Wrist Arthrodesis: Comprehensive Surgical Principles and Techniques
Key Takeaway
Wrist arthrodesis is a highly effective salvage procedure indicated for severe wrist flexion contractures in nonfunctional hands. Primarily utilized to control position and facilitate hygiene, the procedure often incorporates a proximal row carpectomy to correct deformity and supply autologous bone graft. To prevent physeal arrest, fusion is delayed until skeletal maturity. This guide details the step-by-step surgical technique, including the dorsal approach, cartilage denudation, and Steinmann pin fixation for optimal outcomes.
Comprehensive Introduction and Patho-Epidemiology
Total wrist arthrodesis is a highly reliable, definitive, and structurally transformative salvage procedure in the armamentarium of the orthopedic hand and upper extremity surgeon. Historically conceptualized as a procedure of last resort for the eradication of intractable radiocarpal and intercarpal pain, its indications have broadened and evolved significantly over the past several decades. The operation is meticulously designed to provide rigid osseous stability, correct severe multiplanar deformities, and alleviate the debilitating pain associated with end-stage articular degeneration. While frequently and successfully employed for end-stage post-traumatic arthritis (such as advanced Scapholunate Advanced Collapse [SLAC] or Scaphoid Nonunion Advanced Collapse [SNAC]), rheumatoid arthritis with profound carpal subsidence, and various paralytic conditions, its application in the severely contracted, nonfunctional hand represents a highly unique, biomechanically demanding, and clinically challenging scenario.
The patho-epidemiology of the nonfunctional, spastic hand is rooted in profound upper motor neuron lesions. Patients presenting with severe wrist flexion contractures typically suffer from underlying neurological catastrophes, including severe cerebral palsy, devastating traumatic brain injury (TBI), advanced cerebrovascular accidents (stroke), or the ischemic sequelae of an advanced Volkmann ischemic contracture. In these profound neurological deficits, the delicate balance between the flexor and extensor musculature is irrevocably lost. The flexor pronator mass, innervated by the median and ulnar nerves, overpowers the extensor compartments, leading to a relentless, progressive flexion and pronation posture. Over time, this dynamic spasticity transitions into a rigid, fixed myostatic contracture as the sarcomeres shorten, the joint capsules fibrose, and the volar radiocarpal ligaments undergo irreversible adaptive shortening.
In these exceptionally complex cases, the primary goal of surgical intervention paradigm shifts dramatically. The surgeon is no longer operating to restore fine motor kinematics, optimize the tenodesis effect for grip strength, or preserve the dart-thrower's arc of motion. Instead, the surgical objective is fundamentally palliative and facilitative: to control the resting position of the terminal limb, prevent devastating skin maceration in the palmar creases, and dramatically improve the ability of caregivers to perform basic hygiene. A hand driven rigidly into the palm by unyielding spasticity is highly susceptible to recurrent fungal infections, severe intertrigo, pressure ulcerations, and eventual osteomyelitis. By executing a total wrist arthrodesis, the surgeon provides a stable, unified skeletal platform that resists the relentless pull of the spastic flexors, thereby transforming a contracted, unhygienic appendage into a manageable, cosmetically acceptable, and easily nursed limb.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the osseous, ligamentous, and neurovascular anatomy of the wrist is an absolute prerequisite for the safe and effective execution of a total wrist arthrodesis. The radiocarpal joint is a complex, multi-articulated condyloid joint. The osseous architecture involves the biconcave distal articular surface of the radius (comprising the scaphoid and lunate fossae) articulating with the convex proximal surfaces of the scaphoid and lunate. The midcarpal joint, a highly complex articulation between the proximal and distal carpal rows, contributes significantly to the global arcs of flexion, extension, and radial-ulnar deviation. In the setting of total wrist arthrodesis, the surgeon must systematically obliterate these articulations, effectively converting the radius, carpus, and metacarpals into a single, continuous biomechanical lever arm.
The ligamentous anatomy of the wrist is divided into intrinsic and extrinsic systems. The stout volar extrinsic ligaments (such as the radioscaphocapitate and long radiolunate ligaments) are the primary stabilizers of the carpus. In the spastic, contracted hand, these volar structures become densely contracted and fibrotic. Conversely, the dorsal radiocarpal ligaments are often attenuated. Surgical exposure relies on a dorsal approach, necessitating a meticulous understanding of the extensor retinaculum and its six distinct fibro-osseous compartments. The third dorsal compartment, housing the extensor pollicis longus (EPL), serves as the primary anatomical landmark. Transposition of the EPL allows for the subperiosteal elevation of the second compartment (extensor carpi radialis longus and brevis) and the fourth compartment (extensor digitorum communis and extensor indicis proprius). Preserving thick, full-thickness dorsal capsular flaps during this dissection is critical to ensure adequate soft-tissue coverage over the eventual hardware and bone graft, mitigating the risk of wound breakdown and hardware prominence.
Biomechanically, the normal wrist transmits approximately 80% of axial loads through the radiocarpal joint and 20% through the ulnocarpal axis. Following a total wrist arthrodesis, the entirety of the load is transferred directly from the metacarpals through the fused carpal mass into the distal radius. In the functional hand, arthrodesis is typically positioned in 10° to 15° of extension to optimize the length-tension relationship of the extrinsic finger flexors, maximizing grip strength. However, in the spastic, nonfunctional hand, biomechanical priorities dictate a different alignment. Fusing the wrist in neutral or slight flexion reduces the tension on the volar neurovascular bundle—specifically the median nerve—which is acutely at risk of stretch-induced ischemic neuropathy when a severe, long-standing flexion contracture is corrected. Furthermore, incorporating a proximal row carpectomy (PRC) into the arthrodesis procedure biomechanically shortens the skeletal column. This relative shortening of the radius-to-metacarpal distance effectively decompresses the volar soft tissues, allowing for deformity correction without catastrophic neurovascular tension or the need for massive, morbid flexor tendon lengthenings.
Exhaustive Indications and Contraindications
The decision to proceed with a total wrist arthrodesis, particularly in the nonfunctional hand, must be the culmination of a rigorous, multidisciplinary evaluation involving orthopedic surgeons, neurologists, physiatrists, and occupational therapists. The procedure is strictly indicated only when exhaustive conservative measures—including aggressive static and dynamic splinting, targeted botulinum toxin A (Botox) injections into the flexor pronator mass, serial casting, and intensive physical therapy—have definitively failed to halt the progression of the deformity or alleviate the associated nursing burden.
Primary Surgical Indications
The indications for total wrist arthrodesis vary significantly based on the functional status of the extremity. In the nonfunctional, spastic hand, the primary indications include:
* Severe, Fixed Flexion Contractures: Deformities that are rigid and preclude passive extension to a neutral position, often resulting in the digits being forcefully driven into the volar palm, rendering the hand inaccessible.
* Hygiene and Nursing Care Impairment: The inability of caregivers to access and clean the palmar crease, leading to a vicious cycle of recurrent fungal infections, severe skin maceration, intertrigo, and eventual cutaneous breakdown.
* Cosmesis and Limb Positioning: Improving the overall resting posture and appearance of the limb. This provides immense psychological and social benefits to the patient and their caregivers, facilitating easier dressing and integration into daily life.
* Refractory Spasticity Management: Providing a rigid, unyielding skeletal platform to counteract severe, medically refractory flexor spasticity, thereby preventing the recurrence of the deformity.
Absolute and Relative Contraindications
- Open Physes (Absolute): In pediatric patients, the distal radial physis contributes approximately 75% of the longitudinal growth of the radius. Surgical preparation of the radiocarpal joint inevitably destroys this growth plate. Therefore, arthrodesis must be delayed until skeletal maturity (typically age 12 or older). Premature fusion will result in a devastating physeal arrest, severe ulnar positive variance, distal radioulnar joint (DRUJ) dislocation, and a progressive Madelung-type deformity.
- Active Infection (Absolute): Any active local or systemic infection must be completely eradicated prior to the implantation of hardware and bone graft.
- Functionally Adaptable Partial Fusions (Relative): In a hand with preserved function, if the midcarpal joint is spared from arthritis, a partial wrist fusion (e.g., radioscapholunate fusion) may be preferable to preserve a functional arc of motion.
- Critically Compromised Soft Tissue Envelope (Relative): Severe dorsal skin atrophy or previous radiation therapy may preclude safe dorsal exposure and hardware coverage.
Indication Matrix: Functional vs. Nonfunctional Hand
| Clinical Parameter | Functional Hand (e.g., RA, Post-Traumatic) | Nonfunctional Spastic Hand (e.g., CP, TBI) |
|---|---|---|
| Primary Goal | Pain relief, restoration of grip strength, stability | Hygiene, cosmesis, prevention of skin maceration |
| Optimal Position | 10° - 15° Extension, slight ulnar deviation | Neutral to slight flexion, slight ulnar deviation |
| Neurovascular Risk | Low (deformity is usually not severely contracted) | High (median nerve stretch neuropathy during correction) |
| Skeletal Shortening | Rarely required (PRC not typically indicated for length) | Frequently required (PRC utilized to shorten skeletal column) |
| Hardware Choice | Dorsal spanning plate (standard of care) | Steinmann pins (often preferred due to poor bone stock/PRC) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful total wrist arthrodesis. The clinical evaluation must rigorously assess the passive and active range of motion of the wrist, digits, and elbow. In the spastic patient, the surgeon must differentiate between dynamic spasticity (which may resolve under general anesthesia or with nerve blocks) and fixed myostatic contracture (which requires structural release). The viability of the dorsal soft tissue envelope must be scrutinized, as prior surgeries, trauma, or profound disuse atrophy can compromise wound healing.
Radiographic evaluation requires standard posteroanterior (PA), lateral, and oblique views of the wrist. In cases of severe flexion contractures, obtaining true orthogonal views may be technically impossible; however, the surgeon must assess the available bone stock, the presence of severe osteopenia (common in non-ambulatory, spastic patients), and the status of the carpometacarpal (CMC) joints. If the CMC joints are arthritic or unstable, the fusion mass must be extended distally to incorporate the bases of the second and third metacarpals to prevent adjacent segment breakdown.
Physeal Considerations and Timing
As previously emphasized, the timing of the arthrodesis in the pediatric or adolescent patient is governed entirely by skeletal maturity. The surgeon must confirm closure of the distal radial physis radiographically before proceeding. If severe deformity necessitates intervention prior to skeletal maturity, soft tissue procedures—such as fractional lengthening of the flexor tendons, proximal row carpectomy without fusion, or temporary spanning external fixation—must be employed as temporizing measures until definitive arthrodesis can be safely performed.
Patient Positioning and Operating Room Setup
The patient is placed in the supine position with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is critical for the meticulous denudation of articular cartilage. The fluoroscopy unit (C-arm) must be positioned parallel to the hand table, allowing for seamless intraoperative imaging in both the PA and lateral planes without compromising the sterile field. Preoperative intravenous antibiotics are administered within one hour of the initial incision.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a total wrist arthrodesis in the severely contracted hand is a highly orchestrated procedure that demands simultaneous management of the soft tissue contractures and the osseous deformity. The technique detailed below utilizes Steinmann pin fixation, which is particularly advantageous in spastic patients with osteopenic bone stock, or when a proximal row carpectomy (PRC) is performed, rendering standard dorsal plate application technically challenging or impossible due to the shortened skeletal bed.
1. Volar Soft Tissue Release and Preparation
Before addressing the dorsal skeletal anatomy, the volar soft tissue constraints must be evaluated and released. Under general anesthesia, assess the degree of fixed contracture. If the wrist cannot be passively brought to a neutral position, volar releases are mandatory. Make a longitudinal or zig-zag incision over the volar distal forearm. Perform a fractional lengthening of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons at their musculotendinous junctions. In cases of extreme spasticity, a formal flexor-pronator slide may be required. These releases decompress the volar soft tissues, allowing the wrist to be extended without placing catastrophic traction on the median nerve.
2. Dorsal Approach and Extensor Retinaculum Management
Exsanguinate the limb and inflate the tourniquet. Make a dorsal longitudinal incision, approximately 8 to 10 centimeters in length, centered directly over the Lister tubercle and extending from the distal third of the radius to the base of the third metacarpal. Deepen the dissection through the subcutaneous tissues, meticulously identifying and protecting the superficial sensory branch of the radial nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly. Expose the extensor retinaculum. Incise the retinaculum sharply over the third dorsal compartment and transpose the extensor pollicis longus (EPL) tendon radially. Elevate the second compartment (ECRL, ECRB) radially and the fourth compartment (EDC, EIP) ulnarly. This subperiosteal elevation must include thick, robust flaps of the dorsal radiocarpal capsule to expose the underlying radiocarpal and midcarpal articulations fully.
3. Proximal Row Carpectomy (PRC) for Skeletal Shortening
In the severely contracted, nonfunctional hand, excising the proximal carpal row is a critical maneuver. Utilizing sharp dissection, elevators, and rongeurs, systematically excise the scaphoid, lunate, and triquetrum. This maneuver effectively shortens the skeletal column of the wrist by approximately 1.5 to 2.0 centimeters. This skeletal shortening is paramount; it allows the residual carpus (capitate and hamate) to be apposed to the distal radius in a neutral position without placing undue tension on the volar neurovascular bundle. Carefully preserve the volar radiocarpal ligaments during the excision to maintain a stable volar soft-tissue hinge.
4. Joint Preparation and Cartilage Denudation
The success of any arthrodesis relies on the meticulous preparation of the fusion bed. All remaining articular cartilage must be aggressively removed down to healthy, bleeding subchondral bone. Utilize a combination of sharp osteotomes, rongeurs, and a high-speed burr to denude the articular surfaces of the scaphoid and lunate fossae of the distal radius. Similarly, denude the proximal articular surfaces of the capitate and hamate, as well as the intercarpal articulations between the distal carpal row and the bases of the second and third metacarpals. The goal is to create broad, flat, highly vascularized cancellous bone surfaces that will interdigitate perfectly when reduced.
5. Bone Grafting
The excised proximal carpal bones (scaphoid, lunate, triquetrum) serve as an exceptional, highly osteogenic source of local corticocancellous autograft. Using a bone rongeur or a bone mill, morselize these carpal bones into small fragments. Pack this local autograft tightly into all the decorticated radiocarpal, intercarpal, and carpometacarpal spaces. This aggressively supplements the fusion mass and promotes rapid osteointegration. If the local bone stock is severely osteopenic, cystic, or insufficient in volume, the surgeon must be prepared to harvest supplemental cancellous autograft from the ipsilateral anterior iliac crest.
6. Skeletal Fixation via Steinmann Pins
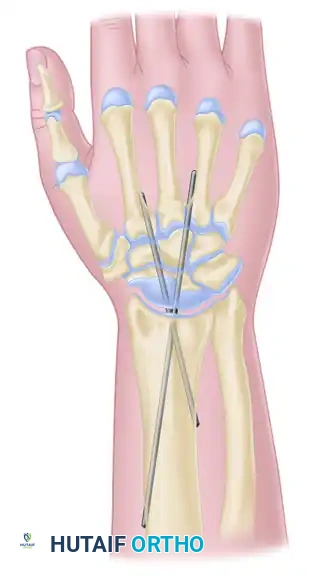
Once the joint surfaces are prepared and grafted, the wrist is reduced into the optimal position for the nonfunctional hand: neutral flexion (0 degrees) and slight ulnar deviation (5° to 10°). Rigid skeletal fixation is then achieved using heavy Steinmann pins.
Select two stout Steinmann pins, typically measuring 7/64 to 9/64 of an inch in diameter. The pins are driven in a retrograde fashion. Introduce the first pin through the dorsal aspect of the second metacarpal head or neck. Drive the pin proximally, traversing the metacarpal shaft, crossing the decorticated midcarpal and radiocarpal intervals, and seating it deeply into the dense medullary canal of the distal radius. Repeat this process with the second pin, introducing it through the third metacarpal.
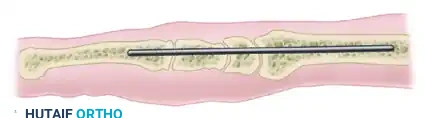
FIGURE 72-10 (A): Lateral schematic demonstrating the longitudinal trajectory of the Steinmann pin traversing the metacarpal, the remaining carpus, and seating securely within the medullary canal of the radius. Note the neutral alignment designed to prevent volar soft tissue tension.
It is critical that the pins cross the fusion sites at divergent angles. This divergent trajectory maximizes multiplanar rotational stability and resists the immense bending moments generated by the spastic flexor musculature. Confirm the precise position, depth, and trajectory of the hardware using multiplanar intraoperative fluoroscopy.
FIGURE 72-10 (B): Anteroposterior (AP) schematic illustrating wrist arthrodesis using two crossed Steinmann pins, providing rigid, divergent stabilization of the radiocarpal and midcarpal intervals.
Once optimal fixation is confirmed, the pins are cut. In the spastic patient population, it is highly recommended to cut the pins deeply beneath the skin surface. Leaving pins prominent or protruding through the skin invites pin tract infections and risks hardware back-out or self-injury during spastic episodes. Meticulously close the thick dorsal capsular flaps over the fusion site and the buried hardware using heavy absorbable sutures. This layer is critical for preventing hardware prominence and protecting the extensor tendons. Close the skin with non-absorbable sutures in a tension-free manner.
Complications, Incidence Rates, and Salvage Management
While total wrist arthrodesis is a definitive and generally reliable procedure, its application in the severely spastic, nonfunctional hand carries a unique and elevated complication profile. The immense, unyielding forces generated by spastic musculature constantly challenge the integrity of the fixation and the biology of the fusion mass. The surgeon must be acutely aware of these potential pitfalls and possess the reconstructive algorithms necessary to manage them.
Major Complications
- Nonunion and Pseudarthrosis: This remains the most frequent complication, particularly at the radiocarpal junction, which is the zone of highest biomechanical stress. Inadequate cartilage denudation, insufficient bone grafting, or premature hardware failure can lead to a fibrous nonunion. Interestingly, in the nonfunctional hand, a stable, asymptomatic fibrous nonunion may still achieve the clinical goals of hygiene and positioning and may not require revision.
- Hardware Failure and Migration: The spastic flexor tone places immense bending and pull-out forces on the Steinmann pins. Pins may migrate proximally into the radius or distally through the metacarpals, potentially breaching the skin. Routine radiographic surveillance is mandatory.
- Median Nerve Neuropathy: Attempting to forcefully correct a severe, long-standing flexion contracture to a neutral position without performing a proximal row carpectomy (PRC) or adequate volar flexor lengthenings will acutely stretch the median nerve. This can lead to devastating ischemia, severe neuropathic pain, and complex regional pain syndrome (CRPS).
- Wound Breakdown and Infection: The dorsal skin of the wrist is inherently thin and poorly vascularized. In spastic, malnourished patients, forcing the wrist into extension can blanch the dorsal skin, leading to full-thickness necrosis, hardware exposure, and deep osteomyelitis.
Complication Management Matrix
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Revision Strategy |
|---|---|---|---|
| Symptomatic Nonunion | 5% - 15% | Poor bone stock, inadequate graft, hardware micromotion | Revision open reduction, rigid plate fixation (if bone stock allows), massive iliac crest bone grafting. |
| Hardware Migration | 10% - 20% | Severe uncontrolled spasticity, non-divergent pin placement | Hardware removal once fusion is solid; early revision if migration causes loss of reduction. |
| Median Nerve Stretch | 2% - 5% | Over-correction of contracture, failure to perform PRC | Immediate release of dressings/cast; if unresolved, return to OR for skeletal shortening (PRC/ostectomy) or carpal tunnel release. |
| Dorsal Wound Necrosis | 3% - 8% | Excessive tension on closure, prominent hardware | Aggressive debridement, hardware removal if infected, coverage with local rotational flaps or free tissue transfer. |
Phased Post-Operative Rehabilitation Protocols
The postoperative management of a total wrist arthrodesis in the spastic patient is as critical as the surgical execution itself. Steinmann pin fixation, while advantageous for its low profile and adaptability to shortened skeletal beds, provides less absolute biomechanical stability than a rigid dorsal spanning plate. Consequently, the spasticity of the flexor musculature will constantly challenge the fixation, necessitating prolonged and rigid external immobilization.
Immediate Postoperative Phase (Weeks 0-4)
In the operating room, immediately following wound closure, the extremity is immobilized in a well-padded, bivalved long-arm cast. The elbow must be strictly immobilized at 90 degrees of flexion to control and neutralize the powerful forces of forearm pronation and supination, which can transmit rotational shear stresses across the radiocarpal fusion site. The forearm is maintained in neutral rotation. If the finger flexors (FDS/FDP) were lengthened volarly during the procedure, the volar aspect of the cast must be extended distally to include the digits in a fully extended position. This prevents the spastic flexors from contracting, which would compromise the tendon lengthening and place secondary deforming forces on the wrist. The limb must be strictly elevated above the level of the heart for the first 48 to 72 hours to mitigate postoperative edema and protect the tenuous dorsal skin envelope.
Intermediate Phase (Weeks 4-8)
At approximately 4 weeks postoperatively, the patient is evaluated in the outpatient clinic. The long-arm cast is carefully removed, and the surgical incisions are inspected for complete epithelialization. Radiographs (PA and lateral) are obtained to assess the position of the Steinmann pins, ensure maintenance of the skeletal alignment, and evaluate for early signs of bridging callus formation. If the clinical progression is satisfactory and the wounds are healed, the immobilization can be converted to a short-arm cast, freeing the elbow. At this stage, passive and active finger flexion is permitted and encouraged to prevent profound, irreversible stiffness of the metacarpophalangeal (MCP) and interphalangeal (IP) joints, provided that the volar flexor tendon lengthenings have healed sufficiently to withstand tension.
Late Phase (Weeks 8-12 and Beyond)
Rigid cast immobilization is typically continued for a minimum total of 8 to 12 weeks. The decision to discontinue casting is based strictly on definitive radiographic evidence of union, defined as the presence of mature, bridging trabeculae across both the radiocarpal and intercarpal intervals. Once osseous union is confirmed, the cast is permanently removed. However, in the severe spastic patient population, a custom-molded, removable thermoplastic splint is often fabricated by occupational therapy. This splint is utilized during periods of high physical activity, transfers, or during severe spastic episodes to provide supplemental support to the newly fused wrist. If the buried Steinmann pins become symptomatic under the skin or migrate superficially after the fusion is completely solid, they may be safely removed in a minor outpatient surgical procedure without compromising the structural integrity of the arthrodesis.
Summary of Landmark Literature and Clinical Guidelines
The evolution of total wrist arthrodesis has been heavily documented in the orthopedic literature, with distinct paradigms emerging for the functional arthritic hand versus the nonfunctional spastic hand. The foundational biomechanical principles of wrist fusion were established by Hastings and others, who demonstrated that the optimal position for grip strength in the functional hand is slight extension (10°-15°). However, literature specific to the spastic, nonfunctional hand—such as the landmark studies by Louis and colleagues—fundamentally shifted this paradigm, proving that neutral or slight flexion is imperative to prevent neurovascular compromise during the correction of severe myostatic contractures.
Clinical guidelines published by the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) emphasize the absolute necessity of delaying radiocarpal fusion until skeletal maturity to avoid devastating physeal arrest. Furthermore, contemporary literature strongly supports the integration of a proximal row carpectomy (PRC) during arthrodesis in the severely contracted hand. Studies have consistently shown that the skeletal shortening provided by a PRC significantly reduces the need for massive, morbid flexor tendon lengthenings and drastically lowers the incidence of postoperative median nerve stretch neuropathy. While dorsal spanning plate fixation remains the gold standard for functional, arthritic wrists due to its superior biomechanical rigidity, Steinmann pin fixation remains a highly validated, guideline-supported technique for the spastic population, particularly when bone stock is poor or when the skeletal bed has been shortened by a PRC, rendering plate application technically prohibitive.
🔗 Read the comprehensive guide: Operative Principles of Lower Extremity Arthrodesis: Ankle and Knee
