Clavicle Fracture Fixation: An Intraoperative Masterclass in Plate Osteosynthesis

Key Takeaway
Join us in the OR for an immersive masterclass on plate fixation of displaced clavicle fractures. We'll meticulously cover comprehensive surgical anatomy, critical preoperative planning, and granular, real-time intraoperative execution. Learn precise instrument handling, reduction techniques, and hardware application, alongside crucial pearls, pitfalls, and postoperative management strategies to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Fellows, welcome to the operating theater. Today, we are undertaking a detailed exploration of a common yet highly critical injury in orthopedic trauma: the displaced, comminuted clavicle fracture. Historically, the orthopedic community adhered to a dogma that nearly all clavicle fractures could be managed non-operatively with a simple sling or figure-of-eight brace, regardless of the degree of displacement. However, modern evidence-based medicine has fundamentally shifted this paradigm. While minimally displaced or non-displaced clavicle fractures are still excellently managed with conservative protocols, those presenting with significant displacement, comminution, or shortening—particularly in high-demand, active individuals—carry an unacceptably high risk for symptomatic nonunion, malunion, and persistent shoulder dyskinesia if left to heal in a deformed position.
The patho-epidemiology of clavicle fractures demonstrates a classic bimodal distribution. We frequently encounter high-energy mechanisms in the younger, active demographic, such as falls from bicycles, motorcycle collisions, or direct contact sports injuries. In these scenarios, the axial load applied to the lateral aspect of the shoulder is transmitted medially, exceeding the structural yield point of the clavicular diaphysis. Conversely, in the elderly, osteoporotic population, simple low-energy falls from a standing height can precipitate these fractures. The midshaft region is the most frequently affected, accounting for approximately 80% of all clavicle fractures, due to its anatomic transition zone from a fixed, robust medial structure to a more mobile, flattened lateral structure.
When a midshaft clavicle fracture occurs, predictable deforming forces immediately act upon the osseous fragments, creating the classic clinical and radiographic deformity. The sternocleidomastoid muscle exerts a strong superior and posterior pull on the proximal (medial) fragment. Simultaneously, the weight of the unsupported upper extremity, combined with the inferior pull of the deltoid, drags the distal (lateral) fragment inferiorly. Furthermore, the robust pectoralis major and latissimus dorsi muscles contract, pulling the entire shoulder girdle medially, resulting in the characteristic overriding and shortening of the fracture ends. This complex, multi-planar deformity is precisely what we aim to correct through open reduction and internal fixation (ORIF).
These are the cases where plate osteosynthesis truly shines. By surgically intervening, we are not merely "fixing a bone"; we are restoring the critical anterior strut of the shoulder girdle. This restoration of anatomical length, alignment, and rotation is paramount for optimizing the biomechanics of the glenohumeral and scapulothoracic articulations. Proper osteosynthesis mitigates the risk of thoracic outlet syndrome caused by hypertrophic callus formation in a malunited fracture, prevents the chronic pain associated with altered scapular kinematics, and dramatically accelerates the patient's return to functional baseline. Today, we will master the nuances of this procedure.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of clavicular anatomy is the absolute prerequisite for safe and effective surgical intervention. The clavicle is not merely a static rod; it is a dynamic, tightly integrated strut.
Osteology and S-Shaped Morphology
The clavicle is a fascinating and unique bone, characterized by its distinct S-shaped curvature when viewed from the superior or inferior aspect. Observe its medial two-thirds, which curve anteriorly. This convex anterior curvature is not merely aesthetic; it creates a vital, widened space for the critical neurovascular structures passing from the cervical region into the upper extremity through the costoclavicular interval. This medial curvature is an evolutionary marvel, enhancing the global positioning and utility of the upper limb, allowing for complex overhead and brachiating movements. Laterally, the curve sharply transitions, turning posteriorly to articulate with the acromion.
In cross-section, the morphology of the clavicle is highly variable and non-uniform along its length. Medially, it is expanded, robust, and prismatic or triangular in shape. As we move laterally into the mid-diaphysis—the most common site of fracture—the bone transitions into a dense, tubular structure. Finally, at its lateral third, it flattens significantly in the superior-inferior plane. This complex, changing morphology is crucial for the surgeon to understand, as it dictates the necessity for meticulous, multi-planar plate contouring to achieve a flush fit without prominent hardware.
Furthermore, the internal architecture of the clavicle is unique among long bones. It is composed primarily of very dense trabecular bone encased in a thick cortical shell, notably lacking a well-defined, continuous medullary canal. This dense intramedullary architecture directly influences our surgical technique; it provides excellent purchase for our cortical and locking screws but requires careful, deliberate drilling to avoid thermal necrosis of the bone, necessitating frequent clearing of the drill flutes and copious irrigation during osteotomy or drilling.
Muscular and Ligamentous Attachments
The clavicle is tightly integrated into the shoulder girdle, serving as the sole osseous link between the axial skeleton and the appendicular upper extremity. It functions as the anterior strut, maintaining the scapula in its proper posterior and lateral position on the thoracic wall. This structural integrity is maintained via strong, complex ligamentous and muscular attachments. Medially, the robust sternoclavicular ligaments provide primary stability, while laterally, the coracoclavicular (CC) ligaments (the conoid and trapezoid) and the acromioclavicular (AC) ligaments tether the clavicle to the scapula.
The muscular attachments are extensive and dictate the deforming forces post-fracture. Superiorly, the platysma muscle lies as a superficial sheet. Deep to this, the sternocleidomastoid muscle attaches to the medial third, providing that notorious superior displacing force on medial fragments. The trapezius muscle inserts along the posterior border of the lateral third. Anteriorly, the pectoralis major originates from the medial half of the anterior clavicle, while the anterior deltoid originates from the lateral third.
Understanding these muscular intervals is critical for both exposure and reduction. For instance, when utilizing an anterior plating approach, the surgeon must carefully elevate the origins of the deltoid and pectoralis major to create an adequate footprint for the implant. Furthermore, recognizing the inferior attachment of the subclavius muscle in the subclavian groove is important, as this muscle acts as a minor dynamic stabilizer but also serves as an anatomical landmark shielding the underlying neurovascular bundle.
Critical Neurovascular Proximity
The superior aspect of the clavicle is largely subcutaneous throughout its entire length, making it a prominent aesthetic contributor to the neck and upper chest contour. While this superficial location facilitates relatively easy surgical access, it places the supraclavicular nerves at significant risk during our approach. These sensory nerves, terminal branches of the cervical plexus (C3-C4), branch out and run obliquely across the superior surface of the clavicle, just deep to the skin and superficial to or within the platysma muscle. Iatrogenic injury to these nerves can lead to bothersome, chronic hyperesthesia, dysesthesia, or a numb patch over the anterior chest wall—a complication that, while not functionally devastating, is a frequent source of patient dissatisfaction.
Deep to the clavicle, particularly along its medial and central thirds, lies a dense and unforgiving neurovascular network. The subclavian artery and vein, along with the trunks and divisions of the brachial plexus, traverse the narrow costoclavicular space directly inferior to the bone. The subclavius muscle provides a thin layer of protection, but it is insufficient against a plunging drill bit or an aggressively placed retractor.
While direct intraoperative injury to these vital structures is statistically rare, the consequences are catastrophic. Aggressive drilling without a depth gauge or protective retractor, excessive inferior soft tissue dissection, or the use of overly long screws that protrude significantly past the inferior cortex can easily lacerate the subclavian vessels or injure the brachial plexus. Therefore, strict adherence to safe surgical principles—such as using a blunt retractor (like a malleable or Darrach) beneath the bone during drilling, and drilling strictly bi-cortically with precise measurement—is non-negotiable.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative management of clavicle fractures requires a nuanced evaluation of the fracture morphology, patient physiology, and functional demands. We no longer treat the radiograph in isolation; we treat the patient.
Absolute indications for immediate or urgent surgical intervention are well-defined and center around impending catastrophic complications. These include open fractures, which require urgent debridement and stabilization to prevent osteomyelitis; fractures associated with acute neurovascular compromise (e.g., a diminished radial pulse or brachial plexopathy directly attributable to fracture fragment impingement); and fractures with severe soft tissue compromise, such as skin tenting where the sharp osseous fragment threatens to necrose the overlying dermis. Additionally, a "floating shoulder"—a concomitant ipsilateral clavicle fracture and scapular neck fracture—often necessitates fixation of at least the clavicle to restore stability to the superior suspensory complex.
Relative indications, which constitute the vast majority of our operative volume, have been heavily influenced by recent prospective randomized trials. These include completely displaced midshaft fractures with no cortical contact, fractures with shortening greater than 1.5 to 2.0 centimeters, and fractures with severe comminution (such as a transverse or Z-type fracture pattern with a rotated butterfly fragment). Furthermore, polytrauma patients benefit from early clavicle fixation to facilitate nursing care, upright positioning, and early mobilization. High-demand patients, such as elite athletes or manual laborers who require rapid return to heavy lifting, are also strong candidates for early osteosynthesis.
Contraindications must be carefully respected to avoid exacerbating patient morbidity. Absolute contraindications include active local or systemic infection, which precludes the implantation of foreign hardware. Severe medical comorbidities that render the patient unfit for general anesthesia or surgery also represent absolute contraindications. Relative contraindications include a poor soft tissue envelope (e.g., severe abrasions, burns, or prior radiation to the chest wall) that would impede wound healing. Additionally, non-ambulatory patients with minimal upper extremity functional demands, or those with severe cognitive impairments who cannot comply with postoperative rehabilitation protocols, are often better served with conservative management.
| Indication Category | Specific Clinical Scenario | Rationale for Intervention / Non-Intervention |
|---|---|---|
| Absolute Indications | Open fracture | Prevent deep osseous infection; facilitate soft tissue management. |
| Absolute Indications | Neurovascular compromise | Relieve impingement on subclavian vessels or brachial plexus. |
| Absolute Indications | Severe skin tenting | Prevent impending skin necrosis and conversion to an open fracture. |
| Absolute Indications | Floating shoulder (unstable) | Restore integrity of the superior shoulder suspensory complex (SSSC). |
| Relative Indications | Shortening > 2.0 cm | Prevent altered shoulder kinematics, weakness, and thoracic outlet symptoms. |
| Relative Indications | 100% displacement / comminution | High risk of symptomatic nonunion (>15%) with conservative care. |
| Relative Indications | Polytrauma / Bilateral fractures | Facilitate early mobilization, respiration, and weight-bearing through arms. |
| Contraindications | Active local infection | Unacceptable risk of hardware seeding and chronic osteomyelitis. |
| Contraindications | Medically unfit / High anesthesia risk | Risk of mortality outweighs the functional benefit of clavicle fixation. |
| Contraindications | Poor soft tissue envelope | High risk of wound dehiscence and exposed hardware requiring flap coverage. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the hallmark of a master surgeon. It allows us to anticipate intraoperative challenges, ensure the availability of appropriate implants, and execute a smooth, efficient procedure.
Advanced Imaging Modalities
Before we even consider bringing the patient to the operating room, a comprehensive radiographic understanding of the fracture pattern is essential. The standard Anteroposterior (AP) radiograph serves as our baseline, but it often underestimates the true degree of displacement due to the overlapping shadows of the ribs and thoracic cavity. Therefore, a Cephalad-Tilted View (often referred to as a Zanca view, typically angled 20 to 60 degrees cephalad) is mandatory. This view projects the clavicle superiorly, isolating it from the underlying thoracic structures and providing a much clearer assessment of superior-inferior displacement and true shortening.
For subtle fractures, particularly in the pediatric population or in cases of suspected birth trauma, an Apical Oblique View (45 degrees anterior, 20 degrees cephalad) can be highly sensitive for detecting minimal displacement. Post-fixation, an Abduction Lordotic View is invaluable. Taken with the shoulder abducted above 135 degrees and the central ray angled 25 degrees cephalad, this view rotates the clavicle on its longitudinal axis, causing a superiorly placed plate to rotate out of profile, thus exposing the osseous shaft and fracture site under the plate for clear assessment of reduction and screw length.
In the modern era, Computed Tomography (CT) with 3-dimensional (3D) volume-rendered reconstructions has become an indispensable tool for complex, highly comminuted fractures, or those with significant shortening and angulation. A CT scan provides unparalleled insight into the true three-dimensional deformity, allowing the surgeon to precisely map the location and size of butterfly fragments. This facilitates the preoperative formulation of a step-by-step reduction strategy, such as deciding whether a lag screw can be utilized for a specific fragment before applying the neutralization plate.
Preoperative Templating and Implant Selection
Templating is a critical step that should not be bypassed. We utilize digital templating software, overlaying implant templates onto scaled radiographs—often using the intact contralateral clavicle as a reference for length and native contour. This allows us to determine the appropriate plate length, ensuring we can achieve a minimum of three bicortical screws (six cortices) of fixation in both the proximal and distal main fragments.
For most diaphyseal fractures, a 3.5-mm limited-contact dynamic compression plate (LC-DCP) or a modern, precontoured clavicle-specific locking plate is preferred. The choice between a superior plating approach and an anteroinferior plating approach is dictated by fracture morphology, patient anatomy, and surgeon preference. Superior plating offers a biomechanical advantage by acting as a tension band against the inferiorly directed deforming forces of the arm's weight. However, it carries a higher risk of hardware prominence. Anteroinferior plating utilizes longer screws directed posteriorly (away from the neurovascular bundle) and is associated with less hardware prominence, but may provide slightly less biomechanical resistance to inferior bending forces.
Screw selection is equally important. Standard cortical screws are utilized for dynamic compression and lag screw fixation to achieve absolute stability. Locking screws are reserved for specific scenarios: osteoporotic bone where traditional screw purchase is compromised, highly comminuted segments where the plate must act as an internal fixator bridging a gap, or in the short lateral segment of distal third fractures where purchase is limited.
Patient Positioning and Operating Room Setup
Our patient is positioned supine on a radiolucent operating table. Proper positioning is critical for both surgical access and intraoperative imaging.

We begin by elevating the head and trunk slightly into a modified "beach chair" position, typically to an angle of about 15 to 30 degrees. This trunk elevation serves multiple purposes: it provides a more ergonomic working angle for the surgical team, reduces venous pressure and subsequent bleeding at the surgical site, and allows the C-arm fluoroscopy unit to easily swing in for cephalad-tilt views without being obstructed by the patient's head or the anesthesia equipment. A small interscapular bump or folded towel can be placed between the shoulder blades to allow the shoulders to fall posteriorly, aiding in the reduction of the shortened clavicle.

The ipsilateral arm must be freely draped and placed on a padded arm board or hand table. This allows the surgeon or assistant to manipulate the arm during the procedure—applying traction, abduction, or rotation—to assist with complex reduction maneuvers. However, for the majority of the case, the arm is positioned comfortably at the patient's side to ensure it does not obstruct the fluoroscopy unit.
Before prepping, we bring the C-arm in to ensure that optimal AP and cephalad-tilt imaging angles are easily attainable without compromising the sterile field or requiring drastic repositioning of the patient. Once confirmed, a wide sterile prep and drape are applied, encompassing the entire shoulder, the base of the neck, the upper chest past the midline, and the ipsilateral arm down to the fingertips. This expansive field allows for potential extension of the incision, access to the iliac crest if autologous bone graft is unexpectedly required, and unhindered manipulation of the extremity.
Step-by-Step Surgical Approach and Fixation Technique
Alright, fellows, let's begin the operative execution. We have completed our formal time-out, confirmed the correct patient, procedure, and site, and verified that appropriate prophylactic intravenous antibiotics were administered within one hour of our incision.
Surgical Incision and Superficial Dissection
For this case, we have opted for a superior approach to apply a precontoured superior plate.
First, I will meticulously infiltrate the proposed incision line and the subcutaneous tissues down to the periosteum with a dilute solution of epinephrine (1:100,000) and bupivacaine. This step serves a dual purpose: it provides preemptive local anesthesia to reduce postoperative narcotic requirements, and critically, it induces intense local vasoconstriction. The clavicular region is highly vascular, and this vasoconstriction significantly limits troublesome capillary and venous bleeding, ensuring a dry, clear visual field.

Next, I make a longitudinal skin incision, precisely in line with the long axis of the clavicle, positioned slightly inferior to its palpable superior border. The length of the incision is dictated by the fracture pattern; it must be sufficient to expose the fracture adequately and allow for proper plate application without excessive soft tissue tension. For a standard midshaft fracture, this is typically an 8 to 10 cm incision. I use a #15 blade, incising cleanly through the epidermis and dermis. Using needle-tip electrocautery on a low setting, we carry our dissection through the subcutaneous fat, maintaining meticulous hemostasis at every step.
Now, we enter a critical phase of the dissection. Just deep to the subcutaneous fat, we encounter the thin, vertically oriented muscle fibers of the platysma. It is imperative to proceed with extreme caution here to identify and protect the supraclavicular nerves. As we discussed, these nerves run obliquely across the clavicle, often embedded within or lying just deep to the platysma fascia.

Using surgical loupe magnification, I carefully dissect through the platysma using a combination of blunt spreading with tenotomy scissors and careful electrocautery. We actively search for these nerve branches. When identified, we attempt to preserve them by dissecting either entirely superior or entirely inferior to their course. If a major branch crosses directly over our planned plating zone, we gently mobilize it and retract it with a vessel loop. Transection of these nerves should be avoided at all costs to prevent postoperative neuromas and chest wall numbness.

Once the platysma is divided and the nerves are protected, we reach the robust periosteal sleeve covering the clavicle. The modern principle of biologic osteosynthesis dictates that we preserve as much of the soft tissue attachments and periosteum as possible, particularly in comminuted areas, to maintain the tenuous blood supply to the fracture fragments. Using a sharp periosteal elevator, I incise the periosteum longitudinally and gently elevate it only a few millimeters circumferentially—just enough to expose the fracture edges and create a footprint for the plate. We strictly avoid circumferential stripping of the bone.
Fracture Reduction and Provisional Stabilization
We now face the core challenge of the procedure: reducing the displaced, shortened fracture. Patience, an understanding of the deforming forces, and proper technique are crucial here.
First, using a curette and copious irrigation, we gently clear the organized hematoma, fibrin clot, and any interposed soft tissue or periosteum from the fracture ends. This is essential to allow for direct cortical bone-on-bone contact and anatomical interdigitation. We must be careful not to discard any small, viable articular fragments that contribute to the structural integrity of the cylinder.

Realignment is achieved through a combination of techniques. Often, an assistant applying gentle, sustained traction along the longitudinal axis of the abducted arm can overcome the muscular deforming forces. Simultaneously, the surgeon uses direct manipulation of the fragments with bone hooks, periosteal elevators, or dental picks. For significantly shortened or chronically displaced fractures where soft tissue contracture has occurred, a small mechanical distractor or a temporary external fixator is incredibly helpful. We insert K-wires or Schanz pins into the main proximal and distal fragments, apply the distractor, and gradually dial in length, allowing the soft tissues to stretch out over several minutes.
Once length is restored, we correct rotation and translation to achieve an anatomical reduction. We maintain this provisional reduction using specialized reduction clamps, such as Weber pointed reduction clamps or Verbrugge clamps. Alternatively, multiple 1.5mm or 2.0mm K-wires can be driven across the fracture site. It is critical to ensure that these provisional K-wires or clamp tines are positioned peripherally, entirely out of the planned trajectory of our definitive plate screws. We then bring in the C-arm and take orthogonal AP and cephalad-tilt fluoroscopic views to definitively confirm that our provisional reduction is anatomic in all planes.
Plate Contouring and Definitive Osteosynthesis
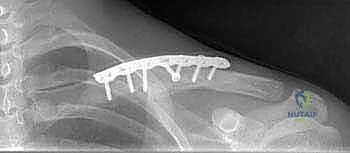
With the fracture anatomically reduced and provisionally stabilized, we proceed to definitive osteosynthesis. Today, we are utilizing a 3.5-mm precontoured superior clavicle locking plate.
Even with precontoured plates, minor adjustments are almost always necessary to match the unique osseous anatomy of the individual patient. A poorly contoured plate will either sit proud, causing skin irritation, or, when screwed down tightly, will force the reduced bone to deform to the shape of the plate, resulting in a loss of our hard-won reduction. We select a plate length that allows for a minimum of three bicortical screws (
Clinical & Radiographic Imaging Archive