Transfer of Extensor Hallucis Longus with Arthrodesis of the Interphalangeal Joint of the Hallux

Key Takeaway
The transfer of the extensor hallucis longus (EHL) combined with arthrodesis of the interphalangeal (IP) joint is a powerful surgical technique for correcting supple hallux varus deformities. By fusing the IP joint, the flexor hallucis longus acts exclusively on the metatarsophalangeal joint, correcting extension contractures. This guide details the Johnson and Spiegl technique, providing orthopedic surgeons with step-by-step instructions, biomechanical rationale, and critical pearls for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Iatrogenic hallux varus represents a profound, multiplanar biomechanical failure of the first ray, most frequently encountered as a devastating complication following aggressive or poorly executed hallux valgus corrective surgery. The deformity is clinically characterized by the medial deviation of the great toe at the metatarsophalangeal (MTP) joint, but this transverse plane abnormality is rarely isolated. It is almost universally accompanied by severe sagittal plane imbalances, specifically MTP joint extension and interphalangeal (IP) joint flexion, producing a rigid claw toe or malleus deformity of the hallux. Furthermore, a coronal plane supination deformity often manifests, rendering the plantar aspect of the toe completely non-functional during the terminal stance phase of the gait cycle. The resulting clinical picture is one of significant pain, profound footwear difficulty, and severe cosmetic dissatisfaction.
The underlying pathophysiology of iatrogenic hallux varus is rooted in a catastrophic musculotendinous and ligamentous imbalance at the first MTP joint. Historically, procedures that aggressively addressed the medial eminence—such as the classic McBride bunionectomy—carried a notoriously high risk of this complication. Over-resection of the medial metatarsal head (colloquially known as "staking the head") eliminates the critical medial bony buttress that stabilizes the proximal phalanx. Concurrently, excessive lateral soft tissue release, particularly the inadvertent or intentional excision of the fibular sesamoid, destroys the lateral tethering complex. This removes the lateral stabilizing forces of the adductor hallucis and the lateral head of the flexor hallucis brevis (FHB).
Once the lateral restraints are compromised, the medial structures—specifically the abductor hallucis and the medial head of the FHB—exert an unopposed deforming force. The abductor hallucis, which normally sits plantar-medial to the MTP joint axis, subluxates dorsally and medially, converting its primary vector into an aggressive adductor and extensor of the proximal phalanx. This dynamic imbalance is progressive; over time, the medial capsule undergoes severe contracture, and the deformity transitions from a flexible, dynamic nuisance to a rigid, fixed structural pathology.
When conservative measures such as wide-toe box shoes, taping, and orthoses fail to alleviate symptoms, surgical intervention becomes mandatory. The algorithmic approach to surgical correction is entirely dictated by the flexibility of the MTP and IP joints, as well as the presence or absence of degenerative articular changes. For a static, rigid, or arthritic MTP joint, primary arthrodesis remains the undisputed gold standard, providing reliable pain relief and functional stability. However, in the presence of a supple deformity without advanced osteoarthritis, joint-sparing dynamic reconstruction is paramount. The transfer of the entire extensor hallucis longus (EHL) tendon, combined with obligate IP joint arthrodesis—pioneered by Johnson and Spiegl—remains the premier surgical method for neutralizing these deforming forces and restoring the biomechanical axis of the first ray.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the first ray is non-negotiable for the orthopedic surgeon attempting this complex reconstruction. The first MTP joint is a highly specialized, multi-axial condylar joint stabilized by a complex interplay of capsuloligamentous structures and dynamic musculotendinous units. The static stabilizers include the medial and lateral collateral ligaments, the sesamoid complex, and the plantar plate. The dynamic stabilizers include the EHL, the extensor hallucis brevis (EHB), the abductor hallucis, the adductor hallucis, the flexor hallucis longus (FHL), and the flexor hallucis brevis (FHB). In the setting of hallux varus, this intricate balance is fundamentally destroyed, requiring surgical re-engineering rather than simple anatomical repair.
The extensor hallucis longus muscle originates from the middle half of the anterior surface of the fibula and the adjacent interosseous membrane. Its tendon descends deep to the superior extensor retinaculum and passes through a distinct compartment in the inferior extensor retinaculum. Distally, it courses over the dorsum of the first MTP joint, inserting firmly into the dorsal base of the distal phalanx. The EHL functions primarily as a powerful extensor of the IP joint, a secondary extensor of the MTP joint, and a weak dorsiflexor of the ankle. Its excursion is significant, making it an ideal candidate for tendon transfer. However, its dorsal position means that in a hallux varus deformity, the EHL often bowstrings medially, exacerbating both the varus and the MTP extension contracture.
The biomechanical rationale for the Johnson and Spiegl procedure is elegant in its simplicity but complex in its execution. By detaching the EHL from the distal phalanx and rerouting it proximally, the surgeon eliminates the primary extensor force across the IP joint. If the IP joint were left intact, the unopposed pull of the massive flexor hallucis longus (FHL) would rapidly and inevitably drive the toe into a rigid, painful flexion deformity (clawing). Therefore, arthrodesis of the IP joint is not merely an adjunct; it is an absolute biomechanical necessity. Fusion of the IP joint provides a distinct secondary advantage: by eliminating motion at the terminal joint, the entire excursion and force vector of the FHL are redirected to the MTP joint. The FHL transforms into an exceptionally powerful plantarflexor of the great toe at the MTP joint, directly counteracting the MTP extension contracture that is universally present in this pathology.
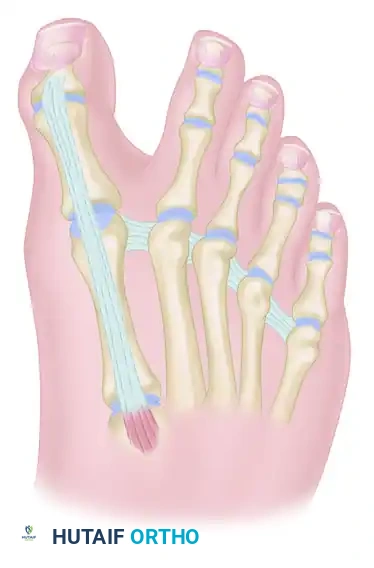
The routing of the transferred EHL tendon is the crux of the dynamic correction. The deep transverse metatarsal ligament (DTML), a robust fibrous band connecting the plantar plates of adjacent metatarsal heads, serves as a critical anatomical pulley. By passing the EHL tendon plantar to the DTML and then routing it dorsally into the base of the proximal phalanx, the vector of the EHL is radically altered. It is converted from a dorsal-medial deforming force into a plantar-lateral correcting tether. The transferred tendon effectively substitutes for the incompetent or absent lateral collateral ligament and conjoint tendon, providing a dynamic lateral restraint that actively plantarflexes and abducts the proximal phalanx during the swing phase of gait. Attempts to utilize a "split" EHL transfer to preserve IP joint motion are biomechanically flawed; a single muscle belly cannot simultaneously provide adequate IP extension and sufficient MTP plantarflexion/abduction, inevitably leading to weakness, attenuation of the transfer, and recurrent deformity.
Exhaustive Indications and Contraindications
The decision to proceed with an EHL transfer and IP joint arthrodesis must be based on a rigorous clinical and radiographic evaluation. Patient selection is the primary determinant of surgical success or failure. The procedure is highly specific in its indications, and expanding these parameters invariably leads to unacceptable complication rates and the need for revision surgery. The surgeon must meticulously assess the flexibility of the deformity, the integrity of the articular cartilage, and the neuromuscular status of the patient.
The primary indication for this procedure is a supple, iatrogenic hallux varus deformity accompanied by a dynamic MTP extension contracture. "Supple" is defined as the ability to passively reduce the MTP joint to a neutral alignment in both the transverse and sagittal planes without encountering a rigid, unyielding block. This flexibility indicates that the medial capsular contracture is not absolute and that the articular surfaces are capable of concentric reduction. Furthermore, the procedure is indicated for patients who have failed previous, less aggressive soft tissue reconstructions, such as isolated medial capsular reefing, abductor hallucis release, or simple EHB tenodesis. These isolated soft tissue procedures often fail because they do not provide a sufficiently robust, dynamic lateral tether to counteract the profound medial imbalance.
Conversely, the contraindications are absolute and must be respected. A rigid or fixed deformity that cannot be passively reduced to neutral is a definitive contraindication. In such cases, attempting a tendon transfer will result in immediate surgical failure, as the transferred EHL will simply stretch out or rupture against the unyielding medial contracture. Similarly, severe degenerative joint disease (osteoarthritis) of the first MTP joint precludes any joint-sparing procedure. Transferring a tendon across an arthritic joint will only exacerbate pain and accelerate joint destruction. Finally, patients with underlying neuromuscular disorders, such as spasticity (e.g., cerebral palsy, stroke) or profound neuropathy (e.g., advanced Charcot arthropathy), are poor candidates. The predictability of tendon transfers relies on normal muscle phasing and proprioception, both of which are compromised in these populations.
Summary of Indications and Contraindications
| Category | Specific Parameter | Clinical Rationale |
|---|---|---|
| Indications | Supple Hallux Varus | MTP joint must be passively correctable to neutral alignment to allow the tendon transfer to function without over-tensioning. |
| Dynamic MTP Extension | The transferred EHL, combined with the redirected FHL post-IP fusion, effectively neutralizes dynamic extension forces. | |
| Failed Soft Tissue Release | Provides a robust, dynamic lateral tether when simple capsular releases or static tenodeses have proven insufficient. | |
| Adequate Bone Stock | Sufficient bone density in the proximal and distal phalanges is required for secure IP joint screw fixation and proximal phalanx tendon anchoring. | |
| Contraindications | Rigid/Fixed Deformity | Inability to passively reduce the joint will lead to immediate attenuation and failure of the tendon transfer. Requires primary MTP arthrodesis. |
| Severe MTP Osteoarthritis | Joint-sparing procedures are contraindicated in the presence of painful, advanced degenerative joint disease. | |
| Neuromuscular Disorders | Spasticity or profound neuropathy compromises the predictable phasing and tensioning required for a successful dynamic transfer. | |
| Active Infection | Any active local or systemic infection is an absolute contraindication to elective reconstructive surgery and hardware implantation. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the foundation of a successful Johnson and Spiegl reconstruction. The clinical examination must go beyond simply observing the deformity. The surgeon must perform a detailed assessment of the first ray's flexibility, utilizing a maneuver akin to the Silfverskiöld test to differentiate between gastrocnemius tightness and isolated first ray pathology. The MTP joint is manipulated through its full arc of motion to assess for crepitus, which may indicate underlying, unappreciated chondral damage. The resting posture of the hallux in a weight-bearing state is documented, paying close attention to the degree of varus, MTP extension, and IP flexion.
Radiographic evaluation requires standard weight-bearing anteroposterior (AP), lateral, and sesamoid axial views of the foot. On the AP view, the surgeon must evaluate the intermetatarsal angle, the hallux valgus/varus angle, and the congruency of the MTP joint. A critical assessment of the metatarsal head morphology is necessary; evidence of previous "staking" (over-resection of the medial eminence) confirms the loss of the medial bony buttress. The sesamoid axial view is paramount for determining the presence, absence, or subluxation of the fibular and tibial sesamoids. The lateral radiograph provides insight into the degree of sagittal plane deformity and allows for templating of the proximal and distal phalanges to select the appropriate length for the 4.0-mm IP joint lag screw.
Patient counseling during the preoperative phase is mandatory and must be exhaustively documented. The patient must be explicitly informed that while a joint-sparing tendon transfer is planned, intraoperative findings—such as unexpected severe cartilage degradation or an inability to achieve a tension-free reduction—may necessitate an immediate pivot to a primary MTP joint arthrodesis. Furthermore, patients must understand the functional trade-offs of the procedure. The primary goal is a stable, plantigrade, and well-aligned toe that fits comfortably in a standard shoe. However, both the EHL transfer and the IP joint arthrodesis will significantly reduce the overall arc of motion of the great toe. The patient must be psychologically prepared to accept this reduction in MTP joint kinematics in exchange for structural correction and pain relief.
The procedure is typically performed under regional anesthesia (e.g., a popliteal sciatic nerve block combined with a saphenous nerve block) or general anesthesia, depending on patient preference and comorbidities. A well-padded calf or thigh tourniquet is applied to ensure a pristine, bloodless surgical field, which is critical for identifying delicate neurovascular structures and assessing tendon excursion. The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the lower extremity to a neutral position, ensuring the foot rests perfectly vertical. This positioning is crucial for accurately assessing the coronal and transverse plane alignment of the hallux during the tendon tensioning phase of the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the Johnson and Spiegl technique demands meticulous soft tissue handling, precise osseous preparation, and an intuitive understanding of dynamic tensioning. The procedure is divided into discrete, highly technical phases, each of which must be completed flawlessly to ensure a successful outcome.
Incision and Surgical Exposure
The approach utilizes an L-shaped or gently curved dorsal incision designed to maximize exposure of both the MTP and IP joints while strictly respecting the dorsal angiosomes of the hallux. The incision is initiated in the first web space, precisely between the midportions of the first and second metatarsals. This proximal starting point is essential for accessing the deep transverse metatarsal ligament later in the procedure. The incision is then extended distally along the dorsolateral aspect of the great toe, curving gently medialward as it approaches the insertion of the EHL tendon at the base of the distal phalanx.

Meticulous, layer-by-layer dissection is required to identify and protect the dorsal medial and dorsal lateral cutaneous nerves of the hallux. These nerves are often enveloped in post-surgical scar tissue from previous bunionectomies. Inadvertent transection or aggressive traction injury to these nerves will result in a painful postoperative neuroma, which can severely compromise an otherwise structurally perfect correction. Retraction should be performed with blunt instruments, and the nerves should be gently mobilized and protected with vessel loops if necessary. Furthermore, extreme care must be taken at the distal extent of the incision to avoid violating the germinal matrix of the nail bed, which would lead to permanent nail dystrophy.
Extensor Hallucis Longus Tendon Harvest
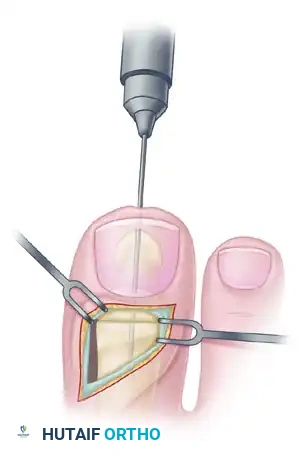
Once the dorsal structures are exposed, the EHL tendon is identified along its entire course over the first ray. The tendon is traced distally to its broad insertion at the dorsal base of the distal phalanx. To maximize the functional length of the graft, the tendon must be sharply divided directly at its osseous insertion; no stump should be left behind.
Following detachment, the EHL tendon is systematically dissected free from the extensor hood mechanism and its proximal fascial attachments. This mobilization must extend 5 to 6 cm proximal to the MTP joint. Adequate proximal mobilization is a critical step; failure to free the muscle belly sufficiently will severely limit tendon excursion, making it impossible to route the tendon under the transverse metatarsal ligament without applying excessive, non-physiologic tension. The mobilized tendon is wrapped in a saline-soaked sponge to prevent desiccation while attention is turned to the interphalangeal joint.
Preparation for Interphalangeal Joint Arthrodesis
With the EHL detached and reflected proximally, the dorsal capsule of the IP joint is fully exposed. A transverse arthrotomy is performed, sharply dividing the collateral ligaments to allow for acute plantarflexion of the distal phalanx. This maneuver "shotguns" the joint, providing excellent visualization of the articular surfaces of both the head of the proximal phalanx and the base of the distal phalanx.

Using a high-speed microsaw or a sharp rongeur, the articular cartilage is systematically resected down to healthy, bleeding subchondral bone. The cuts must be meticulously planned to be perfectly flat and parallel. The goal is to appose the bony surfaces in a neutral position in both the sagittal and coronal planes. Any inadvertent angulation during the bone cuts will result in a malaligned IP joint, leading to abnormal pressure distribution on the plantar aspect of the toe and potential ulceration. The subchondral bone may be further fenestrated with a 2.0-mm drill bit to release marrow elements and promote robust osteogenesis across the arthrodesis site.
IP Joint Fixation (Shives and Johnson Technique)
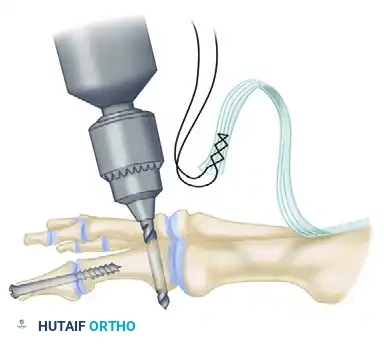
Rigid internal fixation is paramount for achieving a high rate of bony union. The technique advocated by Shives and Johnson utilizes a single 4.0-mm partially threaded cancellous lag screw, which provides exceptional interfragmentary compression and rotational stability. The process begins with retrograde drilling. A 2.0-mm diameter drill bit is introduced longitudinally into the center of the denuded articular surface of the distal phalanx. The drill is advanced distally until it exits the skin at a point exactly 5 mm plantar to the tip of the nail in the midline of the toe.
Next, the denuded articular surfaces of the proximal and distal phalanges are manually apposed in perfect neutral alignment. The drill bit is then inserted in an antegrade fashion through the previously created distal exit hole. It is advanced proximally, following the retrograde path, crossing the IP joint interface, and driven deep into the medullary canal of the proximal phalanx.

To achieve a true biomechanical lag effect, the near cortex (the distal phalanx) must be overdrilled. A 2.7-mm drill bit is used to overdrill the distal phalanx, creating a gliding hole that prevents the screw threads from purchasing in the distal fragment. The entire drill path is then tapped with a 3.5-mm tap to prepare the dense subchondral bone for the cancellous screw.
A 4.0-mm partially threaded cancellous bone screw of appropriate length (typically 26 to 34 mm) is inserted along the prepared path. As the head of the screw engages the distal cortex of the distal phalanx, the threads purchase exclusively in the proximal phalanx. Continued advancement produces robust, dynamic compression across the arthrodesis site, ensuring absolute rigidity.

EHL Tendon Routing and Transfer
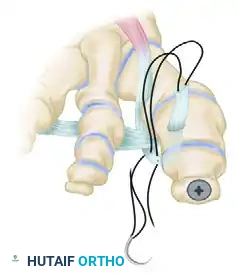
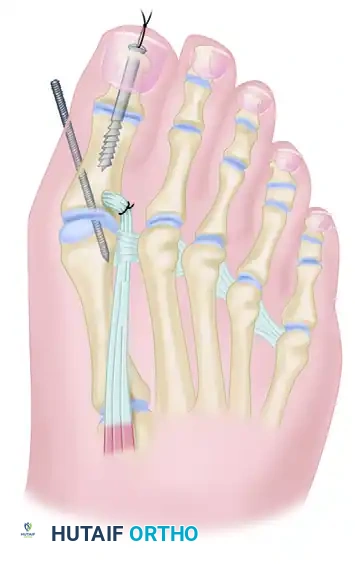
With the IP joint securely fused, the critical dynamic phase of the operation begins. The surgeon must identify the deep transverse metatarsal ligament (DTML) deep within the first web space. This structure is often obscured by scar tissue and requires careful, blunt dissection to isolate safely without injuring the adjacent neurovascular bundles. Once identified, a curved hemostat is passed plantar to the DTML from lateral to medial. The mobilized EHL tendon is grasped and pulled through this space. This is the most vital biomechanical step of the procedure, as it fundamentally changes the vector of the EHL pull from dorsal-medial to plantar-lateral.

Following its passage under the DTML, the EHL tendon is routed dorsally toward the lateral aspect of the base of the proximal phalanx.
An osseous tunnel must be created to anchor the transfer. Using a 3.2-mm or 3.5-mm drill bit, a transverse hole is drilled through the base of the proximal phalanx, passing from lateral to medial. The hole should be positioned approximately 1 cm distal to the articular surface to avoid violating the joint capsule. The EHL tendon is then passed through this tunnel from lateral to medial.
Tensioning the transfer is an art form that requires significant clinical experience. The surgeon applies tension to the EHL tendon while an assistant holds the MTP joint in approximately 10 to 15 degrees of extension and perfect neutral coronal alignment, thereby fully correcting the varus deformity.
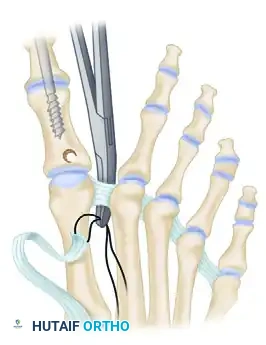
While maintaining this precise tension and alignment, the tendon is sutured back onto itself. Heavy, non-absorbable braided suture (such as #2-0 FiberWire or Ethibond) is used to secure the tendon loop. Multiple figure-of-eight and horizontal mattress sutures are placed to ensure the construct will not slip under physiological load.

The tension must be absolutely perfect. Over-tensioning will result in a rigid, plantarflexed MTP joint that causes significant pain and functional limitation during the toe-off phase of gait. Under-tensioning will fail to provide the necessary lateral tether, leading to rapid recurrence of the varus deformity. Once the suturing is complete, the toe should rest naturally in a neutral, plantigrade alignment without any manual support.
Closure and Radiographic Confirmation
Prior to closure, the tourniquet is deflated, and meticulous hemostasis is achieved using electrocautery. Hematoma formation in the web space can lead to severe fibrosis and compromise the excursion of the transferred tendon. The subcutaneous tissues are closed with interrupted absorbable sutures, ensuring that the knot tails do not irritate the overlying skin. The skin is then closed with non-absorbable monofilament sutures (e.g., 3-0 or 4-0 nylon) using a horizontal mattress or simple interrupted technique.

Intraoperative fluoroscopy is mandatory before the patient leaves the operating room. Standard AP, lateral, and oblique views are obtained to confirm the concentric reduction of the MTP joint, the complete correction of the varus angle, and the optimal placement and compression of the 4.0-mm IP joint screw. The screw threads must be entirely within the proximal phalanx, and the joint line should demonstrate no gapping.

Complications, Incidence Rates, and Salvage Management
While the Johnson and Spiegl technique is highly effective and remains the gold standard for supple hallux varus, it is a technically demanding procedure associated with specific risks. The orthopedic surgeon must be acutely aware of these potential complications, their incidence rates, and the appropriate salvage pathways.
Nonunion of the IP joint is the most frequently encountered osseous complication, occurring in up to 5% to 10% of cases. Risk factors include inadequate resection of the sclerotic subchondral bone, failure to achieve true interfragmentary compression with the lag screw, thermal necrosis during drilling, and patient non-compliance with strict postoperative weight-bearing restrictions. Clinically, a nonunion may present as persistent swelling, pain at the IP joint, or hardware failure (screw breakage). If the nonunion is entirely asymptomatic and structurally stable, it may be managed observationally. However, a painful nonunion requires revision surgery, typically involving removal of hardware, debridement of the fibrous nonunion site, application of structural autograft (e.g., from the calcaneus or proximal tibia), and revision fixation with a larger diameter screw or a dedicated IP joint fusion plate.
Hardware prominence is a common soft-tissue complication. The head of the 4.0-mm screw, located at the very distal tip of the phalanx, has minimal soft tissue coverage. As postoperative edema subsides, the screw head can cause significant irritation, erythema, and even skin breakdown against the toe box of closed shoes. This complication is easily managed but requires patience. The screw should not be removed until solid bony union is unequivocally confirmed on radiographs, typically requiring a minimum of 6 months postoperatively. Once union is achieved, screw removal is a minor outpatient procedure performed under local anesthesia.
Recurrent deformity (undercorrection) and overcorrection (iatrogenic hallux
