Mastering Triple Arthrodesis: An Intraoperative Guide to Hindfoot Reconstruction

Key Takeaway
This masterclass guides fellows through a traditional triple arthrodesis. We delve into comprehensive hindfoot anatomy, meticulous preoperative planning, and step-by-step intraoperative execution. Learn precise joint preparation, reduction techniques, and hardware application, emphasizing neurovascular protection and optimal alignment. Critical pearls and pitfalls are highlighted, along with essential postoperative management strategies for successful fusion and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
Triple arthrodesis represents a foundational cornerstone in the armamentarium of the reconstructive foot and ankle surgeon. Historically described by Ryerson in 1923 for the stabilization of the polio-afflicted flail foot, the procedure has evolved significantly in both its indications and execution. Today, it is not merely a salvage operation for fusing joints, but a highly sophisticated biomechanical realignment strategy. The ultimate objective is the restoration of hindfoot harmony—transforming a painful, severely deformed, and dysfunctional limb into a stable, plantigrade, and mechanically sound platform for ambulation.
The patho-epidemiology of conditions necessitating a triple arthrodesis is diverse, predominantly encompassing end-stage adult acquired flatfoot deformity (AAFD), severe rigid pes cavovarus, post-traumatic osteoarthritis, and inflammatory arthropathies. In the context of AAFD, secondary to posterior tibial tendon (PTT) dysfunction, the progressive attenuation of the medial static restraints—specifically the spring ligament complex, the plantar fascia, and the deltoid ligament—leads to profound peritalar subluxation. The talus plantarflexes and rotates medially, while the calcaneus drifts into extreme valgus, ultimately resulting in a rigid, non-braceable deformity characterized by lateral impingement and medial column collapse.
Conversely, the rigid cavovarus foot, often a sequela of neuromuscular disorders such as Charcot-Marie-Tooth (CMT) disease, presents an entirely different patho-mechanical challenge. Muscle imbalances lead to a plantarflexed first ray, hindfoot varus, and forefoot pronation. Over time, the flexible deformity becomes rigid, leading to degenerative changes within the subtalar, talonavicular, and calcaneocuboid joints. Post-traumatic arthritis, frequently following highly comminuted calcaneus or talus fractures, disrupts the congruency of the articular surfaces, leading to rapid, debilitating joint space narrowing and osteophyte formation that strictly limits the functional capacity of the hindfoot complex.
While modern orthopedic paradigms rightfully emphasize joint-sparing procedures and selective arthrodeses (such as isolated subtalar or double arthrodesis) to preserve adjacent segment kinematics, the traditional triple arthrodesis remains the unequivocal gold standard for severe, fixed deformities. It is a powerful, definitive intervention reserved for cases where the peritalar joint complex is irreversibly damaged or deformed. The decision to proceed with a triple arthrodesis requires meticulous clinical judgment, balancing the loss of transverse tarsal and subtalar motion against the profound benefits of pain eradication and structural realignment.
Detailed Surgical Anatomy and Biomechanics
To master the triple arthrodesis, the surgeon must possess an intimate understanding of the intricate functional anatomy and coupled biomechanics of the hindfoot. The hindfoot and midfoot function not as isolated articulations, but as a complex, interdependent kinetic chain often referred to as the coxa pedis. This functional unit comprises the subtalar (talocalcaneal) joint, the talonavicular (TN) joint, and the calcaneocuboid (CC) joint. Physiologic alignment mandates a congruent talar–first metatarsal relationship in both anteroposterior (AP) and lateral weight-bearing planes, a delicate balance that is entirely dependent on the structural integrity of these three joints.
The subtalar joint is anatomically divided into the anterior, middle, and posterior facets, separated by the tarsal canal and sinus tarsi. The posterior facet is the largest and bears the majority of the axial load, while the anterior and middle facets provide essential stability and guidance during inversion and eversion. The interosseous talocalcaneal ligament and the cervical ligament reside within the sinus tarsi, acting as the primary static restraints against excessive inversion and anterior translation of the talus. During a lateral approach, these ligaments must be meticulously identified and resected to achieve adequate mobilization and exposure of the articular surfaces.
Chopart’s joint, consisting of the TN and CC articulations, serves as the critical transition point between the hindfoot and the midfoot. The TN joint is often conceptualized as the "acetabulum pedis," a highly congruent ball-and-socket joint where the convex talar head articulates with the concave proximal navicular, supported inferiorly by the robust spring ligament (plantar calcaneonavicular ligament). Biomechanically, the TN joint is the keystone of the hindfoot; extensive kinematic studies have demonstrated that fusion of the TN joint virtually eliminates motion in the subtalar and CC joints. Conversely, isolated fusion of the subtalar or CC joints leaves a small, yet clinically significant, degree of residual motion in the unfused articulations.
Biomechanically, the transverse tarsal joint (Chopart's joint) operates through a complex locking and unlocking mechanism dictated by the position of the subtalar joint. When the subtalar joint is in eversion (pronation), the axes of the TN and CC joints become parallel, unlocking the midfoot and allowing for flexibility and shock absorption during the heel-strike phase of gait. When the subtalar joint is in inversion (supination), these axes diverge, locking the midfoot and transforming the foot into a rigid lever arm for terminal stance and push-off. A triple arthrodesis intentionally obliterates this mechanism, fixing the foot in a functional, plantigrade position (typically 5 degrees of valgus) to optimize the mechanical advantage of the gastrosoleus complex and prevent lateral border overload.
Exhaustive Indications and Contraindications
The decision algorithm for performing a triple arthrodesis is nuanced, requiring the surgeon to synthesize the patient's clinical presentation, functional demands, and radiographic findings. The primary indication is a severe, rigid deformity of the hindfoot accompanied by end-stage osteoarthritis in the subtalar, talonavicular, and calcaneocuboid joints. In the setting of adult acquired flatfoot deformity (Stage III or IV), where the deformity is no longer passively correctable and degenerative changes are evident on radiographs, a triple arthrodesis provides the necessary power to correct the profound talonavicular sag and calcaneal valgus.
Similarly, in severe, rigid pes cavovarus, often seen in advanced neuromuscular diseases, the goal is to correct the varus thrust and restore a plantigrade weight-bearing surface. Post-traumatic osteoarthritis, particularly following high-energy intra-articular calcaneus fractures (Sanders Type III or IV) or talar neck fractures with subsequent avascular necrosis, frequently necessitates a triple arthrodesis to address the multi-planar collapse and diffuse pain. Inflammatory arthropathies, such as rheumatoid arthritis, historically formed a large proportion of indications; however, with the advent of disease-modifying antirheumatic drugs (DMARDs), these cases are becoming less frequent, though they still present with profound, destructive, and unstable hindfoot collapse when poorly controlled.
Contraindications must be strictly respected to avoid catastrophic complications. Absolute contraindications include active local or systemic infection, severe peripheral arterial disease compromising soft tissue healing, and a medically unstable patient unable to tolerate the surgical stress or the rigorous postoperative rehabilitation protocol. Relative contraindications include flexible deformities, where joint-sparing osteotomies and tendon transfers can achieve the desired correction while preserving native joint kinematics. Additionally, severe isolated ankle arthritis in the presence of a mobile hindfoot may be a relative contraindication, as fusing the hindfoot will drastically increase the mechanical stress on an already compromised tibiotalar joint, accelerating its degeneration.
The debate between isolated, double, and triple arthrodesis is ongoing in the orthopedic literature. While a double arthrodesis (fusing the subtalar and TN joints while sparing the CC joint) is increasingly popular to preserve lateral column length and theoretically reduce adjacent segment disease, the traditional triple arthrodesis remains unparalleled for achieving maximal deformity correction and ensuring complete eradication of hindfoot pain in the setting of diffuse, tri-joint degenerative disease.
| Category | Indications | Contraindications |
|---|---|---|
| Primary/Deformity | Rigid, end-stage Adult Acquired Flatfoot (Stage III/IV); Rigid pes cavovarus; Severe multi-planar hindfoot malalignment. | Flexible deformities amenable to joint-sparing procedures (osteotomies, tendon transfers). |
| Degenerative/Trauma | Post-traumatic osteoarthritis (calcaneus/talus fractures); Primary generalized hindfoot osteoarthritis. | Isolated single-joint arthritis (consider isolated subtalar or talonavicular fusion instead). |
| Systemic/Neuromuscular | Inflammatory arthropathy (Rheumatoid Arthritis) with multi-joint destruction; Charcot-Marie-Tooth disease; End-stage Charcot neuroarthropathy (salvage). | Active local or systemic infection (Absolute); Severe peripheral vascular disease (Absolute). |
| Soft Tissue/Other | Chronic, irreparable rupture of the spring ligament complex with secondary rigid arthritis. | Uncontrolled medical comorbidities; Inability to comply with strict non-weight-bearing protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the absolute cornerstone of a successful triple arthrodesis. The process begins with a meticulous clinical evaluation. The patient must be observed during standing and ambulation; the deformity may not be fully apparent when the patient is non-weight-bearing. Gait analysis helps identify a varus or valgus thrust, antalgia, and the presence of a limp. The single-limb heel rise test is critical; an inability to perform this test in a patient with pes planovalgus indicates profound PTT dysfunction and likely a rigid deformity.
Furthermore, a comprehensive seated examination is required to assess the range of motion (ROM) of the ankle, hindfoot, and forefoot. Inversion and eversion are almost always severely restricted or painful in patients requiring this procedure. Crucially, the surgeon must evaluate the ankle for an equinus contracture using the Silfverskiöld test. The hindfoot can compensate for some ankle stiffness, but a rigid equinus contracture is a significant pathological finding. Many hindfoot deformities develop secondary Achilles tendon contractures, which must be addressed concurrently, often requiring an Achilles tendon lengthening (ATL) or a gastrocnemius recession to allow the foot to reach a plantigrade position without placing excessive tension on the midfoot fusions.


Imaging is the diagnostic compass for surgical mapping. We routinely obtain weight-bearing AP, lateral, and oblique views of the foot, alongside weight-bearing views of the ankle. These views are indispensable for assessing the severity of the deformity, measuring Meary's angle, Kite's angle, and the talonavicular coverage angle. It is crucial to identify any pre-existing talar tilt or ankle malalignment; a proximal deformity can severely compromise proper hindfoot realignment if not accounted for. While plain radiographs are usually sufficient, advanced imaging such as Computed Tomography (CT) is highly recommended for assessing bone stock, identifying avascular necrosis (AVN) of the talus, and fully appreciating the three-dimensional complexity of post-traumatic deformities.


For the traditional triple arthrodesis, patient positioning is critical to ensure simultaneous, unhindered access to both the medial and lateral aspects of the hindfoot. We utilize a modified lateral decubitus position, colloquially referred to as the "sloppy lateral position." The patient's torso is securely supported within a vacuum beanbag, and an axillary roll is placed in the contralateral axilla to protect the brachial plexus. The contralateral leg is well-padded and slightly flexed. The operative leg is positioned superiorly, allowing the hip to internally and externally rotate freely, granting the surgeon dynamic access to the medial and lateral incisions. A thigh tourniquet is applied to provide a bloodless surgical field, and the C-arm fluoroscopy unit is positioned to allow seamless AP, lateral, and axial imaging without requiring repositioning of the patient.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a triple arthrodesis requires meticulous soft tissue handling, precise joint preparation, and rigid internal fixation. We universally employ a dual-incision technique: a lateral approach to access the subtalar and calcaneocuboid joints, and a dorsomedial approach for the talonavicular joint. This dual-window strategy ensures optimal, direct visualization of all articular surfaces, which is paramount for thorough cartilage debridement and accurate deformity correction.
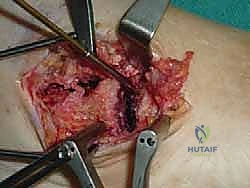
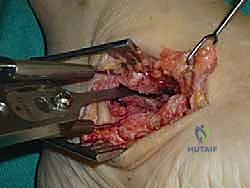
Lateral Exposure of the Subtalar and Calcaneocuboid Joints
The procedure commences with the lateral incision. A 7- to 8-cm slightly curved longitudinal incision is made, originating just distal to the tip of the lateral malleolus and extending distally toward the base of the fourth metatarsal. This trajectory perfectly aligns with the internervous plane and provides direct access to the sinus tarsi and the CC joint.


During the superficial dissection, the surgeon must be acutely vigilant of the sural nerve, which typically courses posterior to the fibula and crosses the lateral surgical field to supply the lateral border of the foot. Meticulous blunt dissection is utilized to identify, mobilize, and protect this nerve, retracting it either dorsally or plantarward. The inferior extensor retinaculum is then incised, and the extensor digitorum brevis (EDB) muscle belly is identified. The EDB is elevated sharply from its calcaneal origin and retracted distally and dorsally. This maneuver exposes the underlying joint capsules, the bifurcate ligament, and the contents of the sinus tarsi.


The crucial next step is the aggressive evacuation of the sinus tarsi. The interosseous talocalcaneal ligament, the cervical ligament, and the fibrofatty tissue (Hoke's tonsil) are completely excised. This allows for the insertion of a lamina spreader into the subtalar joint, distracting the posterior facet for visualization. The calcaneocuboid joint capsule is identically released. Joint preparation is then systematically performed. Using sharp curettes, osteotomes, and occasionally a high-speed burr, all articular cartilage is meticulously denuded down to bleeding subchondral bone. It is imperative to preserve the subchondral bone architecture to prevent structural collapse and loss of height, particularly in the posterior facet of the subtalar joint. We routinely employ subchondral drilling or "feathering" with a fine osteotome to maximize the surface area of bleeding bone, optimizing the biological environment for arthrodesis.



Medial Exposure of the Talonavicular Joint
Once the lateral joints are prepared, attention is immediately directed to the medial side. A 5- to 6-cm longitudinal incision is made centered over the talonavicular joint, typically starting just distal to the medial malleolus and extending to the medial cuneiform. The saphenous vein and nerve are carefully identified in the subcutaneous tissues and retracted dorsally. The deep fascia is incised, and the posterior tibial tendon is identified and retracted plantarward.



A longitudinal capsulotomy is performed over the TN joint. The TN joint is the most challenging of the three to prepare due to its deep, congruent ball-and-socket morphology. A lamina spreader or a Hintermann retractor is invaluable here. The articular cartilage of the talar head and the proximal navicular is meticulously removed using curved curettes. A critical technical pearl is to strictly maintain the hemispherical contour of the talar head and the corresponding concavity of the navicular. Overzealous resection with flat saw cuts will inevitably lead to shortening of the medial column, which biomechanically translates to a severe, iatrogenic flatfoot deformity. The subchondral plate is preserved and aggressively fenestrated to promote robust osteogenesis.



Deformity Correction and Sequential Fixation
The sequence of reduction and fixation is dictated by the primary deformity. In a severe pes planovalgus (flatfoot) deformity, the talonavicular joint is typically reduced and provisionally pinned first to restore the medial longitudinal arch and correct the talar plantarflexion. Conversely, in a rigid cavovarus deformity, the subtalar joint is often reduced first to correct the profound varus thrust, followed by the midtarsal joints. Reduction maneuvers require a combination of manual traction, translation, and rotational correction, frequently utilizing strong threaded Steinmann pins as "joysticks" in the talus and calcaneus.


Once provisional alignment is achieved and confirmed via multi-planar fluoroscopy, definitive fixation is applied. For the subtalar joint, we standardly utilize one or two large-diameter (6.5 mm or 7.3 mm) partially threaded cannulated screws. The primary screw is directed from the non-weight-bearing portion of the posterior calcaneal tuberosity, traversing the posterior facet, and terminating deeply within the dense bone of the talar body or neck. A second, parallel or divergent screw may be added to enhance rotational stability.



Fixation of the talonavicular joint is typically achieved with two or three smaller diameter (4.0 mm or 4.5 mm) cannulated screws. These are introduced from the medial aspect of the navicular, directed proximally and laterally into the talar head and neck. It is crucial to ensure these screws are countersunk to prevent medial soft tissue irritation. Finally, the calcaneocuboid joint is secured. This can be accomplished with a single 4.5 mm cannulated screw directed from the anterior calcaneus into the cuboid, or alternatively, utilizing a low-profile compression staple or a specialized locking plate, particularly if bone stock is compromised.



Any structural voids remaining after reduction are meticulously packed with
Clinical & Radiographic Imaging Archive