Mastering Anterior Cervical Arthrodesis: Operative Techniques and Evidence-Based Management
Key Takeaway
Anterior cervical discectomy and fusion (ACDF) is a highly successful procedure for managing refractory cervical disc disease, radiculopathy, and myelopathy. This comprehensive guide details the surgical anatomy, step-by-step operative techniques, and biomechanical principles of anterior arthrodesis. It emphasizes meticulous patient selection, direct neural decompression, optimal graft selection, and strategies to mitigate severe complications such as recurrent laryngeal nerve palsy, pseudarthrosis, and iatrogenic spinal cord injury.
Introduction to Anterior Cervical Arthrodesis
Anterior cervical discectomy with interbody fusion (ACDF) has gained universal acceptance among orthopaedic surgeons and neurosurgeons as the gold standard for managing refractory symptoms of cervical disc disease, cervical spondylosis, and cervical myelopathy. The extensive body of literature attests to a consistently low incidence of major complications and postoperative morbidity, coupled with a high degree of success in relieving radicular and myelopathic symptoms.
The fundamental philosophical difference in the evolution of these techniques lies in the extent of decompression. Historically, debate centered on whether surgery should be limited to simple discectomy and interbody fusion—relying on indirect decompression and spontaneous osteophyte resorption—or whether an aggressive attempt must be made to enter the spinal canal to remove osteophytes, resect the posterior longitudinal ligament (PLL), and directly decompress the spinal cord and nerve roots. Modern consensus, driven by advanced imaging and microsurgical techniques, heavily favors direct decompression, particularly in the presence of myelopathy or profound structural stenosis.
Extreme care must be exercised during anterior fusion of the cervical spine due to the significant potential for catastrophic complications, including injury to the cervical viscera, major vascular structures, and the spinal cord itself.
Patient Selection and Preoperative Planning
Clinical Evaluation and Indications
The success of anterior cervical arthrodesis is inextricably linked to meticulous patient selection. The primary indications include:
* Cervical Radiculopathy: Refractory to a minimum of 6 weeks of conservative management (physical therapy, NSAIDs, selective nerve root blocks).
* Cervical Spondylotic Myelopathy (CSM): Progressive neurological deficit, gait instability, or upper motor neuron signs (Hoffmann's sign, hyperreflexia, Babinski reflex).
* Recurrent Disc Herniation: Following previous posterior foraminotomy.
* Cervical Trauma: Fracture-dislocations requiring anterior column reconstruction and stabilization.
Clinical Pearl: The "wrong patient" is a primary cause of surgical failure. The cervical spine is a frequent target for psychogenic pain. Careful preoperative evaluation is essential to rule out hysterical personalities, chronic anxiety states, or secondary gain issues (e.g., pending litigation). If a patient has been significantly disabled for more than 1 year with purely subjective findings and no objective neurological deficits, surgery should be approached with extreme caution.
Imaging and Diagnostic Correlation
Often, the discrepancy between the degree of bony spurring or other radiographic changes and the clinical symptoms is striking. Furthermore, the level of neurological involvement does not always coincide with the site of the greatest radiographic findings.
Because plain radiographs cannot provide the necessary information for identifying the precise level(s) of neural compression, advanced imaging is mandatory.
* Magnetic Resonance Imaging (MRI): The modality of choice. It provides detailed visualization of soft disc herniations, cord signal changes (T2 hyperintensity), and neural foraminal stenosis.
* CT Myelography: Strongly recommended for patients with pacemakers, severe claustrophobia, or complex revision anatomy where metallic artifact obscures MRI interpretation.
Correlation of the patient’s symptoms with diagnostic studies is crucial. Literature demonstrates that 14% of asymptomatic patients younger than 40 years of age, and 28% of patients older than 40 years, have significant abnormalities on MRI. Surgery must treat the patient's pathology, not the MRI findings. In descending order of frequency, the disc levels most commonly involved with degenerative changes are C5-C6, C6-C7, and C4-C5.
Surgical Anatomy and The Anterior Approach
Positioning and Neuromonitoring
The patient is positioned supine on a radiolucent operating table. A small gel roll is placed horizontally between the scapulae to allow gentle extension of the cervical spine, which naturally opens the anterior disc spaces. The head is stabilized on a foam donut or Mayfield tongs depending on the required stability.
In selected instances, particularly in patients with pre-existing myelopathy or T2 spinal cord signal abnormalities, continuous monitoring of Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs) is highly recommended. This minimizes the risk of unrecognized spinal cord injury resulting from neck positioning, intraoperative hypotension, or surgical manipulation.
The Surgical Exposure
The anterior approach to the cervical spine utilizes the avascular plane between the visceral and neurovascular compartments of the neck.
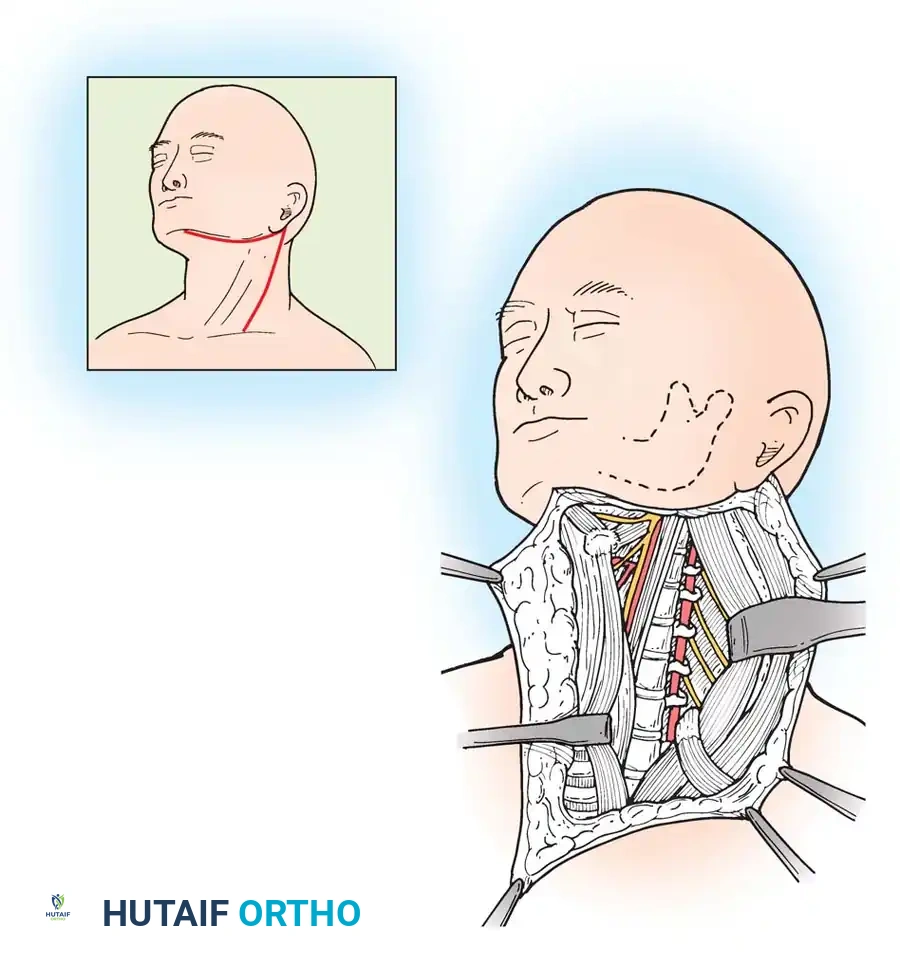
- Incision: A transverse incision is typically made within a natural skin crease for single or two-level pathology. For extensive multilevel corpectomies, a longitudinal incision along the anterior border of the sternocleidomastoid (SCM) may be required.
- Superficial Dissection: The platysma muscle is divided in line with the skin incision. The superficial cervical fascia is incised, mobilizing the SCM laterally and the strap muscles (sternohyoid, sternothyroid) medially.
- Deep Dissection: The middle cervical fascia (pretracheal fascia) is bluntly dissected. The carotid sheath (containing the carotid artery, internal jugular vein, and vagus nerve) is retracted laterally, while the trachea and esophagus are retracted medially.
- Prevertebral Fascia: The prevertebral fascia is incised longitudinally over the midline of the vertebral bodies, exposing the longus colli muscles.
Surgical Warning: Sympathetic nervous system injuries (Horner's Syndrome) are avoided by dissecting in the correct anatomical planes. Keeping the dissection medial to the carotid sheath and avoiding aggressive lateral retraction of the longus colli muscle protects the sympathetic chain.
Recurrent Laryngeal Nerve (RLN) Considerations
An approach from the left side is generally considered less likely to damage the recurrent laryngeal nerve, as its course is more predictable (looping under the aortic arch and ascending in the tracheoesophageal groove). In a right-sided approach, the RLN is in jeopardy from C6 caudally as it loops under the subclavian artery and crosses the surgical field at a more oblique angle.
Apfelbaum, Kriskovich, and Haller demonstrated in a series of 900 patients that RLN palsy is often caused by endotracheal tube compression against the laryngeal mucosa during retractor placement, rather than direct surgical transection.
* Prevention Strategy: The incidence of RLN palsy is significantly decreased by temporarily deflating and reinflating the endotracheal tube cuff after the self-retaining retractors are placed. This allows the tube to reposition itself centrally within the trachea, relieving focal pressure.
Operative Technique: Discectomy, Decompression, and Arthrodesis
Level Localization
Operating at the wrong level is a devastating, yet preventable, complication. Use of an intraoperative localization radiograph with a radiopaque marker is mandatory.
* Technique: A spinal needle is inserted into the anterior annulus. The marker needle should be directed cranially so that the tip butts against the superior endplate, avoiding penetration into the spinal canal. Placing two right-angle bends in the needle, beginning 1 cm proximal to the tip, physically prevents penetration beyond a depth of 1 cm.
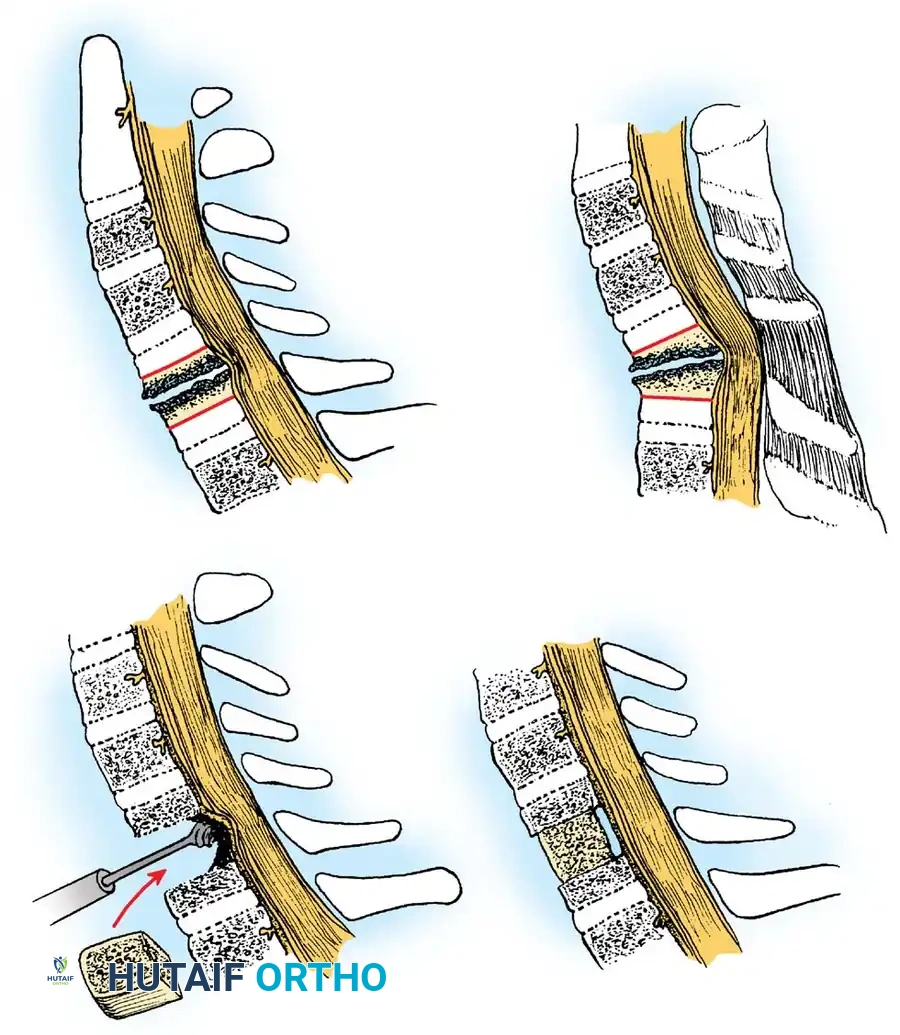
Discectomy and Direct Decompression
Once the correct level is confirmed, the anterior annulus is incised. In the hands of skilled surgeons, utilizing an operating microscope provides unparalleled illumination and magnification.
- Disc Removal: The cartilaginous endplates and nucleus pulposus are removed using pituitary rongeurs and curettes.
- Osteophyte Resection: A high-speed burr is utilized to thin the posterior osteophytes. Small, angled curettes and 1mm or 2mm Kerrison rongeurs are then used to carefully resect the remaining cortical shell away from the dura.
- PLL Resection: If the compression of neural tissue is caused by large osteophytes, extruded disc fragments, or an ossified posterior longitudinal ligament (OPLL), direct decompression by removal of the PLL is recommended. This is especially true if T2 MRI sequences show cord signal abnormality.
Historical Pitfall: Kraus and Stauffer reported severe spinal cord injuries resulting from the historical "drill and dowel" (Cloward) method. Causes included operating a drill without a protective guard (plunging into the canal) and postoperative displacement of the cylindrical dowel graft into the cord. Modern techniques utilizing high-speed burrs under microscopic visualization have largely rendered these specific complications obsolete.
Endplate Preparation and Grafting
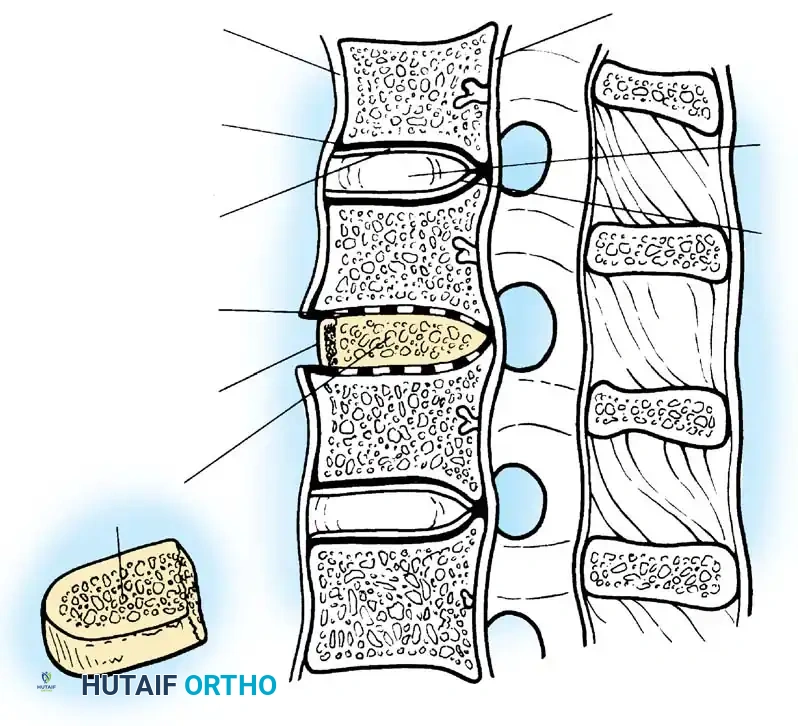
The goal of endplate preparation is to expose bleeding cancellous bone to promote osteogenesis while preserving the structural integrity of the subchondral bone to prevent graft subsidence.
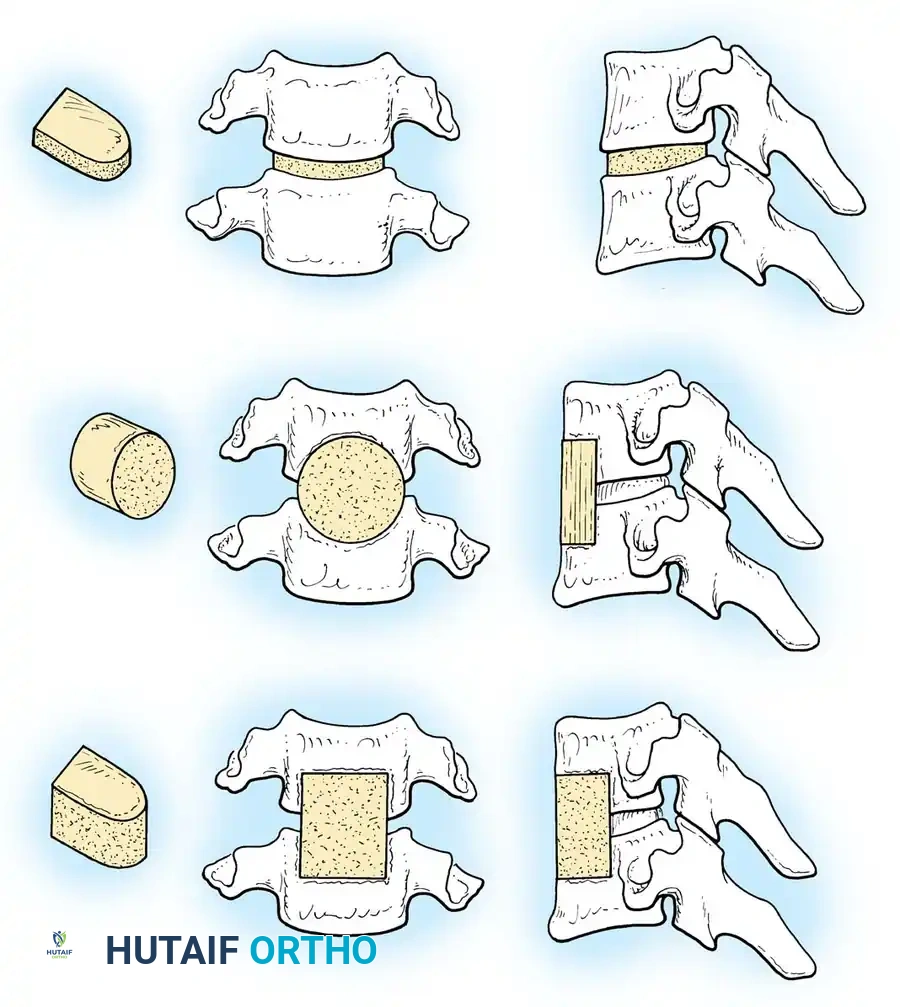
The use of a tricortical graft (Smith-Robinson technique) is highly recommended for interbody fusions. A rectangular graft provides superior biomechanical stability and resistance to subsidence compared to a circular Cloward dowel.
- Autograft vs. Allograft: Autogenous tricortical iliac crest bone graft remains the gold standard for osteoinductivity and osteoconductivity. However, due to donor site morbidity, structural allografts (machined cortical bone) or synthetic cages packed with local autograft/demineralized bone matrix (DBM) are frequently used for single-level procedures with excellent results.
- Multilevel Considerations: Allograft bone should not be used for multilevel interbody fusions without anterior plating due to an unacceptably high nonunion rate.
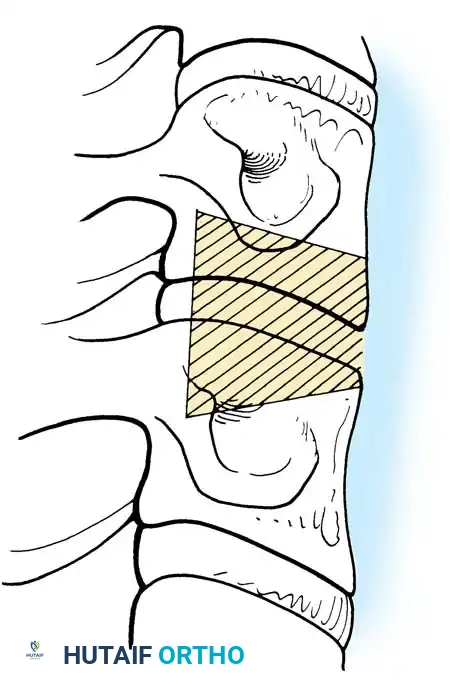
Grafts must be measured accurately, shaped to accommodate the normal cervical lordosis, and tightly fitted under compression. Gentle cervical traction is applied by the anesthesiologist, the graft is tapped into place, and traction is released, locking the graft under physiological compressive loads.
Corpectomy for Multilevel Disease
In cases of severe multilevel spondylosis or OPLL, a cervical corpectomy may be indicated to achieve adequate decompression.
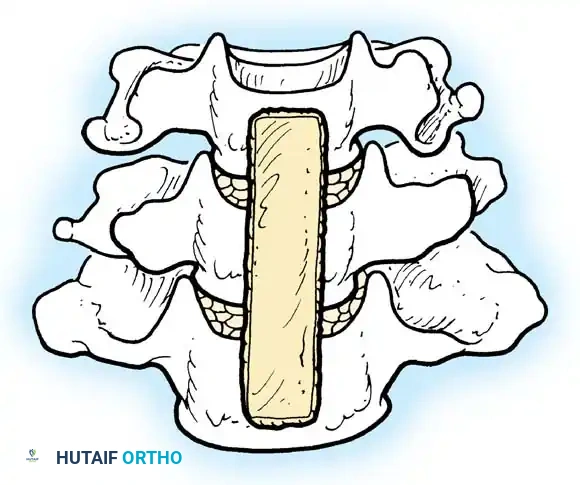
This involves the complete removal of the intervening vertebral body and adjacent discs, followed by reconstruction with a long structural strut graft (fibular allograft or titanium mesh cage) spanning from the intact superior to the intact inferior endplate.
Anterior Instrumentation
Anterior plate stabilization is now a routine adjunct. Modern locking-type plate devices minimize the risk of screws backing out, which historically led to catastrophic esophageal or tracheal perforation.
* Advantages: Plating provides immediate biomechanical stability, increases fusion rates (especially in multilevel procedures), maintains cervical lordosis, and often precludes the need for rigid postoperative external immobilization (e.g., halo-vest).
* Safety: Fixed-angle or variable-angle locking screws preclude the need for bicortical drilling, significantly decreasing the risk of iatrogenic spinal cord injury during screw placement.
Complications and Management Strategies
Macnab summarized the complications of anterior cervical fusion astutely: for every anatomical structure present in the neck, there is a possibility of a surgical error. Poor results stem not only from technical failures but from poor indications.
1. Pseudarthrosis and Graft Collapse
Nonunion of an anterior cervical fusion is relatively unusual in single-level procedures (3% to 7% nonunion rate with autograft). However, with multilevel interbody fusions, the pseudarthrosis rate increases in a nonlinear fashion.
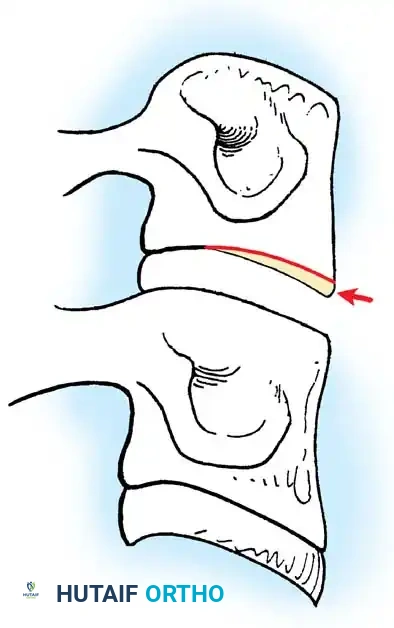
- Pathomechanics: Collapse of the graft leads to sharp angular kyphosis. Combined with nonunion, this can cause recurrent compression of the spinal cord (as seen in the provided figure).
- Risk Factors: Smoking has been definitively documented to increase the pseudarthrosis rate after spinal arthrodesis. Hilibrand et al. demonstrated that smoking has a profound negative impact on healing after multilevel anterior cervical fusion.
- Prevention: Wang et al. showed that the addition of internal fixation (plating) for two-level ACDF significantly reduced the pseudarthrosis rate. When nonunions do occur, they typically manifest at the caudal-most segment of a multilevel construct due to higher biomechanical shear forces at the cervicothoracic junction.
2. Visceral and Airway Complications
- Dysphagia: Difficulty swallowing is the most common postoperative complaint. One prospective study reported a 50% frequency of dysphagia at 1 month after surgery. Fortunately, it is usually transient; at 6 months, only 4.8% of patients experience moderate to severe dysphagia. Meticulous hemostasis, minimizing retraction time, and utilizing low-profile plates reduce this risk.
- Airway Obstruction: A rare but life-threatening complication, typically occurring 12 to 36 hours postoperatively. It is most often secondary to a retropharyngeal hematoma or massive prevertebral edema.
- Management: All anterior surgical wounds must be drained. A soft, closed-suction drainage system is routinely inserted deep into the wound anterior to the spine and maintained for 24 hours. If acute airway compromise occurs, immediate intubation or emergency bedside wound opening is required.
3. Neurological Injury
- Spinal Cord Injury: Direct trauma from instruments (burrs, curettes) or graft displacement. Instruments must be used with extreme caution. Small, angled curettes and Kerrison rongeurs must be sharp to prevent the need for excessive force, which can lead to sudden loss of control and plunging into the dura.
- Dural Tears: If a cerebrospinal fluid (CSF) leak occurs anteriorly, it is challenging to repair directly. Management includes placement of a fascial patch, fibrin glue, and potentially a lumbar subarachnoid drain to divert CSF pressure while the defect heals.
4. Graft Extrusion
Extrusion of a graft is most commonly seen in the treatment of fracture-dislocations of the neck with severe posterior ligamentous instability. It is rarely seen in fusions for degenerative disc disease where the posterior tension band remains intact.
* Management: Unless the graft extrudes more than 50% of its depth, or unless it causes mechanical dysphagia by compressing the esophagus, revision surgery is usually not indicated. The extruded portion is typically resorbed, and the graft ossifies as the arthrodesis matures.
Postoperative Protocol
- Immediate Post-Op: Patients are monitored closely for airway patency and neurological status. The closed-suction drain is typically removed on postoperative day 1 when output is minimal.
- Immobilization: With modern anterior instrumentation, a rigid cervical collar (e.g., Aspen or Miami J) is often used for comfort for 2 to 6 weeks, depending on bone quality and the number of levels fused. Halo-vest external fixation is rarely required unless severe multi-column instability exists and posterior fixation is contraindicated.
- Rehabilitation: Early ambulation is encouraged. Isometric neck strengthening and range-of-motion exercises begin after radiographic evidence of early consolidation (typically 6 to 12 weeks).
- Lifestyle Modification: Absolute smoking cessation is mandatory to mitigate the high risk of pseudarthrosis.
Conclusion
Anterior cervical discectomy and fusion remains a highly effective, biomechanically sound procedure for the treatment of cervical radiculopathy and myelopathy. Superior outcomes are achieved through rigorous patient selection, precise localization, meticulous microsurgical decompression, and rigid biomechanical reconstruction. By adhering to strict anatomical principles and utilizing modern instrumentation, the orthopaedic surgeon can consistently achieve high fusion rates while minimizing the risk of catastrophic complications.
📚 Medical References
- anterior cervical arthrodesis with interbody or strut-grafting, J Bone Joint Surg 83A:668, 2005.
- Hodgson AR, Stock FE: Anterior spine fusion for treatment of tuberculosis of the spine: the operative fi ndings and results of treatment of the fi rst 100 cases, J Bone Joint Surg 42A:295, 1960.
- Howorth MB: Evolution of spinal fusion, Ann Surg 117:278, 1943.
- Hu RW, Bohlman HH: Fracture at the iliac bone graft harvest site after fusion of the spine, Clin Orthop Relat Res 309:208, 1994.
- Hughes SS, Pringle T, Phillips MM, et al: Multilevel cervical corpectomy and fi bular strut grafting, Orthop Trans 20:432, 1996.
- Ido K, Shimizu K, Nakayama Y, et al: Anterior decompression and fusion for ossifi cation of posterior longitudinal ligament in the thoracic spine, J Spinal Disord 8:317, 1995.
- Jenis LG, Leclair W: Late vascular complication with anterior cervical discectomy and fusion, Spine 19:1291, 1994.
- Johnsson R, Stromqvist B, Aspenberg P: Randomized radiostereometric study comparing osteogenic protein-1 (OP-1) and autograft bone in human noninstrumented posterolateral lumbar fusion, Spine 27:2654, 2002.
- Jones AAM, McAfee PC, Robinson RA, et al: Failed arthrodesis of the spine for severe spondylolisthesis: salvage by interbody arthrodesis, J Bone Joint Surg 70A:25, 1988.
- Jorgenson SS, Lowe TG, France J, et al: A prospective analysis of autograft versus allograft in posterolateral lumbar fusion in the same patient: a minimum of 1-year follow-up in 144 patients, Spine 19:2048, 1994.
- Kraus DR, Stauffer ES: Spinal cord injury as a complication of elective anterior cervical fusion, Clin Orthop Relat Res 112:130, 1975.
- Kumar A, Kozak JA, Doherty BJ, et al: Interspace distraction and graft subsidence after anterior lumbar fusion with femoral strut allograft, Spine 18:2393, 1993.
- Kurz LG, Garfi n SR, Booth RE: Harvesting autogenous iliac bone grafts, Spine 14:1324, 1989.
- Lindholm TS, Ragni P, Lindholm TC: Response of bone marrow stroma to demineralized cortical bone matrix in experimental spinal fusion in rabbits, Clin Orthop Relat Res 230:296, 1988.
- Lovell TP, Dawson EG, Nilsson OS, et al: Augmentation of spinal fusion with bone morphogenetic protein in dogs, Clin Orthop Relat Res 243:266, 1989.
- Ludwig SC, Boden SD: Osteoinductive bone graft substitutes for spinal fusion, Orthop Clin North Am 30:635, 1999.
- Macnab I: The blood supply of the lumbar spine and its application to the technique of intertransverse lumbar fusion, J Bone Joint Surg 53B:628, 1971.
- Macnab I: Complications of anterior cervical fusion, Orthop Rev 1:29, 1972.
- Mahvi DM, Zdeblick TA: A prospective study of laparoscopic spinal fusion: technique and operative complications, Ann Surg 224:85, 1996.
- Mathews HH, Evans MT, Molligan HJ, et al: Laparoscopic discectomy with anterior lumbar interbody fusion: a preliminary review, Spine 20:1797, 1995.
- McAfee PC, Regan JR, Zdeblick T, et al: The incidence of complications in endoscopic anterior thoracolumbar spinal reconstructive surgery: a prospective multicenter study comprising the fi rst 100 consecutive cases, Spine 20:1624, 1995.
- McBride ED: A mortised transfacet bone block for lumbosacral fusion, J Bone Joint Surg 31A:385, 1949.
- Meril AJ: Direct current stimulation of allograft in anterior and posterior lumbar interbody fusions, Spine 19:2393, 1994.
- Minamide A, Tamaki T, Kawakami M, et al: Experimental spinal fusion using sintered bovine bone coated with type I collagen and recombinant human bone morphogenetic protein-2, Spine 24:1863, 1999.
- Mooney V, McDermott KL, Song J: Effects of smoking and maturation on long-term maintenance of lumbar spinal fusion success, J Spinal Disord 12:380, 1999.
- Morone MA, Boden SD: Experimental posterolateral lumbar spinal fusion with demineralized bone matrix gel, Spine 23:159, 1998.
- Morone MA, Boden SD, Hair G, et al: Gene expression during autograft lumbar spine fusion and the effect of bone morphogenetic protein-2, Clin Orthop Relat Res 351:252, 1998.
- Nymberg SM, Crawford AH: Video-assisted thoracoscopic releases of scoliotic anterior spines, AORN J 63:561, 1996.
- Overton LM: Arthrodesis of the lumbosacral spine, Clin Orthop 5:97, 1955.
- Prothero SR, Parkes JC, Stinchfi eld FE: Complications after lowback fusion in 1000 patients: a comparison of two series one decade apart, J Bone Joint Surg 48A:57, 1966.
- Ralston EL, Thompson WAL: The diagnosis and repair of pseudarthrosis of the spine, Surg Gynecol Obstet 89:37, 1949.
- Regan JJ, Mack MJ, Picetti GD: The technical report on videoassisted thoracoscopy in thoracic spinal surgery: preliminary description, Spine 20:831, 1995.
- Riley EH, Lane JM, Urist MR, et al: Bone morphogenetic protein-2, Clin Orthop Relat Res 324:39, 1996.
- Robinson RA: Anterior and posterior cervical spine fusions, Clin Orthop Relat Res 35:34, 1964.
- Robinson RA, Riley LH Jr: Techniques of exposure and fusion of the cervical spine, Clin Orthop Relat Res 109:78, 1975.
- Robinson RA, Smith GW: Anterolateral cervical disc removal and interbody fusion for cervical disc syndrome, Bull Johns Hopkins Hosp 96:223, 1955 (abstract). Rogers WA: Fractures and dislocations of the cervical spine: an end-result study, J Bone Joint Surg 39A:341, 1957.
- Rombold C: Treatment of spondylolisthesis by posterolateral fusion, resection of the pars interarticularis, and prompt mobilization of the patient: an end-result study of seventy-three patients, J Bone Joint Surg 48A:1282, 1966.
- Rothman RH: New developments in lumbar disk surgery, Orthop Rev 4:23, 1975.
- Rothman RH, Booth R: Failures of spinal fusion, Orthop Clin North Am 6:299, 1975.
- Sacks S: Anterior interbody fusion of the lumbar spine, J Bone Joint Surg 47B:211, 1965.
- Sacks S: Anterior interbody fusion of the lumbar spine: indications and results in 200 cases, Clin Orthop Relat Res 44:163, 1966.
- Sacks S: Present status of anterior interbody fusion in the lower lumbar spine, Orthop Clin North Am 6:275, 1975.
- Sandhu H, Grewal HS, Parvataneni H:
🔗 Read the comprehensive guide: Operative Principles of Lower Extremity Arthrodesis: Ankle and Knee
