Total Wrist Arthrodesis: The Dorsal Compression Plate Technique
Key Takeaway
Total wrist arthrodesis utilizing a dorsal compression plate is a highly reliable salvage procedure for end-stage radiocarpal and midcarpal arthritis. This technique provides rigid internal fixation, promoting high fusion rates while maintaining optimal wrist alignment. By combining meticulous joint preparation, autologous bone grafting, and dynamic compression principles, surgeons can achieve a stable, pain-free wrist, significantly improving patient grip strength and overall upper extremity function.
Comprehensive Introduction and Patho-Epidemiology
Total wrist arthrodesis remains the unequivocal gold standard salvage procedure for end-stage pancarpal arthritis, severe carpal instability, and complex paralytic deformities of the upper extremity. When joint-preserving procedures, proximal row carpectomy, or partial wrist fusions are no longer viable options due to advanced articular destruction or profound instability, a solid radiocarpal and intercarpal fusion provides a stable, pain-free foundation. This foundation reliably restores grip strength and functional utility to the hand, converting a mechanically disadvantaged and painful appendage into a robust functional terminal effector. The historical evolution of this procedure has transitioned from the use of intramedullary Steinmann pins and cast immobilization—which carried unacceptably high rates of pseudarthrosis and hardware migration—to the modern application of rigid dorsal plate osteosynthesis.
The patho-epidemiology of conditions necessitating total wrist arthrodesis is diverse, encompassing both degenerative and inflammatory cascades. Post-traumatic osteoarthritis, most notably Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC), accounts for a significant proportion of these cases. In the natural history of SLAC and SNAC wrists, the progressive alteration of carpal kinematics leads to predictable patterns of articular wear, culminating in Stage III or IV disease where the radiolunate and midcarpal joints are entirely denuded of cartilage. Similarly, primary osteoarthritis, though less common in the wrist than in the weight-bearing joints of the lower extremity, can progress to end-stage pancarpal involvement, particularly in manual laborers subjected to decades of repetitive axial and torsional loading.
In the realm of systemic inflammatory arthropathies, rheumatoid arthritis frequently targets the radiocarpal and midcarpal joints. The hypertrophic synovitis characteristic of rheumatoid disease inherently attenuates the intrinsic and extrinsic carpal ligaments, leading to profound carpal subluxation, ulnar translation, and eventual volar dislocation of the carpus relative to the distal radius. While total wrist arthroplasty may be considered in low-demand rheumatoid patients with preserved bone stock, those with severe articular destruction, profound deformity, or high functional demands are best served by total wrist arthrodesis. The procedure halts the destructive inflammatory cascade at the wrist level, realigns the hand with the forearm axis, and drastically improves the mechanics of the digital flexors and extensors.
Furthermore, neuromuscular disorders present a unique patho-epidemiologic subset requiring total wrist arthrodesis. Patients with spastic hemiplegia secondary to cerebral palsy, cerebrovascular accidents, or traumatic brain injuries often develop severe flexion contractures of the wrist. This spasticity overpowers the wrist extensors, rendering the hand virtually useless for prehension and creating severe hygiene challenges in the palmar crease. Similarly, in the setting of devastating brachial plexus palsies, establishing a rigid wrist pillar is a prerequisite for successful distal tendon transfers. The Compression Plate Technique, utilizing a dorsal dynamic compression plate (DCP) combined with autologous corticocancellous bone grafting, emerged as a biomechanically superior method to address all these pathologies, neutralizing flexion forces and providing the rigid internal fixation necessary for high union rates.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the dorsal surgical anatomy of the wrist is paramount for the safe and effective execution of a total wrist arthrodesis. The dorsal approach requires meticulous navigation through the extensor retinaculum and the six extensor compartments. The primary surgical window is traditionally developed between the third extensor compartment, which houses the Extensor Pollicis Longus (EPL), and the fourth compartment, which contains the Extensor Digitorum Communis (EDC) and the Extensor Indicis Proprius (EIP). Lister's tubercle, a prominent osseous ridge on the dorsal distal radius, serves as the critical anatomical landmark for identifying this interval. The EPL tendon uses Lister's tubercle as a fulcrum to change its vector toward the thumb; during the surgical approach, the EPL must be released from its compartment and transposed radially to prevent iatrogenic injury and subsequent hardware-induced attrition.
Deep to the extensor tendons lies the dorsal radiocarpal ligamentous complex, primarily composed of the dorsal radiocarpal ligament and the dorsal intercarpal ligament. These structures, along with the dorsal capsule, must be meticulously elevated. It is standard practice to develop an H-shaped or I-shaped capsulotomy, creating robust proximal and distal capsular flaps. This step is not merely for exposure; it is a critical biomechanical and anatomical maneuver. The preserved capsular tissue is later utilized to interpose between the rigid metallic compression plate and the overlying extensor tendons, thereby mitigating the risk of postoperative tendon irritation, tenosynovitis, or frank rupture. Furthermore, the surgeon must be acutely aware of the terminal branches of the Posterior Interosseous Nerve (PIN) located at the floor of the fourth compartment, which are routinely excised during the exposure to provide a degree of regional denervation and postoperative pain relief.
From a biomechanical perspective, the normal wrist is subjected to significant volar flexion forces during routine hand use, driven by the powerful extrinsic finger and wrist flexors. Placing a dynamic compression plate on the dorsal surface of the radius, carpus, and third metacarpal capitalizes on the tension band principle. When the hand attempts to flex volarly under physiologic loading, the dorsal plate is placed under tension. Because the plate is rigidly fixed to the bone, it resists this tension and, in turn, converts the deforming flexion forces into compressive forces across the volar radiocarpal and intercarpal articulations. This dynamic compression is the cornerstone of primary bone healing, ensuring that the arthrodesis site remains under continuous, stable compression throughout the postoperative period.
The optimal position of fusion is a critical biomechanical consideration that directly dictates the functional outcome of the hand. The wrist is typically fused in 10 to 15 degrees of extension and slight ulnar deviation (0 to 5 degrees). This specific alignment maximizes the mechanical advantage of the extrinsic finger flexors through the tenodesis effect, optimizing grip strength. If the wrist is fused in excessive extension, the patient may experience difficulty with activities of daily living that require reaching into confined spaces or performing perineal care. Conversely, fusion in flexion severely compromises grip strength by shortening the functional excursion of the flexor tendons. The plate is aligned along the longitudinal axis of the radius, crossing the central column (lunate and capitate), and anchoring securely into the diaphyseal bone of the third metacarpal, thereby bypassing the mobile ulnar column (fourth and fifth carpometacarpal joints) to preserve the transverse metacarpal arch.
Exhaustive Indications and Contraindications
The decision to proceed with a total wrist arthrodesis must be predicated on a rigorous clinical and radiographic evaluation, balancing the patient's functional demands, pain levels, and underlying pathology. Primary indications represent scenarios where the joint architecture is irreversibly compromised, and joint-preserving procedures are destined to fail. Advanced post-traumatic osteoarthritis, specifically SLAC and SNAC wrists at Stage III or IV, are classic primary indications. In these stages, the degenerative process has extended beyond the radioscaphoid articulation to involve the capitolunate joint, precluding the use of a proximal row carpectomy or a four-corner fusion. Similarly, end-stage pancarpal primary osteoarthritis and advanced Kienböck's disease (Lichtman Stage IV), where lunate collapse has incited global carpal arthritis, strongly warrant total wrist arthrodesis to restore a painless, stable grip.
Rheumatoid arthritis presents a distinct set of indications, often characterized by severe articular destruction, profound carpal subluxation, and ulnar translation of the carpus. In rheumatoid patients with high functional demands, poor bone stock, or a history of extensor tendon ruptures, arthrodesis is favored over arthroplasty. Furthermore, total wrist arthrodesis serves as the ultimate salvage procedure for failed previous surgeries. Nonunions of partial wrist fusions, painful failed proximal row carpectomies, and aseptic loosening or catastrophic failure of total wrist arthroplasties are routinely salvaged with a total wrist fusion. In these revision scenarios, the surgeon must be prepared to manage significant cavitary bone defects, often necessitating massive structural autografting or specialized spanning plates to bridge compromised bone segments.
Despite its reliability, total wrist arthrodesis is subject to strict contraindications that must be respected to avoid catastrophic outcomes. Active infection, whether local to the wrist or systemic, is an absolute contraindication; any septic process must be definitively eradicated with surgical debridement and appropriate antimicrobial therapy prior to the implantation of extensive orthopedic hardware. In the pediatric population, an open distal radial physis represents another absolute contraindication. Arthrodesis plates crossing the physis will inevitably tether growth, leading to severe forearm length discrepancies and angular deformities. In such cases, if stabilization is absolutely necessary, it must be achieved via physeal-sparing techniques or temporary soft-tissue stabilization until skeletal maturity is reached.
Relative contraindications require nuanced clinical judgment. An inadequate soft tissue envelope, often seen in patients with severe burns, prior extensive trauma, or multiple previous surgical incisions, may preclude the use of bulky dorsal hardware due to the unacceptably high risk of wound breakdown and hardware exposure. In these instances, alternative fixation methods, such as intramedullary rods or external fixation, may be considered. Furthermore, quadriplegia, particularly in patients with C6-level spinal cord injuries, represents a critical relative contraindication. These patients rely heavily on the tenodesis effect—utilizing active wrist extension to passively drive finger flexion for prehension. Fusing the wrist eliminates this dynamic tenodesis grasp, potentially devastating the patient's remaining functional independence.
| Category | Specific Condition | Clinical Rationale / Management Strategy |
|---|---|---|
| Primary Indications | SLAC/SNAC Stage III & IV | Global articular destruction precludes partial fusions; requires complete stabilization. |
| Primary Indications | Severe Rheumatoid Arthritis | Halts inflammatory destruction, corrects ulnar translation, provides stable pillar. |
| Salvage Indications | Failed Partial Fusion / TWA | Addresses nonunion or hardware failure; often requires structural iliac crest grafting. |
| Absolute Contraindication | Active Local/Systemic Infection | Hardware implantation in a septic field guarantees failure; requires prior eradication. |
| Absolute Contraindication | Open Distal Radial Physis | Hardware crossing the physis causes growth arrest; delay surgery until skeletal maturity. |
| Relative Contraindication | Quadriplegia (C6 Level) | Fusing the wrist destroys the functional tenodesis grasp required for ADLs. |
| Relative Contraindication | Poor Soft Tissue Envelope | High risk of plate exposure; consider alternative fixation or preliminary flap coverage. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful total wrist arthrodesis, beginning with a comprehensive clinical examination. The surgeon must meticulously assess the patient's current grip strength, digital range of motion, and the integrity of the extrinsic flexor and extensor tendons. Particular attention must be paid to the soft tissue envelope on the dorsal aspect of the wrist, mapping out prior surgical scars that could compromise flap viability during the surgical approach. Furthermore, evaluating the ipsilateral shoulder and elbow is mandatory; a fused wrist will inevitably unmask or exacerbate proximal kinematic deficits, as the patient will no longer be able to compensate for limited shoulder rotation or elbow pronosupination with wrist movements.
Radiographic evaluation requires standard posteroanterior (PA), lateral, and oblique views of the wrist, extending to include the distal third of the radius and the entire metacarpal length. In cases of severe deformity, rheumatoid arthritis, or revision surgery, a non-contrast Computed Tomography (CT) scan is highly recommended. CT imaging provides unparalleled detail regarding the available bone stock, the presence of subchondral cysts, and the precise three-dimensional geometry of the carpal collapse. Digital templating software is then utilized to determine the appropriate plate size—typically a seven-hole or eight-hole 3.5-mm dynamic compression plate (DCP) or a modern, pre-contoured, low-profile wrist fusion plate. Templating ensures that the chosen hardware will adequately span the radiocarpal and midcarpal joints while securing sufficient bicortical purchase in the diaphysis of the third metacarpal.
A critical, often overlooked element of preoperative planning is the evaluation of the Distal Radioulnar Joint (DRUJ). Total wrist arthrodesis fundamentally alters the kinematics of the forearm. By locking the radiocarpal joint, rotational torques normally dissipated through wrist motion are entirely transferred to the DRUJ. If the DRUJ is already arthritic, unstable, or impinged due to carpal settling, the patient will experience severe, debilitating pain during forearm pronation and supination postoperatively. Therefore, if DRUJ pathology is identified preoperatively, concurrent surgical intervention must be planned. This may involve a Darrach procedure (resection of the distal ulna), a Sauvé-Kapandji procedure (DRUJ arthrodesis with proximal ulnar pseudoarthrosis), or an ulnar head arthroplasty, depending on the patient's age and functional demands.
Patient positioning and operating room setup must be orchestrated to facilitate both the primary wrist procedure and the simultaneous harvest of autologous bone graft. The patient is placed supine on the operating table, with the operative arm extended onto a radiolucent hand table to allow for unhindered fluoroscopic access. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field. Simultaneously, the ipsilateral iliac crest is prepped and draped; utilizing the ipsilateral side prevents the patient from experiencing bilateral extremity pain during the postoperative recovery phase. Intravenous prophylactic antibiotics are administered at least 30 minutes prior to tourniquet inflation. The surgical team is often divided, with one surgeon initiating the dorsal wrist exposure while an assistant simultaneously harvests the corticocancellous bone graft from the inner table of the ilium, thereby minimizing total tourniquet and operative time.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the dorsal compression plate technique demands meticulous attention to soft tissue handling and rigid biomechanical fixation. The procedure commences with a 10- to 15-cm longitudinal dorsal incision centered precisely over the radiocarpal joint, extending proximally from the distal third of the radius to the midshaft of the third metacarpal distally. As the dissection deepens through the subcutaneous tissue, the surgeon must carefully identify, mobilize, and protect the dorsal sensory branches of the radial nerve laterally and the dorsal branch of the ulnar nerve medially. Retraction of these nerves must be gentle to prevent postoperative neuromas. The extensor retinaculum is then exposed and incised over the third extensor compartment. The Extensor Pollicis Longus (EPL) tendon is mobilized from its sheath and transposed radially, completely removing it from the impending hardware footprint. The fourth compartment is subsequently elevated subperiosteally, and the finger extensors (EDC and EIP) are retracted ulnarly, providing wide exposure of the dorsal wrist capsule.
Once the capsule is exposed, an H-shaped or I-shaped incision is utilized to create robust proximal and distal capsular flaps. These flaps are meticulously elevated off the underlying carpal bones and distal radius, preserving their integrity for later closure. The radiocarpal, midcarpal, and carpometacarpal joints are now fully visualized. Joint preparation is arguably the most critical step in preventing pseudarthrosis. Using a combination of sharp osteotomes, rongeurs, and a high-speed burr under continuous saline irrigation, the surgeon meticulously denudes the articular cartilage from the radiocarpal joint, the capitolunate articulation, the scaphocapitate articulation, and the carpometacarpal (CMC) joint of the third ray. Decortication must proceed until healthy, bleeding subchondral bone is exposed—often referred to as the "paprika sign." It is imperative to avoid violating the CMC joints of the fourth and fifth rays; preserving ulnar CMC mobility is crucial for maintaining the transverse metacarpal arch, allowing the hand to cup around objects and facilitating a strong power grip.
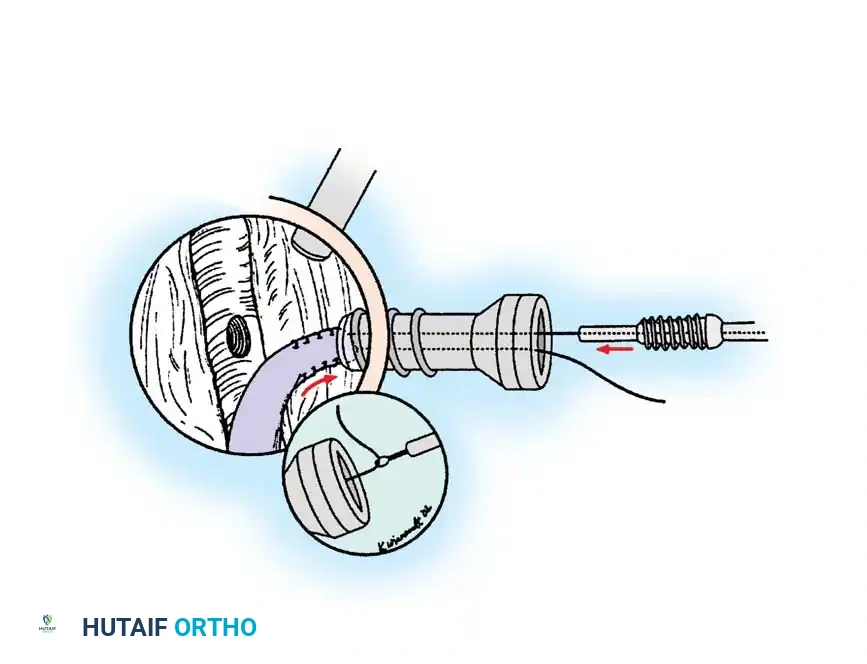
A defining maneuver in this specific technique is the placement of the radial styloid-capitate lag screw, designed to prevent ulnar translation of the carpus and subsequent DRUJ impingement. Prior to applying the dorsal plate, a 3.5-mm cortical lag screw is directed obliquely from the radial styloid into the body of the capitate. As this screw is tightened, it actively pulls the entire carpal mass radially, compressing it against the radial styloid. This maneuver effectively clears the ulnar side of the carpus away from the distal ulna, ensuring that the DRUJ remains unhindered and that forearm pronation and supination are preserved. Following this, a dorsal rectangular trough is prepared, spanning from the distal radius, across the denuded carpus, to the base of the third metacarpal. A flat, rectangular corticocancellous bone graft, previously harvested from the inner table of the iliac crest, is inlaid directly into this prepared bed. The cortical surface of the graft must sit flush with the dorsal cortex of the radius and metacarpal, providing a continuous, flat biomechanical surface for the compression plate.
Plate application and the induction of dynamic compression form the final phase of fixation. A seven-hole or eight-hole, 3.5-mm dynamic compression plate (DCP), or a dedicated pre-contoured wrist fusion plate, is selected and contoured to accommodate the desired 10 to 15 degrees of wrist extension. The plate is positioned directly over the inlaid corticocancellous graft, aligned strictly with the longitudinal axis of the radius and the third metacarpal. The compression sequence is critical: the first screw is inserted into the capitate to anchor the plate centrally. The second screw is placed into the distal radius utilizing the eccentric drilling technique within the dynamic compression hole; as this screw is seated, it shifts the plate proximally, forcefully compressing the radiocarpal joint against the inlaid graft. The distal end of the plate is then secured to the third metacarpal with two or three bicortical screws, ensuring maximum pull-out strength while avoiding excessive volar length that could irritate the intrinsic muscles. Finally, the proximal fixation is completed with additional screws into the radial diaphysis. The capsule is then meticulously closed over the plate using heavy absorbable sutures, providing a vital barrier to protect the extensor tendons, and the EPL is left transposed subcutaneously prior to routine skin closure.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates associated with the dorsal compression plate technique, total wrist arthrodesis is a major reconstructive procedure that carries a distinct profile of potential complications. Nonunion, or pseudarthrosis, is the most profound failure of the procedure, occurring in approximately 2% to 5% of cases. Risk factors for nonunion include patient non-compliance, active tobacco use, inadequate joint decortication, failure to utilize autologous bone graft, and insufficient rigid internal fixation. Nonunions most frequently occur at the third carpometacarpal joint or the radiocarpal articulation and typically present with persistent dorsal wrist pain, swelling, and hardware failure (screw breakage or plate pull-out). Diagnosis is confirmed via a fine-cut CT scan. Salvage management of a symptomatic nonunion requires a demanding revision surgery involving hardware removal, aggressive debridement of the fibrous nonunion site, massive structural corticocancellous grafting (often requiring a fresh iliac crest harvest or femoral head allograft), and rigid re-plating with a longer, more robust spanning construct.
Hardware-related complications and extensor tendon irritation represent the most common postoperative morbidities. Because the dorsal soft tissue envelope of the wrist is exceptionally thin, the bulky nature of a 3.5-mm DCP can cause significant prominence. If the surgeon fails to achieve a robust capsular closure over the plate, or if the distal metacarpal screws are left excessively long dorsally, the overlying extensor tendons (particularly the EDC and the transposed EPL) are subjected to continuous mechanical attrition. This can lead to severe tenosynovitis or frank tendon rupture. The incidence of symptomatic hardware requiring removal ranges from 10% to 20%. If a tendon rupture occurs, salvage management involves hardware removal (provided the fusion mass is solidly healed, typically after 12 to 18 months) and tendon transfer procedures, such as transferring the Extensor Indicis Proprius (EIP) to the ruptured EPL, to restore digital extension.
Distal Radioulnar Joint (DRUJ) impingement and adjacent joint osteoarthritis are biomechanical consequences of converting the wrist into a rigid segment. If the radial styloid-capitate lag screw is omitted or fails, the carpus may settle ulnarly, impinging against the distal ulna. This presents as painful, restricted forearm rotation. Furthermore, fusing the central column increases the lever arm and mechanical stress on the unfused carpometacarpal joints. If the fourth and fifth CMC joints were inadvertently violated or fused during the index procedure, the patient may develop severe ulnar-sided hand pain and lose the ability to cup the hand. Salvage for late DRUJ impingement typically necessitates a secondary Darrach or Sauvé-Kapandji procedure to unload the ulnar compartment. Management of painful
