Arthroscopic Ankle Arthrodesis: An Intraoperative Masterclass on Tibiotalar Fusion

Key Takeaway
Welcome to the operating theater, fellows. Today, we're performing an arthroscopic ankle arthrodesis, a precise technique for end-stage ankle arthritis. We'll meticulously prepare the tibiotalar joint, ensure optimal alignment and vascularity, and achieve stable fixation with cannulated screws. This masterclass emphasizes comprehensive anatomy, meticulous technique, and critical intraoperative decision-making to secure excellent patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Arthroscopic Ankle Arthrodesis (AAA) represents a monumental paradigm shift in the surgical management of end-stage tibiotalar arthritis. Historically, open ankle arthrodesis was the gold standard, often requiring extensive surgical exposures, transmalleolar osteotomies, or massive anterior arthrotomies. While these open techniques reliably achieved fusion, they were fraught with significant soft tissue morbidity, high rates of wound complications, delayed union, and profound postoperative pain. The advent and subsequent refinement of arthroscopic techniques have revolutionized this procedure, offering a minimally invasive alternative that preserves the critical soft tissue envelope, minimizes disruption of the periosteal blood supply, and accelerates functional recovery. Today, arthroscopic arthrodesis is widely considered the procedure of choice for patients with end-stage ankle arthritis presenting with minimal to moderate deformity, yielding fusion rates that consistently match or exceed those of traditional open approaches.

The epidemiology of ankle arthritis diverges significantly from that of the hip and knee. While primary osteoarthritis dominates the pathogenesis of large joint degeneration in the lower extremity, the ankle joint is uniquely resilient to primary degenerative changes, largely due to its highly congruent articular geometry and the superior tensile properties of its articular cartilage. Consequently, over 70% of end-stage ankle arthritis cases are post-traumatic in etiology. These patients typically present with a history of severe rotational ankle fractures, recurrent ligamentous instability, or massive osteochondral lesions of the talus. The resultant biomechanical derangement leads to asymmetric loading, progressive cartilage attrition, and the development of dense, sclerotic subchondral bone with hypertrophic osteophyte formation. Other significant etiologies include systemic inflammatory arthropathies, such as rheumatoid arthritis, and primary degenerative osteoarthritis, though the latter remains relatively rare.
Understanding the pathophysiologic cascade is essential for effective surgical intervention. As the articular cartilage completely erodes, the joint space collapses, leading to bone-on-bone articulation. This mechanical grinding induces profound subchondral sclerosis, which acts as a barrier to vascular ingrowth and subsequent osteogenesis. Furthermore, the formation of massive anterior and posterior osteophytes—often referred to as "kissing lesions"—severely restricts the sagittal plane range of motion, leading to anterior impingement and exacerbating the patient's antalgic gait. The primary goal of arthroscopic arthrodesis is to meticulously debride this sclerotic bone, remove all residual cartilage and fibrotic tissue, and restore a bleeding, vascularized bony bed capable of robust osteogenesis, all while rigidly stabilizing the joint in an optimal biomechanical position.
The typical patient presenting for this procedure is profoundly debilitated. They describe a deep, relentless, aching pain localized to the anterior joint line, which is invariably exacerbated by weight-bearing and ambulation. Clinical examination typically reveals a globally restricted range of motion, with palpable crepitus and significant pain elicited at the extremes of dorsiflexion and plantarflexion. It is absolutely critical during the initial evaluation to differentiate true tibiotalar pathology from adjacent joint degeneration, particularly in the subtalar and transverse tarsal joints. A selective intra-articular injection of local anesthetic under fluoroscopic or ultrasound guidance can serve as an invaluable diagnostic adjunct, confirming that the tibiotalar joint is indeed the primary pain generator before committing to a definitive fusion.
Detailed Surgical Anatomy and Biomechanics
Neurovascular Structures at Risk
A profound, three-dimensional understanding of the ankle's neurovascular anatomy is the bedrock of safe and effective arthroscopic surgery. The ankle joint is enveloped by a complex network of critical structures that are highly vulnerable during portal creation and instrument manipulation. Anteriorly, the neurovascular bundle, comprising the deep peroneal nerve and the anterior tibial artery, represents the most formidable hazard. This bundle typically courses between the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL) tendons at the level of the joint line. Inadvertent injury to the deep peroneal nerve can result in devastating motor deficits, including foot drop, and debilitating neuropathic pain in the first web space. Consequently, the anterocentral portal, historically utilized in early arthroscopic techniques, has been largely abandoned due to its unacceptably high risk of penetrating this critical neurovascular interval.
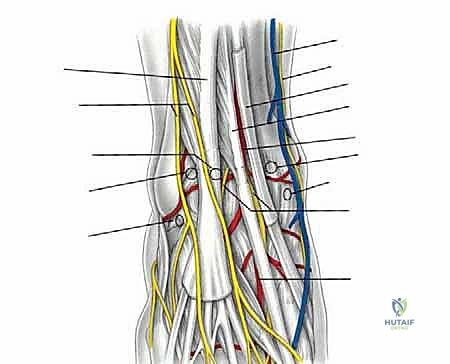
The superficial peroneal nerve (SPN) is another structure at significant risk, particularly during the establishment of the anterolateral portal. The SPN typically pierces the deep fascia of the lateral compartment approximately 10 to 12 centimeters proximal to the tip of the lateral malleolus, subsequently dividing into the medial and intermediate dorsal cutaneous nerves. However, the branching pattern and precise anatomic course of the SPN are notoriously variable. To mitigate the risk of iatrogenic injury, the surgeon must meticulously transilluminate the skin using the arthroscope prior to making the anterolateral incision, and employ a strict "nick and spread" technique, utilizing a hemostat to bluntly dissect down to the joint capsule.

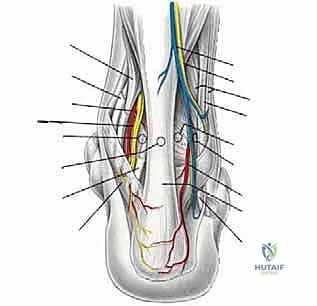
Medially, the great saphenous vein and the accompanying saphenous nerve dictate the placement of the anteromedial portal. This portal is typically established just medial to the tibialis anterior tendon. The surgeon must remain cognizant of the saphenous nerve, which provides sensory innervation to the medial aspect of the leg and hindfoot. Posteriorly, if accessory portals are required, the anatomy becomes equally unforgiving. The posteromedial portal places the tibial nerve and posterior tibial artery at risk, while the posterolateral portal is situated in close proximity to the sural nerve and the small saphenous vein. The flexor hallucis longus (FHL) tendon serves as a critical anatomic landmark during posterior arthroscopy; all instrumentation must remain lateral to the FHL to avoid catastrophic injury to the posteromedial neurovascular bundle.

Osseous and Ligamentous Architecture
The tibiotalar joint is a highly constrained, modified hinge joint, engineered to withstand immense axial loads while facilitating sagittal plane motion. The distal tibia forms a rectangular mortise, bounded by the medial malleolus and the syndesmotic articulation with the lateral malleolus (distal fibula). The talar dome is trapezoidal, being significantly wider anteriorly than posteriorly. This geometric configuration inherently imparts dynamic stability to the ankle joint; during dorsiflexion, the wider anterior portion of the talus wedges into the mortise, tensioning the syndesmotic ligaments and maximizing osseous constraint. Conversely, in plantarflexion, the narrower posterior talus occupies the mortise, relying more heavily on the collateral ligaments for stability.
In the context of end-stage arthritis, this complex osseous architecture is often severely distorted. The formation of massive anterior tibial and talar osteophytes physically blocks dorsiflexion, while posterior osteophytes limit plantarflexion. Furthermore, asymmetric wear of the articular cartilage, particularly in post-traumatic scenarios, frequently leads to coronal plane malalignment, most commonly a varus deformity. When performing an arthroscopic arthrodesis, the surgeon must not only navigate this distorted anatomy but also actively resect these osteophytes to restore the normal anatomic contours of the joint space. This resection is critical not only for adequate visualization and access to the posterior joint but also to permit the reduction of any pre-existing deformity prior to final fixation.
The ligamentous structures of the ankle, while less directly targeted during an arthrodesis, play a crucial role in the joint's residual stability and the surgeon's ability to distract the joint. The robust medial deltoid ligament complex and the lateral collateral ligaments (anterior talofibular, calcaneofibular, and posterior talofibular ligaments) often become contracted in the setting of chronic arthritis. While the application of longitudinal traction is essential for arthroscopic visualization, excessive force can lead to ligamentous rupture or iatrogenic neurapraxia. Therefore, the surgeon must skillfully balance the need for joint distraction with the inherent tension of the contracted soft tissue envelope, often requiring a sequential release of the anterior and posterior capsules to achieve adequate working space.
Exhaustive Indications and Contraindications
The decision to proceed with an arthroscopic ankle arthrodesis requires a meticulous evaluation of the patient's clinical presentation, radiographic parameters, and overall physiological status. While the indications for the arthroscopic approach have expanded significantly over the past two decades, it is not a panacea for all cases of end-stage ankle arthritis. Patient selection is the ultimate determinant of surgical success.
The primary indication for arthroscopic ankle arthrodesis is debilitating, end-stage tibiotalar arthritis that has proven refractory to comprehensive non-operative management. This includes a documented failure of activity modification, specialized orthoses (such as rigid ankle-foot orthoses or rocker-bottom shoes), aggressive physical therapy, systemic non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid or biologic injections. The ideal candidate possesses minimal to moderate coronal plane deformity (generally defined as less than 15 degrees of varus or valgus malalignment) and minimal sagittal plane subluxation. In these patients, the arthroscopic technique offers unparalleled advantages in terms of reduced morbidity and accelerated healing.
However, several distinct clinical scenarios render the arthroscopic approach either relatively or absolutely contraindicated. Massive coronal plane deformities exceeding 15 degrees are notoriously difficult to correct via purely arthroscopic means, as the contracted soft tissues and distorted osseous anatomy often necessitate extensive open releases and structural bone grafting. Similarly, profound bone loss, whether secondary to avascular necrosis (AVN) of the talus, neuropathic (Charcot) arthropathy, or previous failed surgical interventions, typically requires an open approach to facilitate massive structural allografting or the utilization of custom, 3D-printed titanium augments. Active infection remains an absolute contraindication to any definitive arthrodesis procedure.
| Category | Specific Condition | Rationale |
|---|---|---|
| Absolute Indications | End-stage osteoarthritis (Post-traumatic or Primary) | Intractable pain, failed conservative therapy, minimal deformity. |
| Absolute Indications | Rheumatoid or Inflammatory Arthritis | Destruction of articular cartilage requiring stabilization. |
| Absolute Contraindications | Active joint infection (Septic Arthritis) | High risk of systemic dissemination and guaranteed nonunion. |
| Absolute Contraindications | Severe peripheral arterial disease | Inadequate vascularity precludes bone healing and soft tissue recovery. |
| Relative Contraindications | Severe coronal deformity (>15° varus/valgus) | Difficult to correct arthroscopically; often requires open soft tissue release. |
| Relative Contraindications | Significant bone loss or Talar AVN (>50%) | Requires open structural bone grafting to restore joint height and mechanics. |
| Relative Contraindications | Active Charcot Neuroarthropathy | High risk of hardware failure and nonunion due to profound osteolysis. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Advanced Imaging
Surgical success in arthroscopic ankle arthrodesis is predicated upon exhaustive preoperative planning. The clinical assessment must begin with a rigorous evaluation of the patient's gait, overall lower extremity alignment, and neurovascular status. The presence of palpable pedal pulses is mandatory; any clinical suspicion of vascular compromise necessitates a formal vascular surgery consultation and potentially arterial Doppler studies or angiography. Furthermore, the surgeon must carefully assess the mobility and health of the adjacent subtalar and transverse tarsal joints, as an ankle fusion will inevitably increase the biomechanical demands placed upon these articulations.
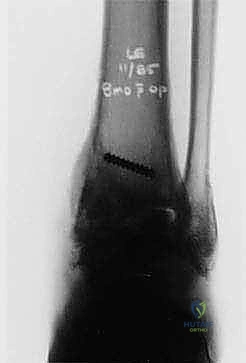
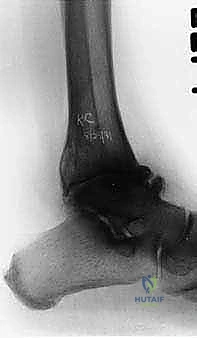
Radiographic evaluation is the cornerstone of preoperative templating. High-quality, weight-bearing anteroposterior (AP), lateral, and mortise views of the ankle are absolutely essential. These radiographs allow the surgeon to precisely quantify the degree of joint space narrowing, the location and magnitude of osteophyte formation, and the exact degree of coronal and sagittal plane malalignment.

In cases where the standard radiographs reveal complex morphologic distortions, significant subchondral cyst formation, or suspected avascular necrosis, advanced imaging becomes mandatory. A non-contrast Computed Tomography (CT) scan with 3D reconstructions provides unparalleled detail of the osseous architecture, allowing the surgeon to map the exact location of subchondral cysts and plan the precise trajectory of the fixation screws. Magnetic Resonance Imaging (MRI) is highly sensitive for detecting early avascular necrosis of the talus, a condition that significantly alters the biological healing potential of the arthrodesis and may necessitate an open approach with vascularized bone grafting.

Patient Optimization and Operating Room Setup
Patient optimization is a critical, non-negotiable phase of the preoperative process. The biological demands of achieving a solid tibiotalar fusion are immense, and any systemic factors that impede osteogenesis must be aggressively mitigated. Smoking cessation is absolutely paramount; nicotine induces profound microvascular vasoconstriction and inhibits osteoblast proliferation. Patients must strictly abstain from all nicotine products for a minimum of three months prior to surgery and three months postoperatively to mitigate the profound risk of nonunion and wound breakdown. Glycemic control in diabetic patients must also be strictly managed, aiming for an HbA1c below 7.0%.
In the operating theater, the patient is typically positioned supine on a standard radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, upward-facing position, which facilitates orthogonal fluoroscopic imaging. A well-padded thigh tourniquet is applied to provide a bloodless surgical field, which is critical for arthroscopic visualization.
Joint distraction is a mandatory component of the setup. While invasive skeletal pin distraction was historically utilized, modern techniques heavily favor non-invasive strap distraction systems. A sterile distraction strap is looped around the hindfoot and attached to a tensioning device at the foot of the bed. This allows the surgeon to apply controlled, longitudinal traction, opening the tibiotalar joint space by 3 to 5 millimeters, which is sufficient for the introduction of standard 4.0mm arthroscopic instrumentation.
Step-by-Step Surgical Approach and Fixation Technique
Portal Placement and Initial Inspection
The procedure commences with the precise establishment of the standard anterior arthroscopic portals. The anteromedial portal is created first, positioned just medial to the tibialis anterior tendon at the level of the joint line. After incising the skin, a hemostat is used to bluntly dissect into the joint capsule, protecting the saphenous nerve. A 4.0mm, 30-degree arthroscope is introduced, and the joint is insufflated with normal saline. Under direct visualization, an 18-gauge spinal needle is utilized to localize the optimal trajectory for the anterolateral portal, ensuring it is placed lateral to the peroneus tertius tendon while avoiding the superficial peroneal nerve.


Upon entering the joint, the surgeon is typically confronted with a dense, fibrotic synovitis and massive anterior osteophytes. An aggressive anterior synovectomy is performed using a mechanized shaver to establish an adequate working space. The anterior tibial and talar osteophytes are then systematically resected using an arthroscopic burr or an osteotome. This resection is not merely for visualization; it is a critical step to unlock the joint, allowing for subsequent deformity correction and facilitating access to the posterior recesses of the tibiotalar articulation.

Meticulous Joint Preparation and Debridement
The hallmark of a successful arthroscopic arthrodesis is the meticulous and exhaustive debridement of the articular surfaces. The goal is to remove all residual hyaline cartilage and penetrate the sclerotic subchondral bone down to a bleeding, vascularized cancellous bed. This is achieved through a systematic, stepwise approach, typically progressing from anterior to posterior. Ring curettes and specialized arthroscopic elevators are utilized to peel the remaining cartilage off the subchondral bone in large sheets.

Attention must be explicitly directed to the medial and lateral gutters. The articular cartilage on the medial aspect of the lateral malleolus and the lateral aspect of the medial malleolus must be thoroughly denuded. Failure to clear the gutters is a common pitfall that prevents adequate compression of the central talar dome into the tibial plafond, leading to a high risk of nonunion.


Once the cartilage is removed, the subchondral bone is addressed. A high-speed arthroscopic burr or microfracture awls are employed to fenestrate the dense, sclerotic bone. The surgeon creates multiple, closely spaced perforations—often referred to as a "fish-scaling" technique—until fat droplets and marrow elements are observed extruding into the arthroscopic fluid. This confirms adequate penetration into the vascularized cancellous bone, creating the optimal biological milieu for osteogenesis.


Deformity Reduction and Provisional Fixation
Following comprehensive joint preparation, the distraction apparatus is completely removed. The surgeon must now manually reduce the joint into the optimal biomechanical position for fusion. The universally accepted target alignment is neutral dorsiflexion (0 degrees), 0 to 5 degrees of valgus, and 5 to 10 degrees of external rotation (matching the contralateral limb). Achieving neutral dorsiflexion is paramount; even a few degrees of plantarflexion will result in a debilitating vaulting gait and severe forefoot overload.
Once the optimal position is achieved, the joint is provisionally stabilized using multiple heavy Kirschner wires (K-wires). These wires are typically driven from the medial and lateral aspects of the distal tibia, across the joint line, and into the body of the talus. The reduction and K-wire placement are rigorously verified using multi-planar fluoroscopy. The surgeon must confirm that the talus is appropriately
Clinical & Radiographic Imaging Archive