Calcaneal Lengthening Osteotomy: A Masterclass in Hindfoot Valgus Correction
Key Takeaway
Step into the operating theater for a masterclass on calcaneal lengthening osteotomy. This guide covers the intricate anatomy of hindfoot valgus, meticulous preoperative planning, and precise intraoperative execution. We'll explore critical surgical steps, instrument use, and real-time decision-making, emphasizing neurovascular protection. Learn to identify and manage potential pitfalls, ensuring optimal patient outcomes through detailed postoperative rehabilitation protocols.
Comprehensive Introduction and Patho-Epidemiology
The calcaneal lengthening osteotomy, classically pioneered by David Evans and subsequently refined by Vincent Mosca, represents a cornerstone in the surgical armamentarium for the correction of severe, symptomatic flexible flatfoot deformities. This intervention is not merely a structural bone cut; it is a profound biomechanical realignment procedure designed to restore the intricate kinematics of the hindfoot and midfoot. By strategically lengthening the lateral column of the foot, the surgeon effectively levers the midtarsal joint back into an anatomic alignment, thereby reducing the peritalar subluxation that characterizes the flatfoot complex. Mastery of this procedure requires an intimate understanding of triplanar foot biomechanics, meticulous surgical technique, and rigorous patient selection.



To fully appreciate the utility of the calcaneal lengthening osteotomy, one must first deconstruct the underlying pathology of the flatfoot, or pes planovalgus. Surgically, we recognize this not as a simple loss of the medial longitudinal arch, but as a complex, multiplanar deformity centered around the talus. The calcaneus deviates laterally into severe valgus, pushing the subtalar joint into obligate eversion. Concurrently, the midfoot sags, characterized by a plantarflexed talus and a dorsolaterally subluxated navicular. The forefoot subsequently supinates to maintain plantigrade contact with the floor, and the entire foot externally rotates relative to the tibia, manifesting clinically as an out-toeing gait and a positive thigh-foot angle.
The concept of the "acetabulum pedis," originally coined by Scarpa, is paramount to understanding this deformity. The acetabulum pedis is the functional articular socket formed by the concave proximal articular surface of the navicular, the spring ligament complex (plantar calcaneonavicular ligament), and the anterior articular facet of the calcaneus. In the normal foot, this socket elegantly cups the talar head. In the flatfoot deformity, the acetabulum pedis externally rotates and everts away from the talar head, leading to profound loss of medial column support. The calcaneal lengthening osteotomy directly addresses this by essentially rotating the acetabulum pedis back medially and dorsally over the talar head, utilizing the intact medial soft tissue hinge.
Epidemiologically, this procedure is most frequently indicated in the pediatric and adolescent population presenting with symptomatic, recalcitrant flexible pes planovalgus, often associated with a short Achilles tendon. However, its utility extends significantly into the adult realm, particularly in the management of Stage IIb Adult Acquired Flatfoot Deformity (AAFD) secondary to posterior tibial tendon dysfunction (PTTD). In these adult cases, the lateral column shortening is a critical component of the deformity that must be addressed to protect medial soft-tissue reconstructions. Regardless of the patient's age, the fundamental biomechanical goal remains identical: to restore the relative lengths of the medial and lateral columns, thereby achieving a stable, plantigrade, and functional foot.
Detailed Surgical Anatomy and Biomechanics
Subtalar Joint Kinematics
The subtalar (talocalcaneal) joint is an anatomical marvel that defies simple mechanical classification. It functions neither as a simple hinge nor a pure ball-and-socket joint. Its axis of rotation is highly oblique, traversing from posterolateral-plantar to anteromedial-dorsal. Specifically, in the transverse plane, the axis deviates approximately 23 degrees medial to the longitudinal axis of the foot. In the sagittal plane, it deviates approximately 41 degrees dorsal from the horizontal plane. This unique obliquity dictates that any motion at the subtalar joint is obligatorily coupled. Subtalar eversion—the hallmark of the flatfoot—produces a simultaneous combined motion of calcaneal valgus, external rotation, and dorsiflexion of the calcaneus relative to the talus.
The Lateral Column and Osteotomy Biomechanics
The lateral column of the foot comprises the calcaneus, the cuboid, and the fourth and fifth metatarsals. In a valgus foot, the lateral column is effectively shortened relative to the medial column. The Evans osteotomy is performed in the anterior calcaneus, precisely between the anterior and middle facets of the subtalar joint, approximately 1 to 1.5 centimeters proximal to the calcaneocuboid (CC) joint. By inserting a structural graft into this osteotomy site, the surgeon forcefully elongates the lateral border of the foot. Biomechanically, this elongation acts through the strong plantar ligaments to push the cuboid and the navicular medially and plantarly. This maneuver effectively reduces the subluxated talonavicular joint, elevates the longitudinal arch, and corrects the hindfoot valgus, all while tensioning the plantar fascia and the spring ligament complex.

Lateral Neurovascular and Tendinous Structures
Executing a lateral approach to the calcaneus demands absolute respect for several critical structures. The sural nerve is the most vulnerable entity during the superficial dissection. It typically courses posterior to the lateral malleolus, descending along the lateral border of the Achilles tendon before curving anteriorly along the lateral aspect of the foot to innervate the lateral heel and the fourth and fifth toes. The incision and subsequent retraction must meticulously protect this nerve to prevent debilitating postoperative neuromas. Deep to the subcutaneous tissues lie the peroneal tendons (fibularis longus and brevis). These tendons run posterior to the lateral malleolus within the common peroneal sheath, secured by the superior and inferior peroneal retinacula. During the osteotomy, these tendons must be carefully mobilized and retracted—typically plantarward—to expose the lateral wall of the anterior calcaneus safely.
The Medial "Danger Zone"
While the surgical approach is entirely lateral, the most catastrophic intraoperative complications occur on the medial side of the calcaneus. The medial neurovascular bundle—comprising the posterior tibial artery, the tibial nerve, and the tendons of the flexor hallucis longus (FHL) and flexor digitorum longus (FDL)—courses directly medial to the calcaneal neck and the sustentaculum tali. When utilizing an oscillating saw to perform the calcaneal osteotomy, the surgeon must exhibit extreme caution to avoid over-penetration of the medial cortex. Plunging through the medial wall can easily transect the posterior tibial artery or the tibial nerve. Therefore, the standard technique dictates cutting the lateral, dorsal, and plantar cortices with the saw, and then carefully completing the medial cortex with a broad osteotome or utilizing it as a greenstick hinge to protect the medial structures.
Exhaustive Indications and Contraindications
Patient selection is the absolute determinant of success for the calcaneal lengthening osteotomy. The primary indication is a severely symptomatic, flexible pes planovalgus deformity that has proven entirely recalcitrant to an exhaustive trial of conservative management, including custom orthoses, physical therapy, and activity modification. The patient typically presents with pain localized to the sinus tarsi—indicative of lateral subfibular impingement—or along the medial longitudinal arch, representing profound strain on the spring ligament and posterior tibial tendon.



Rigorous clinical evaluation is mandatory. The examiner will note the classic "too many toes" sign from a posterior view, reflecting the severe forefoot abduction and hindfoot valgus. Crucially, the deformity must be flexible. This is assessed via the Jack toe raise test or toe standing; in a flexible deformity, engagement of the windlass mechanism via dorsiflexion of the hallux will elevate the longitudinal arch and invert the hindfoot. Furthermore, the Silfverskiöld test is indispensable for evaluating concomitant equinus contractures. If ankle dorsiflexion is limited with the knee extended but corrects with knee flexion, an isolated gastrocnemius contracture is present, necessitating a Strayer procedure. If dorsiflexion is restricted regardless of knee position, a tight Achilles tendon (triceps surae contracture) is diagnosed, requiring a Tendo-Achilles Lengthening (TAL). Addressing the equinus is non-negotiable, as failure to do so will result in massive stress on the midfoot reconstruction and inevitable failure.
Contraindications must be strictly observed to prevent disastrous outcomes. The most absolute contraindication is a rigid flatfoot deformity, most commonly secondary to a tarsal coalition (talocalcaneal or calcaneonavicular). Attempting to lengthen a rigid, arthritic hindfoot will invariably lead to severe pain, joint destruction, and hardware failure. Similarly, advanced arthrosis of the subtalar or talonavicular joints precludes this joint-sparing procedure, pushing the surgical algorithm toward arthrodesis (e.g., subtalar or triple arthrodesis).
| Parameter | Indications for Calcaneal Lengthening | Contraindications for Calcaneal Lengthening |
|---|---|---|
| Deformity Type | Symptomatic, severe flexible pes planovalgus | Rigid flatfoot deformity |
| Joint Status | Preserved articular cartilage in hindfoot/midfoot | Advanced arthrosis of subtalar or talonavicular joints |
| Pathology | Pediatric flexible flatfoot; Stage IIb Adult Acquired Flatfoot | Tarsal coalitions (unless resected simultaneously and mobility restored) |
| Soft Tissue | Competent medial column ligaments (or repairable) | Unreconstructable medial soft tissue failure |
| Neuromuscular | Idiopathic or mild, stable neuromuscular imbalance | Severe, progressive spasticity (relative contraindication) |
Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Evaluation and Templating
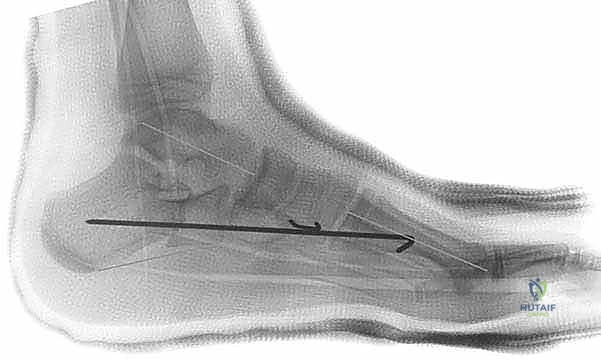
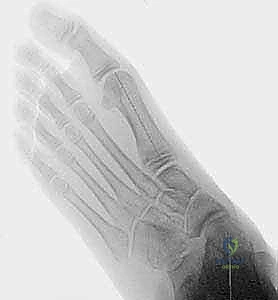
Meticulous preoperative planning begins with high-quality, weight-bearing radiographs of the affected foot and ankle. Essential views include the anteroposterior (AP), lateral, and medial oblique projections. On the AP view, the surgeon assesses the talonavicular coverage angle; an angle greater than 7 degrees indicates significant lateral subluxation of the navicular. The lateral view is critical for evaluating the talar declination angle, the calcaneal pitch, and the presence of a sag at the talonavicular or naviculocuneiform joints (Meary's line).
Templating involves estimating the required length of the lateral column graft. By comparing the medial and lateral column lengths on the AP radiograph, and assessing the degree of talar uncoverage, the surgeon can estimate the necessary distraction gap. Typically, a graft measuring between 8 to 12 millimeters in width is required to achieve optimal correction without overstuffing the lateral column. Over-lengthening is a severe error that forces the foot into a rigid varus position, which is exceptionally poorly tolerated by the patient and often requires revision surgery.
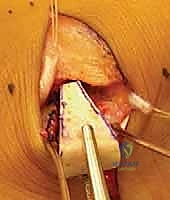
Graft Selection Strategies
The selection of the interpositional graft is a critical decision point. Autologous tricortical iliac crest bone graft (ICBG) remains the historical gold standard due to its unmatched osteoinductive, osteoconductive, and osteogenic properties. However, harvesting ICBG carries significant donor site morbidity, including chronic pain, hematoma, and potential injury to the lateral femoral cutaneous nerve. Consequently, structural allografts—specifically tricortical iliac crest or fibular wedges—have become highly favored. They provide excellent structural support and eliminate donor site morbidity, though they carry a slightly higher risk of delayed union or nonunion. Recently, porous titanium wedges have emerged as a viable synthetic alternative, offering immediate structural stability and promoting osteointegration without the risk of disease transmission associated with allografts.

Patient Positioning and Operating Room Setup
Proper patient positioning is essential for seamless surgical execution. The patient is typically placed in the supine position on a radiolucent operating table. A large, firm bump is placed under the ipsilateral hip. This bump internally rotates the entire lower extremity, bringing the lateral aspect of the foot perfectly parallel to the floor, providing unobstructed access to the surgical site. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying delicate neurovascular structures. The fluoroscopy unit (C-arm) is positioned on the contralateral side of the table, draped sterilely, and must be able to swing freely to obtain intraoperative AP, lateral, and axial views without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
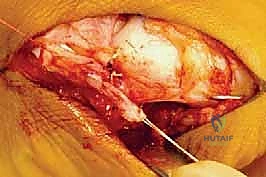
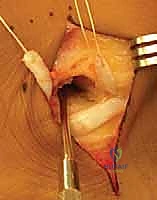
The procedure commences with an oblique lateral incision, often referred to as an Ollier approach, centered over the sinus tarsi. The incision begins slightly proximal and inferior to the tip of the lateral malleolus and extends distally and plantarly toward the base of the fourth metatarsal, directly over the calcaneocuboid joint. Careful, blunt dissection is employed through the subcutaneous tissues. The sural nerve and its communicating branches are meticulously identified, mobilized, and protected with a vessel loop. The nerve is typically retracted dorsally or plantarly depending on its exact anatomical course in the individual patient.
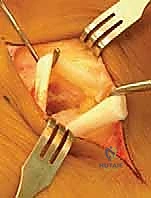


Deep Exposure and Defining the Osteotomy Site
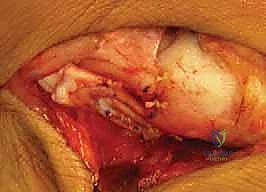
Once the superficial neurovascular structures are secured, attention is turned to the deep fascia. The origin of the extensor digitorum brevis (EDB) muscle is identified within the sinus tarsi. The EDB is sharply elevated from the calcaneus and reflected dorsally. Next, the peroneal retinaculum is incised, and the tendons of the fibularis longus and brevis are identified. These tendons are carefully mobilized and retracted plantarly to expose the lateral wall of the anterior calcaneus. The calcaneocuboid joint is identified visually and confirmed fluoroscopically. The planned osteotomy site is marked 1.0 to 1.5 centimeters proximal to the calcaneocuboid joint line, ensuring the cut will pass between the anterior and middle articular facets of the subtalar joint.



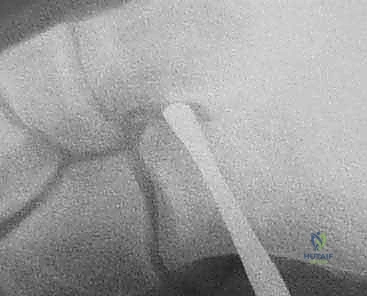
Executing the Osteotomy
Using a sagittal saw equipped with a fine-toothed blade, the osteotomy is initiated perpendicular to the lateral wall of the calcaneus and parallel to the calcaneocuboid joint surface. The saw is used to carefully score and cut the lateral, dorsal, and plantar cortices. Continuous saline irrigation is utilized to prevent thermal necrosis of the bone. Crucially, the saw is stopped just short of the medial cortex. Broad, flat osteotomes are then inserted into the osteotomy site. By gently levering the osteotomes, the medial cortex is either cleanly fractured or utilized as a greenstick hinge. This technique prevents the saw blade from plunging into the medial neurovascular bundle, a catastrophic error.