Arthrodesis of the Wrist: Surgical Techniques & Protocols
Key Takeaway
Wrist arthrodesis is a highly effective salvage procedure for advanced radiocarpal arthritis, severe trauma, and paralytic deformities. Achieving a stable, painless wrist requires meticulous surgical technique, optimal positioning in 10 to 20 degrees of extension, and rigid internal fixation. This guide details evidence-based approaches, including AO/ASIF plating and specialized tenodesis techniques, ensuring high fusion rates and maximal postoperative grip strength for complex wrist pathologies.
Comprehensive Introduction and Patho-Epidemiology
Wrist arthrodesis, defined as the surgical fusion of the radiocarpal, midcarpal, and carpometacarpal articulations, represents the ultimate and most durable salvage procedure in the armamentarium of the upper extremity surgeon. While the modern era of hand surgery has seen a paradigm shift toward motion-preserving procedures—such as proximal row carpectomy (PRC), scaphoid excision with four-corner fusion, and total wrist arthroplasty—total wrist arthrodesis remains the unequivocal gold standard for end-stage pan-carpal disease. It is uniquely capable of transforming a profoundly painful, mechanically unstable, and functionally debilitated extremity into a stable, painless, and powerful unit optimized for forceful grip and manual labor. The philosophical approach to wrist arthrodesis is not merely one of joint ablation, but rather the strategic reconstruction of the upper extremity kinematic chain to maximize the length-tension relationship of the extrinsic flexor tendons.
The patho-epidemiology of conditions necessitating total wrist arthrodesis is diverse, encompassing post-traumatic, inflammatory, and neuromuscular etiologies. The most common post-traumatic drivers are Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC). When these conditions progress to Stage III or IV, involving the radiolunate and midcarpal joints, motion-sparing procedures are frequently contraindicated due to the widespread destruction of articular cartilage and the loss of secondary ligamentous stabilizers. Furthermore, highly comminuted intra-articular fractures of the distal radius (e.g., complex AO Type C3 fractures) that fail to reconstruct or subsequently collapse often lead to rapid, debilitating radiocarpal osteoarthritis, necessitating fusion.
Inflammatory arthropathies, particularly advanced rheumatoid arthritis (RA), present a distinct patho-epidemiological challenge. In RA, chronic synovitis leads to the attenuation of the extrinsic radiocarpal ligaments, most notably the radioscaphocapitate and radiolunate ligaments. This results in the classic ulnar translation of the carpus, volar subluxation, and profound structural collapse. By the time these patients present with Larsen Grade IV or V changes, the carpus is often a monolithic, eroded mass incapable of supporting arthroplasty, making arthrodesis the only viable option for restoring hand function and preventing further tendon attrition.
Neuromuscular disorders also form a critical subset of the epidemiological profile. Patients with spastic hemiplegia secondary to cerebral palsy, severe Volkmann ischemic contracture, or flail extremities following poliomyelitis or devastating brachial plexus injuries require wrist arthrodesis not necessarily for pain relief, but for spatial positioning. In these scenarios, the wrist is frequently locked in severe, non-functional flexion. Arthrodesis serves to place the hand in space, improving hygiene, facilitating the function of whatever residual digital motion remains, and allowing for the potential transfer of redundant wrist flexors or extensors to augment digital function.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex osteology, ligamentous architecture, and biomechanical force vectors of the wrist is mandatory for executing a successful arthrodesis. The wrist is not a single joint but a highly complex intercalated system comprising the radiocarpal, midcarpal, and distal radioulnar joints (DRUJ), all functioning synchronously to position the hand in space. The distal radius presents a biconcave articular surface with an average volar tilt of 11 degrees and a radial inclination of 22 degrees. In the setting of pan-carpal arthritis, this normal anatomical geometry is frequently distorted, with significant dorsal intercalated segment instability (DISI) or volar intercalated segment instability (VISI) deformities requiring correction during the fusion process to restore the anatomical axis.
The biomechanical foundation of wrist arthrodesis is predicated on optimizing the length-tension curve of the extrinsic digital flexors—specifically the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS). Grip strength is a direct function of wrist position. If the wrist is fused in excessive flexion, the extrinsic flexors become actively insufficient; they reach their maximal contraction length before the digits can effectively close around an object, dramatically reducing grip strength. Conversely, if the wrist is fused in excessive extension (greater than 30 degrees), the flexors are stretched to a point of passive insufficiency, and the extensor tendons are subjected to chronic bowstringing and fatigue, increasing the risk of extensor tenosynovitis and rupture over the dorsal hardware.
Therefore, the universally accepted optimal sagittal alignment for a total wrist arthrodesis is between 10 and 20 degrees of extension. In the coronal plane, the long axis of the third metacarpal shaft must be meticulously aligned with the long axis of the radial shaft, typically resulting in a neutral to slight (5-degree) ulnar deviation. This specific posture simulates the natural "dart-thrower's" functional position and maximizes the mechanical advantage of the extrinsic flexors. Intraoperatively, this position can be verified by the tenodesis effect: when the wrist is positioned correctly, passive extension of the wrist should result in a natural, cascading flexion of the digits, indicating optimal flexor tendon tension.
Furthermore, the surgical anatomy of the carpometacarpal (CMC) joints is of critical importance. The second and third CMC joints form the rigid central pillar of the hand. Haddad and Riordan famously emphasized that these joints must always be included in the arthrodesis mass. Failure to decorticate and fuse the capitate to the third metacarpal and the trapezoid to the second metacarpal allows for persistent micromotion at these articulations. Because the lever arm of the fused radiocarpal unit transfers immense stress distally, any unfused, arthritic CMC joint will rapidly become a source of debilitating, recalcitrant pain, often necessitating revision surgery to extend the fusion plate distally.
Exhaustive Indications and Contraindications
The decision algorithm for proceeding with a total wrist arthrodesis requires a meticulous evaluation of the patient's physiological age, functional demands, precise anatomical pathology, and the integrity of surrounding soft tissue envelopes. Patient selection is paramount; the surgeon must ensure that the patient fully comprehends the permanent loss of radiocarpal and midcarpal motion and is willing to trade this mobility for absolute stability and pain relief.
The primary indications for total wrist arthrodesis revolve around end-stage joint destruction where motion-preserving salvage is impossible. This includes SLAC and SNAC wrists that have progressed to Stage III (involving the capitolunate articulation) or Stage IV (pan-carpal involvement). Severe post-traumatic osteoarthritis following highly comminuted, irreparable distal radius fractures is another absolute indication. In the realm of inflammatory arthropathies, advanced rheumatoid arthritis with profound carpal collapse, ulnar translation, and impending or actual extensor tendon rupture dictates immediate fusion to salvage the remaining function of the hand. Furthermore, massive carpal bone loss secondary to tumor resection (e.g., giant cell tumor of the distal radius) or the sequelae of treated pyogenic or tuberculous osteomyelitis frequently requires arthrodesis with structural bone grafting.
Contraindications must be carefully weighed to prevent catastrophic surgical failures. The absolute contraindications include the presence of active, untreated local or systemic infection, which precludes the use of extensive internal fixation hardware and bone grafting. Severe vascular compromise to the extremity that would prevent wound healing or bone union is also an absolute contraindication. Relative contraindications require nuanced surgical judgment. For instance, an open distal radial physis in a pediatric patient is a strong relative contraindication, as iatrogenic injury will cause severe growth arrest; however, if fusion is absolutely mandatory, specialized physeal-sparing techniques must be employed.
Below is an exhaustive breakdown of the indications and contraindications for total wrist arthrodesis:
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Absolute Indications | SLAC/SNAC Stage III & IV; Severe Pan-carpal Osteoarthritis. | Articular cartilage is completely denuded; motion preservation will result in persistent, debilitating pain. |
| Inflammatory Indications | Rheumatoid Arthritis (Larsen Grade IV/V) with ulnar translation. | Prevents progressive deformity, stabilizes the kinematic chain, and protects extensor tendons from attrition. |
| Neuromuscular Indications | Spastic hemiplegia (Cerebral Palsy), severe Volkmann's contracture, Brachial Plexus palsy. | Arthrodesis places the hand in a functional spatial position, improving hygiene and facilitating tendon transfers. |
| Salvage Indications | Failed partial carpal fusions, failed total wrist arthroplasty, massive tumor resection. | Provides a definitive, stable construct when all other reconstructive or joint-sparing options have been exhausted. |
| Absolute Contraindications | Active pyogenic infection, untreated osteomyelitis, profound ischemia. | Hardware placement and bone grafting in an infected or ischemic bed will inevitably lead to catastrophic failure. |
| Relative Contraindications | Open distal radial physis (age < 12-14), severely compromised dorsal soft tissue envelope. | Requires specialized techniques (physeal sparing) or preliminary soft tissue reconstruction (e.g., free flap) prior to fusion. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful wrist arthrodesis, mitigating intraoperative surprises and ensuring the biomechanical goals of the procedure are met. The clinical evaluation must go beyond the wrist joint itself. The surgeon must evaluate the entire upper extremity kinematic chain, including elbow and shoulder range of motion, as the patient will rely on these proximal joints to compensate for the loss of wrist mobility. A thorough assessment of the distal radioulnar joint (DRUJ) is critical; if the DRUJ is arthritic or unstable, concurrent procedures such as a Darrach resection, Sauvé-Kapandji procedure, or distal ulnar tenodesis must be planned to prevent residual ulnar-sided wrist pain.
Radiographic evaluation requires a high-quality, orthogonal series of the wrist, including posteroanterior (PA), true lateral, and oblique views. These images allow the surgeon to assess the degree of carpal collapse, bone stock quality, and the presence of cystic changes that may require extensive curettage and grafting. In cases of severe trauma, previous surgery, or complex deformity, a non-contrast Computed Tomography (CT) scan with 3D reconstructions is highly recommended. The CT scan provides unparalleled detail regarding the precise location of osteophytes, the exact volume of bone graft required to fill structural defects, and the spatial relationship of the carpus to the distal radius, which is essential for planning deformity correction.
Pre-operative templating is essential for selecting the appropriate hardware. Modern AO/ASIF techniques utilize pre-contoured dorsal spanning plates (such as the Weiss and Hastings design) that are manufactured with the optimal 10 to 20 degrees of extension built into the plate geometry. Templating on the lateral radiograph ensures that the plate will adequately span from the robust diaphyseal bone of the distal radius, across the carpus (specifically targeting the capitate for central fixation), and securely engage the diaphysis of the third metacarpal. If a straight plate is to be used, the surgeon must plan the exact location and angle of the bend to be performed intraoperatively using plate benders.
Patient positioning and operating room setup must be optimized for efficiency and safety. The patient is placed in the supine position with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and typically inflated to 250 mmHg following exsanguination with an Esmarch bandage. Intravenous antibiotics are administered 30 minutes prior to inflation. The fluoroscopy unit (C-arm) is positioned either parallel to the hand table or coming in from the distal end, ensuring that true PA and lateral intraoperative images can be obtained seamlessly without compromising the sterile field. Preparation for autologous bone graft harvesting (from the ipsilateral iliac crest or proximal tibia) should be completed concurrently if local bone graft (from Lister's tubercle or the distal radius) is deemed insufficient.
Step-by-Step Surgical Approach and Fixation Technique
The evolution of wrist arthrodesis techniques has dramatically reduced the historically high pseudarthrosis rates (which once approached 30% with cast immobilization alone) to modern union rates exceeding 95%. This success is directly attributable to the application of rigid internal fixation principles utilizing the AO/ASIF techniques. While several approaches exist, the dorsal approach with rigid plating remains the gold standard.
The Dorsal Approach with AO/ASIF Plating
The dorsal approach provides excellent exposure to the radiocarpal, midcarpal, and carpometacarpal joints, allowing for meticulous joint preparation and the application of a robust tension-band construct.
1. Incision and Retinacular Management:
A longitudinal dorsal incision is made, centered precisely over Lister's tubercle. The incision extends proximally along the distal radial shaft and distally to the mid-shaft of the third metacarpal. Full-thickness fasciocutaneous flaps are elevated to protect the dorsal sensory branches of the radial and ulnar nerves. The extensor retinaculum is identified and meticulously divided. A step-cut technique is highly recommended; this allows the retinaculum to be repaired later as an interpositional flap between the extensor tendons and the dorsal hardware, mitigating the risk of tendon attrition. The extensor pollicis longus (EPL) is released from the third dorsal compartment and transposed radially. The extensor digitorum communis (EDC) tendons are retracted ulnarly, exposing the dorsal joint capsule.
2. Joint Preparation and Decortication:
The dorsal capsule is incised longitudinally and elevated as a thick flap. Lister's tubercle is excised using a rongeur or osteotome, creating a perfectly flat bed for the proximal segment of the fusion plate. This excised bone is preserved for use as local autograft. The critical phase of the operation is the meticulous decortication of the articular surfaces. Using a combination of a high-speed burr, sharp osteotomes, and curettes, the articular cartilage and subchondral sclerotic bone of the radiocarpal joint (scaphoid fossa, lunate fossa), the midcarpal joint (scaphocapitate, lunocapitate), and the second and third carpometacarpal joints are entirely removed. The decortication must proceed until healthy, bleeding cancellous bone is exposed, creating an optimal osteoinductive and osteoconductive environment.
3. Bone Grafting and Plate Application:
The decorticated joint spaces are densely packed with autogenous cancellous bone graft. If the local bone from Lister's tubercle and the distal radius is insufficient, supplemental graft from the iliac crest or advanced allograft matrices must be utilized. The pre-contoured wrist fusion plate is then applied. The plate is positioned so that the pre-bent angle sits directly over the radiocarpal joint, imparting the desired 10 to 20 degrees of extension.
Fixation begins distally. Cortical screws are placed through the plate into the diaphysis of the third metacarpal. A central screw is then meticulously targeted into the dense bone of the capitate, which acts as the keystone of the carpal arch. With the distal and central fixation secure, the plate is used as a reduction tool. As the proximal portion of the plate is clamped to the distal radius, it automatically reduces the wrist into the correct degree of extension. Proximal fixation is then achieved using locking or non-locking cortical screws in the radial diaphysis. Intraoperative fluoroscopy is utilized to confirm that the hardware does not violate the DRUJ, that screws are of appropriate length, and that the coronal alignment is perfect.
The Radial/Lateral Approach (Haddad and Riordan)
For specific clinical scenarios, Haddad and Riordan described a highly effective alternative utilizing a radial or lateral approach. This technique involves an incision centered over the radial styloid, extending proximally along the radius and distally toward the second metacarpal.
The profound advantage of this approach is the complete preservation of the dorsal soft tissue envelope and the extensor tendon compartments. By avoiding dorsal hardware, the risk of extensor tenosynovitis or rupture is drastically reduced, and the cosmetic appearance of the dorsal wrist remains unaltered. Furthermore, the distal radioulnar joint (DRUJ) is completely bypassed and preserved. The decortication is performed through the radial window, and fixation is typically achieved using stout Steinmann pins or specialized radial column plates. Haddad and Riordan reported exceptional historical success with this technique, noting only one failure in 24 wrists. However, this approach provides less rigid biomechanical stability compared to dorsal plating and requires a longer period of postoperative cast immobilization.
Limited and Partial Fusions
In highly selected patients where pathology is strictly isolated, a complete pan-carpal arthrodesis may be avoided. Radioscapholunate (RSL) fusion is indicated for post-traumatic arthritis strictly limited to the radiocarpal joint, sparing the midcarpal articulation. Bach et al. demonstrated high success rates in pain relief while preserving a functional arc of midcarpal motion. The Smith-Petersen technique, primarily described for severe rheumatoid arthritis, utilizes the excised distal end of the ulna as an interpositional bone graft. However, this technique is largely of historical interest and carries the distinct disadvantage of providing limited access for comprehensive radiocarpal decortication.
Distal Ulnar Stabilization: FCU and ECU Tenodesis
When wrist arthrodesis is performed in the setting of severe DRUJ destruction (common in RA or post-traumatic collapse), a concurrent distal ulnar resection (Darrach procedure) is often required. However, simply resecting the distal ulna can lead to painful dorsal subluxation of the remaining ulnar stump, a condition known as radioulnar impingement. To prevent this, a robust dynamic stabilization utilizing slips of the flexor carpi ulnaris (FCU) and extensor carpi ulnaris (ECU) is highly recommended.
Step-by-Step Tenodesis Technique:
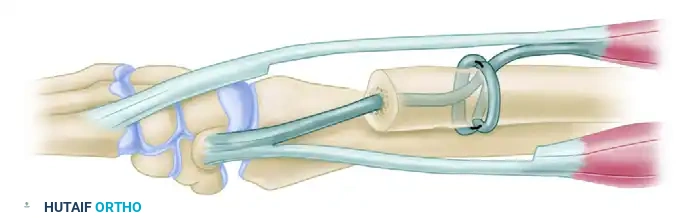
Following the resection of the distal ulna, the medullary canal of the remaining ulnar stump is identified. A drill is used to create a medullary canal tunnel starting from the distal cut end, extending proximally, and exiting through a transverse dorsal cortical hole. A second, independent dorsopalmar transverse tunnel is drilled slightly proximal to the first.
A distally based slip of the flexor carpi ulnaris (FCU) is harvested. Using a suture passer or a 20-gauge wire loop, this FCU slip is passed into the medullary canal tunnel from the distal end and pulled out through the dorsal cortical window.
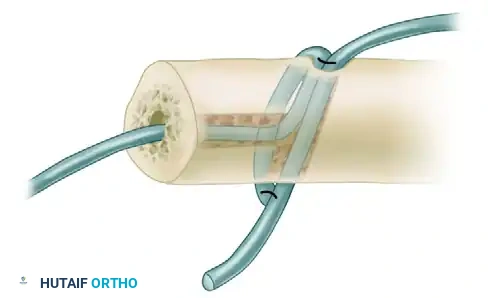
FIGURE A: The FCU slip is passed through the medullary canal and out the dorsal tunnel of the distal ulna.
Subsequently, a distally based slip of the extensor carpi ulnaris (ECU) is harvested. This slip is passed through the proximal dorsopalmar tunnel, entering dorsally and exiting on the palmar aspect of the ulna.
To achieve rigid stabilization, the forearm is placed in maximal supination. Both the FCU and ECU tendon slips are pulled under maximal tension. While maintaining this tension, the slips are securely sutured to each other using heavy, nonabsorbable braided suture (e.g., #2 FiberWire or Ethibond). This creates a robust, dynamic weave that securely tethers the distal ulna, preventing dorsal migration during forearm rotation.
FIGURE B: Completion of the weave. The ECU and FCU tendons are pulled taut with the forearm in supination and sutured to each other, creating a robust dynamic stabilization of the distal ulna.
Pediatric Considerations in Wrist Arthrodesis
Performing a wrist arthrodesis in the pediatric population requires meticulous adherence to physiological principles, primarily concerning the distal radial physis. The distal radial physis is responsible for approximately 75% of the longitudinal growth of the radius and does not close until 17 to 19 years of age. Iatrogenic injury during decortication or hardware placement will result in devastating growth arrest, leading to severe ulnar positive variance and secondary deformity.
If arthrodesis is absolutely necessary in a young child (e.g., severe spasticity or tumor), physeal-sparing techniques must be employed. Fixation should rely on smooth Kirschner wires that cross the physis centrally and perpendicularly to minimize growth disruption, rather than rigid plates. However, due to the massive amount of unossified cartilage in the pediatric carpus, achieving solid fusion is notoriously difficult. It is strongly recommended to postpone the operation until the patient is at least 10 to 12 years old, allowing for sufficient carpal ossification. If the physis has already been partially destroyed by trauma or infection, an intentional complete epiphysiodesis should be performed at the time of fusion to prevent tethered, asymmetrical growth.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates associated with modern rigid internal fixation, wrist arthrodesis is a major reconstructive undertaking with a distinct complication profile. The surgeon must be prepared to identify and manage these complications promptly to prevent catastrophic functional loss.
Nonunion or pseudarthrosis was historically the most dreaded complication, with rates approaching 30% in the era of cast immobilization. With the advent of AO/ASIF dorsal plating and meticulous decortication, nonunion rates have plummeted to between 0% and 7%. Risk factors for nonunion include active smoking, poor bone stock (severe osteopenia), inadequate joint decortication, and failure to include the CMC joints in the fusion mass. Management of a symptomatic nonunion requires revision surgery, removal of broken hardware, aggressive debridement of the pseudarthrosis site, structural iliac crest bone grafting, and application of a new, robust compression plate.
Hardware prominence and extensor tendon irritation represent the most common postoperative complaints. The dorsal soft tissue envelope of the wrist is exceptionally thin. Even with low-profile pre-contoured plates, the extensor tendons (particularly the EPL and EDC) can rub against the hardware, leading to tenosynovitis or outright spontaneous rupture. Studies indicate that symptomatic hardware requiring plate removal occurs in 10% to 15% of patients. To mitigate this, meticulous repair of the extensor retinaculum over the plate is mandatory.
Below is a summary of common complications, their incidence, and management strategies:
| Complication | Estimated Incidence | Etiology & Risk Factors | Salvage & Management Strategy |
|---|---|---|---|
| Nonunion / Pseudarthrosis | 2% - 7% | Smoking, inadequate decortication, failure to fuse 2nd/3rd CMC joints. | Revision open reduction internal fixation (ORIF) with structural autogenous iliac crest bone graft. |
| Symptomatic Hardware | 10% - 15% | Thin dorsal soft tissue envelope, prominent screw heads, straight plates. | Plate removal (only after solid radiographic union is confirmed, typically > 6-9 months). |
| Extensor Tendon Rupture | 1% - 3% | Attrition over dorsal plate, failure to interpose retinaculum. | Tendon transfer (e.g., EIP to EPL) and simultaneous hardware removal. |
| DRUJ Instability / Pain | 5% - 10% | Unrecognized pre-operative DRUJ arthritis, failed Darrach resection. | Distal ulnar tenodesis (FCU/ECU weave) or conversion to Sauvé-Kapandji procedure. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 5% | Unclear etiology, exacerbated by poor pain control and prolonged casting. | Aggressive physical therapy, stellate ganglion blocks, gabapentinoids, Vitamin C prophylaxis. |
Phased Post-Operative Rehabilitation Protocols
The success of a wrist arthrodesis is heavily dependent on a structured, phased postoperative rehabilitation protocol. While the AO/ASIF plate provides rigid internal fixation, the construct is still vulnerable to catastrophic failure if subjected to premature cyclical loading or massive torque before biological union occurs.
Phase 1: Immediate Postoperative Phase (Weeks 0 - 2)
Immediately following wound closure, the extremity is placed in a bulky, well-padded compressive dressing and a rigid volar and dorsal plaster splint. The wrist is immobilized in the fused position. Crucially, the elbow is flexed to 90 degrees, and the forearm is positioned in neutral to full supination—especially if a distal ulnar tenodesis was performed, to protect the tendon weave. The primary goals during this phase are aggressive edema control, pain management, and the immediate initiation of active range of motion (ROM) of the digits, elbow, and shoulder to prevent stiffness and reduce the risk of CRPS.
Phase 2: Subacute Immobilization (Weeks 2 - 6)
At the first postoperative clinic visit (typically 10 to 14 days), the splint is removed, and the surgical site is meticulously inspected for signs of dehiscence or infection. Sutures or staples are removed. The patient is then transitioned into a custom-molded, rigid short-arm cast or a thermoplastic Munster-style splint (if forearm rotation needs to be controlled). Strict immobilization of the wrist is continued. Patients are instructed to avoid any lifting, pushing, or pulling with the operative extremity. Digital ROM exercises are intensified, focusing on achieving full composite flexion and extension.
