is split longitudinally. The anterior half of the peroneus brevis is harvested, while the posterior half remains intact. The split is carried distally to the peroneal tubercle.
Step 3: Distal Tendon Preparation
Attention is directed distally near the calcaneocuboid joint. The peroneus brevis tendon is identified and delivered into the distal aspect of the wound.
The separate distal sheath enclosing the peroneus brevis is divided. The tendon is split longitudinally (if performing a split harvest), ensuring that the distal 1 to 2 inches of the tendon remain firmly and anatomically attached to its insertion at the styloid process of the base of the fifth metatarsal. A Krackow whipstitch using a high-tensile, non-absorbable #2 suture is placed in the proximal free end of the graft to facilitate passage and tensioning.
Step 4: Fibular Tunnel Preparation
The lateral malleolus is exposed subperiosteally. A 4.5-mm drill bit is used to create a transosseous tunnel through the fibula. The tunnel is oriented from anterior to posterior, located approximately 1 cm proximal to the distal tip of the fibula, mimicking the anatomic origin of the ATFL and CFL.
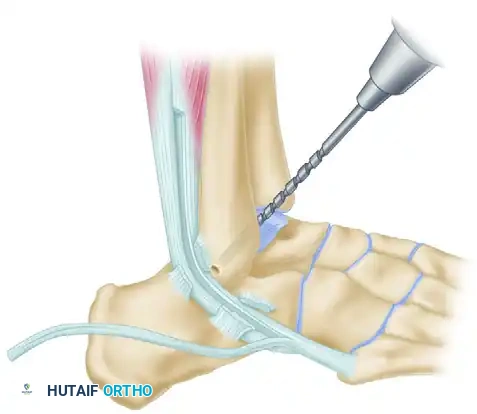
The tunnel must be cleared of any bony debris and sharp cortical edges using a small curette and a rasp to ensure smooth passage of the tendon graft and prevent abrasive fraying of the tendon over time.
Step 5: Tendon Routing and Fibular Fixation
The prepared tendon graft is passed through the fibular tunnel from anterior to posterior.
Surgical Pearl: The ankle must be held in a strictly neutral position (0 degrees of dorsiflexion/plantarflexion and neutral inversion/eversion) during tensioning. Over-tightening in eversion will restrict subtalar motion, while under-tensioning will fail to stabilize the joint. The tendon is sutured to the robust periosteum over the anterior aspect of the fibula using multiple #0 non-absorbable sutures to establish the first point of rigid fixation.
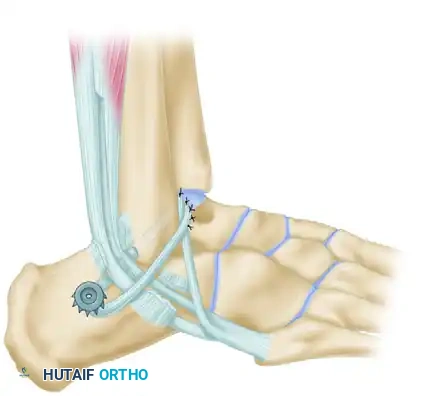
Step 6: Calcaneal Fixation
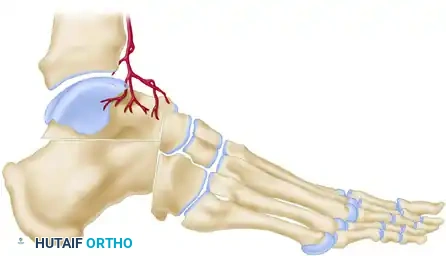
The tendon is then passed deep to the peroneus longus tendon, directing it toward the lateral wall of the calcaneus to recreate the vector of the CFL. A pilot hole is drilled into firm subchondral bone on the lateral aspect of the calcaneus, slightly posterior and inferior to the subtalar joint axis. A 4.0-mm fully threaded cancellous screw, paired with a polyacetal spiked ligament washer, is selected.
Surgical Warning: A screw length of 30 mm is typically sufficient. The surgeon must add 3 to 4 mm to the measured depth to accommodate the thickness of the spiked washer. It is absolutely critical that the screw does not penetrate the medial calcaneal cortex, as this could severely tether the flexor hallucis longus (FHL) tendon or injure the medial neurovascular bundle.
The tendon is pulled inferiorly to establish maximum tension. A #11 blade is used to create a small longitudinal slit directly through the substance of the tendon. The screw and washer are inserted through this slit. While maintaining strict distal traction on the tendon, the screw is advanced until the spiked washer gains firm, compressive purchase against the lateral calcaneal cortex, locking the tendon to the bone.
Step 7: Final Routing and Closure
The remaining free end of the tendon (usually 2 to 3 cm long) is passed superficial to the peroneus longus tendon. It is looped back upon itself and attached securely to the tip of the fibula and the adjacent periosteum using multiple interrupted non-absorbable sutures, creating a reinforced figure-of-eight construct.
The tourniquet is deflated, meticulous hemostasis is achieved, and the wound is closed in a layered fashion.
Complex Deformities: Triple Arthrodesis for Cavovarus and Calcaneocavus
When hindfoot varus is rigid, or severe cavus deformities are present, soft tissue reconstruction alone is futile. Structural realignment via complex arthrodesis is mandated.
Siffert, Forster, and Nachamie Triple Arthrodesis
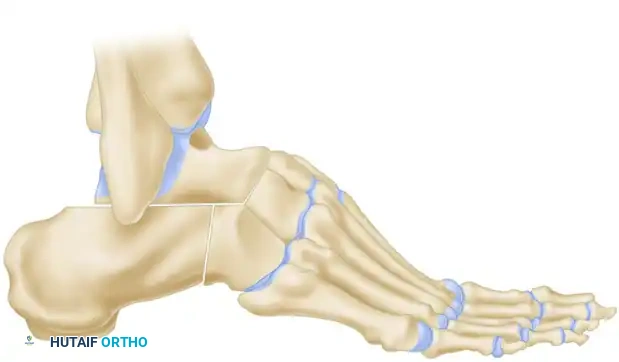
For severe, rigid cavus deformities, the Siffert modification of the triple arthrodesis is the procedure of choice. This technique relies on the resection of a precise dorsal wedge to plantarflex the forefoot and flatten the longitudinal arch.
A bi-planar wedge of bone is removed via osteotomy from the midtarsal and subtalar joints. Crucially, the superior articular portion of the talar head is retained to form a structural osseous "beak."
The soft tissue structures anterior to the ankle joint (extensor tendons, dorsalis pedis artery, deep peroneal nerve) are left entirely undisturbed to maintain vascularity and anterior stability.

In the final reconstructed position, the forefoot is displaced plantarward, and the dorsal cortex of the navicular is locked securely beneath the remaining "beak" of the talar head. This bony lock prevents dorsal subluxation of the midfoot under weight-bearing loads and maintains the corrected arch height.
Arthrodesis for Calcaneocavus Deformity
Clinical & Radiographic Imaging Archive