Masterclass: Surgical Repair of Dislocating Peroneal Tendons with Indirect Fibular Groove Deepening

Key Takeaway
This masterclass provides an exhaustive, real-time guide to surgical repair of dislocating peroneal tendons. We cover essential anatomy, meticulous preoperative planning, precise intraoperative steps for indirect fibular groove deepening, and critical pearls to navigate potential pitfalls. Fellows will gain a deep understanding of technique, rationale, and comprehensive postoperative management, ensuring successful outcomes for chronic peroneal instability.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are addressing a fascinating, highly nuanced, and frequently mismanaged pathology: chronic dislocating peroneal tendons. This masterclass will focus specifically on the surgical repair of this condition utilizing the indirect fibular groove deepening technique. This intervention is not merely an exercise in repositioning aberrant tendinous structures; it is a critical restorative procedure aimed at re-establishing the intricate biomechanics of the lateral ankle complex, thereby preventing long-term disability, chronic pain, and progressive tendinopathic degeneration. Our ultimate objective is to provide a dynamically stable, pain-free ankle capable of withstanding the extreme physiological loads demanded by both activities of daily living and high-level athletics.
Peroneal tendon subluxation or frank dislocation from the retrofibular groove remains a relatively rare but profoundly significant etiology of lateral ankle pain. The true incidence is likely underreported, as the acute injury often masquerades as, or is misdiagnosed as, a simple lateral ankle sprain involving the anterior talofibular ligament (ATFL). This diagnostic oversight allows the initial acute injury to evolve into the chronic instability we are addressing today. When the superior peroneal retinaculum (SPR) fails to heal in an anatomically competent position, the tendons are permitted to translate anteriorly over the lateral malleolus during active eversion and dorsiflexion, establishing a vicious cycle of mechanical attrition and progressive tissue failure.
The pathogenesis of this condition is deeply rooted in the specific biomechanical forces applied to the ankle joint during trauma. The classic mechanism of injury involves a sudden, forceful dorsiflexion of the ankle coupled with a violent, maximal contraction of the peroneal musculature. This specific kinematic profile is frequently encountered in activities such as Alpine skiing, where the tip of the ski catches, forcing the ankle into extreme dorsiflexion while the skier actively attempts to correct their balance. Similarly, springboard diving, gymnastics, and American football present high-risk environments for this injury pattern. Alternatively, a mechanism involving resisted plantarflexion and inversion, while the peroneals are actively contracting to stabilize the hindfoot, can also precipitate subluxation. This latter mechanism is often intimately associated with concomitant lateral ankle ligamentous instability, complicating both the clinical picture and the surgical decision-making process.
Understanding the natural history of peroneal tendon instability is paramount for the treating orthopedic surgeon. If accurately diagnosed in the acute setting, conservative management—consisting of manual reduction followed by strict immobilization in a short-leg cast with the ankle in slight plantarflexion and inversion for four to six weeks—can yield successful outcomes in approximately fifty percent of cases. However, due to the aforementioned high rates of misdiagnosis, patients frequently present in the chronic phase. In these delayed presentations, recurrent subluxation and chronic dislocation are the norm. The repetitive mechanical friction of the tendons translating over the sharp posterior ridge of the fibula inevitably leads to profound tendinopathy, longitudinal split tears (particularly of the peroneus brevis), and eventual functional incompetence of the lateral compartment.
Detailed Surgical Anatomy and Biomechanics
Before we make our incision, we must possess an encyclopedic understanding of the lateral ankle's architectural blueprint. The surgical anatomy dictates our approach, our potential complications, and ultimately, our success.
Musculotendinous Architecture and Zonal Anatomy
The peroneus longus and brevis are the two primary dynamic stabilizers of the lateral ankle, both taking their origin from the proximal and middle thirds of the lateral fibular shaft. As these muscle bellies course distally, they transition into tendinous structures and share a common synovial sheath proximal to the distal tip of the fibula. The spatial relationship between these two tendons is critical: the peroneus brevis tendon lies directly against the posterior surface of the distal fibula, positioned anterior and medial to the peroneus longus tendon. This anatomical arrangement explains why the peroneus brevis is disproportionately subjected to mechanical shear and split tears when the complex subluxates over the fibular ridge.
Distal to the fibula, the common sheath bifurcates, and each tendon enters its own distinct synovial sheath, physically separated by the peroneal tubercle on the lateral wall of the calcaneus. The peroneus brevis continues distally to insert onto the base of the fifth metatarsal, serving as a powerful evertor and secondary plantarflexor. The peroneus longus, however, takes a sharp turn at the cuboid groove, traversing the plantar aspect of the midfoot to insert onto the base of the first metatarsal and the medial cuneiform, playing a vital role in plantarflexing the first ray and stabilizing the medial longitudinal arch.
To systematically evaluate and treat pathology, we divide the peroneal tendons into three distinct anatomical zones. Zone I encompasses the retrofibular groove and is the most common site of pathology in chronic dislocations. As the tendons sublux, the brevis is forcefully compressed against the sharp posterolateral bony ridge by the overlying longus, leading to longitudinal split tears. Zone II is located between the distal tip of the fibula and the cuboid tunnel, often associated with peroneal tubercle hypertrophy. Zone III is located within the cuboid tunnel itself, primarily involving the peroneus longus and occasionally a painful, fragmented os peroneum.
The Retrofibular Groove and Osseous Morphology
The retrofibular groove, situated on the posterior surface of the distal fibula, serves as the primary osseous restraint for the peroneal tendons. This groove is lined with a specialized layer of fibrocartilage that facilitates smooth, frictionless gliding of the tendons during ankle range of motion. The morphological characteristics of this groove—specifically its depth, width, and contour—are highly variable among individuals and play a massive role in the predisposition to instability.
Anatomical studies have demonstrated that a distinct, concave groove is present in approximately 80% of the population. In the remaining 20%, the posterior surface of the fibula is entirely flat or, pathologically, even convex. Patients with a flat or convex fibular morphology are at a substantially elevated risk for peroneal tendon instability, as the osseous constraint is inherently deficient. This anatomical variance is the primary rationale for the fibular groove deepening procedure we will perform today.
Furthermore, a critical structure known as the fibrocartilage rim is located on the posterolateral border of the fibula. This rim acts as an extension of the osseous groove, effectively deepening the sulcus by an additional 2 to 4 millimeters. During acute traumatic dislocations, this fibrocartilage rim is frequently avulsed or attenuated, drastically reducing the effective depth of the groove and contributing to chronic instability even if the superior peroneal retinaculum is surgically repaired.

The Superior Peroneal Retinaculum and Pathoanatomic Classification
The Superior Peroneal Retinaculum (SPR) is the primary soft-tissue restraint preventing lateral and anterior translation of the peroneal tendons. It is a distinct band of deep fascia that is continuous with the periosteum of the distal fibula. Crucially, the SPR typically does not attach directly to the fibrocartilage rim or the posterolateral edge of the bone itself, but rather to the periosteum slightly anterior to the ridge. The width, thickness, and insertional footprint of the SPR are highly variable, with multiple distinct anatomical patterns described in the literature. The most common configuration involves a bifurcated insertion, sending bands to both the Achilles tendon sheath and the lateral wall of the calcaneus.
The fiber orientation of the SPR is generally parallel to the calcaneofibular ligament (CFL). This parallel alignment is of immense clinical significance, as it explains why severe inversion injuries—which classically rupture the ATFL and CFL—can simultaneously place immense tensile stress on the SPR, leading to concomitant peroneal tendon instability.

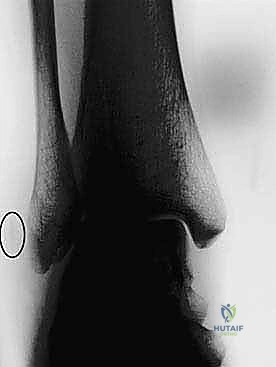
Peroneal dislocations are formally classified by Eckert and Davis into three distinct grades based on the specific pathoanatomy observed at the time of surgical exploration. Grade I injuries involve the SPR being stripped directly off the fibular periosteum, allowing the tendons to dislocate anteriorly beneath the retinaculum. Grade II injuries involve the avulsion of the fibrous rim from the posterolateral aspect of the fibula along with the SPR. Grade III injuries are characterized by a frank bony avulsion fracture of the posterolateral fibular rim attached to the SPR, frequently visible on radiographs as the pathognomonic "fleck sign." Later, Oden added a Grade IV classification, describing a posterior tear of the SPR with the tendons dislocating superficial to the retinaculum, though this remains exceedingly rare.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for dislocating peroneal tendons must be carefully weighed, taking into account the chronicity of the injury, the patient's functional demands, and the presence of concomitant pathology.
Surgical management is absolutely indicated for patients presenting with chronic, symptomatic peroneal tendon subluxation or dislocation that has failed a dedicated trial of conservative management. These patients typically report pain, a subjective feeling of instability, and a palpable or audible snapping sensation over the lateral malleolus during activities. Furthermore, surgical intervention is indicated when advanced imaging (MRI or Ultrasound) reveals significant intrasubstance tearing, particularly longitudinal split tears of the peroneus brevis, which will not heal without mechanical debridement, tubularization, and restoration of a stable gliding environment.
In the acute setting, the indications for surgery are more nuanced. While conservative management can be attempted in the general population, acute primary surgical repair is increasingly recommended for elite, high-demand athletes. Early surgical stabilization in this demographic minimizes the risk of recurrent instability, prevents the development of secondary tendinopathy, and often allows for a more predictable and accelerated return to competitive play. Additionally, the presence of a Grade III injury (bony avulsion or "fleck sign") with significant displacement may warrant acute surgical fixation to restore the osseous anatomy of the fibular groove.
Contraindications to the indirect fibular groove deepening and SPR repair are standard for most elective orthopedic procedures but require strict adherence. Active local or systemic infection is an absolute contraindication. Severe peripheral vascular disease that compromises the healing potential of the lateral ankle soft tissue envelope precludes surgical intervention, as the risk of catastrophic wound breakdown outweighs the benefits of tendon stabilization. Relative contraindications include poorly controlled diabetes mellitus, heavy tobacco use (which significantly increases the risk of wound complications and delayed healing), and patients who are functionally non-ambulatory or unable to comply with the rigorous post-operative rehabilitation protocol.
| Category | Specific Indications | Specific Contraindications |
|---|---|---|
| Clinical Presentation | Chronic symptomatic subluxation/dislocation; Failed conservative therapy (4-6 weeks cast/boot); Persistent lateral ankle pain with dynamic snapping. | Asymptomatic subluxation (incidental finding); Medically unfit for anesthesia; Non-ambulatory patient status. |
| Pathoanatomic Findings | Concomitant peroneus brevis/longus split tears; Shallow or convex retrofibular groove; Grade III Eckert & Davis avulsion fractures. | Severe, end-stage degenerative joint disease of the ankle/subtalar joint (requires fusion rather than isolated soft tissue repair). |
| Patient Factors | High-demand elite athletes (acute setting); Patients with high functional requirements for eversion strength. | Active soft tissue infection over the lateral malleolus; Severe peripheral vascular disease; Non-compliance with post-op protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful surgical outcome. This begins with a comprehensive clinical evaluation and is heavily augmented by advanced imaging modalities.
Clinical Evaluation and Diagnostic Maneuvers
Our patient today presents with chronic symptoms, a hallmark of delayed diagnosis. The classic historical narrative involves a vague, deep posterolateral ankle pain that radiates proximally along the fibular shaft, frequently accompanied by a distinct popping or snapping sensation during dynamic activity. A detailed history often reveals an initial trauma involving forced dorsiflexion with a lateral ankle "pop," or a history of recurrent inversion-supination sprains leading to chronic lateral ankle instability.
On physical examination, we meticulously palpate the lateral compartment. We look for fullness and diffuse tenderness along the course of the peroneal tendons, which is highly indicative of underlying tendinopathy and tenosynovitis. Localized, pinpoint tenderness directly over the posterior ridge of the fibula strongly raises the index of suspicion for an attritional peroneus brevis split tear. Assessing muscle strength is critical; pain elicited with an inversion stretch or active resisted eversion confirms tendon involvement. However, profound weakness of active eversion in the absence of significant pain should immediately raise a red flag for a complete, retracted tendon rupture, which completely alters the surgical algorithm.
Dynamic diagnostic maneuvers are essential. The Peroneal Tunnel Compression Test is performed by having the patient execute active eversion against manual resistance while the examiner firmly palpates the posterior border of the fibula. In cases of instability, this maneuver frequently elicits palpable snapping, audible popping, and sharp pain as the tendons subluxate. Furthermore, dynamic observation during active circumduction of the ankle—specifically transitioning from plantarflexion/inversion to dorsiflexion/eversion—may demonstrate visible, frank dislocation of the tendons anterior to the fibula, with spontaneous relocation upon returning to plantarflexion.


Advanced Imaging Modalities
Plain radiography remains the initial imaging step. Standard anteroposterior, mortise, and lateral views of the ankle are essential to rule out occult fractures, malalignments, or large osteochondral defects of the talar dome. The surgeon must meticulously scrutinize the lateral and mortise views for the "fleck sign"—a small, thin avulsion fracture off the posterolateral ridge of the distal fibula. This finding is pathognomonic for a Grade III SPR avulsion injury. Because this fracture fragment can be exceedingly subtle, a "hot lamp" or digital windowing is often required for definitive visualization.
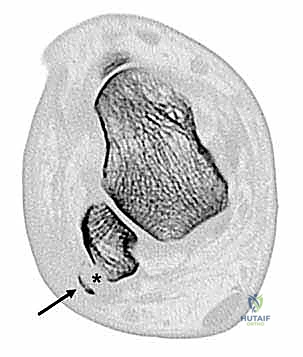
Computed Tomography (CT) is an invaluable adjunct, particularly when the diagnosis remains equivocal or when precise osseous mapping is required. Axial CT slices provide definitive, high-resolution visualization of the retrofibular groove's morphology, allowing the surgeon to accurately quantify the degree of convexity or concavity. CT is also highly sensitive for detecting small, non-displaced avulsion fractures that may be obscured on plain radiographs. In cases of chronic dislocation, axial CT can definitively capture the tendons residing anterior to the fibular ridge.
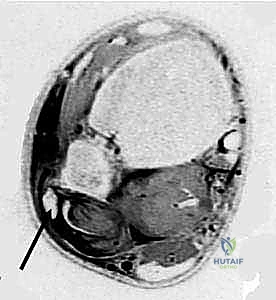
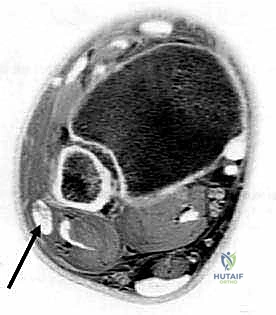
Magnetic Resonance Imaging (MRI) is the gold standard for comprehensive soft tissue assessment. It provides unparalleled visualization of the SPR's integrity, identifying attenuation, stripping, or frank rupture. MRI exquisitely details the health of the tendons themselves, readily identifying tenosynovitis, intrasubstance degeneration, and the presence, length, and severity of longitudinal split tears. Finally, dynamic Ultrasound, while heavily operator-dependent, offers the unique advantage of real-time, dynamic evaluation. It allows the clinician to visualize the tendons subluxating under provocative maneuvers in the clinic, confirming the diagnosis when static imaging is inconclusive.
Patient Positioning and Operating Room Setup
For this procedure, optimal patient positioning is the lateral decubitus position. The patient is placed on a well-padded bean bag, ensuring all bony prominences (particularly the contralateral peroneal nerve at the fibular head) are meticulously protected. The operative leg is positioned upward, and the hip and knee are slightly flexed to relax the tension on the sural nerve and the lateral anatomical structures.
A well-padded thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the delicate split tears of the peroneus brevis and safely mobilizing the sural nerve. The leg is prepped and draped in a standard sterile orthopedic fashion, allowing for full, unrestricted exposure from the proximal third of the leg down to the forefoot.
Fluoroscopy (C-arm) should be available in the operating room. While not strictly required for the soft tissue dissection, it is an invaluable tool for confirming drill trajectory and depth during the indirect fibular groove deepening phase, ensuring we do not inadvertently breach the anterior cortex or the distal tibiofibular syndesmosis. The surgical team must ensure all specialized instrumentation, including a small joint burr, curved tamps, and suture anchors (typically 4.5mm or smaller), are available on the back table prior to incision.
Step-by-Step Surgical Approach and Fixation Technique
We now move to the surgical intervention. The indirect fibular groove deepening technique is elegant because it preserves the native fibrocartilage gliding surface of the retrofibular groove, unlike older, direct-burring techniques that left raw, bleeding bone exposed to the tendons, resulting in severe postoperative adhesions.
Soft Tissue Dissection and Tendon Exposure
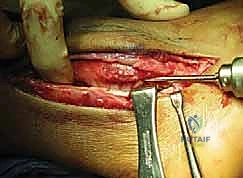
A longitudinal, slightly curved incision is made along the posterior border of the distal fibula, extending from approximately 5 centimeters proximal to the tip of the lateral malleolus down to the level of the peroneal tubercle on the calcaneus. The incision should be placed slightly posterior to the fibula to avoid placing the final skin closure directly over the bony prominence, which can lead to painful shoe wear.
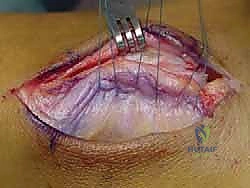
Blunt dissection is carried through the subcutaneous tissues. Meticulous hemostasis is maintained using bipolar electrocautery. The most critical structure to identify and protect during this superficial dissection is the sural nerve. The sural nerve typically courses posterior to the peroneal tendons, crossing the lateral border of the Achilles tendon before traveling distally along the lateral aspect of the foot. Its anatomical course is variable; therefore, gentle spreading with tenotomy scissors is mandatory until the nerve is visualized, mobilized, and gently retracted posteriorly with a vessel loop.
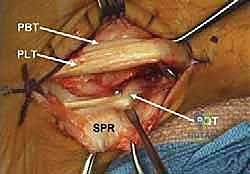
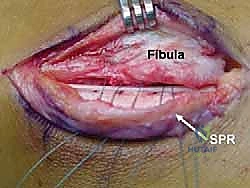
Once the subcutaneous tissues are cleared, the Superior Peroneal Retinaculum (SPR) is identified. In chronic cases, the SPR is often thickened, attenuated, or entirely stripped off the fibula, forming a redundant pseudo-pouch anteriorly. The SPR is sharply incised longitudinally, leaving a 2 to 3-millimeter cuff of tissue attached to the fibular periosteum to facilitate later repair. The peroneal tendon sheath is opened, and the tendons are delivered from the retrofibular groove for thorough inspection.

Tendon Inspection and Management of Intrasubstance Pathology
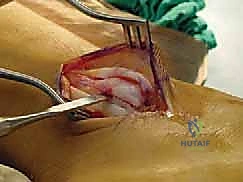
With the tendons exposed, we perform a systematic, 360-degree inspection of both the peroneus longus and brevis. We evaluate for tenosynovitis, which, if present, is addressed with a meticulous tenosynovectomy using a rongeur or scalpel, taking care to preserve the underlying epitenon.
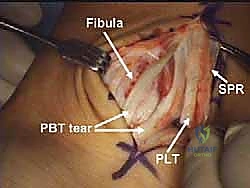
The peroneus brevis is critically evaluated for longitudinal split tears, which are present in a significant majority of chronic dislocation cases. These tears occur as the brevis is crushed between the fibular ridge and the overlying longus tendon. If a split tear is identified, the surgical management depends on the percentage of viable tendon remaining. If less than 50% of the cross-sectional area is involved, the degenerative portion is sharply excised, and the remaining healthy tendon is tubularized using a running, locking 3-0 non-absorbable suture.
If the split tear involves more than 50% of the tendon substance, simple debridement may leave the tendon functionally incompetent. In these severe cases, the degenerative tissue is excised, and the proximal and distal stumps of the brevis are tenodesed to the intact peroneus longus tendon (side-to-side tenodesis) using robust, non-absorbable figure-of-eight sutures. The peroneus longus is also inspected; while less commonly torn, any pathology here is addressed in a similar fashion. Once the tendons are repaired and tubularized, they are temporarily retracted anteriorly to expose the retrofibular groove.
Indirect Fibular Groove Deepening Procedure
This is the crux of the masterclass: the indirect deepening of the fibular groove. The goal is to create a deep, concave sulcus while absolutely preserving the native posterior fibrocartilage. We begin by identifying the distal tip of the fibula. Using a 3.2mm drill bit, a tunnel is created starting at the distal tip of the fibula, directing the drill proximally along the longitudinal axis of the fibular shaft for a distance of approximately 3 to 4 centimeters. The drill must remain entirely within the cancellous bone of the fibula, staying parallel to the posterior cortex. Fluoroscopy can be utilized here to confirm the trajectory and prevent cortical breach.


Once the longitudinal tunnel is established, we use a curette or a small motorized burr to carefully hollow out the cancellous bone immediately deep to the posterior cortex of the fibula. We are essentially creating a hollow void beneath the retrofibular groove. Extreme care must be taken not to violate the posterior cortical wall or the articular cartilage of the syndesmosis medially.
With the cancellous void created, we take a curved bone tamp and a mallet. The tamp is placed gently against the intact posterior cortex of the fibula (the floor of the retrofibular groove). With controlled, precise strikes of the mallet, the posterior cortex is impacted anteriorly into the previously created cancellous void. Because the cortex in this region is relatively thin and flexible, it will hinge and collapse inward without fracturing completely, effectively deepening the groove by several millimeters.
The result is a profoundly deepened, concave osseous tunnel that is still lined by pristine, native fibrocartilage. We then reduce the repaired peroneal tendons back into this newly deepened groove. We dynamically test the stability by taking the ankle through a full range of motion, specifically forceful dorsiflexion and eversion. The tendons should now sit deeply within the sulcus without any tendency to subluxate over the lateral ridge.

Superior Peroneal Retinaculum Reconstruction and Closure
While the osseous deepening provides the primary mechanical block, a robust soft-tissue repair of the SPR is mandatory to complete the stabilization. If the native SPR is robust and a sufficient fibular cuff was preserved, a direct, pants-over-vest repair is performed using #2-0 non-absorbable braided sutures. The posterior leaf of the SPR is advanced and sutured to the anterior fibular periosteal cuff, ensuring appropriate tension.
In cases where the SPR is
Clinical & Radiographic Imaging Archive


