

Comprehensive Introduction and Patho-Epidemiology
Peroneal tendon pathology is a frequently underestimated and misdiagnosed etiology of chronic lateral ankle pain, often overshadowed by the more ubiquitous lateral ankle sprain. The spectrum of disease ranges from acute tenosynovitis to chronic tendinosis, longitudinal split tears, and complete ruptures. Understanding the pathomechanics of these lesions requires an appreciation of the complex interplay between the dynamic stabilizers of the lateral hindfoot and the static osseous and retinacular constraints. When non-operative modalities fail, surgical intervention is not merely about restoring tendon continuity; it demands a comprehensive reconstruction of the biomechanical environment to prevent recurrence. This chapter provides an exhaustive, intraoperative masterclass on the evaluation, decision-making, and surgical execution of peroneal tendon repair and reconstruction.
The mechanisms of injury dictating peroneal tendon tears are multifaceted, with subluxation-induced attrition tears being the most prevalent. Chronic lateral ankle instability leads to repetitive subluxation of the peroneal tendons over the sharp posterolateral edge of the fibula. This relentless mechanical friction generates longitudinal splitting, predominantly affecting the peroneus brevis due to its direct interposition between the fibula and the peroneus longus. Compressive tears represent another distinct pathomechanical entity, wherein the peroneus brevis is crushed between the unyielding posterior fibula and a taut, superficial peroneus longus tendon, particularly in the setting of a congenitally shallow or tight retromalleolar groove.
Acute traumatic tears, while less common in isolation, are frequently associated with high-energy mechanisms such as displaced intra-articular calcaneal fractures, severe inversion injuries, or forced dorsiflexion of an everted foot. These acute events can cause sudden, violent eccentric contraction leading to rupture. Furthermore, pathology specific to the peroneus longus must be distinguished from brevis lesions. Longus tears are classically located distally, either at the level of a hypertrophied peroneal tubercle or within the cuboid groove. At the cuboid, the tendon undergoes a sharp angular change in trajectory, subjecting it to immense sheer stress, often exacerbated by the presence of an enlarged or fractured os peroneum.
Beyond direct mechanical trauma, the operating surgeon must remain vigilant regarding systemic and local etiological factors that compromise tendon integrity. Systemic conditions such as rheumatoid arthritis, seronegative spondyloarthropathies, hyperparathyroidism, and advanced diabetic neuropathy induce microvascular compromise and collagen degradation, predisposing the patient to spontaneous rupture. Locally, a history of multiple corticosteroid injections into the tendon sheath remains a notorious iatrogenic catalyst for catastrophic tendon failure. Crucially, underlying biomechanical malalignment—specifically a cavovarus hindfoot posture—places exponential stress on the lateral compartment, acting as a primary driver for recurrent peroneal pathology if left unaddressed during reconstructive surgery.
Detailed Surgical Anatomy and Biomechanics
Musculotendinous Architecture and Vascularity
A profound mastery of regional anatomy is the cornerstone of successful peroneal reconstructive surgery. The peroneus longus and peroneus brevis originate within the lateral compartment of the leg, both receiving motor innervation from the superficial peroneal nerve (L4, L5, S1). The peroneus brevis originates from the distal two-thirds of the lateral fibular shaft and the adjacent intermuscular septa. Its tendon courses anterior and deep to the peroneus longus within the retromalleolar groove, ultimately inserting onto the tuberosity at the base of the fifth metatarsal. Biomechanically, the brevis serves as the primary evertor of the foot and assists in ankle plantarflexion, acting as a critical dynamic stabilizer against inversion stress.
The peroneus longus originates more proximally, arising from the fibular head and the proximal two-thirds of the lateral fibular shaft. Its tendon travels posterior and superficial to the brevis tendon behind the lateral malleolus. Distal to the fibula, it passes inferior to the peroneal tubercle of the calcaneus, enters the plantar aspect of the foot through the cuboid groove, and traverses obliquely to insert onto the plantar posterolateral aspect of the medial cuneiform and the base of the first metatarsal. The longus is a powerful plantarflexor of the first ray and an evertor of the foot, playing an indispensable role in stabilizing the medial longitudinal arch during the terminal stance phase of gait. Notably, both tendons possess critical watershed zones of relative avascularity—the brevis within the retromalleolar groove and the longus at the cuboid turn—rendering these specific regions highly susceptible to degenerative tearing and delayed healing.
Retinacular Constraints and Osteology
The stability of the peroneal tendons is heavily reliant upon a complex network of fibrous slings and osseous morphology. The Superior Peroneal Retinaculum (SPR) is the primary static restraint preventing anterior subluxation of the tendons out of the retromalleolar groove. This robust, 1 to 2-cm fibrous band originates from the posterolateral aspect of the distal fibula and inserts onto the lateral wall of the calcaneus and the Achilles tendon sheath. The SPR is contiguous with a fibrocartilaginous ridge situated on the posterolateral fibular border, which effectively deepens the groove. Attenuation, stripping, or rupture of the SPR and its associated ridge is the sine qua non of recurrent peroneal tendon dislocation. The Inferior Peroneal Retinaculum (IPR), located further distally, stabilizes the tendons as they diverge toward their respective insertions but is less frequently implicated in primary subluxation pathology.
The osteology of the lateral ankle and hindfoot dictates the mechanical stress experienced by the tendons. The posterolateral fibular groove exhibits significant anatomical variation; cadaveric studies demonstrate that it is concave in approximately 82% of individuals, flat in 11%, and convex in 7%. A flat or convex groove intrinsically predisposes the patient to tendon subluxation and subsequent attrition tears. Distally, the peroneal tubercle of the calcaneus serves to separate the longus and brevis tendons into distinct synovial sheaths. Hypertrophy of this tubercle can result in severe stenosis and mechanical impingement, predominantly affecting the peroneus longus. Further distally, the cuboid groove represents a high-friction anatomical pulley where the longus tendon is redirected plantarward; pathology here is frequently associated with the os peroneum, a sesamoid bone present in roughly 20% of the population.
Neurovascular Considerations
Navigating the neurovascular landscape of the lateral ankle is fraught with potential pitfalls. The superficial peroneal nerve provides motor innervation to the lateral compartment before piercing the deep fascia to supply sensory innervation to the dorsum of the foot. However, it is the sural nerve that demands the utmost vigilance during the surgical approach. The sural nerve is formed by the confluence of the medial sural cutaneous nerve and the sural communicating branch, coursing subcutaneously along the posterolateral aspect of the calf and ankle.
It runs in close proximity to the small saphenous vein, passing an average of 10 to 15 millimeters posterior to the tip of the lateral malleolus. The nerve frequently crosses the planned surgical incision line for peroneal tendon exploration. Iatrogenic injury to the sural nerve—whether through direct transection, aggressive retraction, or entrapment within scar tissue—can precipitate a devastating neuroma or complex regional pain syndrome (CRPS), often resulting in postoperative morbidity that eclipses the original tendon pathology. Meticulous blunt dissection and early identification of the nerve are non-negotiable tenets of this procedure.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for peroneal tendon pathology requires a nuanced synthesis of clinical findings, advanced imaging, and the patient's functional demands. Non-operative management, comprising non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy, lateral heel wedges, and judicious immobilization, is generally the first-line approach for acute tenosynovitis or first-time, non-displaced subluxation events. However, surgical intervention becomes indicated when these conservative measures are exhausted without symptomatic relief, or when structural integrity is fundamentally compromised.
Surgical indications include symptomatic longitudinal split tears of the peroneus brevis or longus that have failed 3 to 6 months of conservative care. Acute complete ruptures, particularly in high-demand athletes, warrant early primary repair to prevent retraction and irreversible muscle atrophy. Chronic recurrent subluxation or dislocation of the peroneal tendons, which inevitably leads to attrition tearing, is an absolute indication for surgical stabilization, typically involving SPR repair and potentially fibular groove deepening. Furthermore, the presence of space-occupying lesions within the tendon sheath—such as low-lying muscle bellies (e.g., peroneus quartus), symptomatic os peroneum with associated longus tearing, or hypertrophic osteophytes at the peroneal tubercle—necessitates surgical decompression and debridement.
Contraindications to peroneal tendon repair are primarily related to the patient's overall physiological status and the local soft tissue envelope. Active local or systemic infection is an absolute contraindication. Severe peripheral vascular disease or poorly controlled diabetes mellitus with significant microvascular compromise drastically increases the risk of catastrophic wound healing complications and should prompt extreme caution or outright avoidance of elective surgery. Relative contraindications include profound, fixed equinovarus deformities where soft tissue balancing alone will fail without concurrent major osseous reconstruction, or patients with profound non-compliance who are unable to adhere to the rigorous postoperative rehabilitation protocols required for successful tendon healing.
| Clinical Scenario | Indication for Surgery | Contraindication / Relative Contraindication |
|---|---|---|
| Acute Complete Rupture | High-demand athlete, significant retraction, failure of acute immobilization. | Sedentary patient with high surgical risk, severe peripheral neuropathy. |
| Chronic Split Tear | Persistent pain >3-6 months despite PT, bracing, and NSAIDs. | Active overlying cellulitis or deep space infection. |
| Recurrent Subluxation | Symptomatic instability, palpable/audible clunk, failure of taping/bracing. | Asymptomatic subluxation (incidental finding), lack of patient compliance. |
| Hypertrophic Tubercle | MRI-confirmed impingement, localized pain refractory to non-operative care. | Severe peripheral arterial disease (PAD) precluding incisional healing. |
| Associated Cavovarus | Tendon repair MUST be combined with calcaneal osteotomy/ligament balancing. | Unwillingness to undergo complex hindfoot reconstruction. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Diagnostic Modalities
Pre-operative planning is initiated with a rigorous history and physical examination. The surgeon must ascertain the chronicity of the symptoms, previous interventions (especially corticosteroid injections), and the precise anatomical location of the pain. Pain localized strictly to the retromalleolar space suggests brevis pathology or SPR insufficiency, whereas pain tracking distally to the lateral calcaneal wall or plantar cuboid strongly implicates the peroneus longus. Physical examination must include a meticulous assessment of hindfoot alignment. A subtle cavovarus foot places the lateral column under immense tension; failing to recognize and surgically correct this underlying osseous deformity (e.g., via a lateralizing calcaneal osteotomy or dorsiflexing first metatarsal osteotomy) guarantees eventual failure of the soft-tissue tendon repair.
Imaging is critical for surgical templating. Weight-bearing radiographs of the foot and ankle are mandatory to evaluate overall alignment, rule out fractures, and assess the osseous architecture. The axial calcaneal (Harris heel) view is particularly useful for evaluating the morphology of the lateral calcaneal wall and identifying a hypertrophied peroneal tubercle. While ultrasound provides excellent dynamic assessment of tendon subluxation, Magnetic Resonance Imaging (MRI) remains the gold standard for defining intra-substance tendon pathology.
MRI allows for the precise evaluation of tendon morphology, the presence of longitudinal splits, tenosynovitis, and the integrity of the retinacular structures. It also helps identify anomalous anatomy, such as a low-lying peroneus brevis muscle belly or a peroneus quartus muscle, which can contribute to retromalleolar overcrowding.
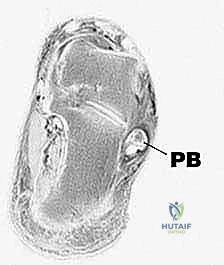
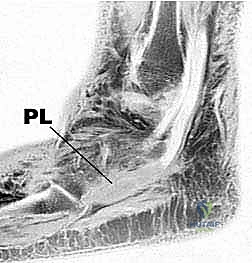
Fellows, observe the MRI sequences above. Note the fluid distension within the common peroneal sheath and the heterogeneous signal intensity within the peroneus brevis, classic hallmarks of a longitudinal split tear. However, always remember that MRI can occasionally underestimate the true longitudinal extent of the tear, which will only be fully appreciated upon direct surgical visualization.
Patient Positioning and Hemostasis
Optimal patient positioning is paramount for unhindered access to the posterolateral ankle. The patient is placed in the supine position on a standard radiolucent operating table. A well-padded bump (typically a rolled blanket or sandbag) is placed beneath the ipsilateral hip. This maneuver internally rotates the lower extremity, bringing the lateral malleolus and the entire course of the peroneal tendons into a direct, orthogonal view for the surgeon. The contralateral leg is carefully padded and secured to prevent inadvertent shifting during the procedure.
A pneumatic tourniquet is applied to the proximal thigh over adequate soft padding. Exsanguination of the limb using an Esmarch bandage, followed by tourniquet inflation (typically to 250-300 mmHg, depending on the patient's systolic blood pressure and thigh circumference), is essential to provide a pristine, bloodless surgical field. This is critical because the identification of fine longitudinal tendon splits and the meticulous protection of the sural nerve require optimal visualization. The operative extremity is then elevated on a specialized ankle block or stacked blankets to allow the surgeon to freely manipulate the foot through a full range of motion—particularly eversion and inversion—which is necessary for dynamic intraoperative testing of tendon excursion and retinacular stability. Fluoroscopy should be draped and immediately available in the room for any concurrent osseous procedures.
Step-by-Step Surgical Approach and Fixation Technique
The Approach and Sural Nerve Protection
The surgical approach requires a deliberate and meticulous technique. A curvilinear incision is utilized, beginning approximately 2 to 3 centimeters proximal to the tip of the lateral malleolus, situated midway between the posterior border of the fibula and the anterior border of the Achilles tendon. The incision is carried distally, curving gently around the lateral malleolus and extending toward the base of the fifth metatarsal, following the anatomical trajectory of the peroneal tendons.
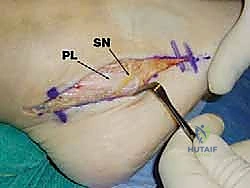
Deepening the incision through the subcutaneous fat must be performed with extreme caution. The sural nerve is the primary structure at risk. Using blunt dissection with a small hemostat or Metzenbaum scissors, the nerve is identified as it courses obliquely across the operative field, typically accompanied by the small saphenous vein. Once identified, the nerve is gently mobilized and protected with a vessel loop. Retraction of the nerve should be minimal and strictly intermittent to prevent traction neuropraxia. The deep fascia is then identified, revealing the Superior Peroneal Retinaculum (SPR) and the underlying peroneal tendon sheath.
Sheath Excision and Tendon Debridement
The SPR and the common peroneal tendon sheath are incised longitudinally, directly over the tendons. It is imperative to leave a 2 to 3-millimeter cuff of the SPR attached to the fibula to facilitate robust anatomical repair during closure. Upon opening the sheath, inflammatory tenosynovium is often encountered and must be meticulously debrided using a combination of sharp dissection and a rongeur. This tenosynovectomy allows for a comprehensive 360-degree inspection of both the peroneus brevis and longus tendons.

The tendons are systematically evaluated for longitudinal splits, fraying, and areas of severe tendinosis. The peroneus brevis is most commonly torn, frequently exhibiting a classic "C-shaped" or longitudinal split configuration as it wraps around the fibula. The peroneus longus is inspected down to the level of the cuboid groove. The surgical decision-making matrix at this juncture is dictated by the "Rule of 50%."
If less than 50% of the cross-sectional area of the tendon is compromised by the tear or degenerative tissue, the diseased portion is sharply excised. The remaining healthy tendon is then tubularized. Tubularization is performed using a continuous running or interrupted suture technique with a non-absorbable or slowly absorbable monofilament suture (e.g., 3-0 Prolene or PDS), burying the knots within the tendon substance to minimize postoperative friction.

Advanced Reconstruction and Groove Deepening
If the intraoperative assessment reveals that greater than 50% of the tendon's cross-sectional area is non-viable or irreparably torn, simple tubularization is insufficient and will likely lead to structural failure. In these severe cases, a tenodesis is indicated. The diseased segment of the affected tendon (usually the brevis) is resected, and the proximal and distal stumps are tenodesed (sutured) to the adjacent, intact peroneal tendon (usually the longus) in a side-to-side fashion. This is performed with the foot held in neutral dorsiflexion and slight eversion to ensure appropriate resting tension. In rare instances where both tendons are catastrophically damaged, an allograft reconstruction (e.g., semitendinosus or gracilis) or a local tendon transfer (e.g., flexor hallucis longus) may be required.
Following tendon repair or reconstruction, the osseous morphology must be addressed. If the fibular retromalleolar groove is flat or convex, a groove deepening procedure is mandatory to prevent recurrent subluxation. This is typically performed via a cortical window technique. A sagittal saw and osteotomes are used to elevate a rectangular osteochondral flap from the posterior fibula. The underlying cancellous bone is curetted or burred away, and the cortical flap is gently tamped back into place, creating a deep, concave trough. Finally, the tendons are reduced into the newly deepened groove, and the SPR is meticulously repaired over them using heavy non-absorbable sutures or suture anchors placed into the posterolateral fibula, ensuring the tendons glide smoothly without impingement or subluxation during dynamic ankle range of motion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, peroneal tendon repair and reconstruction carry a distinct profile of potential complications. The surgeon must be prepared to identify and manage these adverse events promptly to optimize patient outcomes. Sural nerve injury remains the most feared and frequently litigated complication. The incidence of sural neuritis or neuroma formation ranges from 5% to 9% in the literature. This can result from direct transection, aggressive traction, or entrapment in postoperative scar tissue. Management of a symptomatic neuroma often requires surgical exploration, neuroma excision, and burying the proximal nerve stump deep within the muscular belly of the lateral compartment to prevent recurrent surface irritation.
Recurrent tearing or persistent subluxation of the peroneal tendons occurs in approximately 3% to 5% of cases. This catastrophic failure is most commonly attributed to technical errors during the index procedure, such as failing to recognize and deepen a convex fibular groove, inadequate repair of the SPR, or, critically, failing to address an underlying cavovarus hindfoot deformity. A lateralizing calcaneal osteotomy is often required in the salvage setting to mechanically offload the lateral compartment.
Postoperative stiffness and tendon adhesions are common, particularly if the period of postoperative immobilization is excessively prolonged. Extensive tenosynovectomy and sheath reconstruction inherently create a pro-fibrotic environment. Patients may complain of a pulling sensation or limited inversion. Aggressive, early physical therapy is the primary preventative measure. In refractory cases, arthroscopic or open tenolysis may be indicated to liberate the tendons from dense scar tissue.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Sural Neuritis / Neuroma | 5% - 9% | Iatrogenic traction, entrapment in scar, direct transection. | Gabapentinoids, diagnostic blocks; surgical excision and burying of proximal stump. |
| Recurrent Tear / Subluxation | 3% - 5% | Missed cavovarus deformity, inadequate SPR repair, flat fibular groove. | Revision surgery: Groove deepening, SPR reconstruction with tissue anchors, calcaneal osteotomy. |
| Tendon Adhesions / Stiffness | 10% - 15% | Prolonged immobilization, excessive bleeding/scarring. | Aggressive physical therapy; open or tendoscopic tenolysis if refractory >6 months. |
| Wound Dehiscence / Infection | 2% - 4% | Poor soft tissue envelope, diabetes, smoking, PAD. | Local wound care, oral/IV antibiotics; surgical debridement and delayed closure if deep. |
Phased Post-Operative Rehabilitation Protocols
The success of peroneal tendon reconstruction is inextricably linked to a rigorous, phased postoperative rehabilitation protocol. The delicate balance between protecting the surgical repair and preventing debilitating adhesions dictates the timeline of recovery. The protocol is generally divided into four distinct phases, tailored to the specific extent of the surgical intervention (e.g., simple tubularization versus complex tenodesis with groove deepening).
Phase I: Maximum Protection (Weeks 0-2)
Immediately postoperatively, the patient is placed in a well-padded, short-leg plaster splint with the ankle immobilized in slight equinus and eversion. This position minimizes tension on the repaired tendons and the SPR. The patient is strictly non-weight-bearing (NWB) on the operative extremity, utilizing crutches or a knee scooter. Strict elevation above the level of the heart is mandated to control edema and facilitate optimal wound healing. At the two-week mark, sutures are removed, and the surgical site is inspected.
Phase II: Controlled Mobilization (Weeks 2-6)
Following suture removal, the patient is transitioned into a controlled ankle motion (CAM) boot. Weight-bearing status is gradually advanced. For isolated tendon repairs, partial weight-bearing may commence at week 3, progressing to weight-bearing as tolerated (WBAT) by week 4 to 6. If a groove deepening or osteotomy was performed, NWB status is maintained for a full 4 to 6 weeks to allow for osseous integration. Crucially, early active and passive range of motion (ROM) exercises are initiated during this phase. Therapy focuses on sagittal plane motion (plantarflexion and dorsiflexion) to prevent adhesions, while strictly avoiding active eversion and passive inversion, which place direct stress on the healing repair.
Phase III: Strengthening and Proprioception (Weeks 6-12)
Once clinical healing is evident and the patient is comfortably WBAT in the CAM boot, weaning into a supportive lace-up ankle brace begins. Physical therapy intensifies, introducing isometric eversion strengthening and progressing to isotonic exercises using resistance bands. Proprioceptive training is a cornerstone of this phase, utilizing balance boards and unstable surfaces to retrain the neuromuscular feedback loop of the lateral ankle dynamic stabilizers. Gait training focuses on normalizing the heel-to-toe mechanics and restoring the functional medial arch support provided by the peroneus longus.
Phase IV: Return to Sport and Advanced Function (Months 3-6+)
The final phase focuses on sport-specific or occupation-specific functional restoration. Plyometric exercises, lateral agility drills, and running progressions are introduced. Return to full, unrestricted athletic competition is typically permitted between 4 and 6 months postoperatively, contingent upon the patient demonstrating symmetrical ankle ROM, at least 90% eversion strength compared to the contralateral limb, and the ability to perform dynamic, multi-directional movements without pain or apprehension.
Summary of Landmark Literature and Clinical Guidelines
The evolution of peroneal tendon surgery is heavily informed by several landmark anatomical and clinical studies that have shaped modern orthopedic guidelines. The foundational understanding of peroneal tendon pathology is rooted in the classification systems developed by Krause and Brodsky, which categorize tears based on the degree of tendon involvement and guide the surgical algorithm (e.g., tubularization for <50% involvement versus tenodesis for >50%).
A critical paradigm shift in the literature has been the recognition of the fibular retromalleolar groove's morphology. Titley and colleagues definitively demonstrated the high prevalence of flat or convex fibular grooves in patients with recurrent subluxation. Current clinical consensus, supported by numerous retrospective cohorts, strongly advocates for prophylactic groove deepening in conjunction with SPR repair for any patient exhibiting instability, as isolated soft-tissue repair is associated with unacceptably high recurrence rates.
Furthermore, the biomechanical studies by Philbin and colleagues have elucidated the intricate relationship between hindfoot alignment and peroneal tendon stress. Their work underscores the modern clinical guideline that isolated peroneal tendon repair in the setting of an uncorrected cavovarus foot is an incomplete procedure destined for failure. Consequently, current literature mandates a holistic approach, frequently combining peroneal tendon reconstruction with lateralizing calcaneal osteotomies, dorsiflexing first metatarsal osteotomies, or lateral ligamentous reconstruction (e.g., modified Broström-Gould) to ensure a biomechanically sound and durable surgical outcome. Mastery of these literature-driven principles is essential for any surgeon undertaking the complex reconstruction of the lateral ankle.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding repair-of-peroneal-tendon-tears