PIP Joint Fracture-Dislocation ORIF: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on Proximal Interphalangeal (PIP) joint fracture-dislocation open reduction and internal fixation (ORIF). We'll meticulously cover surgical anatomy, preoperative planning, precise intraoperative steps, instrument selection, fixation techniques, and critical pearls to ensure optimal outcomes for these challenging finger injuries. Learn to restore stability and function for complex articular fractures.
Comprehensive Introduction and Patho-Epidemiology
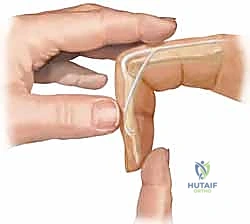
The proximal interphalangeal (PIP) joint is the functional epicenter of the human digit, responsible for the vast majority of the flexural sweep required for power grasp and fine pinch kinematics. When we encounter a PIP joint fracture-dislocation, we are not merely managing a "jammed finger"—a colloquialism that dangerously minimizes the severity of the pathology. We are confronting a complex, intra-articular disruption involving a delicate interplay of osteochondral architecture and a highly specialized soft tissue envelope. If mismanaged, these injuries relentlessly progress to devastating long-term stiffness, chronic pain, early-onset post-traumatic osteoarthritis, and profound functional impairment of the entire hand. The primary objective of any intervention is not simply radiographic reduction, but the restoration of stable, anatomic congruence that permits immediate, protected early active motion.
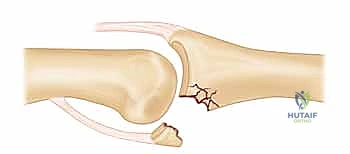
The pathogenesis of PIP fracture-dislocations is dictated by the magnitude, vector, and velocity of the deforming force. Dorsal fracture-dislocations are overwhelmingly the most common variant, typically resulting from a combination of axial loading and hyperextension. As the middle phalanx is driven dorsally over the condyles of the proximal phalanx, the volar plate is placed under immense tensile stress. The volar plate invariably fails at its distal insertion on the middle phalanx, frequently avulsing a variable-sized osteochondral fragment from the volar base. The size of this volar lip fragment is the primary determinant of residual joint stability; fragments encompassing more than 30% to 50% of the articular arc compromise the ginglymus contour, rendering the joint incompetent to resist dorsal subluxation during extension.
Conversely, volar fracture-dislocations are relatively rare and usually result from a violent rotatory or laterally directed force applied to a semi-flexed digit. These injuries are pathognomonically associated with disruption of the central slip of the extensor mechanism and at least one collateral ligament, often leading to a highly unstable configuration that requires meticulous operative repair to prevent a rigid boutonnière deformity. Pilon-type injuries represent the highest energy spectrum, characterized by severe axial impaction that drives the proximal phalanx head into the middle phalanx base, resulting in central articular depression and explosive bicondylar comminution. These pilon variants routinely defy closed management and demand sophisticated osteosynthesis or dynamic distraction techniques.
Understanding the epidemiology and precise pathomechanics is essential for the orthopedic surgeon. These injuries disproportionately affect young, active individuals, particularly athletes participating in ball sports, and manual laborers. The socioeconomic impact of a stiff, painful PIP joint in this demographic cannot be overstated. A delayed presentation is common, as patients frequently underestimate the injury. Therefore, a high index of suspicion, a rigorous clinical examination, and a precise radiographic workup are paramount to intercepting the pathology before irreversible capsular contracture and cartilage degradation occur.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Congruence
The PIP joint is a true ginglymus, or hinge joint, uniquely designed to provide a massive arc of motion in the sagittal plane while rigidly resisting coronal and transverse plane forces. The articular geometry is defined by the bicondylar head of the proximal phalanx, which features distinct radial and ulnar condyles separated by a shallow intercondylar groove. This convex surface articulates with the reciprocally biconcave base of the middle phalanx, which features a prominent median ridge. This inherent bony congruence is the primary static stabilizer of the joint, facilitating approximately 120 degrees of flexion and extension. This specific arc accounts for roughly 85% of the total digital motion required for an effective composite grasp.
Because the joint depends heavily on this interlocking bony architecture, any disruption of the articular contour—particularly at the volar base of the middle phalanx—drastically alters the joint's center of rotation. A loss of the volar buttress allows the proximal phalanx condyles to slide volarly, or conversely, the middle phalanx to subluxate dorsally. The cam-shaped design of the proximal phalanx head means that the collateral ligaments are relatively lax in extension but become maximally taut in full flexion. This biomechanical nuance is critical; it explains why unstable dorsal fracture-dislocations often require a flexed posture to maintain reduction, utilizing the tensioned collateral ligaments to tether the middle phalanx to the proximal phalanx.

The Volar Plate and Checkrein Ligament Complex
The volar plate is a robust, thick, fibrocartilaginous structure that forms the floor of the PIP joint. Distally, it has a broad, firm insertion into the volar base of the middle phalanx. Proximally, it thins out and becomes membranous, transitioning into two distinct, thickened lateral bands known as the checkrein ligaments. These checkrein ligaments anchor firmly to the periosteum of the proximal phalanx diaphysis. The volar plate is the primary restraint against hyperextension. During active flexion, the membranous proximal portion folds upon itself, allowing the plate to glide proximally without impeding the arc of motion.
The vascular anatomy surrounding the volar plate is intricate and unforgiving. Branches of the proper digital arteries traverse transversely beneath the checkrein ligaments to supply the joint capsule, the volar plate itself, and the crucial vincula brevia and longa that perfuse the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. Surgical approaches to the volar PIP joint require exquisite dissection to preserve these neurovascular bundles. Iatrogenic injury to these vessels can result in catastrophic avascular necrosis of the fracture fragments or profound flexor tendon adhesions.
Collateral Ligaments and the Extensor Mechanism
Coronal stability is governed by the collateral ligament complex, which consists of the proper collateral ligaments (PCL) and the accessory collateral ligaments (ACL). The PCL originates from the dorsal-lateral aspect of the proximal phalanx head and inserts into the volar-lateral base of the middle phalanx. It is the primary restraint to varus and valgus stress and is maximally taut in flexion. The ACL originates volarly to the PCL and inserts directly into the lateral margins of the volar plate. The ACL is taut in extension and stabilizes the volar plate against the proximal phalanx. In dorsal fracture-dislocations, the radial collateral ligament is injured almost six times more frequently than the ulnar collateral ligament, a fact that should guide your clinical examination.
Dorsally, the extensor mechanism provides dynamic stability and limits volar translation of the middle phalanx. The central slip, a direct continuation of the extensor digitorum communis, inserts onto the dorsal tubercle of the middle phalanx base. The conjoint lateral bands run obliquely along the joint's axis, coalescing distally to form the terminal tendon. The transverse retinacular ligaments connect the extensor mechanism to the volar plate, coordinating their movement during digital flexion and extension. A complete understanding of this dynamic web is essential; for a true dislocation to occur, multiple components of this soft tissue envelope—typically the volar plate, at least one collateral ligament, and portions of the extensor apparatus—must be catastrophically disrupted.
Exhaustive Indications and Contraindications
Operative Thresholds and Classification Systems
The decision to proceed with operative intervention for a PIP fracture-dislocation is predicated on identifying inherent instability that cannot be managed with functional bracing or extension-block splinting. We categorize dorsal fracture-dislocations based on the percentage of articular surface involved at the volar base of the middle phalanx. Stable injuries involve less than 30% of the articular surface and remain concentrically reduced in full extension. Tenuous injuries involve 30% to 50% of the articular surface; these will subluxate in full extension but can be maintained in a reduced position with less than 30 degrees of PIP joint flexion.
Unstable injuries—the primary indication for Open Reduction and Internal Fixation (ORIF)—involve greater than 50% of the articular surface, or involve 30% to 50% but require more than 30 degrees of flexion to maintain a concentric reduction. Immobilizing a PIP joint in greater than 30 degrees of flexion for any prolonged period guarantees severe, often irreversible, flexion contractures. Furthermore, any fracture-dislocation that is irreducible by closed means, typically due to soft tissue interposition (such as the volar plate, lateral band, or an osteochondral fragment), mandates immediate operative exploration.
Pilon fractures of the PIP joint, characterized by central articular depression and splaying of the volar and dorsal cortices, are almost universally unstable and require surgical reconstruction. Volar dislocations with a rotatory component, where the proximal phalanx condyle becomes buttonholed between the central slip and the lateral band, also represent an absolute indication for open reduction. The ultimate goal of surgery is to restore a congruent, stable articular surface that can withstand the forces of early, active rehabilitation.
Contraindications to Internal Fixation
While the indications for surgery are broad for unstable patterns, absolute and relative contraindications must be respected to avoid disastrous outcomes. Absolute contraindications include active, untreated localized or systemic infection, and severely compromised soft tissue envelopes (e.g., massive crush injuries or burns) that preclude safe surgical incisions. Operating through heavily traumatized or necrotic skin significantly increases the risk of hardware exposure, deep infection, and subsequent amputation.
Relative contraindications include severe patient non-compliance or cognitive impairment that would prevent adherence to the rigorous, mandatory postoperative rehabilitation protocol. A technically perfect ORIF will fail miserably if the patient cannot participate in early active motion. Furthermore, in cases of extreme comminution where the fragments are too small to hold fixation (the "bag of bones" scenario), traditional ORIF may be contraindicated. In these instances, dynamic external fixation (e.g., Suzuki frame), volar plate arthroplasty, or hemi-hamate autograft reconstruction are more appropriate salvage techniques than futile attempts at screw fixation in osteoporotic, pulverized bone.
| Parameter | Indications for ORIF / Surgical Intervention | Contraindications to ORIF |
|---|---|---|
| Articular Involvement | >50% of volar articular base | <30% involvement (Stable in extension) |
| Reduction Stability | Requires >30° flexion to maintain reduction | Maintains reduction with <30° flexion |
| Closed Reduction | Irreducible (soft tissue interposition) | Easily reducible and stable dynamically |
| Fracture Pattern | Pilon fractures, displaced unicondylar fractures | Undisplaced, stable fracture patterns |
| Soft Tissue Status | Intact or repairable soft tissue envelope | Active infection, severe crush/burns |
| Bone Quality | Adequate bone stock for screw/pin purchase | Severe osteopenia, "bag of bones" comminution |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Radiographic Analysis
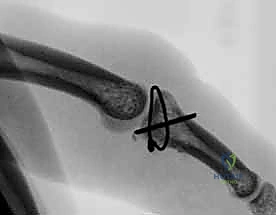
Exceptional surgical outcomes begin with an exhaustive radiographic evaluation. Standard posteroanterior (PA) and true lateral radiographs are mandatory, but they are often insufficient for complex fracture-dislocations. The true lateral radiograph is the most critical view; it must be taken with the PIP joint in full extension (if possible) to accurately assess the degree of subluxation and the exact percentage of articular involvement. A poorly positioned lateral view can artificially obscure a dorsal subluxation, leading to disastrous nonoperative mismanagement.

We must meticulously look for the "V-sign" on the lateral radiograph. This sign represents a divergence of the dorsal articular surfaces of the proximal and middle phalanges, creating a V-shaped gap. The presence of a V-sign is pathognomonic for an incompletely reduced joint and persistent dorsal subluxation. Additionally, dynamic fluoroscopy in the clinic or preoperative holding area is invaluable. By actively flexing and extending the joint under live fluoroscopy, the surgeon can pinpoint the exact degree of flexion at which the joint hinges or subluxates, providing a definitive biomechanical assessment of stability.

For pilon fractures or highly comminuted patterns, a dedicated computed tomography (CT) scan with fine (0.5mm) sagittal and coronal reconstructions is highly recommended. CT imaging allows for precise 3D mapping of the articular depression, identification of the primary fracture lines, and preoperative templating for hardware placement. Knowing the exact size and location of the fragments dictates whether you will utilize 1.0mm or 1.2mm screws, a condylar blade plate, or if the defect requires a bone graft.
Operating Room Setup and Anesthesia
The procedure is typically performed under regional anesthesia (axillary or supraclavicular brachial plexus block) combined with monitored anesthesia care (MAC) or a wide-awake local anesthesia no tourniquet (WALANT) approach. The WALANT technique is gaining immense popularity for PIP joint surgery, as it allows the surgeon to assess active, unresisted joint motion and the stability of the fixation intraoperatively before skin closure. If a block is used, an upper extremity tourniquet is applied and inflated to 250 mmHg after exsanguination with an Esmarch bandage to ensure a bloodless field, which is critical for visualizing 1-2mm articular fragments.
The patient is positioned supine with the operative arm extended on a radiolucent hand table. The surgeon should be seated comfortably, utilizing loupe magnification (minimum 3.5x, preferably 4.5x) and a sterile, focused headlight. A mini-C-arm fluoroscopy unit must be draped and positioned perpendicular to the hand table, allowing for effortless transition between PA, lateral, and oblique views without manipulating the delicately reduced fracture. Proper ergonomic setup and specialized micro-instrumentation (dental picks, micro-freers, fine reduction forceps) are non-negotiable prerequisites for this level of intra-articular surgery.
Step-by-Step Surgical Approach and Fixation Technique
Exposure Strategies: Volar versus Dorsal Approaches
The choice of surgical approach is dictated entirely by the fracture pattern. For the classic unstable dorsal fracture-dislocation with a large volar lip fragment, a volar approach is mandatory. We typically utilize a volar Bruner (zigzag) incision or a mid-lateral incision. The Bruner incision provides extensive exposure but requires meticulous elevation of the neurovascular bundles. Once the skin flaps are elevated, the flexor tendon sheath is identified. We perform a release of the A3 pulley and retract the FDS and FDP tendons laterally.

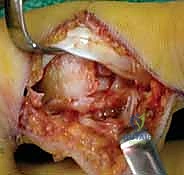
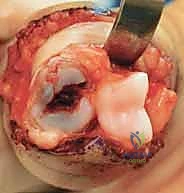
This exposes the volar plate. In the "shotgun" approach, the collateral ligaments are sharply released from the proximal phalanx, and the joint is hyperextended, completely exposing the articular surfaces of both the proximal and middle phalanges. This provides unparalleled visualization of the volar fragment and the articular step-off. Care must be taken to preserve the distal attachment of the volar plate to the fracture fragment to maintain its blood supply.



Conversely, for pilon fractures with significant dorsal comminution, or volar fracture-dislocations, a dorsal approach is utilized. A dorsal longitudinal or gently curved incision is made. The extensor mechanism is split longitudinally between the central slip and the lateral band, or a central slip-splitting approach is used. This allows direct access to the dorsal articular surface. In complex pilon injuries, combined volar and dorsal approaches may be necessary to elevate central depressed fragments and apply buttress fixation.
Fracture Reduction and Provisional Fixation
Once the fracture site is exposed, the hematoma is meticulously irrigated, and small, non-viable, loose cartilaginous debris is removed. Using a dental pick or a micro-freer elevator, the volar base fragment is gently mobilized and anatomically reduced to the middle phalanx shaft. The reduction must be absolutely perfect; even a 1mm articular step-off in the PIP joint is poorly tolerated and will lead to rapid joint destruction.



Provisional fixation is achieved using 0.028-inch or 0.035-inch Kirschner wires (K-wires). These wires should be placed peripherally to avoid cluttering the central portion of the fragment, where definitive screws will be placed. The K-wires can be used as "joysticks" to manipulate the fragment into position before driving them across the fracture site. Fluoroscopy is utilized at this stage to confirm anatomic restoration of the ginglymus contour and the elimination of the V-sign on the true lateral view.
Definitive Osteosynthesis and Construct Selection
For solid, single volar lip fragments, lag screw fixation is the gold standard. We utilize 1.0mm, 1.2mm, or 1.5mm headless compression screws or standard cortical screws. The glide hole is drilled in the volar fragment, and the thread hole is drilled into the dorsal cortex of the middle phalanx. Extreme care must be taken not to over-tighten the screws, as the volar fragment can easily split, turning a simple fixation into a salvage situation. Usually, two screws are preferred to provide rotational stability.


If the fragment is comminuted but the articular surface is intact, a tiny volar buttress plate (e.g., 1.2mm or 1.5mm grid plate) can be applied to hold the fragments in place without relying on lag screw compression. In cases of severe comminution where internal fixation is impossible, dynamic external fixation (the Suzuki frame) is employed. This construct utilizes rubber bands and K-wires to provide continuous longitudinal traction, utilizing ligamentotaxis to align the fragments while permitting active PIP joint motion. For chronic injuries or massive bone loss (>50%), a hemi-hamate autograft is harvested from the distal articular surface of the hamate and contoured to reconstruct the volar base of the middle phalanx, restoring both stability and the articular arc.






Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Complications
The surgical management of PIP joint injuries is fraught with potential complications. Intraoperatively, the most common error is iatrogenic fragmentation of the volar lip during screw insertion. This occurs when the drill bit is too large, the screw is over-torqued, or the fragment was primarily too small to accommodate the hardware. If this occurs, the surgeon must immediately pivot to a salvage technique, such as K-wire fixation, a hook plate, or dynamic external fixation.
In the early postoperative period, loss of reduction is a devastating complication, occurring in up to 5-10% of cases. This is usually due to inadequate initial fixation, premature unprotected motion, or patient non-compliance. Superficial and deep infections occur in roughly 2-4% of cases, particularly with the use of external fixators (pin tract infections). Prompt aggressive debridement and targeted antibiotic therapy are required to prevent septic arthritis, which rapidly destroys the remaining cartilage.
Late Complications and Salvage Procedures
Post-traumatic stiffness is the most ubiquitous late complication, affecting nearly all patients to some degree. Flexion contractures are common if the joint was immobilized in excessive flexion, while extension deficits occur due to volar plate scarring and extensor mechanism adhesions. Tenolysis and capsulotomy may be indicated at 6 to 12 months post-injury if a plateau in therapy is reached, provided the articular surface remains congruent.
Post-traumatic osteoarthritis is the inevitable end-stage of an imperfectly reduced joint. When pain becomes debilitating and function is severely compromised, salvage procedures are indicated. For the index and middle fingers, where lateral stability is paramount for pinch strength, PIP joint arthrodesis (fusion) in 40 to 50 degrees of flexion is the procedure of choice. For the ring and small fingers, where a functional arc of motion is prioritized for power grasp, surface replacement arthroplasty (using silicone elastomers or pyrocarbon implants) can provide excellent pain relief and functional motion, though patients must accept lifting restrictions.
| Complication | Estimated Incidence | Prevention / Management Strategy |
|---|---|---|
| Post-Traumatic Stiffness | 60 - 80% | Rigid fixation allowing early active motion; aggressive hand therapy. |
| Loss of Reduction / Hardware Failure | 5 - 10% | Accurate preoperative templating; avoid over-torquing screws; use buttress plates for comminution. |
| Flexion Contracture | 20 - 30% | Avoid immobilizing >30° flexion; dynamic extension splinting post-op. |
| Post-Traumatic Osteoarthritis | 15 - 25% | Anatomic articular reduction (<1mm step-off); late salvage via arthrodesis or arthroplasty. |
| Infection (Superficial/Deep) | 2 - 4% | Meticulous soft tissue handling; prophylactic antibiotics; aggressive pin care for ex-fix. |
Phased Post-Operative Rehabilitation Protocols
Early Protective Phase and Edema Control
The success of PIP joint ORIF relies heavily on a meticulously structured, phased rehabilitation protocol managed by a certified hand therapist. The immediate postoperative phase (Days 1-14) focuses on edema control, wound healing, and protecting the osteosynthesis. A bulky, compressive dressing is applied in the operating room. Within 3 to 5 days, this is transitioned to a custom thermoplastic extension-block splint.
For dorsal fracture-dislocations, the splint is fabricated to block the final 10 to 20 degrees of extension, preventing tension on the volar plate repair and the volar fracture fragment. Crucially, the splint allows for full active flexion. Patients are instructed to perform active flexion exercises hourly. Passive flexion is strictly avoided early on, as it can inadvertently place excessive stress on the hardware. Edema management utilizing compressive wraps (Coban) and elevation is critical to prevent the organization of protein-rich fluid into dense, restrictive scar tissue around the collateral ligaments.
Intermediate Motion and Late Strengthening
During the intermediate phase (Weeks 3-6), radiographic healing begins to consolidate. The extension block is gradually reduced by 10 degrees each week until full active extension is permitted. If dynamic external fixation (Suzuki frame) was utilized, it is typically removed in the clinic at 4 to 5 weeks postoperatively. Once hardware or frames are removed, therapy intensifies to include gentle passive range of motion (PROM) and dynamic splinting if a flexion contracture is developing.
The late phase (Weeks 6-12) focuses on maximizing the total active motion (TAM) arc and initiating progressive strengthening. Blocking exercises are introduced to isolate FDS and FDP glide. Work hardening and sport-specific training commence around week 8. It is imperative to counsel the patient preoperatively that maximal medical improvement (MMI) for a PIP joint fracture-dislocation frequently takes 6 to 12 months, and the joint will likely remain permanently thicker than the contralateral uninjured digit due to capsular hypertrophy.
Summary of Landmark Literature and Clinical Guidelines
The evolution of PIP joint fracture-dislocation management is deeply rooted in several landmark biomechanical and clinical studies. Hastings and Carroll provided the foundational classification system, emphasizing the critical threshold of 30% to 50% articular involvement and its direct correlation to joint instability. Their work established the biomechanical rationale for operative intervention in fragments exceeding this threshold.
The advent of dynamic distraction external fixation, popularized by Suzuki et al., revolutionized the treatment of highly comminuted pilon fractures. By applying the principle of ligamentotaxis, the Suzuki frame maintains joint space and reduces fragments without opening the fracture site, allowing for immediate active motion and cartilage nourishment. This technique remains the gold standard for "bag of bones" injuries where internal fixation is impossible.
More recently, the utilization of the hemi-hamate autograft, detailed by Williams and Hastings, has provided a robust salvage option for chronic fracture-dislocations or acute injuries with massive (>50%) volar bone loss. By harvesting the anatomically similar distal articular surface of the hamate, surgeons can reconstruct the volar buttress and restore the ginglymus contour. Current clinical guidelines universally stress that regardless of the technique chosen—be it lag screws, plating, external fixation, or grafting—the paramount goal is achieving a stable joint that permits immediate, protected active motion to combat the PIP joint's relentless propensity for stiffness.
