Masterclass: Corrective Calcaneal Osteotomy & Subtalar Arthrodesis for Malunion

Key Takeaway
This masterclass guides fellows through calcaneal osteotomy and subtalar arthrodesis for malunited fractures. We cover intricate anatomy, meticulous preoperative planning, and a granular, real-time intraoperative execution. Learn precise instrument use, critical decision-making, and techniques to restore hindfoot alignment and function, addressing post-traumatic arthritis and impingement. Pearls for avoiding pitfalls and managing complications are also discussed.
Comprehensive Introduction and Patho-Epidemiology
The management of a calcaneal malunion represents one of the most formidable challenges in reconstructive foot and ankle surgery. A malunited calcaneal fracture is profoundly more complex than a simple skeletal deformity; it is a multi-planar derangement that completely alters the intricate biomechanics of the hindfoot. The initial trauma, typically a high-energy axial load, shatters the normal architecture of the calcaneus, particularly devastating the posterior facet and the lateral wall. When this complex fracture pattern is allowed to heal in a pathologic position—whether due to non-operative management, loss of fixation, or an initial failure to recognize the severity of the displacement—it initiates a relentless cascade of degenerative and mechanical problems.
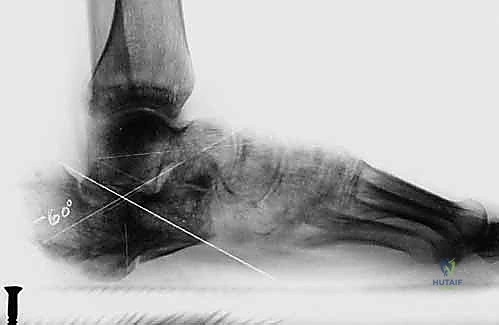
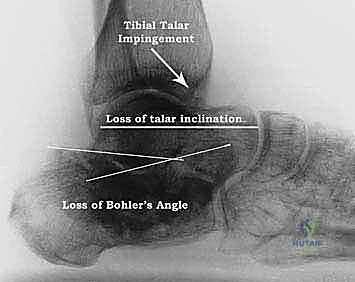
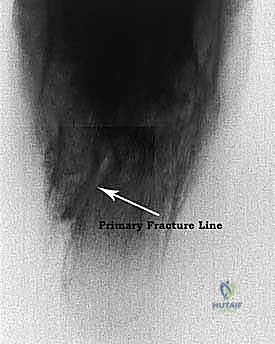
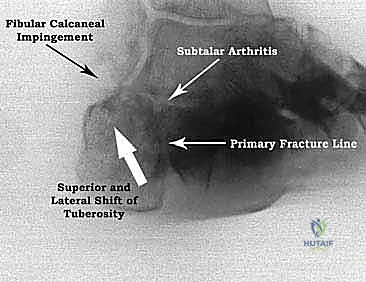
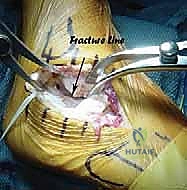
The patho-anatomy of a calcaneal malunion is classically characterized by a constellation of specific deformities: loss of calcaneal height, an increase in heel width, varus or valgus malalignment of the tuberosity, and profound incongruity of the subtalar joint. The primary fracture line often traverses the posterior facet, leading directly to posttraumatic subtalar arthritis, which is a primary generator of deep, aching hindfoot pain. Furthermore, the loss of calcaneal height—reflected by a flattened or reversed Böhler's angle—decreases the talar inclination angle. This horizontal positioning of the talus leads to anterior talotibial impingement during ankle dorsiflexion, severely restricting sagittal plane motion and causing anterior ankle pain.

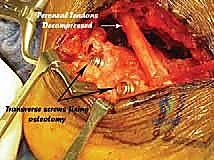
Simultaneously, the lateral wall of the calcaneus frequently "blows out" during the initial axial load. As this lateral expansion consolidates, it obliterates the normal fibular sulcus, leading to severe fibulocalcaneal impingement. The distal fibula abuts the expanded lateral calcaneal wall, mechanically trapping the peroneal tendons (longus and brevis) and the sural nerve. The displaced peroneal tendons are forced into a compressed, abnormal trajectory, precipitating chronic tenosynovitis, subluxation, and potentially longitudinal tears. Concurrently, the sural nerve is subjected to chronic friction and entrapment within the lateral scar tissue, resulting in debilitating neuropathic pain, dysesthesia, or profound hypoesthesia along the lateral border of the foot.

Epidemiologically, calcaneal fractures account for approximately 60% of all tarsal fractures, and despite advancements in open reduction and internal fixation (ORIF) and minimally invasive techniques, a significant subset of these injuries progresses to symptomatic malunion. The Stephens and Sanders classification system categorizes these malunions based on the presence of a lateral wall exostosis, subtalar arthritis, and varus/valgus malalignment, guiding our surgical decision-making. Type I malunions feature a lateral exostosis with a preserved subtalar joint; Type II involves a lateral exostosis with subtalar arthritis but no varus/valgus deformity; and Type III, the most severe, encompasses a lateral exostosis, subtalar arthritis, and a significant varus or valgus deformity of the calcaneal body. Today’s masterclass focuses on the definitive management of these complex Type II and Type III deformities via corrective calcaneal osteotomy combined with subtalar arthrodesis.

Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
A profound understanding of hindfoot osteology is the absolute prerequisite for executing a corrective osteotomy safely and effectively. The calcaneus is the largest tarsal bone, functioning as the primary lever arm for the Achilles tendon and the foundational weight-bearing structure of the heel. We must intimately understand the spatial relationships of the tuberosity, the posterior facet, the sustentaculum tali, and the anterior process. In a malunion, the Angle of Gissane—formed by the intersection of the downward slope of the posterior facet and the upward slope of the anterior process—is typically disrupted or blunted. Böhler's angle, normally between 20 and 40 degrees, is critically diminished, reflecting the collapse of the posterior facet and the proximal migration of the tuberosity.

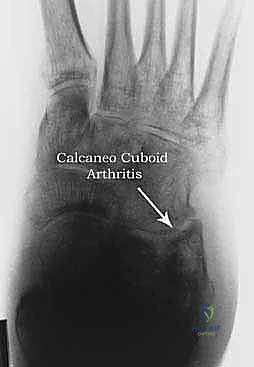
The talus, which sits atop the calcaneus to form the subtalar joint, dictates the translation of rotational forces from the leg into the foot. The loss of calcaneal height directly affects the talus, forcing it into a dorsiflexed (horizontal) position relative to the tibia. This not only causes the aforementioned anterior talotibial impingement but also fundamentally alters the mechanics of the transverse tarsal joint (Chopart's joint). The horizontal talus unlocks the talonavicular and calcaneocuboid joints, leading to midfoot hypermobility, arch collapse, and secondary degenerative changes across the midfoot over time.
Neurovascular and Soft Tissue Architecture
The surgical approach to the lateral hindfoot is fraught with neurovascular landmines. The sural nerve is our primary structure of concern on the lateral aspect. Originating from the tibial and common peroneal nerves, it courses posterior to the lateral malleolus and runs anteriorly along the lateral aspect of the foot. In the setting of a lateral wall blowout, the normal fat pad protecting the nerve is obliterated, and the nerve is often encased in dense, unyielding scar tissue directly overlying the bony prominence. Meticulous, sharp dissection is required to mobilize and protect this nerve; aggressive retraction will inevitably lead to a devastating traction neuritis.
Deep to the sural nerve lie the peroneal tendons within their retinacular sheath. The expanded lateral wall pushes these tendons laterally and superiorly against the fibula. The surgeon must carefully incise the superior peroneal retinaculum to mobilize the tendons, inspecting them thoroughly for longitudinal splits or severe tendinosis, which may require concomitant debridement or tubularization. Medially, the posterior tibial neurovascular bundle (comprising the posterior tibial artery, tibial nerve, and posterior tibial vein) represents the ultimate danger zone. When performing the medial completion of the calcaneal osteotomy, the saw blade or osteotome must exit the medial cortex strictly posterior and inferior to the sustentaculum tali to avoid catastrophic injury to these critical structures.

Ligamentous Constraints and Subtalar Stability
The intrinsic stability of the hindfoot relies heavily on the robust ligamentous complexes within the sinus tarsi and tarsal canal. The interosseous talocalcaneal ligament and the cervical ligament are the primary stabilizers of the subtalar joint. A critical surgical pearl during the preparation for an in-situ or corrective fusion is the preservation of these interosseous ligaments whenever possible. The raw text correctly highlights: "Do not incise the interosseous ligaments if possible, as these will help stabilize the sustentacular fragment to the talus."

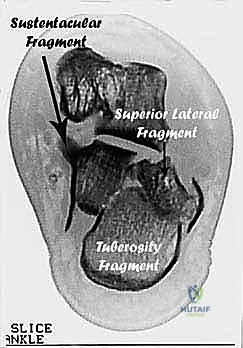
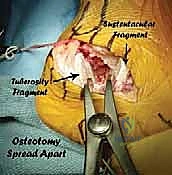
The sustentacular fragment (the anteromedial portion of the calcaneus) is strongly tethered to the talus by the deltoid ligament complex and the interosseous ligaments. Because this fragment rarely displaces significantly during the initial fracture, it serves as our anatomically constant "anchor." By preserving the interosseous ligaments, we maintain this vital connection, utilizing the stable talus-sustentaculum complex as the foundation against which we will translate and fix the mobilized calcaneal tuberosity. Conversely, the fibulocalcaneal ligament laterally is often contracted and scarred due to the impingement; this ligament must be systematically released to allow for adequate mobilization of the subtalar joint and correction of the varus/valgus deformity.
Exhaustive Indications and Contraindications
The decision to proceed with a corrective calcaneal osteotomy and subtalar arthrodesis is not to be taken lightly. This is a major reconstructive procedure with a steep learning curve and a significant complication profile. The primary indication is a patient presenting with a painful, mature calcaneal malunion that has failed exhaustive conservative management (including custom orthotics, bracing, physical therapy, and targeted corticosteroid injections). The pain must be clearly localized to the subtalar joint (indicating arthritis) and/or the lateral fibulocalcaneal interval (indicating impingement).
A thorough assessment of the deformity's magnitude dictates the exact procedure. A simple in-situ subtalar arthrodesis is reserved strictly for Stephens and Sanders Type II malunions where the primary issue is isolated subtalar arthritis without significant loss of height or severe axial plane deformity. However, for Type III malunions—characterized by profound loss of calcaneal height, severe varus or valgus of the tuberosity, and unyielding anterior talotibial impingement—a corrective osteotomy (often a Romash-type sliding osteotomy or a bone-block distraction arthrodesis) is absolutely mandatory. Fusing the subtalar joint in situ in the presence of a severe multi-planar deformity will fail to address the anterior impingement, the lever-arm dysfunction of the Achilles, and the altered midfoot biomechanics, ultimately leading to a poor clinical outcome.
Contraindications must be rigorously respected. Active infection, whether superficial or deep, is an absolute contraindication; any suspicion of osteomyelitis must be aggressively worked up and treated prior to considering reconstruction. Severe peripheral arterial disease (PAD) is another absolute contraindication, as the extensile lateral approach requires robust soft tissue perfusion for healing; non-invasive vascular studies (ABIs, TCOMs) are mandatory in any patient with a history of smoking, diabetes, or absent palpable pulses. Relative contraindications include profound uncontrolled diabetes, active smoking (which exponentially increases the risk of wound necrosis and nonunion), and severe psychiatric or cognitive disorders that preclude strict adherence to the demanding non-weight-bearing postoperative protocol.
| Category | Indications for Corrective Osteotomy & Fusion | Absolute / Relative Contraindications |
|---|---|---|
| Clinical | Intractable hindfoot pain failing 6+ months of conservative care. | Active local or systemic infection (Absolute). |
| Mechanical | Severe lateral fibulocalcaneal impingement with peroneal entrapment. | Severe peripheral arterial disease / ischemia (Absolute). |
| Anatomic | Loss of calcaneal height with anterior talotibial impingement. | Active, heavy tobacco use (Relative - high risk of flap necrosis). |
| Radiographic | Stephens & Sanders Type III (Arthritis + Varus/Valgus + Impingement). | Charcot neuroarthropathy of the hindfoot (Relative - requires modified approach). |
| Functional | Achilles lever-arm dysfunction due to proximal tuberosity migration. | Medical non-compliance or inability to remain non-weight-bearing (Absolute). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Radiographic Assessment
Thorough preoperative planning is the blueprint for surgical success; improvising during a calcaneal reconstruction is a recipe for disaster. The clinical examination must be exhaustive. The surgeon should evaluate the patient standing, noting the alignment of the hindfoot (varus or valgus) and the presence of a widened heel. A critical diagnostic maneuver is palpating for the "fibular sulcus" just distal to the lateral malleolus. In a healthy ankle, there is a distinct indentation; in a malunion with lateral wall blowout, this sulcus is completely obliterated, replaced by a hard, bony prominence. The surgeon must also assess ankle dorsiflexion (often limited by talar impingement) and carefully map out the sensory distribution of the sural nerve, documenting any preoperative deficits.
Standard plain radiography includes weight-bearing AP, lateral, and axial heel views of both feet. The unaffected foot provides the essential template for anatomical restoration. On the lateral view, we meticulously measure Böhler's angle, the angle of Gissane, and the talar inclination angle, assessing the degree of anterior tibial impingement. The axial view confirms the varus/valgus alignment of the tuberosity and the extent of the lateral wall expansion. Broden views (internal rotation views at varying degrees of cephalad angulation) are exceptionally useful for evaluating the posterior facet incongruity and the precise location of the fibulocalcaneal impingement.
Advanced Imaging and Surgical Templating
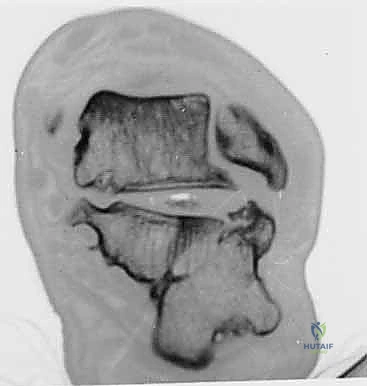
While plain films provide the foundation, a fine-cut Computed Tomography (CT) scan with multi-planar reconstructions (axial, coronal, sagittal, and 3D volumetric) is the undisputed gold standard and an absolute requirement for preoperative planning. The CT scan provides a high-fidelity, three-dimensional roadmap of the internal architecture. It allows the surgeon to precisely quantify the degree of subtalar arthritis, the exact volume of the lateral wall exostosis, and the precise location of the primary oblique fracture line. Crucially, the coronal sequences definitively demonstrate the relationship between the fibula, the peroneal tendons, and the lateral calcaneal wall, confirming the mechanical impingement.

Surgical templating is performed using the CT and lateral radiographs. If a bone-block distraction arthrodesis is planned, the surgeon must calculate the exact height of the structural graft required to restore the talar inclination angle and decompress the anterior ankle. If a Romash-type sliding osteotomy is chosen, the angle and trajectory of the osteotomy cut must be templated to ensure that sliding the tuberosity fragment distally and inferiorly will simultaneously restore heel height, correct the varus/valgus malalignment, and tension the Achilles tendon appropriately. This mathematical precision minimizes intraoperative guesswork.
Patient Positioning and Operating Room Setup
Proper patient positioning is critical for optimal exposure and fluoroscopic access. The patient is typically placed in the lateral decubitus position on a radiolucent operative table, utilizing a vacuum bean bag for rigid stabilization. The operative leg is padded meticulously, ensuring all bony prominences (especially the contralateral common peroneal nerve) are protected. A high-thigh pneumatic tourniquet is applied.
The fluoroscopy unit (C-arm) must be positioned to allow unhindered, orthogonal views of the hindfoot (AP, lateral, and axial) without requiring the surgeon to constantly readjust the leg. The monitor should be placed directly in the surgeon's line of sight. Prior to prepping and draping, a "dry run" with the C-arm is mandatory to confirm that perfect lateral and axial views can be obtained effortlessly. The leg is then prepped and draped in standard sterile fashion, ensuring the drape extends proximal to the knee to allow for assessment of rotational alignment during the reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
The Extensile Lateral Approach and Soft Tissue Management
The procedure begins with an extensile lateral approach, heavily modified based on the presence of prior surgical scars. The classic L-shaped incision is utilized, starting vertically just lateral to the Achilles tendon, curving smoothly at the junction of the plantar and lateral skin, and extending anteriorly toward the calcaneocuboid joint. This creates a full-thickness fasciocutaneous flap. The absolute priority during the initial dissection is the identification and protection of the sural nerve. The nerve is often encased in dense scar tissue directly overlying the lateral wall blowout; it must be meticulously neurolysed and retracted gently with the flap.
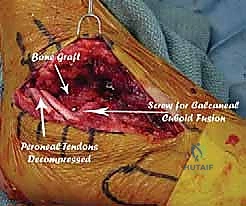
Once the flap is elevated, the peroneal sheath is identified. The superior peroneal retinaculum is carefully incised, and the peroneal tendons (longus and brevis) are mobilized. They are frequently flattened, frayed, or subluxated due to the underlying bony prominence. The tendons are retracted anteriorly and superiorly, exposing the massive lateral wall exostosis. Using a broad osteotome or an oscillating saw, the lateral wall exostosis is radically resected. This step is therapeutic in two ways: it immediately decompresses the fibulocalcaneal impingement space, and it provides a rich source of autologous cancellous bone graft that will be utilized later in the arthrodesis.

Joint Preparation and the Corrective Osteotomy
With the lateral wall decompressed, the subtalar joint is fully exposed. A lamina spreader is inserted into the posterior facet to distract the joint. All remaining articular cartilage and dense subchondral sclerotic bone down to bleeding cancellous bone must be meticulously removed using sharp curettes, osteotomes, and a high-speed burr. The preparation must extend into the middle and anterior facets if they are involved. Crucially, as emphasized previously, the interosseous ligaments in the sinus tarsi should be preserved if possible to maintain the stable relationship between the talus and the sustentacular fragment.
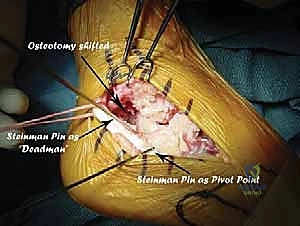
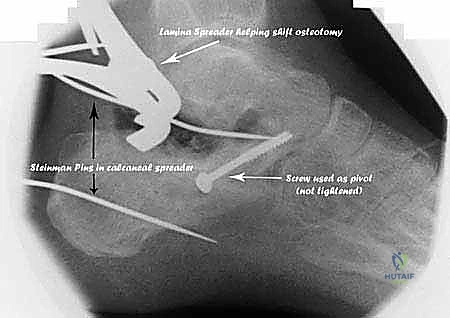
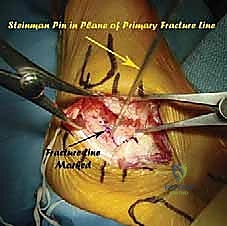
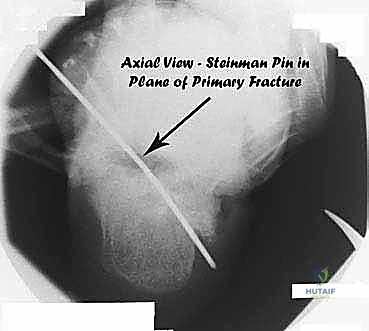
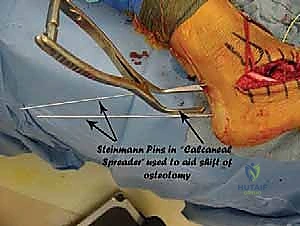
The corrective osteotomy is then executed. For a severe Type III malunion, an osteotomy that mimics the primary fracture line is often required. An oscillating saw is used to create an oblique cut starting posterior to the posterior facet and exiting inferiorly, completely freeing the malunited tuberosity fragment. Extreme caution is exercised as the saw blade approaches the medial cortex to avoid plunging into the posterior tibial neurovascular bundle. Once the osteotomy is complete, a large distractor or a specialized lamina spreader is utilized to translate the tuberosity fragment distally, inferiorly, and out of varus/valgus. This complex multi-planar translation restores calcaneal height, corrects the talar inclination angle, and eliminates anterior talotibial impingement.
Structural Grafting and Rigid Internal Fixation
The translation of the tuberosity creates a substantial bony void within the subtalar joint and the osteotomy site. This void must be filled with structural bone graft to maintain the correction and facilitate arthrodesis. A tricortical iliac crest autograft or a robust structural allograft (such as a femoral head or specifically milled calcaneal wedge) is precisely contoured and impacted into the distracted space. The previously harvested autograft from the lateral wall exostectomy is packed tightly into all remaining interstices to maximize the osteogenic potential of the construct.

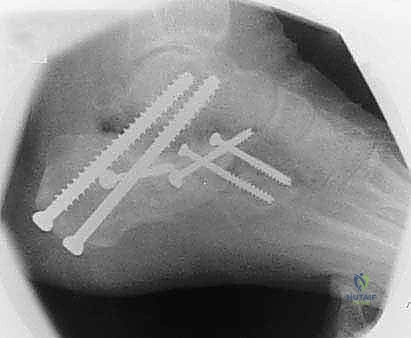
Rigid internal fixation is paramount. Provisional fixation is achieved with heavy threaded Kirschner wires, and the overall alignment is rigorously verified under multi-planar fluoroscopy. Definitive fixation typically involves two or three large-diameter (6.5mm or 7.3mm) partially threaded cannulated screws. These are placed from the posterior non-weight-bearing aspect of the
Clinical & Radiographic Imaging Archive