First MTP Arthrodesis and Lesser MTP Resection: A Comprehensive Surgical Guide

Key Takeaway
Arthrodesis of the first metatarsophalangeal (MTP) joint combined with resection of the lesser MTP joints is a highly effective salvage procedure for severe forefoot deformities, particularly in rheumatoid arthritis. This technique reestablishes the plantar fat pad, corrects fixed deformities, and restores weight-bearing biomechanics. Success relies on precise osteotomies, optimal hallux positioning (20 degrees valgus, 15 degrees dorsiflexion), and meticulous soft-tissue balancing to ensure a stable, plantigrade foot.
Comprehensive Introduction and Patho-Epidemiology
Arthrodesis of the first metatarsophalangeal (MTP) joint combined with resection arthroplasty of the lesser MTP joints remains a cornerstone salvage procedure for patients presenting with severe, end-stage forefoot deformities. Historically popularized for the management of the classic rheumatoid forefoot by pioneers such as Hoffman, Clayton, Thompson, and Mann, this comprehensive reconstruction addresses a highly complex pathoanatomy. The clinical presentation is typically characterized by severe hallux valgus, fixed dorsal dislocation of the lesser toes, and the painful, debilitating distal migration of the plantar fat pad. While the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies has significantly reduced the incidence of end-stage rheumatoid foot deformities, this surgical approach remains highly relevant. It is frequently employed today for severe degenerative joint disease, neglected post-traumatic deformities, and revision scenarios where previous forefoot surgeries have failed catastrophically.
The patho-epidemiology of the rheumatoid and severe degenerative forefoot is driven by chronic, relentless synovial hypertrophy and capsular distension. In the rheumatoid patient, the initial insult is an aggressive synovitis that systematically attenuates the capsuloligamentous constraints of the MTP joints. The collateral ligaments and the critical plantar plate are weakened, rendering the joints fundamentally unstable. As the intrinsic muscles spasm and the extrinsic flexor and extensor tendons gain a mechanical advantage over the compromised static stabilizers, the proximal phalanges are inexorably driven into dorsal subluxation and eventual frank dislocation. This dorsal displacement of the phalanges exerts a reciprocal plantarward force on the lesser metatarsal heads, driving them deep into the plantar soft tissues.
This biomechanical collapse initiates a devastating cascade affecting the plantar weight-bearing structures. Normally, the prominent metatarsal heads are cushioned by a robust plantar fat pad, which is tethered to the bases of the proximal phalanges via the plantar aponeurosis and the plantar plate. As the phalanges dislocate dorsally, they drag the protective plantar fat pad distally into the sulcus of the toes. Consequently, the prominent, plantar-flexed metatarsal heads are left covered only by a thin layer of atrophic skin and subcutaneous tissue. This loss of functional padding results in the formation of intractable plantar keratoses (IPKs), adventitial bursitis, and severe weight-bearing pain that profoundly limits patient mobility.
Thompson and Mann extensively documented the clinical efficacy and biomechanical rationale of this combined reconstructive approach. They demonstrated that meticulous, cascaded resection of the lesser metatarsal heads, combined with the establishment of a rigid, stable medial column via first MTP arthrodesis, effectively decompresses the forefoot and allows the distally migrated fat pad to recede beneath the newly contoured weight-bearing metatarsal stumps. Furthermore, they noted that this reconstruction allows patients to tolerate a significantly greater variety of footwear and restores a functional, pain-free gait. Notably, even if the tips of the shortened lesser toes do not achieve full ground contact during static stance, dynamic balance, proprioception, and overall patient satisfaction remain exceptionally high, provided the medial column is rigidly stabilized.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of forefoot anatomy and biomechanics is essential for executing this complex reconstruction and avoiding catastrophic postoperative failures. The first ray, comprising the first metatarsal and the medial cuneiform, is the primary load-bearing structure of the forefoot during the terminal stance and toe-off phases of the gait cycle. The first MTP joint is a highly complex, multi-axial articulation stabilized by a robust capsuloligamentous complex, including the strong medial and lateral collateral ligaments, the sesamoid complex, and the plantar plate. The Windlass mechanism, driven by the plantar fascia, relies on the integrity of the first MTP joint to elevate the medial longitudinal arch and create a rigid lever for propulsion. When the first MTP joint is rendered incompetent by severe hallux valgus or rheumatoid destruction, load is pathologically transferred to the lesser metatarsals, exacerbating their collapse.
The lesser MTP joints are condylar articulations that rely heavily on soft-tissue constraints for stability, as they possess minimal intrinsic bony congruence. The primary static stabilizer against dorsal dislocation is the plantar plate, a thick, fibrocartilaginous structure that originates from the metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. The collateral ligaments, consisting of the proper collateral ligament (stabilizing the joint in flexion) and the accessory collateral ligament (inserting into the plantar plate), provide crucial coronal and sagittal plane stability. In the setting of chronic synovitis or severe mechanical overload, the plantar plate attenuates or ruptures, usually beginning at the second MTP joint, leading to the classic crossover toe deformity and subsequent dorsal dislocation.
The intrinsic and extrinsic musculature of the forefoot plays a critical role in the pathogenesis of lesser toe deformities. The lumbricals and interossei normally flex the MTP joints and extend the interphalangeal joints. However, as the proximal phalanx subluxates dorsally, the axis of rotation shifts. The intrinsic muscles, along with the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB), migrate dorsal to the MTP joint's axis of rotation, converting them into deforming forces that exacerbate the dorsal dislocation. Simultaneously, the flexor digitorum longus (FDL) and flexor digitorum brevis (FDB) pull the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints into rigid flexion, creating the classic hammer toe or claw toe deformity that frequently accompanies severe MTP joint pathology.
Biomechanical restoration during surgery relies on two fundamental principles: stabilizing the medial column and restoring the metatarsal parabola. Arthrodesis of the first MTP joint restores the medial weight-bearing column, effectively bypassing the destroyed joint and providing a stable buttress against which the foot can pivot during push-off. Resection of the lesser metatarsal heads must be meticulously planned to recreate the normal cascade (often referred to as the Maestro curve), where the first and second metatarsals are approximately equal in length, and the third, fourth, and fifth metatarsals progressively shorten. Failure to respect this biomechanical cascade, such as leaving a lesser metatarsal excessively long relative to its neighbors, will inevitably result in focal pressure concentration, recurrent IPKs, and transfer metatarsalgia.
Exhaustive Indications and Contraindications
The decision to proceed with a first MTP arthrodesis and lesser MTP resection is reserved for end-stage pathology where joint-sparing procedures are no longer viable. The classic indication remains the severe rheumatoid forefoot, characterized by advanced joint destruction, profound deformity, and intractable pain. However, the indications have broadened to encompass severe, neglected degenerative joint disease, advanced post-traumatic arthrosis, and complex revision scenarios. Patients with multiple failed previous forefoot surgeries, such as failed silastic implants, recurrent severe hallux valgus with crossover toes, or iatrogenic metatarsal cascade disruptions, are excellent candidates for this definitive salvage procedure.
A critical prerequisite for this surgery is the presence of severe, uncorrectable deformity combined with significant pain that limits activities of daily living. Patients typically present with a triad of severe hallux valgus (often exceeding 40 to 50 degrees), overriding or rigidly dislocated lesser toes, and painful plantar callosities beneath the lesser metatarsal heads. The presence of ulcerations over the dorsal PIP joints (due to shoe friction) or plantar IPKs (due to bone prominence) further solidifies the indication, provided there is no active, deep soft-tissue or bone infection. The primary goal of the procedure is not cosmetic perfection, but rather the creation of a painless, plantigrade, and shoeable foot.
Contraindications must be meticulously respected to avoid devastating complications such as catastrophic infection or ischemic necrosis of the digits. Absolute contraindications include active local or systemic infection, profound peripheral arterial disease (PAD) that precludes soft-tissue healing, and severe medical comorbidities that make the patient an unacceptable anesthetic risk. Relative contraindications include a history of non-compliance, active Charcot neuroarthropathy (which may require more extensive midfoot or hindfoot stabilization), and poorly controlled diabetes mellitus with profound peripheral neuropathy. In neuropathic patients, the lack of protective sensation significantly increases the risk of postoperative hardware failure, nonunion, and recurrent ulceration, necessitating extreme caution and potentially altered fixation strategies.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | End-stage Rheumatoid Arthritis, Severe DJD | Joint destruction precludes any joint-sparing or soft-tissue realignment procedures. |
| Salvage Indications | Failed silastic arthroplasty, multiple failed bunionectomies | Restores medial column stability and eliminates pain from failed implants or recurrent deformity. |
| Absolute Contraindications | Active osteomyelitis, critical limb ischemia (ABI < 0.5) | High risk of systemic sepsis or catastrophic ischemic necrosis requiring amputation. |
| Relative Contraindications | Severe peripheral neuropathy, active Charcot | High risk of nonunion, hardware failure, and unrecognized postoperative complications. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative assessment and meticulous surgical planning are critical for achieving a successful outcome in this complex reconstruction. The clinical evaluation must begin with a rigorous assessment of the vascular status. Given the extensive soft-tissue dissection, the longitudinal tension placed on the digital arteries during realignment, and the frequent presence of systemic vasculopathy in rheumatoid patients, robust vascular inflow is absolutely mandatory. Palpation of the dorsalis pedis and posterior tibial pulses is the minimum requirement; any absence or asymmetry dictates the need for non-invasive vascular studies, including Ankle-Brachial Indices (ABI), Toe-Brachial Indices (TBI), and potentially arterial Doppler ultrasonography. A TBI of less than 0.7 or an absolute toe pressure of less than 40 mmHg should prompt a formal vascular surgery consultation prior to any operative intervention.
Skin integrity and dermatologic health must be carefully evaluated. The dorsal skin over prominent, dislocated PIP joints is often paper-thin, atrophic, and prone to breakdown, dictating the need for careful tissue handling and potentially prophylactic PIP joint arthroplasty to relieve tension. Plantar skin must be assessed for deep, ulcerated IPKs. If a plantar ulcer is present but superficial and uninfected, the resection of the underlying metatarsal head will typically allow it to heal postoperatively. However, deep ulcerations probing to bone require a preoperative MRI to rule out osteomyelitis. Bone quality must also be assessed clinically and radiographically; rheumatoid patients and elderly individuals frequently exhibit profound osteopenia, which directly influences the choice of internal fixation, often shifting the preference from rigid plate-and-screw constructs to load-sharing intramedullary devices like Steinmann pins.
Radiographic assessment requires high-quality, weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot. The AP view is utilized to assess the degree of first MTP joint destruction, the intermetatarsal angle, and the extent of lesser MTP joint subluxation or frank dislocation. Crucially, the AP radiograph is used for templating the metatarsal resection cascade. The surgeon must calculate the amount of bone to be resected from the first metatarsal to achieve a stable fusion, and subsequently plan the resection levels for the lesser metatarsals to recreate a smooth, laterally sloping parabola. The lateral view is essential for evaluating the sagittal alignment of the first ray, assessing for any dorsal elevation that must be corrected during the arthrodesis, and visualizing the plantar displacement of the lesser metatarsal heads.
Patient positioning and anesthesia are optimized for prolonged forefoot exposure. The procedure is typically performed under general anesthesia or a robust regional block (such as a popliteal sciatic nerve block combined with a saphenous nerve block), which provides excellent intraoperative muscle relaxation and prolonged postoperative analgesia. The patient is positioned supine on the operating table with a bump placed under the ipsilateral hip to internally rotate the leg to a neutral position, allowing the foot to rest perfectly vertical. A well-padded thigh or calf tourniquet is applied to ensure a bloodless surgical field, though the tourniquet should be deflated prior to final closure in patients with questionable vascularity to meticulously assess digital perfusion. Intravenous prophylactic antibiotics are administered within one hour of the surgical incision.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the combined first MTP arthrodesis and lesser MTP resection is a meticulously orchestrated sequence. The procedure invariably begins with the stabilization of the medial column. Establishing the correct length, rotation, and sagittal alignment of the first ray is the foundational step that dictates the subsequent resection levels for the lesser metatarsals.
First MTP Joint Exposure and Preparation
The approach to the first MTP joint is typically performed via a dorsal longitudinal incision, approximately 6 to 8 cm in length, centered over the joint and positioned just medial to the extensor hallucis longus (EHL) tendon. In patients with severely compromised soft-tissue envelopes, such as those with advanced rheumatoid disease or a history of chronic systemic corticosteroid use, a direct medial approach may be preferable to preserve the dorsal vascular plexus and avoid catastrophic dorsal skin necrosis. Deep dissection must carefully identify and retract the dorsomedial branch of the superficial peroneal nerve to prevent painful neuroma formation. The joint capsule is incised longitudinally, and a meticulous, aggressive synovectomy is performed, utilizing a rongeur and scalpel to remove all hypertrophic, destructive rheumatoid pannus that frequently invades the subchondral bone.
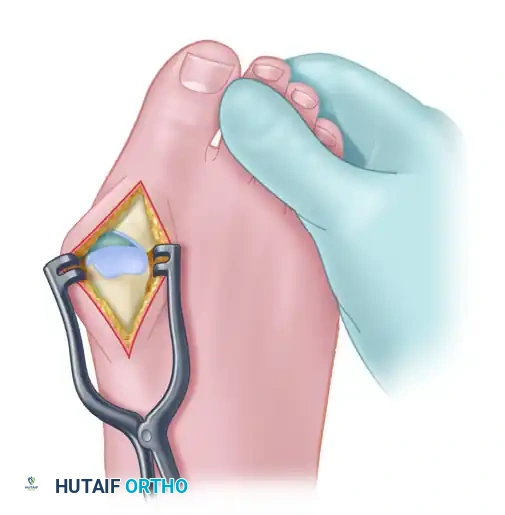
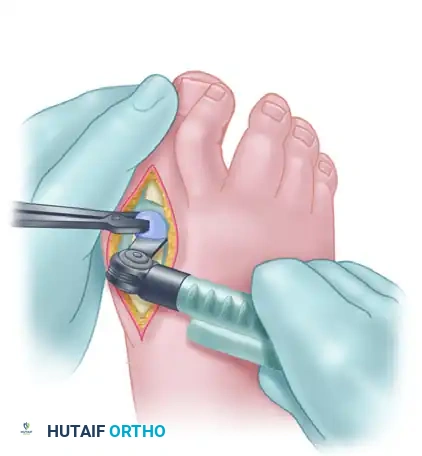
Joint preparation requires the complete removal of articular cartilage and subchondral bone to expose healthy, bleeding cancellous bone. The capsule is released medially and laterally off the metatarsal head and the base of the proximal phalanx to achieve full, unhindered exposure. Using an oscillating sagittal saw, a flat cut is created across the first metatarsal head, typically removing 3 to 5 mm of distal bone. The orientation of this cut is absolutely critical: the saw blade must be positioned with the hallux held in approximately 10 to 15 degrees of valgus and 15 degrees of dorsiflexion relative to the plantar aspect of the foot (the weight-bearing surface), not the declinated metatarsal shaft.
Following the metatarsal cut, the base of the proximal phalanx is completely freed from its soft-tissue attachments, including the plantar plate and flexor hallucis brevis insertions. The proximal 3 to 5 mm of the proximal phalanx is excised. It is imperative that the osteotomy of the phalanx is perfectly parallel to the metatarsal cut while holding the toe in the aforementioned optimal position of valgus and dorsiflexion.
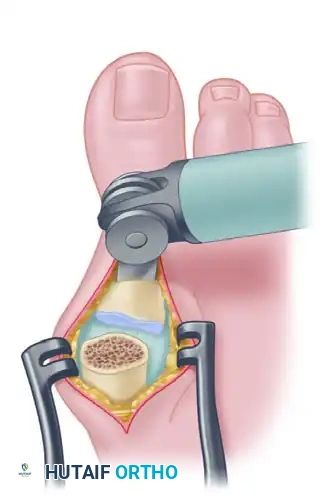
Alternatively, commercially available cannulated conical reamers (the cup and cone technique) can be utilized. This method allows for infinite multiplanar adjustment of the MTP joint position prior to fixation and provides excellent, congruent cancellous bone contact. However, it may lack the intrinsic rotational stability provided by a perfectly executed flat cut, and it often results in less overall shortening—a factor that must be carefully considered when concurrent lesser metatarsal resections demand significant medial column shortening to maintain an appropriate cascade.
First MTP Joint Fixation Strategies
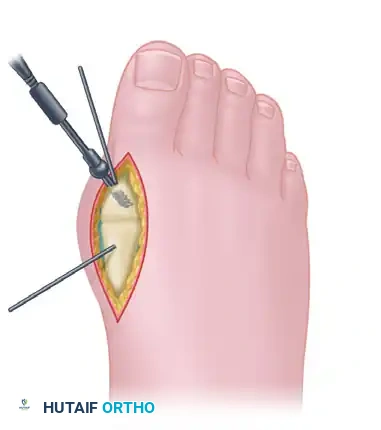
The choice of fixation for the first MTP arthrodesis depends heavily on the patient's bone stock, compliance, and the surgeon's preference. In patients with excellent bone density, an interfragmentary lag screw combined with Kirschner wires or a neutralization plate is highly effective. The joint is temporarily stabilized with two 0.054-inch (1.4-mm) K-wires. A lag screw (typically 3.5 mm or 4.0 mm) is placed across the MTP joint, usually from distal-medial to proximal-lateral, to achieve robust interfragmentary compression across the prepared cancellous surfaces.
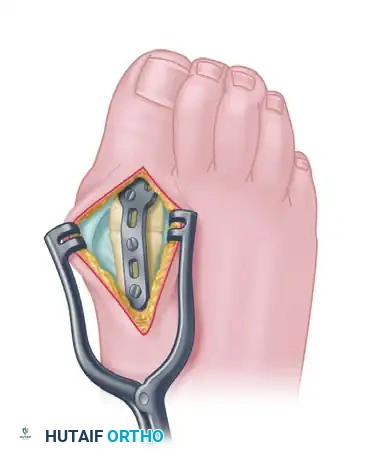
The current gold standard for patients with normal to moderately osteopenic bone is the dorsal plate construct. A precontoured, low-profile titanium MTP fusion plate (incorporating built-in valgus and dorsiflexion angles) is applied to the dorsal aspect of the joint. The plate is secured using 3.0-mm or 3.5-mm locking and non-locking screws. This construct provides superior biomechanical stability, excellent resistance to plantar gapping, and allows for earlier postoperative mobilization compared to isolated screw or pin fixation.
In cases of severe, profound osteopenia—frequently encountered in advanced rheumatoid arthritis—screws may fail to achieve adequate purchase. In such salvage scenarios, the use of two 1/8-inch, double-threaded Steinmann pins is indicated. The pins are drilled in a retrograde fashion, starting at the base of the proximal phalanx and exiting through the tip of the distal phalanx. The joint is reduced into perfect alignment, and the pins are then driven antegrade across the MTP joint and deep into the medullary canal of the first metatarsal. While this technique provides excellent longitudinal stability in osteoporotic bone, it violates the interphalangeal joint, potentially leading to stiffness or arthrosis, and is therefore strictly reserved for cases where screw or plate fixation is impossible.

Lesser MTP Joint Exposure and Resection
Once the first MTP joint is prepared and provisionally or definitively fixed, attention is directed to the lesser rays. The lesser MTP joints are approached through two dorsal longitudinal incisions, strategically placed in the second and fourth web spaces to minimize skin bridges and optimize exposure. Each incision begins deep in the web space and extends proximally for approximately 3 to 4 cm over the intermetatarsal space.

Deep dissection requires careful identification of the extensor tendons. The extensor digitorum longus (EDL) and the deeper, slightly lateral extensor digitorum brevis (EDB) are traced distally to the base of the proximal phalanx. If severe, rigid contractures are present, a Z-lengthening or frank tenotomy of the EDL may be required to allow for adequate plantarflexion of the toe. The MTP joints are entered strategically: medial to the extensor tendons for the second and third joints, and lateral to the tendons for the fourth and fifth joints.
The base of the proximal phalanx is circumferentially freed from all capsuloligamentous attachments using sharp dissection. In cases of chronic dislocation, the base of the phalanx may be rigidly ankylosed to the dorsal neck of the metatarsal; this must be carefully pried off with an elevator before the soft tissues can be fully detached. Longitudinal traction is applied to the toe, and a dorsal longitudinal incision is made over the distal metatarsal. The soft tissues are stripped medially and laterally, and a Freer elevator is used to circumferentially clear the metatarsal head and surgical neck. Strict adherence to dissecting only on the bone is vital to protect the common digital nerves and arteries located in the intermetatarsal spaces.
The lesser metatarsal heads are resected at the level of the surgical neck using an oscillating saw. The resection must be meticulously angled from dorsal-distal to plantar-proximal to prevent a prominent plantar bony ridge, and it must create a gentle, laterally sloping cascade to mimic the normal metatarsal parabola. A curved McGlamry or Hohmann retractor is highly effective for protecting the delicate plantar structures during the saw cut. Failing to remove the entire metatarsal head, particularly leaving the plantar condyles intact, will inevitably result in recurrent plantar keratosis and surgical failure.
Soft Tissue Balancing and Lesser Ray Fixation
Following bony resection, the plantar soft tissues are addressed. If significant adventitial synovial cysts or severely hypertrophied bursae are present on the plantar aspect, only the dorsal half of the cyst should be excised. A rongeur is used to gently debride the underlying soft tissues. It is a crucial surgical principle to avoid aggressive resection of plantar tissue; preserving the remaining fat and fibroadipose tissue is absolutely vital to ensure adequate plantar padding beneath the newly resected, shortened metatarsal stumps.
The lesser toes must then be stabilized to maintain alignment and allow the soft tissues to heal in a corrected position. Severe fixed PIP deformities are addressed via excisional arthroplasty, which involves resecting the head and neck of the proximal phalanx through a separate dorsal elliptical incision over the PIP joint. Mild, flexible deformities may be addressed via closed osteoclasis. Each lesser ray is then stabilized with a 6-inch-long, 0.054-inch (1.4-mm) Kirschner wire. The wire is driven retrograde through the tip of the toe, across the straightened DIP and PIP joints. The toe is held in perfect alignment, and the wire is advanced proximally across the resected MTP space and driven deep into the medullary canal of the metatarsal shaft.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the combined first MTP arthrodesis and lesser MTP resection carries a significant risk profile, primarily due to the severe baseline pathology, compromised soft-tissue envelopes, and frequent medical comorbidities of the patient population. Comprehensive understanding of potential complications and their salvage management is mandatory for the operating surgeon.
Nonunion of the first MTP joint is a well-documented complication, with reported incidence rates ranging from 5% to 10%. Risk factors include severe osteopenia, inadequate bone preparation, poor fixation constructs, smoking, and non-compliance with postoperative weight-bearing restrictions. Fortunately, many nonunions are asymptomatic fibrous unions that do not require further intervention. However, if a nonunion is symptomatic and accompanied by hardware failure or loss of alignment, revision surgery is indicated. Salvage typically involves hardware removal, aggressive debridement of the nonunion site to bleeding bone, application of autologous bone graft or orthobiologics, and robust revision internal fixation, often utilizing a highly stable dorsal plate or, in extreme cases of bone loss, a structural bone block.
Malunion of the first MTP joint is arguably more detrimental to patient function than an asymptomatic nonunion. Excessive dorsiflexion leads to a "cock-up" deformity, resulting in painful shoe impingement dorsally and a failure of the hallux to participate in weight-bearing, which exacerbates transfer metatarsalgia to the lesser rays. Conversely, excessive plantarflexion results in severe pressure over the interphalangeal joint and tip of the toe. Varus or valgus malalignment can lead to adjacent toe impingement or medial shoe wear issues. Symptomatic malunions require corrective closing or opening wedge osteotomies through the fusion mass to restore the optimal alignment of 10 to 15 degrees of valgus and 15 degrees of dorsiflexion relative to the floor.
Vascular compromise of the lesser digits is a catastrophic complication that demands immediate recognition and intervention. The "30-Minute Rule" is a critical postoperative protocol: the circulatory status of the toes must be monitored obsessively immediately following surgery. A blanched, white toe indicates arterial compromise, usually resulting from excessive longitudinal traction along the K-wire that tethers the digital arteries. A cyanotic, blue toe indicates venous congestion, often caused by excessive shortening that kinks the delicate venous drainage system. If normal capillary refill and color do not return within 30 minutes, the compressive dressing must be released. If ischemia persists, the longitudinal K-wire must be immediately removed to allow the digit to shorten and relieve tension on the neurovascular bundle, prioritizing viable tissue over perfect radiographic alignment.
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| First MTP Nonunion | 5% - 10% | Poor bone stock, inadequate fixation, smoking | Observation if asymptomatic; revision arthrodesis with bone grafting and rigid plating if painful. |
| First MTP Malunion | 3% - 8% | Incorrect intraoperative positioning (excessive dorsiflexion/plantarflexion) | Corrective osteotomy through the fusion mass to restore optimal sagittal and coronal alignment. |
| Vascular Compromise (Digit) | 1% - 3% | Arterial tethering (over-distraction) or venous kinking (over-shortening) | Immediate release of dressings; removal of K-wire to relieve longitudinal tension; vascular consult if unresolved. |
| Recurrent Plantar Keratosis | 10% - 15% | Inadequate metatarsal head resection, failure to restore the Maestro curve | Conservative care (custom orthotics); revision osseous resection of the prominent metatarsal stump. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is phased to protect the delicate soft-tissue reconstruction, ensure osseous union of the first MTP joint, and gradually restore weight-bearing function. The immediate postoperative phase (0 to 24 hours) focuses on edema control and vascular monitoring. A meticulous, sterile, firm compression dressing is applied in the operating room to maintain the alignment of the lesser toes and control swelling. The foot is kept strictly elevated above heart level. As previously emphasized, the vascular status of the digits is monitored continuously during this critical window.
During the early healing phase (Days 1 to 14), the patient is typically transitioned to a lighter-weight compression dressing before discharge. Ambulation is permitted, but it is strictly limited to weight-bearing on the heel and the lateral border of the foot utilizing a rigid-soled postoperative shoe or a controlled ankle motion (CAM) boot. The rigid sole is essential to prevent any dorsiflexion forces across the forefoot, which could disrupt the first MTP fixation or bend the lesser toe K-wires. Patients are instructed to minimize time spent with the foot dependent and to meticulously keep the pin sites clean and dry. Suture removal is generally performed at the two-week postoperative clinic visit, provided the incisions are fully healed and dry.
The intermediate phase (4 to 6 weeks) marks the removal of the percutaneous hardware. The longitudinal K-wires stabilizing the lesser toes (and the Steinmann pins in the hallux, if utilized for first MTP fixation) are typically removed in the outpatient clinic setting between 4 and 6 weeks postoperatively. This removal allows the soft tissues
