Mastering Calcaneal Malunions: Advanced Techniques in Subtalar and Triple Arthrodesis
Key Takeaway
Calcaneal malunions frequently cause chronic pain and severe disability due to altered hindfoot biomechanics, loss of heel height, and subtalar arthritis. Surgical management ranges from lateral exostectomy to complex subtalar distraction realignment arthrodesis and reconstructive osteotomies. This guide provides an evidence-based, step-by-step approach to evaluating and treating calcaneal malunions, emphasizing precise patient selection, structural grafting techniques, and complication avoidance to restore optimal foot kinematics.
Comprehensive Introduction and Patho-Epidemiology
Pain and severe disability frequently persist following fractures of the calcaneus, even when the initial injury was managed with skillful operative or nonoperative techniques. This chronic morbidity is especially pronounced in patients whose occupations require ambulation over uneven or rough terrain, heavy lifting, or prolonged standing. The pathoanatomy of a calcaneal malunion is exceedingly complex and multi-planar, typically characterized by a profound loss of calcaneal height, increased heel width, varus deformity of the calcaneal tuberosity, and severe derangement of the subtalar joint kinematics. When intra-articular fractures heal in a displaced position, the resulting incongruity inevitably leads to rapid, post-traumatic subtalar osteoarthritis, which serves as the primary pain generator for the majority of these patients.
Deformities associated with the nonoperative management of displaced intra-articular calcaneal fractures, or those following failed open reduction and internal fixation (ORIF), lead to a predictable and devastating cascade of biomechanical failures. The loss of heel height directly decreases the talocalcaneal angle (talar inclination), resulting in a horizontal orientation of the talus within the ankle mortise. This horizontal talus causes rigid anterior ankle impingement, mechanically restricting dorsiflexion as the talar neck abuts the anterior lip of the distal tibia. Concurrently, the lateral wall blowout—a hallmark of axial load calcaneal injuries—creates a massive bony exostosis that impinges upon the lateral malleolus and the intervening peroneal tendons, a condition known as subfibular impingement.
The epidemiological burden of calcaneal malunions remains significant despite advancements in primary fracture care. Historically, a large subset of these injuries was managed nonoperatively, leading to a high incidence of late reconstructive presentations. Today, while operative intervention is more common, malunions still occur due to initial comminution, loss of fixation, patient non-compliance, or delayed presentations. The socioeconomic impact is staggering, as the typical demographic involves working-age males who sustain high-energy trauma, such as falls from a height or motor vehicle collisions. The resulting chronic pain, altered gait mechanics, and inability to accommodate standard footwear often preclude a return to pre-injury employment levels.
Clinical Pearl: When evaluating a patient with a calcaneal malunion, carefully assess ankle dorsiflexion. A horizontal talus secondary to loss of calcaneal height will mechanically block the anterior distal tibia, limiting dorsiflexion to less than 10 degrees. This is a primary indication for a distraction bone-block arthrodesis rather than an in situ fusion, as restoring the talar declination angle is the only way to resolve the anterior impingement and restore functional ankle kinematics.
Detailed Surgical Anatomy and Biomechanics
A masterful understanding of hindfoot anatomy and biomechanics is an absolute prerequisite for tackling the reconstructive challenges of a calcaneal malunion. The subtalar (talocalcaneal) joint is a complex, tri-planar articulation consisting of three distinct facets: the posterior, middle, and anterior facets. The posterior facet is the largest and bears the majority of the axial load transferred from the tibia through the talus. In a calcaneal fracture, the primary fracture line typically splits the posterior facet, driving the lateral articular fragment inferiorly into the cancellous body of the calcaneus. The middle facet is supported by the sustentaculum tali, a dense cortical medial projection that often remains anatomically tethered to the talus via the robust deltoid and talocalcaneal ligaments, making it a critical constant landmark during surgical reconstruction.
The kinematics of the subtalar joint are best conceptualized as a mitered hinge, dictating the coupled motion of the hindfoot and midfoot. During normal gait, subtalar eversion unlocks the transverse tarsal joints (talonavicular and calcaneocuboid), allowing the midfoot to become flexible for shock absorption during the heel-strike phase. Conversely, subtalar inversion locks the transverse tarsal joints, converting the foot into a rigid lever arm necessary for effective propulsion during the toe-off phase. In a calcaneal malunion with post-traumatic arthritis, this intricate coupling is destroyed. The hindfoot is often locked in a varus position, forcing the midfoot into a rigid, supinated posture that prevents normal shock absorption and drastically alters the plantar pressure distribution, frequently leading to lateral column overload and secondary midfoot arthritis.
The lateral wall of the calcaneus is a critical anatomical zone in the context of malunions. The lateral wall is composed of thin cortical bone that invariably blows out laterally during the initial axial compression injury. As this blowout consolidates, it forms a dense, malunited exostosis that encroaches upon the subfibular space. The peroneal tendons (brevis and longus), which normally glide smoothly posterior and inferior to the lateral malleolus, become compressed, subluxated, or severely tenosynovitic against this exostosis. Furthermore, the sural nerve, which courses along the lateral hindfoot, is highly susceptible to entrapment within the post-traumatic scar tissue or direct compression by the expanded lateral wall, leading to debilitating neuropathic pain.
The Achilles tendon and the triceps surae complex are also profoundly affected by the altered biomechanics of a calcaneal malunion. The calcaneal tuberosity acts as the lever arm for the Achilles tendon. When calcaneal height is lost and the tuberosity is displaced superiorly and anteriorly, the effective lever arm is drastically shortened. This results in a significant loss of plantarflexion power, clinically manifesting as an inability to perform a single-leg heel raise and a visibly weakened push-off during the gait cycle. Restoring the anatomical length and height of the calcaneus through reconstructive osteotomy or distraction arthrodesis is therefore essential not only for joint realignment but also for restoring the physiological tension and mechanical advantage of the Achilles-gastrocnemius-soleus complex.
Exhaustive Indications and Contraindications
The decision to proceed with surgical reconstruction of a calcaneal malunion must be carefully weighed against the patient's symptoms, functional demands, and medical comorbidities. The primary indication for surgical intervention is intractable, localized hindfoot pain that has failed exhaustive nonoperative management, including custom orthoses, rigid ankle-foot orthoses (AFOs), non-steroidal anti-inflammatory drugs (NSAIDs), and targeted corticosteroid injections. Patients typically present with a combination of lateral subfibular impingement pain, deep subtalar joint pain secondary to post-traumatic osteoarthritis, and anterior ankle pain due to talotibial impingement.
The specific surgical procedure chosen—whether an in situ subtalar arthrodesis, a bone-block distraction arthrodesis, a reconstructive osteotomy, or a triple arthrodesis—depends entirely on the morphological characteristics of the malunion. In situ subtalar fusion is indicated for patients with isolated subtalar arthritis who have maintained adequate heel height, possess a relatively normal talar declination angle, and exhibit no signs of anterior ankle impingement. Bone-block distraction arthrodesis is strictly indicated when there is a profound loss of calcaneal height resulting in a horizontal talus and a mechanical block to ankle dorsiflexion. Triple arthrodesis is reserved for cases where the severe initial trauma has led to concurrent, symptomatic osteoarthritis or subluxation of the talonavicular and calcaneocuboid joints.
Contraindications to calcaneal malunion reconstruction must be rigorously respected to avoid catastrophic complications. Active infection, whether localized to the hindfoot or systemic, is an absolute contraindication to any reconstructive arthrodesis. Severe peripheral vascular disease (PVD) is another absolute contraindication; the tenuous soft tissue envelope of the hindfoot will reliably fail to heal in the presence of inadequate arterial inflow. Charcot neuroarthropathy, particularly in the acute or subacute inflammatory phases, precludes standard arthrodesis techniques due to the high risk of catastrophic implant failure and progressive bone resorption.
Smoking and tobacco use represent the most significant modifiable relative contraindications in hindfoot reconstructive surgery. The vasoconstrictive effects of nicotine, combined with the cellular toxicity of carbon monoxide, drastically impair osteogenesis and angiogenesis. High nonunion rates and residual lateral pain (present in up to 64% of patients) are heavily correlated with tobacco use. Many academic orthopedic surgeons mandate strict smoking cessation, confirmed by negative serum or urine cotinine levels, for a minimum of six weeks prior to and three months following any complex hindfoot arthrodesis.
| Parameter | Indications | Contraindications |
|---|---|---|
| In Situ Subtalar Arthrodesis | Isolated subtalar OA, preserved heel height, normal talar declination, neutral hindfoot alignment. | Severe anterior ankle impingement, profound loss of calcaneal height, active infection. |
| Distraction Bone-Block Arthrodesis | Severe loss of heel height, horizontal talus, anterior ankle impingement (<10° dorsiflexion), subtalar OA. | Inadequate soft tissue envelope, severe PVD, active smoking (relative/absolute depending on surgeon). |
| Reconstructive Osteotomy (Romash) | Severe varus malalignment of the tuberosity, lateral impingement, loss of height requiring multi-planar correction. | Poor bone stock, advanced age with low functional demand, Charcot neuroarthropathy. |
| Triple Arthrodesis | Subtalar OA combined with symptomatic talonavicular and calcaneocuboid OA or structural midfoot subluxation. | Isolated subtalar disease, normal midtarsal joint function, active osteomyelitis. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful calcaneal malunion reconstruction. The clinical evaluation must be exhaustive. The surgeon must assess the patient's gait, noting any antalgic features, lack of push-off, or varus thrust. The hindfoot alignment should be evaluated from behind while the patient is weight-bearing; a varus malalignment of the heel is a common and functionally devastating deformity that must be corrected to prevent lateral column overload. Range of motion of the ankle, subtalar, and midtarsal joints must be documented. Crucially, ankle dorsiflexion must be tested with the knee both extended and flexed to differentiate between gastrocnemius tightness and a hard, bony anterior impingement block caused by a horizontal talus. The subfibular space must be palpated to assess for exostosis prominence, peroneal tendon subluxation, and sural nerve irritability (Tinel's sign).
Radiographic evaluation begins with standard weight-bearing views of the foot and ankle, including anteroposterior (AP), lateral, and mortise views, as well as a Harris axial heel view. On the lateral radiograph, the surgeon must measure Böhler's angle and the angle of Gissane, both of which are typically depressed or obliterated in a malunion. The talar declination angle (talocalcaneal angle) must be assessed; a normal angle is approximately 20 to 30 degrees, whereas a horizontal talus will approach 0 degrees. The Harris heel view is critical for evaluating the varus or valgus alignment of the calcaneal tuberosity and the extent of the lateral wall blowout. Contralateral, normal foot radiographs should always be obtained to serve as an anatomical template for restoring height and alignment.
Advanced imaging with a high-resolution Computed Tomography (CT) scan is absolutely mandatory for all calcaneal malunions. The CT scan provides a three-dimensional understanding of the deformity, the status of the subtalar and midtarsal articular cartilage, and the exact volume of the lateral wall exostosis. Surgical decision-making is heavily guided by the structural morphology of the malunion as seen on CT. The Stephens and Sanders CT Classification provides a prognostic framework based on the presence of lateral wall exostosis, subtalar arthritis, and hindfoot alignment.
Type I Malunion
Characterized by a large lateral wall exostosis with an intact, relatively normal subtalar joint. Patients primarily present with subfibular impingement and peroneal tendinopathy.

Type II Malunion
Characterized by a large lateral wall exostosis combined with significant post-traumatic subtalar arthritis. The hindfoot alignment remains relatively neutral.

Type III Malunion
The most severe form, characterized by a lateral exostosis, significant subtalar arthritis, and a calcaneal body malalignment of more than 10 degrees of hindfoot varus.
Patient positioning is critical for optimizing surgical exposure and facilitating fluoroscopic imaging. For isolated subtalar arthrodesis, lateral exostectomy, or distraction bone-block procedures, the patient is typically placed in the lateral decubitus position on a radiolucent beanbag. All bony prominences must be meticulously padded. A high-thigh tourniquet is applied to provide a bloodless surgical field. The contralateral leg is flexed at the hip and knee and padded away from the operative field to allow unimpeded lateral fluoroscopic imaging. The C-arm should be brought in from the anterior aspect of the patient, allowing the surgeon to obtain perfect lateral, AP, and Harris axial views without manipulating the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The Posterolateral Approach
For complex malunions requiring subtalar arthrodesis, the posterolateral approach offers distinct advantages over traditional extensile lateral or Gallie-type posterior approaches. The incision is placed longitudinally, just anterior to the Achilles tendon and posterior to the peroneal tendons. The benefits include minimization of soft tissue dissection and devascularization, which is critical in a foot that has already suffered significant trauma. It provides excellent, direct visualization of the posterior facet of the subtalar joint and allows easier access to the medial subtalar capsule and the sustentaculum tali, facilitating the medial releases necessary for deformity correction. Furthermore, this approach significantly decreases the risk of iatrogenic damage to the sural nerve, which is often encased in scar tissue more anteriorly.
Lateral Exostectomy and Joint Preparation
Regardless of the specific arthrodesis technique, addressing the lateral wall blowout is mandatory. Through the posterolateral approach, the sural nerve is identified and protected. The peroneal tendons are retracted anteriorly. The massive lateral exostosis is identified; it often abuts the tip of the fibula. Using an osteotome or a sagittal saw, a radical lateral exostectomy is performed to completely decompress the subfibular space. The resected cortical and cancellous bone should be carefully preserved and morselized for later use as local autograft. Following the exostectomy, a thorough medial, posterior, and lateral subtalar capsulotomy is performed to mobilize the joint. All remaining articular cartilage and fibrous scar tissue must be denuded from the posterior facet using curettes and osteotomes, exposing healthy, bleeding subchondral bone.
Subtalar Distraction Realignment Arthrodesis
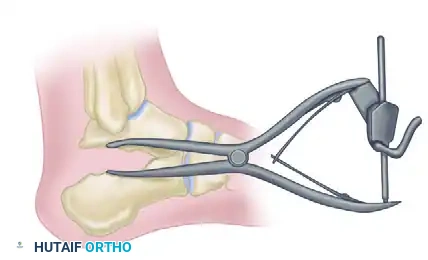
Distraction arthrodesis is strictly indicated for patients with disabling pain, severe loss of heel height, and less than 10 degrees of ankle dorsiflexion due to anterior impingement. Once the joint is prepared and mobilized, a laminar spreader is inserted into the posterior aspect of the subtalar joint. The surgeon carefully and progressively distracts the joint to restore calcaneal height, correct the varus deformity, and, most importantly, restore the talar inclination angle to relieve anterior impingement.

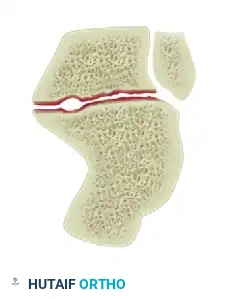
While the joint is held in distraction, a structural tricortical autograft is harvested, typically from the ipsilateral anterior iliac crest. The graft is meticulously shaped into a tapered wedge to match the created defect. The anterior wedge bone graft is inserted into the distracted joint space to maintain the corrected height and alignment.
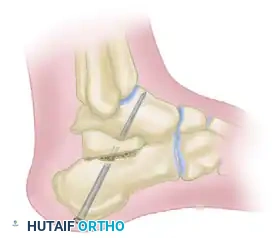
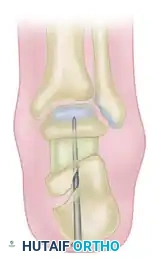
Rigid fixation is paramount. The arthrodesis and the structural graft are secured using two or three large-diameter (7.3 mm or 8.0 mm) cannulated titanium screws. The guide pins are directed from the posteroinferior aspect of the calcaneal tuberosity, aiming anteriorly, superiorly, and slightly medially into the dense bone of the talar body and neck. A strict lag technique must be utilized to achieve maximal compression across the graft interfaces.
Reconstructive Osteotomy (Romash Technique)
Romash described a highly effective reconstructive osteotomy of the calcaneus combined with subtalar arthrodesis for severe malunions characterized by profound varus and shortening. This technique essentially re-creates the primary fracture line through the calcaneal body. By mobilizing the osteotomy, the surgeon can reposition the calcaneal tuberosity medially to narrow the heel, alleviate lateral impingement, and translate the tuberosity inferiorly to return height to the heel. The concurrent subtalar arthrodesis definitively addresses the post-traumatic arthritis. This technique requires extensive soft tissue release and is technically demanding, but it offers powerful multi-planar correction without the need for massive structural grafts.
The Gallie Subtalar Fusion Technique
The Gallie technique is a classic posterior approach to subtalar fusion, utilizing a mortise and tenon structural grafting concept. While less commonly used today for complex malunions requiring multi-planar correction (as it does not easily allow for massive distraction or varus/valgus correction), it remains a biomechanically sound method for in situ fusion where robust structural stability is required.
The skin incision is placed just lateral to the tendo calcaneus, extending distally toward the calcaneal tuberosity.

The posterior aspect of the subtalar joint is identified. Using a sharp osteotome, the surgeon removes a rectangular mortise of bone spanning directly across the subtalar joint, removing the posterior articular surfaces.

This mortise is extended deep into the joint, reaching through to the transverse sinus (sinus tarsi) to ensure adequate depth for the graft.

A robust, rectangular block of cortical-cancellous bone is then harvested from the anteromedial surface of the proximal tibia.

The tibial graft is carefully prepared and contoured on the back table to perfectly match the dimensions of the created subtalar mortise.

The structural graft is carefully impacted into the subtalar mortise. The cortical face of the graft provides immediate structural stability against shear forces, while the cancellous portion promotes rapid osteointegration.
If necessary, the graft can be divided in two to fill the medial and lateral aspects of the mortise more precisely, ensuring maximum bone-to-bone contact and preventing any rotational instability.

Triple Arthrodesis: Indications and Controversies
If the midtarsal joints (talonavicular and calcaneocuboid) are arthritic or structurally involved in the malunion, a triple arthrodesis is advisable. For a severe crushing fracture of the calcaneus—whether fresh or malunited—triple arthrodesis has historically been recommended. In these catastrophic injuries, there is not only complete derangement of the subtalar joint but also subluxation of the calcaneocuboid and talonavicular joints caused by the severe depression of the sustentaculum tali.
Biomechanical Principle: With subtalar fusion alone in the presence of a depressed sustentaculum tali, the head and neck of the talus are left projecting forward without medial support. This creates a constant, pathologic lever arm during weight-bearing that places immense stress on the midfoot and actively interferes with subtalar fusion consolidation.
According to Conn, triple arthrodesis is preferable to isolated subtalar fusion in these severe cases because the talonavicular, calcaneocuboid, and subtalar joints function with a reciprocal, coupled action. Fusing all three does not significantly add to the patient's clinical disability, as little functional midtarsal motion remains after the original crushing injury. However, modern orthopedic consensus dictates a more joint-preserving approach. Many surgeons believe that triple arthrodesis offers no functional advantage in the majority of patients with standard calcaneal malunions. Current Recommendation: Unless the midtarsal joints are overtly arthritic or structurally compromised by the malunion, arthrodesis should be strictly limited to the subtalar joint. Motion in the midtarsal joints may actually increase compensatorily with activity post-fusion and should be meticulously preserved whenever possible.
Complications, Incidence Rates, and Salvage Management
The surgical reconstruction of calcaneal malunions is fraught with potential complications, demanding meticulous surgical technique and strict patient compliance. The most devastating complication is nonunion of the arthrodesis site. The subtalar joint is notoriously difficult to fuse due to its complex contours and the immense shear forces it experiences during weight-bearing.
Surgical Warning: Trnka et al. reported an alarming 29 complications following subtalar bone block arthrodesis. Notably, four out of the five nonunions in their series occurred in patients where structural allografts were utilized. The use of bulk allograft in calcaneal malunion reconstruction is strongly cautioned against. Autologous structural graft (e.g., tricortical iliac crest) remains the gold standard, providing essential osteoinductive and osteogenic properties that allografts lack.
Malunion or residual deformity is another significant risk. Failure to adequately correct the varus alignment of the calcaneal tuberosity will result in persistent lateral column overload, leading to chronic lateral foot pain, recurrent peroneal tendinopathy, and eventual breakdown of the fifth metatarsal base. Intraoperative fluoroscopy must be utilized obsessively to confirm neutral to slight valgus alignment of
