Metacarpophalangeal Joint Arthrodesis: Comprehensive Surgical Guide
Key Takeaway
Metacarpophalangeal (MCP) joint arthrodesis is a highly reliable salvage procedure for severe arthritis, instability, or deformity. The modified tension band technique by Stern and Segmüller provides robust fixation, utilizing Kirschner wires and a figure-of-eight stainless steel wire. Optimal fusion angles range from 20 to 30 degrees of flexion, depending on the digit. Meticulous joint preparation and rigid internal fixation ensure high union rates and excellent functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
Metacarpophalangeal (MCP) joint arthrodesis is a definitive, highly reliable salvage procedure utilized in the management of severe joint destruction, intractable pain, and gross instability. While motion-preserving alternatives such as silicone or pyrolytic carbon arthroplasty are frequently favored—particularly in the low-demand rheumatoid hand—arthrodesis remains the absolute gold standard for young, high-demand patients, heavy manual laborers, and individuals presenting with profound bone loss, chronic infection sequelae, or unreconstructable paralytic deformities. The fundamental objective of MCP joint arthrodesis is to provide a rigidly stable, painless osseous pillar against which the thumb can effectively pinch, or to restore the functional cascade of the ulnar digits for sustained power grip.
The patho-epidemiology of conditions necessitating MCP joint arthrodesis is diverse, reflecting a spectrum of inflammatory, traumatic, and neurologic etiologies. Rheumatoid arthritis (RA) historically represented the most common indication; however, the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies has dramatically altered the epidemiological landscape. Today, surgeons are increasingly performing this procedure for post-traumatic osteoarthritis, which typically manifests following high-energy crush injuries, intra-articular fractures, or neglected dislocations that result in severe articular comminution and subsequent chondrolysis. In these scenarios, the native joint architecture is often entirely obliterated, rendering arthroplasty biomechanically unviable due to the lack of supportive collateral ligaments and adequate bone stock.
Furthermore, neurologic conditions resulting in paralytic hand deformities represent a critical, albeit less common, subset of patients requiring MCP fusion. In combined median and ulnar nerve palsies, the loss of intrinsic muscle function leads to a profound claw deformity, characterized by MCP joint hyperextension and interphalangeal joint flexion. When dynamic tendon transfers are contraindicated due to a lack of available donor musculature or severe joint contractures, an MCP arthrodesis effectively stabilizes the proximal phalanx, preventing hyperextension and allowing the extrinsic extensor tendons to transmit force distally to extend the interphalangeal joints. Understanding the specific patho-epidemiology driving the joint destruction is paramount, as it directly dictates the choice of surgical approach, the method of internal fixation, and the anticipated postoperative rehabilitation trajectory.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the intricate surgical anatomy and biomechanics of the metacarpophalangeal joint is an absolute prerequisite for executing a successful arthrodesis. The MCP joint is a diarthrodial condyloid joint, formed by the articulation of the convex, asymmetric metacarpal head and the shallow, concave base of the proximal phalanx. The metacarpal head is not perfectly spherical; it is wider on its volar aspect than on its dorsal aspect. This unique geometry creates a "cam effect," whereby the collateral ligaments are relatively lax in extension—allowing for abduction and adduction—but become maximally taut in flexion, providing critical mediolateral stability during grip. When performing an arthrodesis, the surgeon must completely dismantle this ligamentous complex to gain adequate exposure of the articular surfaces.
The soft tissue envelope surrounding the MCP joint is highly specialized and leaves little margin for error regarding hardware placement. Dorsally, the extensor mechanism forms a complex aponeurotic hood over the joint. The central slip of the extensor digitorum communis (EDC) is centrally positioned, flanked by the sagittal bands which tether the extensor tendon and prevent its subluxation during active flexion. Deep to the extensor mechanism lies the thin dorsal joint capsule. The paucity of subcutaneous fat over the dorsal aspect of the MCP joint makes prominent internal fixation devices, such as Kirschner wires or bulky plates, highly susceptible to causing skin irritation, hardware erosion, and extensor tendon attritional ruptures. Volarly, the joint is supported by the thick fibrocartilaginous volar plate, which is intimately associated with the A1 pulley of the flexor tendon sheath.
Biomechanically, the functional utility of the hand is heavily dependent on the spatial orientation of the fused MCP joint. The optimal angle of fusion is not uniform across the hand; rather, it must meticulously adhere to the natural cascade of the digits. The index finger is typically fused in 20 to 25 degrees of flexion. This relatively extended position optimizes pulp-to-pulp and key pinch with the thumb, prioritizing precision over power. Moving ulnarly, the angle of fusion progressively increases: the long finger is fused at 25 to 30 degrees, the ring finger at 30 to 35 degrees, and the small finger at 35 to 40 degrees. This greater degree of flexion in the ulnar digits is critical for maintaining a strong power grip and accommodating the natural cupping of the transverse metacarpal arch. Malrotation is the most poorly tolerated error in finger arthrodesis. Because the axes of flexion of the fingers normally converge toward the scaphoid tubercle, even a seemingly trivial 5-degree rotational error at the MCP joint can result in up to 1.5 cm of digital overlap at the fingertips during flexion, severely impairing the patient's ability to grasp objects.
Exhaustive Indications and Contraindications
The decision to proceed with a metacarpophalangeal joint arthrodesis requires a nuanced evaluation of the patient's functional demands, the etiology of joint destruction, and the status of the adjacent joints. The procedure is inherently a trade-off: the patient sacrifices a significant arc of motion in exchange for absolute stability and the eradication of pain. Consequently, patient selection and comprehensive preoperative counseling are of paramount importance.
Primary indications for MCP joint arthrodesis include advanced post-traumatic osteoarthritis characterized by severe articular comminution or chronic, unbraceable instability. In the rheumatoid population, while arthroplasty is generally preferred, arthrodesis is indicated in cases of advanced disease with severe ulnar drift, volar subluxation, and inadequate bone stock or soft tissue integrity to support a silicone spacer. Paralytic deformities, such as intractable claw hand deformities resulting from complex nerve palsies where tendon transfers are not viable, also serve as robust indications. Furthermore, arthrodesis is the definitive salvage procedure for a failed silicone or pyrolytic carbon implant arthroplasty, particularly when complicated by significant osteolysis or particulate synovitis. Finally, sequelae of septic arthritis resulting in total joint destruction necessitate fusion, provided the infection has been definitively eradicated prior to the reconstructive effort.
Contraindications must be strictly respected to avoid catastrophic postoperative complications. Active, untreated local or systemic infection is an absolute contraindication; any arthrodesis attempted in an infected bed is virtually guaranteed to fail and may lead to osteomyelitis or systemic sepsis. Severe vascular compromise to the digit is another absolute contraindication, as the surgical dissection and subsequent immobilization can precipitate digital ischemia and necrosis. Relative contraindications include non-compliant patients who are unable to adhere to stringent postoperative rehabilitation protocols, as well as patients with concomitant severe arthritis of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints in the same digit. A completely stiff ray severely limits hand function and may be more detrimental to the patient than the pre-existing pathology.
Indications and Contraindications Summary
| Category | Specific Condition | Clinical Rationale and Considerations |
|---|---|---|
| Absolute Indications | Severe Post-Traumatic OA | Joint is unreconstructable; high-demand patient requires stable pinch/grip. |
| Absolute Indications | Failed Arthroplasty with Bone Loss | Lack of bone stock and ligamentous support precludes revision arthroplasty. |
| Absolute Indications | Unreconstructable Paralytic Claw Hand | Stabilizes the proximal phalanx to allow extrinsic extension of the IP joints. |
| Relative Indications | Advanced Rheumatoid Arthritis | Reserved for cases with profound ulnar drift, volar subluxation, or failed prior soft tissue balancing. |
| Absolute Contraindications | Active Local or Systemic Infection | High risk of hardware seeding, osteomyelitis, and systemic dissemination. |
| Absolute Contraindications | Severe Digital Ischemia | Surgical exposure and tourniquet use may precipitate irreversible digital necrosis. |
| Relative Contraindications | Concomitant Severe PIP/DIP Arthritis | Fusing the MCP joint in a digit with stiff IP joints creates an entirely rigid, non-functional ray. |
| Relative Contraindications | Patient Non-Compliance | Inability to follow immobilization protocols increases the risk of hardware failure and nonunion. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful metacarpophalangeal joint arthrodesis. The clinical evaluation must extend beyond the affected joint to encompass the entire upper extremity. The surgeon must thoroughly assess the soft tissue envelope, noting any prior surgical scars, areas of skin atrophy, or signs of compromised vascularity. The mobility and stability of the adjacent proximal interphalangeal (PIP), distal interphalangeal (DIP), and carpometacarpal (CMC) joints must be rigorously documented. Fusing an MCP joint places significantly increased biomechanical stress on the adjacent IP joints; therefore, pre-existing IP joint arthritis may rapidly accelerate following an MCP fusion.
Radiographic evaluation is mandatory and should include true anteroposterior (AP), lateral, and oblique views of the affected hand and specific digits. These images allow the surgeon to assess the degree of bone loss, the presence of osteophytes, and the overall alignment of the ray. In cases of revision surgery following a failed arthroplasty, or in the setting of severe post-traumatic deformity, a computed tomography (CT) scan with 3D reconstructions is highly recommended. The CT scan provides invaluable information regarding the volumetric bone stock available for fixation and helps identify occult cystic changes or fracture lines that could compromise hardware purchase. Preoperative templating, whether digital or analog, is utilized to determine the anticipated bone resection angles and to estimate the appropriate sizing of internal fixation devices, particularly if headless compression screws or dorsal plates are to be utilized.
Patient positioning and operating room setup must be optimized to facilitate seamless surgical execution and intraoperative imaging. The procedure is typically performed under regional anesthesia, such as a supraclavicular or axillary brachial plexus block, which provides excellent intraoperative operating conditions and prolonged postoperative analgesia. General anesthesia may be employed based on patient preference or if prolonged surgical duration is anticipated (e.g., multiple concurrent fusions). The patient is placed in the supine position with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg (or 100 mmHg above the patient's systolic blood pressure) following meticulous exsanguination of the limb with an Esmarch bandage. A mini-C-arm fluoroscopy unit must be draped into the sterile field and positioned to allow for unimpeded, orthogonal imaging throughout the procedure. Continuous fluoroscopic feedback is critical for confirming osteotomy angles, verifying perfect joint reduction, and ensuring precise hardware placement.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an MCP joint arthrodesis demands precision, respect for the soft tissues, and rigid adherence to biomechanical principles. While numerous fixation constructs exist, the underlying principles of joint preparation and alignment remain universal. The following details the modified tension band technique, alongside contemporary alternatives.
Incision, Exposure, and Joint Preparation
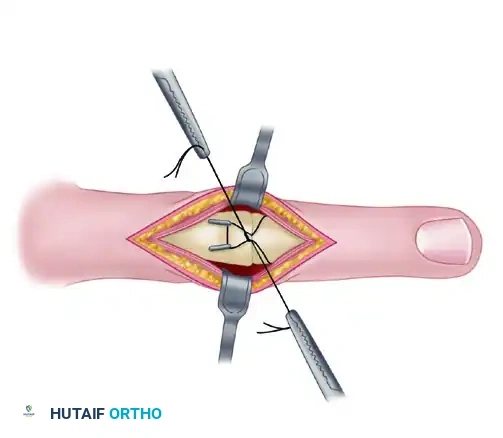
The approach begins with a dorsal longitudinal or transverse incision centered over the MCP joint. A longitudinal incision is generally preferred if multiple adjacent joints are being addressed, if future hardware removal is anticipated, or if extensive exposure of the metacarpal shaft is required. The dissection proceeds carefully through the subcutaneous tissues, with meticulous hemostasis achieved via bipolar electrocautery. The dorsal sensory branches of the radial and ulnar nerves must be identified and gently retracted using vessel loops to prevent painful postoperative neuromas.
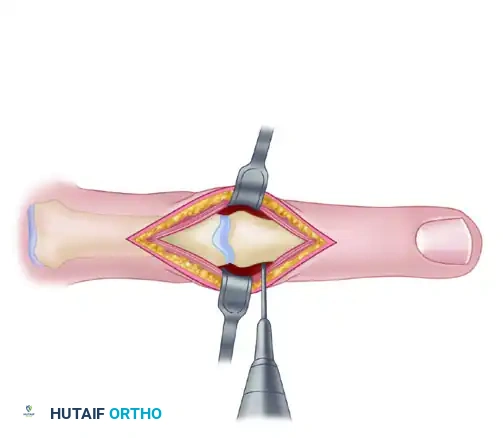
The extensor mechanism is identified, and the extensor hood and joint capsule are split longitudinally, precisely in the midline of the central extensor tendon. The extensor mechanism is retracted radially and ulnarly, exposing the dorsal aspect of the joint. To achieve comprehensive exposure, the collateral ligaments must be sharply released from their origins on the metacarpal head. This critical maneuver allows the joint to be hyperflexed—the so-called "shotgun" approach—completely exposing the articular surfaces of both the metacarpal head and the proximal phalangeal base.
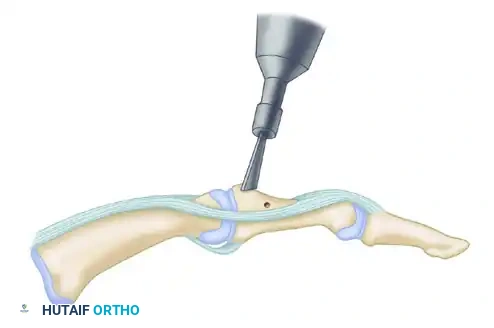
Using a rongeur, curette, or high-speed burr, all remaining articular cartilage and fibrous tissue are meticulously removed. The subchondral bone is aggressively debrided down to healthy, bleeding cancellous bone. This step is non-negotiable; a robust biologic environment is essential for achieving a solid osseous union.
Osteotomy and Surface Shaping
The preparation of the bony surfaces dictates the final alignment and stability of the arthrodesis. Two primary techniques are employed:
- Flat Cuts: Utilizing a microsagittal saw or sharp osteotomes, the articular surfaces are resected to achieve the desired angle of fusion. The cuts must be perfectly parallel when the joint is placed in the target position. While technically straightforward, flat cuts shorten the digit and offer minimal intrinsic stability prior to fixation.
- Cup-and-Cone (Ball-and-Socket) Technique: This highly advantageous technique preserves digital length and allows for infinite micro-adjustments in angulation and rotation. A concave reamer is used on the proximal phalangeal base to create a "socket," while a convex reamer or rongeur shapes the metacarpal head into a matching "ball." This intrinsic congruency maximizes cancellous bone contact and significantly enhances the stability of the final construct.
Tension Band Arthrodesis Technique
The modified tension band technique (Stern et al.; Segmüller) provides exceptional biomechanical stability by converting the physiological flexion forces exerted by the flexor tendons into dynamic compressive forces across the palmar aspect of the arthrodesis site.
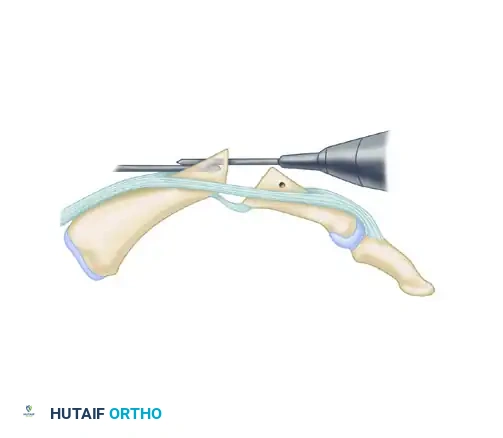
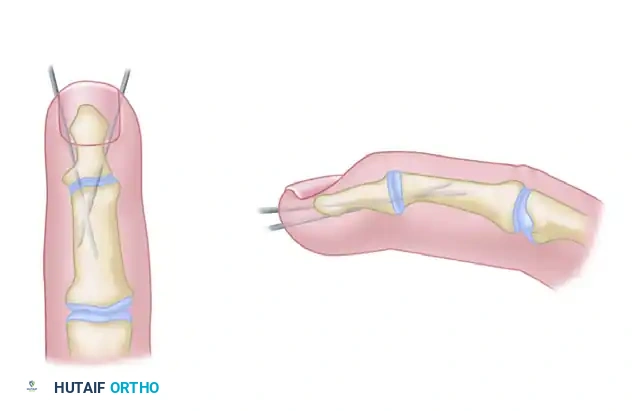
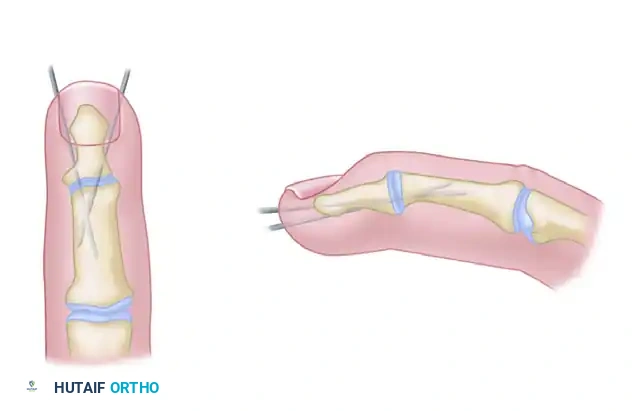
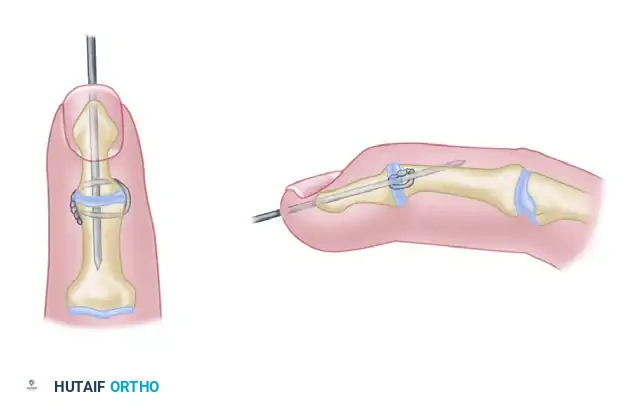
First, prepare for the tension band by drilling a transverse hole through the proximal phalanx using a 0.028-inch Kirschner wire. This hole must be positioned 5 to 10 mm distal to the fusion site and slightly dorsal to the midaxial line. Thread a 24-gauge or 26-gauge stainless steel wire through this hole, leaving equal lengths on both sides.
Next, drive two 0.035-inch or 0.045-inch K-wires retrograde into the metacarpal head. These wires should be directed proximally and dorsally, exiting the dorsal cortex of the metacarpal approximately 10 to 15 mm proximal to the fusion site. Withdraw the wires until their distal tips are flush with the resected surface of the metacarpal head.
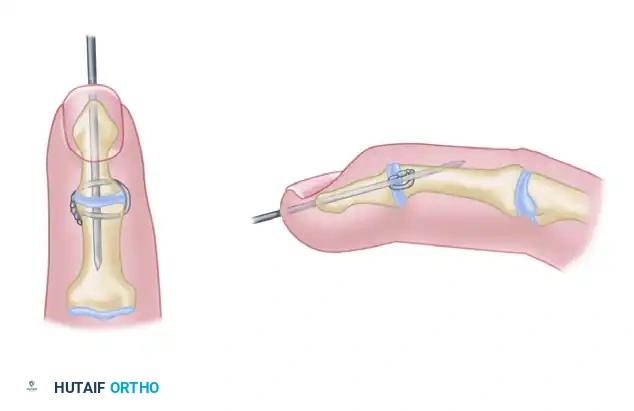
Reduce the joint, meticulously compressing the cut bone surfaces together. This is the critical moment to assess for malrotation. Flex the adjacent digits to ensure the fingertips point symmetrically toward the scaphoid tubercle. Once alignment is perfect, drive the K-wires antegrade across the arthrodesis site and into the proximal phalanx. Crucially, seat the tips of the K-wires firmly into the palmar cortex of the proximal phalanx without penetrating it, preventing hardware back-out and flexor tendon irritation.
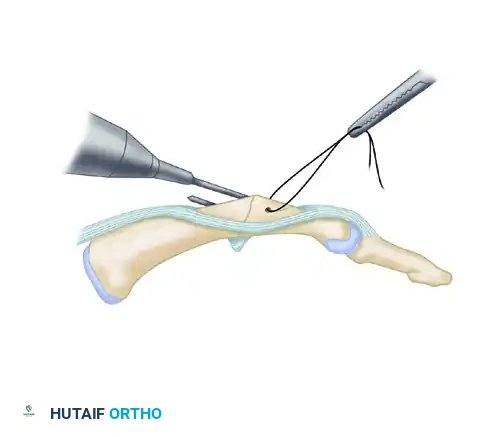
Finally, loop the stainless steel wire around the protruding dorsal ends of the K-wires in a figure-of-eight configuration. Obtain biplanar fluoroscopy to confirm alignment. Twist the ends of the steel wire together symmetrically to generate compression. Bend the proximal ends of the K-wires 180 degrees over the steel wire loops, cut them short, and bury the sharp ends deep to the extensor mechanism.
Alternative Fixation Techniques
While the tension band is robust, the thin dorsal skin can make prominent hardware problematic. Alternative techniques are frequently employed based on surgeon preference and patient anatomy.
Crossed Kirschner Wires: A simple, cost-effective method involving two crossed 0.045-inch K-wires. While lacking dynamic compression, it is highly effective for patients with poor soft tissue envelopes. The wires can be left proud for easy removal in the clinic after clinical union is achieved.
Interfragmentary Wire and Longitudinal K-wire: This technique utilizes a single longitudinal K-wire for axial stability, supplemented by an interosseous wire loop placed in the dorsal cortex to provide compression and control rotation.
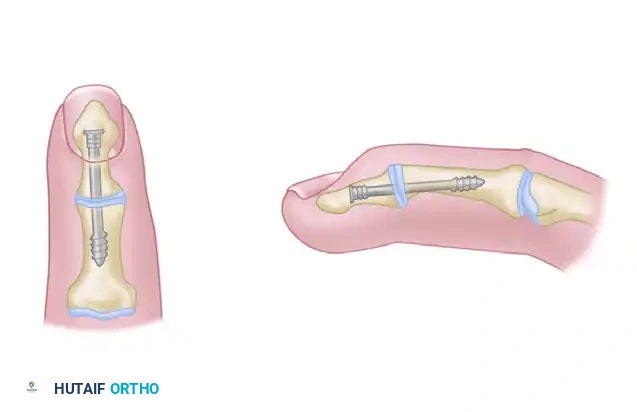
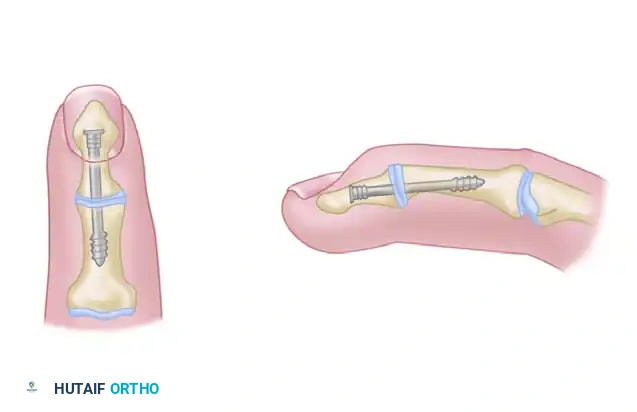
Headless Compression Screws: Headless compression screws (e.g., Herbert, Acutrak) are increasingly preferred due to their ability to be completely buried, eliminating dorsal hardware prominence. The screw is typically inserted antegrade from the dorsal base of the proximal phalanx into the metacarpal shaft. The cup-and-cone preparation is highly recommended when using screws, as it provides the intrinsic rotational stability that a single screw lacks.
Following definitive fixation, the wound is thoroughly irrigated. The extensor mechanism is meticulously repaired using 4-0 absorbable sutures, ensuring smooth tendon glide over any buried hardware. The skin is closed with non-absorbable sutures, and a bulky, non-compressive soft dressing reinforced with a volar plaster splint is applied.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, metacarpophalangeal joint arthrodesis carries a distinct profile of potential complications. Anticipating these pitfalls and understanding the appropriate salvage pathways is essential for the operating surgeon. The most significant complications involve failures of biologic healing (nonunion), errors in spatial alignment (malunion), and soft tissue morbidities related to the internal fixation construct.
Nonunion is a devastating complication, occurring in approximately 5% to 10% of cases across large clinical series. The etiology is often multifactorial, with significant risk factors including active smoking, inadequate surgical debridement of sclerotic subchondral bone, thermal necrosis generated by the improper use of power saws, and insufficient mechanical stability of the fixation construct. Patients typically present with persistent pain at the arthrodesis site, swelling, and a lack of bridging trabeculae on serial radiographs beyond 12 weeks. The management of a symptomatic nonunion mandates a revision surgical procedure. The fibrous nonunion must be aggressively excised back to bleeding bone, autologous cancellous bone graft (typically harvested from the distal radius or iliac crest) must be interposed, and rigid internal fixation—often utilizing a dorsal locking plate—must be applied to ensure absolute stability.
Malunion, particularly rotational malunion, represents a profound functional failure even in the presence of solid osseous healing. As previously noted, the digital cascade requires precise rotational alignment; a minor deviation at the MCP joint is magnified distally, resulting in digital scissoring and a severely compromised grip. Angular malunions, such as excessive extension or excessive flexion, impair pinch mechanics and power grip, respectively. If recognized intraoperatively, malalignment must be corrected immediately before final hardware tightening. If a symptomatic malunion is diagnosed postoperatively after consolidation has occurred, a corrective closing-wedge or rotational osteotomy through the fusion mass is required, followed by rigid re-fixation.
Hardware prominence is uniquely problematic at the MCP joint due to the exceptionally thin dorsal soft tissue envelope. Prominent Kirschner wires, bulky wire knots from tension bands, or proud screw heads can cause severe skin irritation, ulceration, and direct mechanical abrasion of the overlying extensor tendons, potentially leading to attritional tenosynovitis or outright tendon rupture. If hardware becomes symptomatic after definitive clinical and radiographic union has been achieved, routine hardware removal is indicated and typically resolves the issue. Infection, ranging from superficial pin tract erythema to deep osteomyelitis, requires prompt intervention. Superficial infections associated with exposed K-wires are generally managed with oral antibiotics and local pin care; however, deep infections necessitate aggressive surgical debridement, removal of all hardware, culture-directed intravenous antibiotics, and eventual revision arthrodesis once the infectious burden is cleared.
Complications and Salvage Management Summary
| Complication | Estimated Incidence | Primary Prevention Strategy | Definitive Salvage Management |
|---|---|---|---|
| Nonunion | 5 - 10% | Meticulous bone debridement; rigid fixation; smoking cessation. | Revision arthrodesis with autologous bone grafting and rigid plate fixation. |
| Rotational Malunion | 2 - 5% | Intraoperative assessment of digital cascade prior to final fixation. | Corrective rotational osteotomy through the fusion mass and re-fixation. |
| Hardware Prominence | 15 - 25% | Burying K-wire ends deep to extensor mechanism; using headless screws. | Hardware removal after confirmation of solid radiographic union. |
| Extensor Tendon Rupture | < 2% | Precise repair of extensor hood; avoiding dorsal hardware protrusion. | Hardware removal, tendon debridement, and primary repair or tendon transfer. |
| Deep Infection | 1 - 3% | Strict sterile technique; avoiding surgery in presence of active infection. | Aggressive I&D, hardware removal, IV antibiotics, delayed reconstruction. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following metacarpophalangeal joint arthrodesis must strike a delicate balance between protecting the healing arthrodesis site and preventing stiffness in the adjacent, non-operated joints. A phased, clearly communicated protocol is essential for optimizing functional outcomes and preventing hardware failure.
Phase I: Immediate Postoperative Phase (0 to 2 Weeks)
The primary goals during the first two weeks are wound healing, edema control, and strict protection of the fixation construct. Immediately following surgery, the hand is immobilized in a bulky, non-compressive soft dressing reinforced with a custom volar plaster or fiberglass splint. The wrist is positioned in approximately 20 to 30 degrees of extension to optimize venous and lymphatic return, while the fused MCP joint is supported in its surgically determined angle. Strict elevation of the extremity above the level of the heart is enforced to minimize postoperative edema, which can compromise wound healing and exacerbate pain. The patient is instructed to perform active range of motion exercises of the shoulder and elbow to prevent proximal stiffness.
Phase II: Early Mobilization and Splinting (2 to 6 Weeks)
At the first postoperative clinic visit (typically 10 to 14 days), the bulky dressing is removed, and the surgical incision is inspected. Sutures are removed if the wound is adequately healed. If rigid internal fixation (such as a tension band or headless compression screw) was achieved and the patient is deemed compliant, a prolonged period of rigid cast immobilization is usually unnecessary. Instead, a custom-fabricated thermoplastic splint is provided. This splint protects the MCP joint but is designed to allow free, unrestricted motion of the wrist and the proximal and distal interphalangeal (PIP and DIP) joints. Aggressive active and active-assisted range of motion of the PIP and DIP joints is initiated immediately. This is a critical step; failure to mobilize the IP joints early will result in profound stiffness and tendon adhesions, negating the functional benefits of the MCP arthrodesis.
Phase III: Consolidation and Weaning (6 to 12 Weeks)
Serial radiographs (AP, lateral, and oblique views) are obtained at the 6-week mark to assess for the presence of bridging trabeculae across the arthrodesis site. If clinical stability is apparent (absence of pain with gentle stress) and early radiographic consolidation is visible, the patient is gradually weaned from the thermoplastic splint during the day, utilizing it only for high-risk activities, manual labor, or sleep. Progressive strengthening exercises, focusing on grip and pinch strength, are introduced under the guidance of a certified hand therapist. Passive stretching of the IP joints may be initiated if residual stiffness persists.
Phase IV: Return to Unrestricted Activity (> 12 Weeks)
Final radiographic evaluation is typically performed at 10 to 12 weeks postoperatively. Once definitive, robust osseous union is confirmed radiographically and the patient is pain-free at the fusion site, all restrictions are lifted. The patient is cleared to return to heavy manual labor, contact sports, and all activities of daily living. It is important to counsel the patient that maximal grip strength and functional adaptation to the fused joint may take up to 6 to 12 months to fully realize.
Summary of Landmark Literature and Clinical Guidelines
The evolution of metacarpophalangeal joint arthrodesis is deeply rooted in biomechanical research and extensive clinical outcome studies. A thorough understanding of the landmark literature provides the evidence-based foundation for contemporary surgical decision-making.
The biomechanical superiority of the tension band technique in the hand was definitively established by the foundational work of Stern et al. and the modifications proposed by Segmüller. Their studies demonstrated that dorsally applied tension band constructs effectively neutralize the powerful volar bending moments exerted by the extrinsic flexor tendons, converting these disruptive forces into beneficial dynamic compression at the volar cortex of the arthrodesis site. This principle remains the gold standard against which newer fixation modalities are measured.
The conceptualization and popularization of the cup-and-cone (ball-and-
