Knee Arthrodesis: A Lifelong Knee Solution for Trauma & TKA
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Knee Arthrodesis: A Lifelong Knee Solution for Trauma & TKA. Knee arthrodesis knee is a surgical salvage option for conditions like infected total knee arthroplasty (TKA) and severe knee trauma. This durable solution provides a stable, painless extremity, allowing for ambulation with less energy expenditure than an amputation. It's often chosen for patients needing a lifelong, functional knee fusion.
Comprehensive Introduction and Patho-Epidemiology
Knee arthrodesis remains an indispensable and highly effective salvage procedure within the armamentarium of the complex reconstructive orthopedic surgeon. Historically viewed as a procedure of last resort, it is now recognized as a definitive, lifelong solution for patients suffering from catastrophic joint destruction, most notably secondary to recalcitrant periprosthetic joint infection (PJI) following total knee arthroplasty (TKA), massive oncologic resections, and severe, unsalvageable periarticular trauma. The primary objective of knee arthrodesis is to provide the patient with a stable, painless, and durable lower extremity capable of sustaining functional ambulation over a lifetime, thereby avoiding the profound physical and psychological morbidity associated with amputation.
The physiological and metabolic advantages of knee arthrodesis over above-the-knee amputation (AKA) cannot be overstated, particularly in the context of the geriatric population or patients with significant cardiopulmonary comorbidities. Biomechanical studies and gait analyses have consistently demonstrated that the energy expenditure required for ambulation with a fused knee is significantly less than the energy expenditure demanded by an AKA with a prosthesis. For an elderly patient with compromised cardiopulmonary reserve, the increased metabolic demand of an AKA—often exceeding 60% above baseline—frequently results in the patient becoming permanently nonambulatory and wheelchair-bound. Conversely, a successful knee arthrodesis preserves the continuity of the limb and the proprioceptive feedback of the foot and ankle, allowing these fragile patients to maintain a functional degree of independence.
In the younger, high-demand post-traumatic demographic, knee arthrodesis serves a slightly different but equally critical role. Following high-energy trauma that results in devastating intra-articular comminution, massive bone loss, or severe soft tissue stripping, arthrodesis offers a highly durable construct that can withstand the rigors of heavy manual labor and physically demanding activities. Unlike a primary or revision TKA, which would be subject to rapid aseptic loosening, polyethylene wear, or mechanical failure under such extreme cyclical loading, a solid osseous fusion provides a permanent mechanical column.
The pathogenesis necessitating knee arthrodesis is almost universally characterized by extensive bone loss and profound soft tissue compromise. In the setting of an infected TKA, the combination of osteolysis from chronic infection, the mechanical destruction from loose components, and the obligate radical surgical débridement required to eradicate the pathogen leaves massive cavitary and segmental osseous defects. The resultant gap between the viable distal femur and proximal tibia frequently averages 4 centimeters but can easily exceed 7 to 10 centimeters in severe cases. Addressing this critical bone defect—whether through acute shortening, massive structural allografts, or distraction osteogenesis via bone transport—constitutes the fundamental surgical challenge of the procedure.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the altered surgical anatomy is paramount when undertaking a knee arthrodesis, particularly in the revision or salvage setting. The surgical approach is almost universally anterior, typically utilizing the patient's pre-existing midline longitudinal incision to minimize the risk of devascularizing the already precarious anterior skin flaps. In the context of a chronically infected TKA, the surgeon must anticipate a complete or near-complete deficiency of the extensor mechanism. The quadriceps tendon, patella, and patellar tendon are frequently attenuated, necrotic, or entirely absent due to prior resections or chronic infection, leading to a significant anterior soft tissue defect that complicates wound closure and hardware coverage.

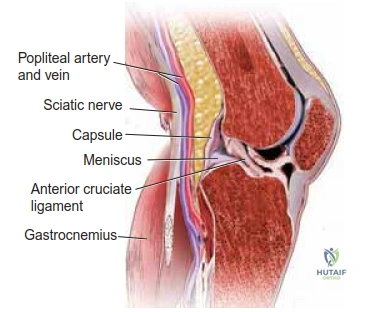
Achieving optimal bleeding bone contact between the distal femur and proximal tibia is the biological cornerstone of a successful arthrodesis. This requires meticulous preparation of the bone ends, which often necessitates the complete elevation of the posterior capsule off the posterior aspects of both the distal femur and proximal tibia. This posterior capsular release allows for the translation and coaptation of the osseous surfaces. However, this maneuver places the posterior neurovascular structures at significant risk. Directly posterior to the posterior capsule lies the popliteal artery, the popliteal vein, and the sciatic nerve as it bifurcates into the tibial and common peroneal nerves.
The proximity of this neurovascular bundle to the posterior aspects of the femur and tibia at the level of the residual joint space cannot be ignored. The popliteal artery is tethered proximally at the adductor hiatus and distally at the soleal arch. Because of these rigid anatomical fixation points, acute shortening of the limb by more than 5 to 6 centimeters during the fusion process can lead to severe kinking, redundancy, and subsequent thrombosis of the popliteal vessels. Furthermore, the anterior osseous structures are extremely subcutaneous, lacking a robust muscular envelope. The blood supply to this region is often tenuous, secondary to the relatively avascular nature of the scarred extensor mechanism remnants and the disruption of the genicular anastomoses from prior surgeries.
Biomechanically, the fused knee converts the lower extremity into a single, rigid lever arm extending from the center of the femoral head to the ankle mortise. This massive lever arm generates profound bending moments and torsional stresses at the fusion site during the stance phase of gait. To achieve successful arthrodesis, the chosen fixation construct must be robust enough to neutralize these immense forces until solid osseous union occurs. Furthermore, the loss of knee flexion eliminates the limb's primary shock-absorbing mechanism, transferring abnormal stresses to the ipsilateral hip, the contralateral hip (often exacerbated by a limb-length discrepancy), and the lumbar spine.
Exhaustive Indications and Contraindications
The decision to proceed with a knee arthrodesis is highly complex and must be individualized, weighing the patient's physiological age, functional demands, medical comorbidities, and the anatomical realities of the affected limb. The primary indication remains the infected total knee arthroplasty that has failed traditional two-stage revision, or where the host bone stock is so profoundly depleted that reimplantation of a revision prosthesis is biomechanically impossible.

Other absolute indications include severe, unsalvageable periarticular trauma resulting in massive articular destruction, unreconstructible extensor mechanism disruption in the setting of a TKA, and limb-sparing oncologic resections where endoprosthetic reconstruction is contraindicated. In specific scenarios, such as a patient with profound neurological deficits (e.g., severe poliomyelitis, complete femoral nerve palsy) resulting in a flail, unstable knee, arthrodesis provides the necessary stability for weight-bearing.
While knee arthrodesis is a powerful salvage tool, several relative and absolute contraindications exist. Severe, symptomatic ipsilateral hip or ankle arthritis is a strong relative contraindication. Because the knee will no longer accommodate motion, the adjacent joints must possess sufficient mobility and stability to compensate during the gait cycle; fusing the knee in the presence of a stiff, arthritic hip will lead to severe functional impairment and accelerated degeneration of the hip. Similarly, advanced degenerative disc disease or spinal stenosis can be significantly exacerbated by the altered gait mechanics of a fused knee.
| Category | Indications for Knee Arthrodesis | Contraindications (Relative & Absolute) |
|---|---|---|
| Infectious | Recalcitrant PJI failing 2-stage exchange; PJI with massive bone loss precluding reimplantation. | Active, uncontrolled systemic sepsis (Requires clearance prior to definitive fusion). |
| Traumatic | Unsalvageable intra-articular comminution; severe bone loss; irreparable extensor mechanism loss. | Severe ipsilateral hip/ankle arthritis (Relative); Contralateral AKA (Relative - creates severe mobility restriction). |
| Oncologic | Post-tumor resection where endoprosthetic reconstruction is not viable or has failed. | Terminal prognosis where prolonged rehabilitation is not aligned with goals of care. |
| Vascular / Soft Tissue | Stable soft tissue envelope capable of covering the arthrodesis site. | Severe Peripheral Vascular Disease (Absolute); Inadequate soft tissue coverage without flap options (Absolute). |
A thorough vascular assessment is critical. Severe peripheral vascular disease (PVD) is an absolute contraindication, as the compromised blood flow will invariably lead to nonunion, wound breakdown, and ultimate amputation. Contralateral above-knee amputation is generally considered a strong relative contraindication; a patient with one AKA and one fused knee will face catastrophic difficulties with transfers, sitting in standard chairs, and navigating stairs, often rendering them entirely dependent. However, in highly selected, highly motivated patients, arthrodesis may still be chosen over bilateral AKA to preserve some degree of upright pivot transferring.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the sine qua non of a successful knee arthrodesis. The process begins with an exhaustive history and physical examination, documenting all previous surgical incisions, traumatic wounds, and the presence of prior soft tissue flaps. The integrity of the anterior skin envelope dictates the surgical approach and the potential need for preoperative plastic surgery consultation for soft tissue expansion or planned flap coverage. Comorbidities that impair bone healing—such as active smoking, poorly controlled diabetes mellitus, chronic corticosteroid use, and malnutrition—must be optimized prior to surgical intervention.
Physical examination must include a rigorous assessment of the ipsilateral hip and ankle range of motion. Any fixed equinus contracture at the ankle will severely impede ambulation with a fused knee and must be addressed concurrently, typically via a percutaneous Achilles tendon lengthening (TAL) or a gastrocnemius-soleus recession. Vascular status is evaluated by palpating the dorsalis pedis and posterior tibialis pulses; any asymmetry or absence warrants a formal non-invasive vascular study (ABI, arterial duplex) and a vascular surgery consultation.

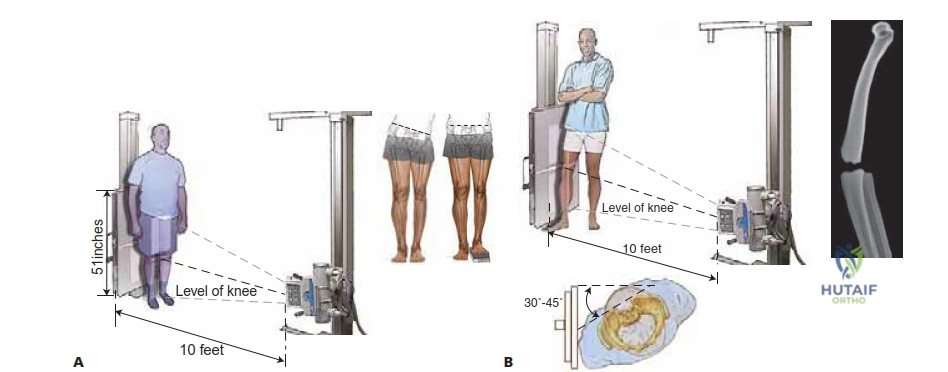
Imaging is critical for determining the method of fixation and managing the inevitable limb-length discrepancy (LLD). The gold standard imaging modality is the long-standing, anteroposterior (AP) erect lower limb radiograph, alongside a long lateral view. To obtain accurate measurements, the pelvis must be leveled using blocks under the shorter limb, preventing the patient from compensating via ankle equinus or contralateral knee flexion. These radiographs allow the surgeon to precisely calculate the anticipated bone defect once the infected or damaged bone ends are resected.
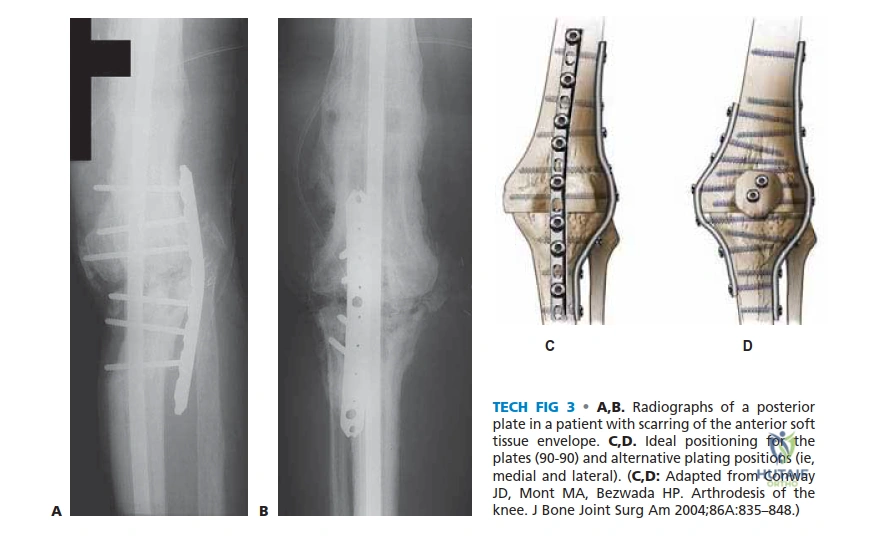
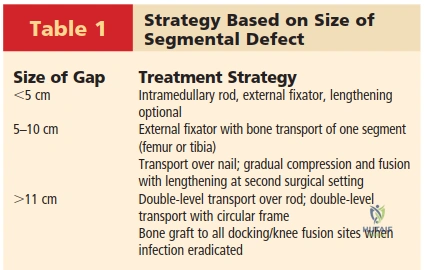
The magnitude of the bone gap directly dictates the surgical strategy. Defects less than 5 to 6 centimeters can generally be managed with acute compression using an intramedullary nail or dual plating. However, acute compression of gaps exceeding 5 to 6 centimeters carries an unacceptably high risk of kinking the popliteal vessels, leading to acute limb ischemia. For these massive defects, the surgeon must plan for gradual compression, bone transport using a circular or unilateral external fixator, or acute shortening with a planned, staged proximal femoral or tibial lengthening. Magnetic resonance imaging (MRI) or advanced nuclear imaging (e.g., WBC scans) may be utilized to delineate the extent of osteomyelitis, though surgeons must be cautious not to over-resect bone based solely on MRI edema, which can mimic active infection.
Step-by-Step Surgical Approach and Fixation Technique
Approach and Joint Preparation
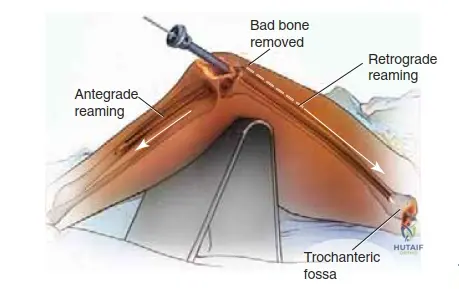
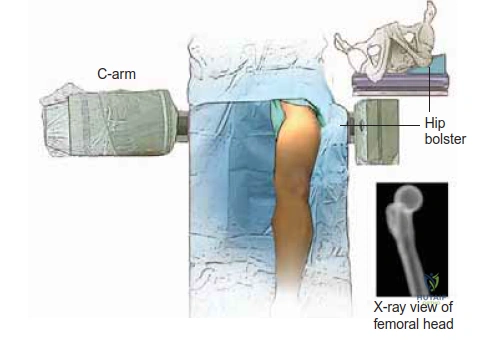
The patient is typically positioned supine on a radiolucent Jackson or flat orthopedic table to facilitate unimpeded fluoroscopic imaging from the hip to the ankle. A standard anterior midline approach is utilized, incorporating prior incisions where possible to avoid narrow skin bridges. Deep dissection involves excision of the pseudocapsule, removal of all retained hardware, and meticulous extraction of every fragment of polymethylmethacrylate (PMMA) bone cement. Retained cement within the medullary canals will obstruct intramedullary nailing and act as a nidus for recurrent infection. The bone ends are radically débrided back to bleeding, viable host bone using a combination of oscillating saws and high-speed burrs. The posterior capsule is carefully elevated off the distal femur and proximal tibia to protect the popliteal vessels during the bone resection and subsequent compression.
Intramedullary Nailing Techniques
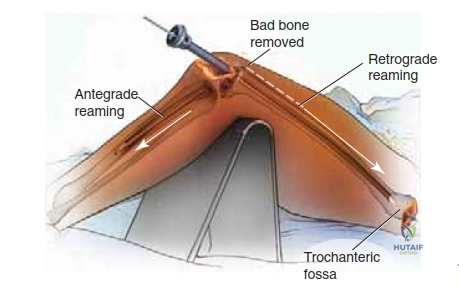
For defects amenable to acute shortening (<5-6 cm), the long intramedullary (IM) arthrodesis nail is the biomechanical gold standard. It functions as a load-sharing device, effectively neutralizing the massive bending moments across the fusion site. When utilizing a long, single-piece IM rod (such as those manufactured by Biomet, Smith & Nephew, or Stryker), the piriformis fossa serves as the critical anatomical landmark for antegrade femoral entry. Currently, trochanteric-starting intramedullary knee fusion rods are not widely available, necessitating a piriformis start to ensure linear alignment through the femoral and tibial canals.
The Stryker intramedullary rod is particularly notable as it is engineered with 5 degrees of valgus bend. This subtle valgus contour counteracts the mild varus mechanical axis that would otherwise result from inserting a perfectly straight rod from the hip to the ankle, thereby restoring a more physiologic mechanical alignment. Furthermore, this system features a proximal compression bolt end cap. Once the rod is inserted and distally interlocked, this end cap engages the proximal interlocking screw within a dynamic slot, allowing the surgeon to dial in an additional 1 centimeter of acute, rigid compression across the arthrodesis site, maximizing primary bone stability.
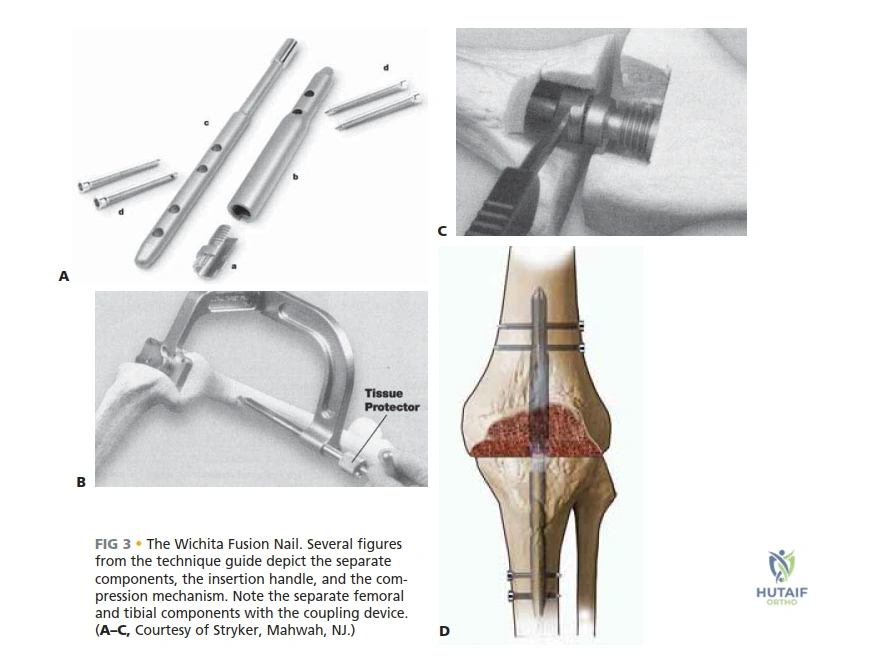
Short intramedullary fusion rods, such as the Wichita Fusion Nail (Stryker), offer an alternative when complete canal traversal is not desired. This modular device consists of two separate segments (a 14 cm femoral rod and a 16 cm tibial rod) of varying diameters, which are independently interlocked into their respective medullary canals. A central coupling device is then engaged to pull the two segments together, compressing the bone ends. However, the Wichita nail is strictly indicated for primary arthrodesis where robust, healthy metaphyseal bone is present. If the distal femur and proximal tibia are merely thin "cortical shells" devoid of cancellous bone—as is common in revision TKA—the short rods will fail to achieve adequate purchase, leading to toggling, loss of fixation, and nonunion due to the inability to neutralize the long lever arms.
External Fixation and Bone Transport
In the presence of active, virulent infection, or when dealing with massive bone defects (>6 cm) where acute shortening is unsafe, external fixation is the treatment of choice. The preferred construct is often a biplanar unilateral frame, such as the Orthofix LRS (Limb Reconstruction System), utilizing long, smooth rails (65 to 80 cm) mounted anteriorly and laterally from the proximal femur to the distal tibia. This wide span adequately neutralizes forces without leaving permanent hardware in the infected bed.

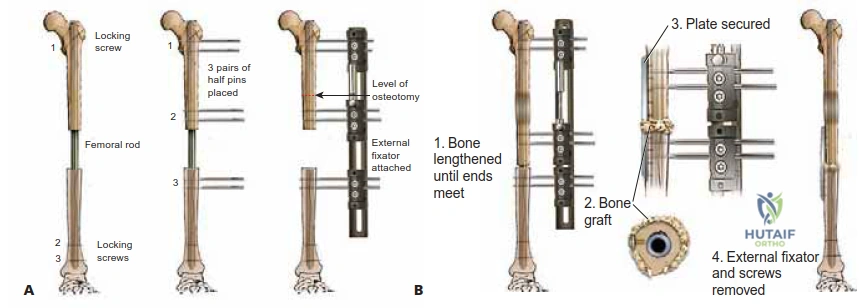
External fixation allows for immediate stabilization following the explantation of an infected TKA. Once the infection is clinically eradicated (often 6 to 8 weeks post-débridement), bone grafting can be safely performed. For large defects, the external fixator facilitates distraction osteogenesis via bone transport. A corticotomy is performed in the proximal healthy femur or distal tibia, and a bone segment is gradually transported (typically 1 mm per day) to dock at the knee defect. This elegant technique maintains the overall length of the limb—ideally leaving it 1 cm shorter than the contralateral side to assist with swing-phase clearance—while filling the massive gap with biologically active regenerate bone.
Regardless of the fixation method, autologous bone grafting is mandatory for achieving fusion after PJI, performed only when the infection is definitively cleared. The gold standard for harvesting large volumes of highly osteogenic autograft with minimal donor site morbidity is the Reamer-Irrigator-Aspirator (RIA) system (Synthes, Inc.). Through a small 2-cm incision, the RIA is introduced into the contralateral femur, harvesting copious amounts of morselized cancellous bone and marrow elements to pack into the arthrodesis site.
Complications, Incidence Rates, and Salvage Management
Knee arthrodesis is a major salvage procedure fraught with a high complication profile, commensurate with the severe pathology it aims to treat. The surgeon must be prepared to manage both early perioperative complications and late mechanical failures. The most devastating early complication is acute vascular compromise. As previously discussed, acute shortening of the limb by more than 5 to 6 centimeters can cause the popliteal artery to kink. If distal pulses are lost upon compression of the bone ends, the surgeon must immediately distract the fusion site until flow is restored, and transition to a gradual compression strategy utilizing an external fixator.

Nonunion is a frequent complication, with incidence rates reported between 10% and 15% in the literature, largely dependent on the host's biological capacity and the method of fixation. Nonunions are particularly common when short intramedullary devices are used in osteopenic bone, or when the soft tissue envelope is inadequate. Management of a nonunion typically requires revision fixation—often transitioning from an external fixator to a long intramedullary nail once infection is cleared—combined with aggressive repeat autologous bone grafting (e.g., RIA graft) and potentially the use of orthobiologics such as Bone Morphogenetic Proteins (rhBMP-2).

Recurrent infection is the nemesis of the salvage surgeon, occurring in up to 10% to 20% of cases performed for PJI. The presence of a massive intramedullary implant spanning the entire femur and tibia provides a vast surface area for biofilm formation. If a deep infection recurs after a solid fusion is achieved, chronic suppressive antibiotics may be employed. However, if the infection occurs prior to union, or is associated with systemic sepsis, the hardware must be removed. In these catastrophic scenarios, the ultimate salvage is an above-the-knee amputation.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion | 10% - 15% | Poor bone stock, inadequate compression, smoking, malnutrition. | Revision fixation (e.g., ExFix to IM Nail), RIA bone grafting, BMP. |
| Recurrent Infection | 10% - 20% | Retained cement, inadequate initial débridement, compromised soft tissues. | Hardware removal, aggressive I&D, antibiotic spacers, potential AKA. |
| Vascular Kinking | < 5% | Acute shortening > 5-6 cm tethering the popliteal vessels. | Immediate intraoperative distraction; convert to gradual ExFix compression. |
| Severe LLD (>4cm) | 30% - 50% | Massive bone resection without concomitant transport/lengthening. | Contralateral shoe lift; staged proximal femoral lengthening. |
Late complications are primarily biomechanical. The rigid lever arm of the fused knee alters gait kinematics, leading to accelerated wear of adjacent joints. Contralateral hip arthritis frequently develops secondary to the longer length of the contralateral limb, while ipsilateral hip and lumbar spine arthritis develop due to the increased rotational and bending moments transferred across the pelvis during the swing and stance phases of gait. These problems are addressed sequentially as they arise, often requiring total hip arthroplasty or spinal decompression/fusion in the years following the successful knee arthrodesis.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following knee arthrodesis is highly dependent on the chosen fixation construct and the quality of the host bone. Because the ultimate goal is rigid osseous union, early rehabilitation focuses heavily on protecting the fusion site while optimizing the function of the adjacent joints and the cardiovascular system.
For patients treated with a long, rigid intramedullary nail that achieves excellent cortical purchase, immediate protected weight-bearing is often permissible. Patients are mobilized on postoperative day one with physical therapy, utilizing a walker or bilateral crutches. Weight-bearing is typically advanced as tolerated, as the cyclical axial loading provided by ambulation actually promotes osteogenesis and compression at the fusion site through the dynamic locking mechanism of the nail. Conversely, patients treated with dual plating or external fixation may require a period of restricted weight-bearing (e.g., toe-touch only) for 6 to 8 weeks until early bridging callus is visualized on serial radiographs.

Managing the limb-length discrepancy is a critical component of the rehabilitation phase. The average shortening associated with knee arthrodesis after an infected TKA is approximately 4 centimeters. To prevent severe pelvic obliquity and subsequent secondary spinal pathology, the patient must be fitted with a custom shoe lift on the ipsilateral side. It is crucial to counsel the patient preoperatively regarding this reality; a 3-to-4-inch shoe lift can be cumbersome, but it is biomechanically essential. Ideally, the final limb length should be left approximately 1 to 1.5 centimeters shorter than the contralateral side to allow the stiff, extended leg to clear the ground during the swing phase of gait without requiring the patient to severely vault or circumduct the hip.
Long-term rehabilitation transitions toward gait training and energy conservation. Physical therapists work closely with the patient to develop a smooth, energy-efficient gait pattern. Strengthening of the
Clinical & Radiographic Imaging Archive

