Tibiotalocalcaneal Arthrodesis with Medullary Nailing: An Intraoperative Masterclass

Key Takeaway
This masterclass provides an immersive, step-by-step guide to tibiotalocalcaneal arthrodesis using a medullary nail. We cover comprehensive surgical anatomy, meticulous preoperative planning, precise intraoperative techniques, and critical pearls for success. Learn to manage complex hindfoot deformities, from patient positioning and incision to joint preparation, guidewire placement, nail insertion, and postoperative rehabilitation, all from the operating surgeon's perspective.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a rigorous examination of a challenging yet profoundly rewarding reconstructive procedure: Tibiotalocalcaneal (TTC) Arthrodesis utilizing a Medullary Nail. This is a critical, end-stage salvage operation reserved for patients suffering from severe, debilitating ankle and hindfoot pathology. The overarching objective is to restore a pain-free, biomechanically stable, and functionally aligned lower extremity, thereby salvaging the limb and restoring the patient's ambulatory capacity. When we utilize the term "medullary," we refer to the placement of the implant within the inner marrow cavity of a long bone; the commonly used term "intramedullary" is, from an etymological and academic standpoint, redundant.
The primary goal of this operation is to create a rigid, stable, and pain-free ankle and hindfoot, fused in an optimal functional position. Biomechanically, this necessitates achieving a plantigrade foot posture—where the plantar aspect of the foot rests at a precise 90-degree angle to the longitudinal axis of the tibia. Furthermore, we must meticulously dial in approximately 5 to 7 degrees of hindfoot valgus. It is imperative that the second ray of the foot is perfectly congruent with the anteromedial crest of the tibia in the coronal plane. This precise alignment is not merely an aesthetic goal; it is an absolute biomechanical requirement for normal gait mechanics, ensuring equitable pressure distribution under the heel and the first and fifth metatarsal heads during the stance phase of the gait cycle. Failure to achieve this alignment inevitably leads to adjacent joint arthritis, lateral column overload, or recurrent ulceration.

In highly complex reconstructive scenarios involving posttraumatic, neuropathic, or avascular talar body bone loss, a direct tibiocalcaneal arthrodesis (excluding the talus entirely) may be indicated. The broader, more encompassing term, pan-talar arthrodesis, refers to the fusion of all osteological structures articulating with the talus: the distal tibia, calcaneus, navicular, and cuboid. This essentially combines an ankle fusion with a triple arthrodesis, a formidable undertaking reserved for the most catastrophic pan-articular destruction.

Etiology and Disease Progression
The patient presenting for a TTC arthrodesis typically possesses a highly complex orthopaedic history that has severely compromised their gait, weight-bearing capacity, and overall quality of life. The chief complaint is almost universally severe, chronic, unrelenting pain in the ankle and hindfoot that has proven completely refractory to exhaustive conservative management. The etiologies driving this pathology are diverse but share a common endpoint of joint destruction. Posttraumatic arthritis remains one of the most frequent indications. These patients often present with a severely compromised soft tissue envelope, retained hardware from previous open reduction and internal fixation (ORIF) attempts, profound deformity, and significant medullary canal sclerosis that will challenge our reaming protocols.
Neuropathic arthropathy, commonly referred to as Charcot neuroarthropathy, represents another major demographic for this procedure. Patients suffering from long-standing diabetes mellitus, spinal cord injuries, or hereditary neuropathies frequently present with devastating midfoot and hindfoot collapse. They exhibit profound intrinsic muscle loss, recurrent plantar ulcerations, and a chaotic radiographic picture of multiple fractures in varying, often arrested, stages of healing. In these neuropathic patients, the goal shifts from purely pain relief to creating a stable, braceable, and ulcer-free plantigrade limb, thereby averting major lower extremity amputation.

Avascular necrosis (AVN) of the talus, inflammatory arthritides (such as advanced rheumatoid arthritis), and failed previous surgical interventions (including nonunions of prior arthrodesis attempts or catastrophic failures of total ankle arthroplasty) round out the primary indications. In cases of failed total ankle replacement, the surgeon is often confronted with massive contained or uncontained bone defects that require structural allografting in conjunction with rigid medullary nail fixation to span the defect and achieve ultimate consolidation.

The Biomechanical Rationale for Medullary Nailing
The evolution of TTC arthrodesis has seen a paradigm shift toward medullary nailing, largely driven by superior biomechanical principles. Historically, crossed lag screws or anterior/lateral plating constructs were utilized. However, these constructs act as load-bearing devices, which are prone to fatigue failure, particularly in the osteopenic bone frequently encountered in our rheumatoid and Charcot populations. A medullary nail, conversely, acts as a load-sharing device. By occupying the central mechanical axis of the tibia, talus, and calcaneus, the nail neutralizes bending moments far more effectively than eccentric plating.
Furthermore, modern medullary nails offer internal compression mechanisms. The ability to generate active, sustained compression across both the tibiotalar and talocalcaneal interfaces simultaneously is a massive advantage. According to Perren’s strain theory, absolute stability and compression are requisite for primary bone healing. The rigid intramedullary construct minimizes interfragmentary strain, facilitating direct osteonal crossing.
Finally, the percutaneous or mini-open nature of nail insertion minimizes further insult to an already precarious soft tissue envelope. While the joint preparation requires open exposure, the fixation itself does not necessitate the extensive periosteal stripping required for bulky locking plates. This preservation of the extraosseous blood supply is paramount in achieving union in high-risk, dysvascular, or diabetic patients.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, an exhaustive, three-dimensional understanding of the regional anatomy is absolutely paramount. The ankle and hindfoot represent a highly congested, complex anatomic zone, rich with vital neurovascular structures, intricate muscular intervals, and critical osteological landmarks that dictate our surgical approach and hardware placement.
Osteology and Joint Relationships
The distal tibia forms the superior and medial aspects of the ankle joint mortise, contributing the tibial plafond and the medial malleolus. Its medullary canal is the ultimate destination for the proximal segment of our nail. The surgeon must carefully evaluate the tibial bow, both in the coronal and sagittal planes, as excessive bowing may lead to anterior cortical impingement or even fracture during nail insertion. The fibula, forming the lateral malleolus, serves as the lateral wall of the ankle mortise. In the frequently utilized lateral transfibular approach, a segment of the distal fibula is resected to gain access to the tibiotalar and subtalar joints. This osteotomy must be meticulously planned to preserve the integrity of the distal tibiofibular syndesmosis proximally, which provides crucial stability to the remaining construct.
The talus is the central keystone of this reconstruction. It articulates with the tibia, fibula, calcaneus, and navicular. Uniquely, the talus is devoid of any muscular or tendinous attachments; its stability is entirely ligamentous, and its blood supply is notoriously precarious, entering primarily through the tarsal canal and sinus tarsi. This makes it highly vulnerable to avascular necrosis following trauma or extensive surgical dissection. The calcaneus, the largest tarsal bone, forms the foundation of the heel. Its tuberosity is the critical target for our plantar entry point. The trajectory of the guidewire through the calcaneus dictates the final alignment of the entire construct.

While the navicular and cuboid are not directly incorporated into a standard TTC arthrodesis, their spatial orientation is profoundly influenced by hindfoot alignment. If the hindfoot is fused in excessive varus, the transverse tarsal joint becomes locked, leading to rigid lateral column overload and subsequent midfoot arthrosis. Conversely, excessive valgus unlocks the midfoot, potentially leading to medial column collapse. Thus, the 5 to 7 degrees of valgus we aim for is the precise "sweet spot" that maintains physiological midfoot biomechanics.

Neurovascular Structures and Muscular Intervals
The surgical approaches to the ankle and hindfoot are fraught with neurovascular landmines. When utilizing a medial approach—often necessary for correcting severe valgus deformities or addressing medial soft tissue contractures—the surgeon must meticulously identify and protect the structures residing behind the medial malleolus. The mnemonic "Tom, Dick, And Very Nervous Harry" serves as a reminder of the anterior-to-posterior arrangement: Tibialis posterior tendon, flexor Digitorum longus tendon, posterior tibial Artery, posterior tibial Vein, tibial Nerve, and flexor Hallucis longus tendon. The saphenous nerve and great saphenous vein lie more anteriorly but are still vulnerable during superficial dissection.

When executing the lateral transfibular approach, our primary superficial concern is the superficial peroneal nerve. This nerve typically pierces the deep fascia in the middle third of the leg and courses subcutaneously over the anterolateral aspect of the distal fibula. Iatrogenic injury here can result in devastating neuromas and profound numbness over the dorsum of the foot. More posteriorly on the lateral side, the sural nerve and small saphenous vein must be protected during the posterior soft tissue releases.

Perhaps the most critical neurovascular consideration occurs during the establishment of the plantar entry portal for the medullary nail. The incision on the plantar aspect of the heel places the medial and lateral plantar nerves and arteries at significant risk. These structures originate from the posterior tibial neurovascular bundle and course distally beneath the abductor hallucis muscle. The calcaneal branches of the tibial nerve are also highly vulnerable here. Meticulous blunt dissection down to the plantar cortex of the calcaneus, utilizing a tissue protector sleeve for all reaming and drilling steps, is an absolute, non-negotiable requirement to prevent catastrophic plantar denervation or vascular compromise.

Exhaustive Indications and Contraindications
Patient selection is the cornerstone of success in complex hindfoot reconstruction. TTC arthrodesis is a definitive, irreversible procedure; it is the end of the line for joint preservation. Therefore, the indications must be stringent, and the contraindications must be respected to avoid disastrous outcomes such as infected nonunions or eventual amputations.
| Category | Specific Conditions |
|---|---|
| Primary Indications | End-stage posttraumatic osteoarthritis of the tibiotalar and subtalar joints. |
| Severe rheumatoid arthritis or other inflammatory arthritides causing pan-articular destruction. | |
| Charcot neuroarthropathy with severe deformity, instability, or recurrent ulceration (salvage). | |
| Avascular necrosis of the talar body with subsequent collapse and arthritis. | |
| Paralytic deformities (e.g., polio, drop foot with rigid equinovarus) requiring rigid stabilization. | |
| Failed total ankle arthroplasty (salvage procedure, often requiring structural allograft). | |
| Nonunion or malunion of prior ankle or subtalar arthrodesis attempts. | |
| Absolute Contraindications | Active, untreated local or systemic infection (osteomyelitis, septic arthritis). |
| Severe peripheral vascular disease (inadequate arterial inflow to support soft tissue healing and bone union). | |
| Medically unstable patients unable to tolerate prolonged anesthesia or the physiological stress of surgery. | |
| Lack of a viable soft tissue envelope to cover the surgical site or hardware. | |
| Relative Contraindications | Active smoking or nicotine use (significantly increases nonunion and wound complication rates). |
| Severe osteoporosis (may compromise hardware purchase, though nails are better than plates). | |
| Uncontrolled diabetes mellitus (HbA1c > 8.0% correlates with dramatically higher complication rates). | |
| Patient non-compliance or inability to adhere to strict, prolonged non-weight-bearing protocols. |
Clinical Decision Making
The decision to proceed with a TTC arthrodesis rather than an isolated ankle or subtalar fusion requires careful clinical and radiographic correlation. Diagnostic injections of local anesthetic into the subtalar or tibiotalar joints under fluoroscopic guidance can be invaluable. If a patient with severe ankle arthritis experiences complete pain relief from an isolated ankle injection, and the subtalar joint appears radiographically pristine, an isolated ankle fusion is the standard of care. We do not routinely sacrifice a healthy, asymptomatic subtalar joint.
However, if the subtalar joint is arthritic, or if there is severe deformity (such as profound valgus collapse in a flatfoot deformity) that cannot be corrected without incorporating the subtalar joint, a combined TTC arthrodesis is mandated. In cases of severe talar avascular necrosis, the talus often lacks the structural integrity to support an isolated ankle fusion, necessitating the extension of the fusion down to the calcaneus to achieve a stable base of support.
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is where the battle is won or lost. The surgeon must anticipate the deformity correction, select the appropriate hardware dimensions, and plan for any necessary adjunctive procedures, such as structural bone grafting or Achilles tendon lengthening.
Imaging Modalities and Templating
Our radiographic evaluation begins with standard, high-quality, weight-bearing anterior-posterior (AP), lateral, and mortise views of the ankle and foot. In cases of complex deformity, long-cassette alignment films (hip-to-ankle) are mandatory to assess the overall mechanical axis of the lower extremity. We must ensure that our hindfoot correction harmonizes with any existing knee or hip pathology.

Computed Tomography (CT) is indispensable. A fine-cut CT scan provides a three-dimensional understanding of bone stock, the presence of subchondral cysts, and the exact geometry of the deformity. It is particularly crucial when planning for a failed total ankle arthroplasty, allowing us to quantify the exact volume of bone loss and order the appropriate structural femoral head or distal tibial allografts. Magnetic Resonance Imaging (MRI) is utilized selectively, primarily to assess the vascular status of the talus in suspected AVN or to evaluate for occult osteomyelitis in our diabetic Charcot population.

Templating is a critical exercise. Using digital templating software on calibrated radiographs, we determine the anticipated length and diameter of the medullary nail. The nail must be long enough to bypass the isthmus of the tibia to prevent stress risers and subsequent peri-prosthetic fractures. We must also carefully evaluate the tibial bow; a very straight, long nail inserted into a tibia with a pronounced anterior bow will inevitably impinge on the anterior cortex, risking fracture or preventing complete seating of the implant.

Patient Positioning and Operating Room Setup
Patient positioning depends entirely on the chosen surgical approach and the surgeon's preference. The lateral decubitus position is highly favored when utilizing the lateral transfibular approach. It provides unencumbered access to the lateral aspect of the fibula, ankle, and subtalar joint. A beanbag is used to secure the patient, and all bony prominences are meticulously padded.
Alternatively, the patient may be positioned supine with a large bump placed beneath the ipsilateral hip to internally rotate the leg, bringing the lateral malleolus anteriorly. This position is advantageous if a medial approach is also anticipated, or if simultaneous access to the iliac crest for autogenous bone graft harvesting is required. A radiolucent triangle or a specialized foot positioner can be utilized to hold the leg.

A sterile tourniquet is applied to the proximal thigh. Fluoroscopy is absolutely essential. The C-arm should be positioned such that perfectly orthogonal AP and lateral views of the tibia, ankle, and calcaneus can be obtained swiftly and effortlessly. The surgeon must verify these views prior to prepping and draping to ensure the table or the contralateral leg does not obstruct the beam.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution demands meticulous soft tissue handling, aggressive joint preparation, precise deformity correction, and flawless hardware deployment. We will detail the procedure utilizing the standard lateral transfibular approach, which provides exceptional exposure to both the tibiotalar and subtalar joints.
Surgical Exposure and Joint Preparation
A longitudinal incision is made over the distal fibula, beginning approximately 10 to 15 centimeters proximal to the tip of the lateral malleolus and extending distally, curving slightly anteriorly toward the base of the fourth metatarsal. The dissection is carried down through the subcutaneous tissues, taking extreme care to identify and retract the superficial peroneal nerve anteriorly and the sural nerve posteriorly. The periosteum over the distal fibula is incised.

A fibular osteotomy is performed using an oscillating saw, typically 2 to 3 centimeters proximal to the level of the tibial plafond. The distal fibular segment is then meticulously excised. This involves sharp dissection of the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and the robust posterior talofibular ligament (PTFL). The excised fibula is passed to the back table, where it is morselized using a bone mill to serve as autogenous bone graft later in the procedure.

With the fibula removed, the lateral aspect of the tibiotalar and subtalar joints is widely exposed. A lamina spreader or a specialized joint distractor is inserted to open the articulations. This is the most critical phase for achieving union: the joint preparation. Using a combination of sharp osteotomes, ring curettes, and high-speed cutting burrs, every square millimeter of articular cartilage must be eradicated. We must aggressively debride down to
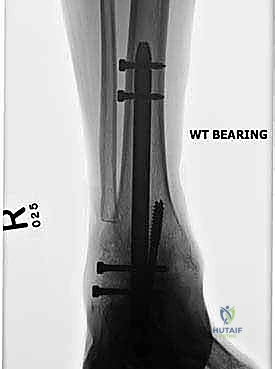
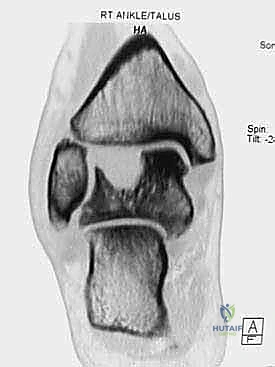
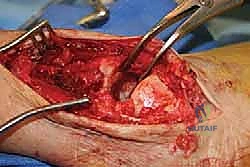
Clinical & Radiographic Imaging Archive