Ponseti Method for Congenital Talipes Equinovarus: An Intraoperative Masterclass

Key Takeaway
This masterclass provides an exhaustive, real-time guide to the Ponseti method for congenital clubfoot. Fellows will learn intricate anatomical considerations, precise manipulation techniques, and serial casting application. We'll cover percutaneous Achilles tenotomy, crucial pearls and pitfalls, and long-term postoperative management, ensuring comprehensive understanding of this gold-standard treatment for talipes equinovarus.
Comprehensive Introduction and Patho-Epidemiology
Congenital talipes equinovarus, universally recognized as clubfoot, represents one of the most complex and historically challenging pediatric orthopaedic deformities. The Ponseti method has revolutionized the management of this condition, shifting the paradigm from extensive, complication-prone surgical releases to an elegant, biomechanically sound, and minimally invasive approach. This definitive chapter elucidates the intricate anatomical principles, precise manipulative techniques, and rigorous bracing protocols that constitute the Ponseti method. Mastery of this technique is not merely an exercise in plaster application; it demands a profound comprehension of infantile foot kinematics, the pathophysiology of fibroplasia, and the spatial relationships of the tarsal bones during sequential correction.
The global incidence of idiopathic clubfoot is approximately 1 to 2 per 1,000 live births, with a notable male predominance (ratio of 2:1) and bilateral involvement occurring in nearly 50% of cases. While the precise etiology remains a subject of ongoing investigation, contemporary evidence suggests a multifactorial origin involving a complex interplay of genetic susceptibility and environmental factors. Histological studies of the medial and posterior ligamentous structures reveal an abundance of densely packed collagen fibers and an increased presence of myofibroblasts, suggesting a transient, localized fibroplasia. This fibrotic process leads to the severe contractures characteristic of the deformity, tethering the calcaneus, navicular, and cuboid in severe medial and plantar deviation relative to the talus.
The pathognomonic presentation of clubfoot is encapsulated by the acronym CAVE, representing the four primary components of the deformity: Cavus, Adductus, Varus, and Equinus. Cavus, the abnormally high longitudinal arch, is primarily driven by the severe plantarflexion of the first ray relative to the hindfoot. Adductus refers to the medial deviation of the forefoot and midfoot, driven by the medial subluxation of the navicular on the talar head. Varus describes the inversion of the hindfoot, where the calcaneus is rigidly locked in an inverted position beneath the talus. Finally, Equinus is the fixed plantarflexion of the ankle joint, predominantly caused by a severely contracted Achilles tendon and posterior ankle capsule. Left uncorrected, the child will bear weight on the dorsolateral aspect of the foot, leading to severe gait abnormalities, early-onset osteoarthritis, and profound functional disability.

Understanding the temporal progression of these fibrotic changes is critical for the timing of intervention. The viscoelastic properties of the infantile ligaments and joint capsules are highly responsive to the mechanical stress applied during the first few weeks of life. The Ponseti method capitalizes on this unique window of biological plasticity, utilizing serial manipulations to induce stress-relaxation and creep within the contracted tissues. This biological remodeling, guided by precise mechanical forces, allows for the gradual restoration of normal tarsal alignment without the need for destructive surgical incisions that inevitably lead to joint stiffness and degenerative changes in adulthood.
Detailed Surgical Anatomy and Biomechanics
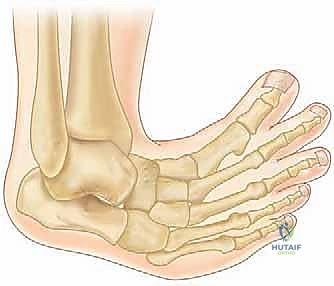
A rigorous understanding of the altered osteology and soft tissue tethering in the clubfoot is the absolute prerequisite for successful manipulation. The deformity is not a simple planar deviation but a complex, three-dimensional malalignment of the tarsal bones, primarily centered around the subtalar joint complex (talocalcaneonavicular joint). In the clubfoot, the talus is in severe equinus and its neck is medially deviated. However, the most critical concept to grasp is that the talus is the only bone that remains within the ankle mortise; the rest of the foot (calcaneus, navicular, and cuboid) rotates rigidly as a single unit around the talus.
The calcaneus in a clubfoot is severely inverted (varus), plantarflexed (equinus), and internally rotated beneath the talus. The anterior tuberosity of the calcaneus is positioned directly beneath the head of the talus, rather than lateral to it. This internal rotation of the calcaneus is the primary driver of the hindfoot varus. The navicular is profoundly medially displaced, often articulating with the medial aspect of the talar neck rather than the articular surface of the talar head. This leaves the lateral aspect of the talar head prominent and palpable beneath the skin. Similarly, the cuboid is medially displaced on the anterior calcaneus.

The soft tissue anatomy is characterized by profound contractures of the posteromedial structures. The Achilles tendon is universally foreshortened and thickened, acting as the primary tether preventing ankle dorsiflexion. The posterior tibialis tendon, flexor digitorum longus, and flexor hallucis longus are also contracted, contributing to the varus and equinus. The master knot of Henry, where the flexor tendons cross, is often tight and drawn proximally. Ligamentous contractures are severe, particularly involving the posterior talofibular ligament, the calcaneofibular ligament, the deep deltoid ligament, the talonavicular ligament (spring ligament), and the bifurcate ligament. The plantar fascia and intrinsic plantar musculature are also contracted, maintaining the cavus deformity.
Neurovascular considerations are paramount, particularly when planning the percutaneous Achilles tenotomy. The medial neurovascular bundle, containing the posterior tibial artery and the tibial nerve, lies immediately posterior to the medial malleolus and the contracted flexor tendons. The anatomy is distorted, and these structures may be pulled closer to the Achilles tendon than in a normal foot. Furthermore, vascular anomalies are highly prevalent in idiopathic clubfoot. Angiographic and Doppler studies have demonstrated that the anterior tibial artery is absent or severely hypoplastic in up to 85% of affected limbs. Consequently, the vascular supply to the foot is often heavily reliant on the posterior tibial and peroneal arteries, making the preservation of the medial neurovascular bundle during intervention absolutely critical.
Exhaustive Indications and Contraindications
The Ponseti method is universally recognized as the gold standard for the initial management of almost all forms of congenital clubfoot. Its efficacy is highest when initiated within the first few weeks of life, capitalizing on the maximal viscoelasticity of the neonatal ligaments. Idiopathic clubfoot, occurring in an otherwise healthy infant without associated syndromic or neuromuscular abnormalities, is the primary indication. The method is highly successful in these cases, achieving complete correction of the deformity in over 90% of patients without the need for extensive surgical release.
However, the indications extend beyond the simple idiopathic presentation. The Ponseti method is also the first-line treatment for complex or atypical clubfeet. These variants present with a more rigid, severe deformity characterized by a deep transverse plantar crease, a deep posterior heel crease, severe equinus, and a short, stubby foot with a hyperextended first metatarsophalangeal joint. While standard manipulation techniques must be modified to prevent iatrogenic complications such as cast slippage or midfoot breaches, the foundational principles of serial casting remain applicable and effective. Furthermore, syndromic clubfeet (e.g., associated with arthrogryposis multiplex congenita, Larsen syndrome, or diastrophic dysplasia) and neurogenic clubfeet (e.g., associated with myelomeningocele) are also initially managed with the Ponseti method. Although the recurrence rates are higher and the number of casts required may be greater, initial non-operative management significantly reduces the complexity and extent of any subsequent surgical interventions.
Contraindications to the Ponseti method are exceedingly rare. Absolute contraindications are virtually non-existent in the neonatal period, provided the skin is intact and there are no severe, life-threatening comorbidities precluding cast application. Relative contraindications primarily revolve around delayed presentation or specific syndromic rigidities that fail to progress after an extended series of casts. While historically, older children (beyond 1-2 years of age) were considered poor candidates, contemporary evidence supports the use of modified Ponseti casting even in neglected or recurrent clubfeet in toddlers and older children, often delaying or minimizing the need for extensive bony procedures.
Table 1: Indications and Contraindications for the Ponseti Method
| Category | Specific Conditions | Clinical Considerations |
|---|---|---|
| Primary Indications | Idiopathic Congenital Talipes Equinovarus | Gold standard; >90% success rate; initiate within first weeks of life. |
| Expanded Indications | Complex/Atypical Clubfoot | Requires modified technique to prevent cast slippage; highly effective. |
| Expanded Indications | Syndromic Clubfoot (e.g., Arthrogryposis) | First-line treatment; may require more casts; reduces eventual surgical burden. |
| Expanded Indications | Neurogenic Clubfoot (e.g., Spina Bifida) | First-line treatment; careful monitoring for insensate skin breakdown is crucial. |
| Expanded Indications | Neglected/Delayed Presentation | Effective in older infants and toddlers; may require concurrent extensive soft tissue releases if casting plateaus. |
| Relative Contraindications | Active Skin Infection/Ulceration | Must resolve prior to casting to prevent severe soft tissue compromise. |
| Relative Contraindications | Severe Vascular Compromise | Requires careful assessment; tight casting may exacerbate ischemia. |
| Absolute Contraindications | None in the typical neonatal presentation | The method is universally attempted prior to considering surgical alternatives. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning in the context of the Ponseti method involves meticulous clinical assessment, classification of the deformity severity, and preparation of the clinical environment. The initial clinical examination is critical for establishing the baseline severity and distinguishing idiopathic clubfoot from postural deformities or syndromic associations. Postural clubfoot, which results from intrauterine crowding, presents with similar CAVE components but is fully correctable passively and does not exhibit the rigid fibrotic tethering of true clubfoot. A thorough physical examination must also evaluate the hips for developmental dysplasia (DDH), the spine for occult dysraphism, and the hands and face for syndromic features.
Objective assessment systems, most notably the Pirani score and the Dimeglio classification, are utilized to quantify the severity of the deformity and track progress throughout the casting phase. The Pirani score evaluates six clinical signs (three in the midfoot, three in the hindfoot), scoring each as 0 (normal), 0.5 (mildly abnormal), or 1 (severely abnormal). This provides a reliable, reproducible metric to communicate severity and predict the number of casts required, as well as the likelihood of requiring a percutaneous Achilles tenotomy. Documentation should include photographic records of the foot from multiple angles (anterior, posterior, medial, lateral, and plantar) prior to the initiation of treatment.



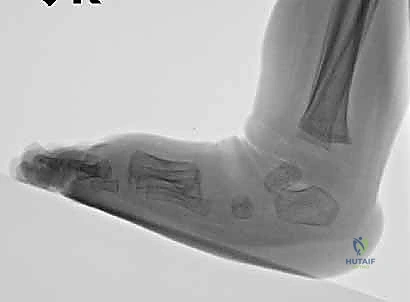
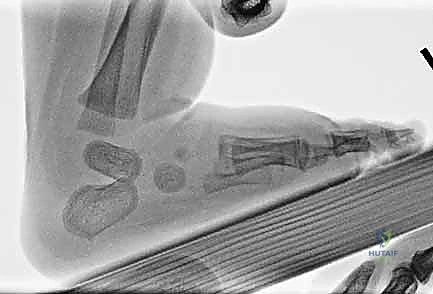
Standard radiographic evaluation is generally not indicated in the neonatal period. The tarsal bones, primarily the navicular and cuboid, are entirely cartilaginous at birth and do not possess ossific nuclei, rendering plain radiographs largely uninterpretable for assessing precise anatomical alignment. However, forced dorsiflexion lateral radiographs become a critical tool later in the treatment algorithm. Once the cavus, adductus, and varus have been corrected, and the clinician is assessing the need for an Achilles tenotomy, a lateral radiograph in maximal dorsiflexion can differentiate true ankle dorsiflexion from a spurious midfoot breach (rocker-bottom deformity). If the tibiocalcaneal angle remains in equinus despite apparent clinical dorsiflexion, a tenotomy is mandated.
Patient positioning and environmental control are essential for successful cast application. The procedure is typically performed in an outpatient clinic setting. The infant should be relaxed; utilizing a pacifier dipped in sucrose solution, allowing the mother to breastfeed, or providing a bottle during the procedure significantly reduces infant distress and muscle guarding. The infant is positioned supine on the examination table. The surgeon stands at the foot of the table, while a skilled assistant stands opposite or to the side. The assistant's role is critical: they must hold the knee flexed at 90 degrees to relax the gastrocnemius, control the thigh, and assist in applying the plaster while the surgeon maintains the precise manipulative reduction.
Step-by-Step Surgical Approach and Fixation Technique
The Ponseti method is a highly choreographed sequence of manipulations and cast applications. The fundamental principle is the simultaneous correction of adductus, varus, and cavus by abducting the foot around the head of the talus, followed by the correction of equinus. Attempting to correct these components in isolation, or applying pressure to the wrong anatomical landmarks, will inevitably lead to failure and iatrogenic deformity.
Phase 1 Initial Manipulation and Cavus Correction
The first step in the Ponseti sequence is the correction of the cavus deformity. Cavus is driven by the plantarflexion of the first ray relative to the hindfoot. To correct this, the forefoot must be supinated. This is counterintuitive to many inexperienced practitioners who attempt to pronate the forefoot to correct the apparent clinical supination of the clubfoot. Pronating the forefoot actually exacerbates the cavus and locks the underlying tarsal pathology.




The surgeon locates the head of the talus, which is prominent on the dorsolateral aspect of the foot. The thumb of the stabilizing hand is placed firmly against the lateral aspect of the talar head. This is the fulcrum for all subsequent manipulations. The index finger of the stabilizing hand wraps around the medial malleolus. With the opposite hand, the surgeon grasps the forefoot, specifically elevating the first metatarsal to align it with the rest of the foot, effectively supinating the forefoot to match the supination of the hindfoot. This creates a normal longitudinal arch. The first cast is applied in this supinated position, with no attempt made to correct the adductus or equinus at this stage.
Phase 2 Abduction and Varus Correction
Once the cavus is corrected (usually after the first cast), the subsequent 3 to 4 casts focus on correcting the adductus and varus simultaneously. This is achieved through the principle of kinematic coupling in the subtalar joint. As the calcaneus is abducted (externally rotated) beneath the talus, it naturally everts, correcting the varus.




The surgeon again identifies the lateral head of the talus and applies counter-pressure with the thumb. The opposite hand grasps the forefoot and midfoot and gently abducts the entire foot around the talar head in a horizontal plane. The foot is held in maximal supination during this abduction. Crucially, the surgeon must never touch or apply pressure to the calcaneus or the lateral cuboid. Touching the calcaneus prevents it from abducting and everting, effectively blocking the correction. The abduction is continued until the foot reaches approximately 60 to 70 degrees of external rotation relative to the tibial axis. This gradual stretching of the medial soft tissues allows the navicular to glide laterally back over the talar head.
Phase 3 Percutaneous Achilles Tenotomy for Equinus
Equinus is the final component to be addressed. It is imperative that no attempt is made to dorsiflex the ankle until the foot is fully abducted (60-70 degrees) and the heel is in valgus or neutral. Attempting premature dorsiflexion will result in a midfoot break (rocker-bottom foot), as the rigid Achilles tendon will prevent hindfoot dorsiflexion, forcing the movement to occur through the midtarsal joints.



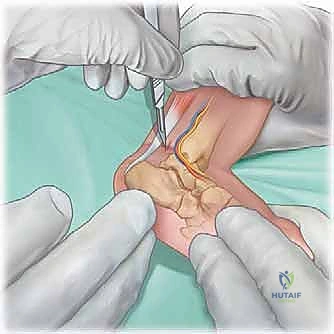
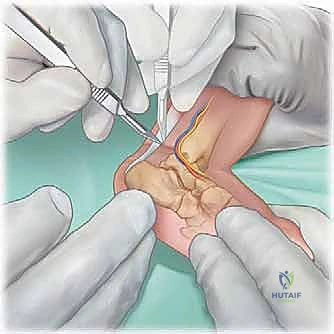
In over 80% to 90% of idiopathic cases, the Achilles tendon remains too tight to achieve the requisite 15 to 20 degrees of dorsiflexion, necessitating a percutaneous tenotomy. This is typically performed in the clinic under local anesthesia (EMLA cream and/or lidocaine infiltration) or in the operating room under brief sedation. The foot is prepped and draped. The surgeon palpates the tight Achilles tendon. A No. 15 or No. 11 scalpel blade is introduced parallel to the tendon, approximately 1.5 cm proximal to the calcaneal insertion, entering from the medial side to avoid the neurovascular bundle. The blade is rotated 90 degrees, and the tendon is sectioned from anterior to posterior while the foot is held in forced dorsiflexion. A distinct "pop" is felt, and immediate dorsiflexion of 15 to 20 degrees should be achievable.
Cast Application and Molding Principles
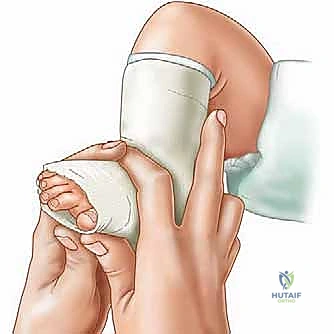
The application of the plaster cast is as critical as the manipulation itself. We utilize fast-setting plaster of Paris, as it allows for precise molding that cannot be achieved with fiberglass. The limb is heavily padded with cast padding, paying particular attention to the bony prominences (talar head, medial malleolus, heel).


The cast is applied in two stages. First, a short leg cast is applied while the surgeon maintains the precise manipulative position. The plaster is meticulously molded around the heel, the malleoli, and the arch, ensuring the heel is well-seated and the forefoot is appropriately supinated and abducted. The thumb pressure on the talar head is maintained until the plaster sets. Once the short leg portion is firm, the cast is extended above the knee to the proximal thigh, with the knee flexed at 90 degrees. This long-leg configuration is mandatory; it prevents the cast from slipping off the conical infant leg and controls tibial rotation, ensuring the abduction forces are transmitted to the foot and not dissipated through the knee. The final post-tenotomy cast is applied with the foot in 70 degrees of abduction and 15 degrees of dorsiflexion, and is left in place for 3 weeks to allow the tendon to heal in its lengthened state.




Complications, Incidence Rates, and Salvage Management
While the Ponseti method minimizes the severe complications associated with extensive surgical releases, technical errors in manipulation and casting can lead to significant iatrogenic issues. The most common pitfall is the development of a rocker-bottom foot (midfoot breach). This occurs when the clinician attempts to dorsiflex the foot against a tight Achilles tendon before achieving full abduction and heel eversion. The force bends the foot at the midtarsal joint, crushing the cartilaginous structures and creating a severe cavovarus deformity masked by apparent dorsiflexion. Management requires immediate removal of the cast, a period of rest to allow soft tissue recovery, and a return to phase 1 casting to re-establish the arch and correct the midfoot alignment prior to a proper tenotomy.
Cast slippage is another frequent complication, particularly in complex or atypical clubfeet, which possess a short, plantarflexed first ray and a severe equinus that creates a "slippery" conical shape. If a cast slips, the heel pulls up inside the plaster, causing pressure necrosis over the anterior ankle and exacerbating the equinus. To prevent this, the knee must be flexed to 90 degrees, and the plaster must be meticulously molded over the calcaneal tuberosity. If slippage occurs, the cast must be removed immediately, the skin assessed, and a modified casting technique (often utilizing a more acute knee flexion angle or specific complex clubfoot modifications) implemented.
Recurrence of the deformity is the most significant long-term challenge, occurring in up to 30% to 50% of cases, almost exclusively due to non-compliance with the post-operative bracing protocol. Recurrence typically presents with a loss of dorsiflexion (recurrent equinus) followed by a return of varus and adductus. Early recurrences are managed with a brief repeat course of serial casting (usually 2-3 casts) to regain the correction. If the child is over 2 to 3 years of age and presents with a dynamic supination deformity during gait (driven by an overactive tibialis anterior muscle), a Tibialis Anterior Tendon Transfer (TATT) to the lateral cuneiform is indicated. This procedure rebalances the foot biomechanics, converting a deforming supinatory force into a corrective dorsiflexion force, and is highly successful in preventing further relapse.
Table 2: Complications and Salvage Management
| Complication | Incidence Rate | Etiology / Mechanism | Salvage / Management Strategy |
|---|---|---|---|
| Rocker-Bottom Foot | 5% - 10% (User dependent) | Premature dorsiflexion before full abduction; midfoot breach. | Remove cast; rest period; restart Phase 1 casting to restore arch; perform tenotomy only when fully abducted. |
| Cast Slippage | 10% - 15% | Poor molding; insufficient knee flexion; atypical clubfoot morphology. | Immediate removal; assess skin; re-cast with meticulous heel molding and 90-110° knee flexion. |
| Skin Breakdown / Ulceration | < 5% | Pressure points from poor padding or cast slippage (especially heel/dorsum). | Cast removal; local wound care; delay casting until fully healed; optimize padding technique. |
| Recurrence (Early) | 30% - 50% | Non-compliance with Foot Abduction Orthosis (bracing). | Repeat serial casting (2-4 casts); re-educate parents on strict bracing adherence. |
| Recurrence (Late / Dynamic) | 15% - 20% | Overactive Tibialis Anterior muscle pulling foot into supination. | Tibialis Anterior Tendon Transfer (TATT) to the lateral cuneiform; possible repeat Achilles lengthening. |
| Neurovascular Injury | < 1% | Direct injury to medial bundle during percutaneous tenotomy. | Surgical exploration and repair (rare); prevention via precise medial-to-lateral blade orientation is key. |





Phased Post-Operative Rehabilitation Protocols
The successful completion of the casting phase and the Achilles tenotomy represents only the first milestone in the Ponseti method. The long-term maintenance of correction is entirely dependent on a rigorous, phased bracing protocol. The biological tendency of the fibrotic tissues to contract persists for several years, typically until the child reaches 4 to
Clinical & Radiographic Imaging Archive




